Patients with
Back Pain
Dr Nick Pendleton
TIMELINE
About this presentation
• The scenarios in this slide
presentation are based wholly or
partly on real patients who have
presented to GP surgeries. They
have been anonymised for use as
a teaching tool for GPs in
Training. For realism the patients
have been given fictional names,
ages and professions.
David Morris
•
•
•
•
•
•
39 years old
Works at a Hotel as a Waiter
Infrequent attender
Usually well
No diagnosed conditions of note
Married , son aged 12
First Consultation – 20 March 2013
Saw Doctor A (GP Partner)
Accidental Fall
• Slipped at work on a greasy kitchen floor.
Fell on right side. Got up and carried on.
Stiffness and bruising 48 hours later. Still has
niggle of pain R loin. Examination normal.
Continue nsaids should settle with time
Second Consultation – 9 May 2013
Saw Doctor B (GP Partner)
• Hip pain esp nocte – following a fall
onto R hip 4-5/52 ago. Refer to
physiotherapist
Third Consultation – 7 June 2013
Doctor B again
Back pain – appt at physio end of
June!
• Expedite letter
• Rx Tramadol
Entry in notes – 10 June 2013
• Urine dipstick test – NEGATIVE.
No sign of infection
Fourth Consultation – June 17 2013
Spoke to Dr C (ST3 Trainee), TRIAGE CALL
• Hip pain – since fall. Also now back pain.
Suspect it is to do with walking because of
hip pain. No red flags. Taking
paracetamol/codeine/tramadol regularly.
Works as a waiter and looks after son.
Struggling. Physio next week....
Fourth Consultation – June 17 2013
Continued...
• Wants sick note/examination as insisting on
scan. Don’t think will need it but reassess
and see what u feel. c/o muscle spasms. ?
Diazepam for a few days.
Outcome – appt given for same day
Fifth Consultation – June 17 2013
Saw Dr D (FY2 Trainee)
• Hip pain – since fall 5/52 ago. Now c/o pain
in lower back. Altered gait to compensate for
R hip pain. No red flags. No neuro
symptoms. Tramadol stopped, didn’t help.
can’t sleep due to pain.
Fifth Consultation – June 17 2013
• Examination – tender ant joint line R hip.
Feels like there is a deep haematoma in R
thigh. No SIJ tenderness. SLR ok, good ROM,
some lower back spasm. No neurology.
• Keen for scan – explained why this is not
appropriate. Rx Codeine 30 mg, diazepam (2
mg x 28). Aware of red flags. To return if
present. MED3 2/52 ACUTE BACK PAIN
RED FLAGS?
• A search of the literature has
shown that 163 Red Flags for
sinister back pain have been
identified!
• Referred pain that is segmental or band-like
• Escalating pain which is poorly responsive to treatment
(including medication)
• Different character or site to previous symptoms
• Funny feelings, odd sensations or heavy legs (multisegmental)
• Lying flat increases pain
• Agonising pain causing anguish & despair
• Gait disturbance, unsteadiness, especially on stairs (not
just a limp)
• Sleep grossly disturbed due to pain being worse at
night
RED FLAGS FOR METASTATIC SPINAL CORD COMPRESSION Greenhalgh & Selfe 2009
• Past Medical History of Cancer (but note
25% of patients do not have a diagnosed
primary)
• A Combination of Red Flags increases
suspicion (the greater number of red flags
the higher the risk and the greater the
urgency)
Sixth Consultation – June 26 2013
Saw Dr E (GP Partner)
• Back pain – weakness right leg, sensation
loss laterally and reduced knee jerk. Needs
scan, if worsens for immediate review,
bowel and urinary function ok and no
sensation loss in perineal area.
• Rx Co-codamol, Naproxen
• MRI SCAN REFERRAL (Lumbar spine)
Seventh Consultation – July 1 2013
Spoke to Dr F (ST3 Trainee)
• Needs MED3, saw Dr E last week. No bladder
or bowel symptoms, no numb bum.
• MED3 2 weeks – Back pain
Eighth Consultation – July 4 2013
Spoke to Dr G (GP Partner)
• Leg pain worse, numbness spread round
from top of leg from lateral aspect to inner.
No bowel, bladder symptoms, no
parasthesia or weakness other than this.
Already referred MRI Scan. Advised re cauda
equina symptoms
• Management plan is sound
CAUDA EQUINA
SYMPTOMS ?
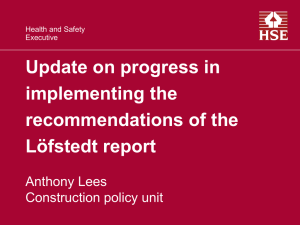
Spinal Cord Anatomy
L1/L2
Cauda Equina Syndrome
• Cauda Equina syndrome is caused by
compression of nerve roots distal to the
level of spinal cord termination (Usually
L1/L2)
• Trauma, vertebral fracture or
displacement, disc herniation, a tumour or
metastatic deposit or an abscess
• Permanent neurological damage can occur
Cauda Equina Syndrome
Low back pain and:
• Bladder dysfunction, usually retention.
• Sphincter disturbance
• Saddle anaesthesia
• Lower limb weakness
• Gait disturbance
• The symptoms and signs depend on
the level of compression
Pain and Deficits Associated with Specific Nerve Roots
Nerve Root
Pain
Sensory
Deficit
Motor Deficit
Reflex Deficit
L2
Anterior medial
thigh
Upper thigh
Slight quadriceps
weakness; hip
flexion; thigh
adduction
Slightly diminished
suprapatellar
L3
Anterior lateral
thigh
Lower thigh
Quadriceps
weakness; knee
extension; thigh
adduction
Patellar or
suprapatellar
L4
Posterolateral thigh, Medial leg
anterior tibia
Knee and foot
extension
Patellar
L5
Dorsum of foot
Dorsum of foot
Dorsiflexion of foot
and toes
Hamstrings
S1-2
Lateral foot
Lateral foot
Plantar flexion of
foot and toes
Achilles
S3-5
Perineum
Saddle
Sphincters
Bulbocavernosus;
anal
Ninth Consultation – July 15 2013
Spoke to Dr E
• MED3 – back pain with neurological
involvement, 2 weeks
• Tenth Consultation with Dr E
• 31st July
• MED3
Eleventh Consultation – August 12 2013
Spoke to Dr H (GP Partner)
• MED3 – back pain with neurology, 2 weeks
22 August 2013. Dr A, logged on at home
reading routine letters
MRI REPORT LUMBAR SPINE 14 August 13
• Diffuse abnormal signal of the bone marrow
and large right and paravertebral soft tissue
masses. Consistent with tumoural process.
Consider lymphoma.
• Encasement of right L3 and L4 nerve roots
• Encasement of the right ureter with
secondary hydronephrosis
Did the Scan result fit with the clinical symptoms?
Nerve
Root
Pain
Sensory Motor
Deficit Deficit
Reflex
Deficit
L3
Anterior
lateral thigh
Lower thigh
Patellar or
suprapatellar
L4
Posterolateral Medial leg
thigh, anterior
tibia
Quadriceps
weakness;
knee
extension;
thigh
adduction
Knee and foot Patellar
extension
Consultation with Dr A, 23 August 2013
12th consultation, was asked tci urgently
Breaking bad news, at end of morning clinic
Came with his wife
Possibly lymphoma
This is a type of cancer
Already spoken to Haematology Consultant
and arranged appt next week
• Next step is a biopsy
•
•
•
•
•
•
Consultation with Dr A, 23 August 2013
• David: “So all this has been caused
by a slipping in the kitchen?!”
Summary of Timeline
Date and Doctor
Diagnosis Code
Outcome
20 March, Dr A
Accidental Fall
Should settle with time
9 May, Dr B
Hip Pain
Physio referral
7 June, Dr B
Back Pain
Expedite Physio, Rx
17 June, Dr C
Hip Pain
Given appt tci
17 June, Dr D
Hip Pain
Analgesia, request for scan declined
26 June, Dr E
Back Pain
MRI SCAN lumbar spine referral
1 July, Dr F
Back Pain
MED3
4 July, Dr G
Leg Pain
Advice re: cauda equina symptoms
15 July, Dr E
Back Pain
MED3
31 July, Dr E
Back Pain
MED3
12 August, Dr H
Back Pain
MED3
14 August
HAD MRI SCAN
Faxed to surgery
22 August, Dr A
Read report
Appt next day to discuss result
Letter from Haematologist – 1 Oct 2013
• Well, paresthesia on thigh has resolved
• No lymphadenopathy
• CT-Guided Biopsy Result – Diffuse Large BCell Lymphoma
• Treatment – To have Chemotherapy
Victor Parker
•
•
•
•
•
•
66
Moderate COPD, borderline DM
On Seretide and Spiriva inhalers
Ex-smoker
Retired Joiner
Lives with wife
Consultation No. 1
•
•
•
•
•
I‘ve got pain in my back!
It came on over the weekend
I had been stretching up to paint the ceiling
Its really sore
Its next to my right shoulder blade
• Examined: no bony tenderness
• Conclusion: likely to have strained back by painting
ceiling
• Analgesia Rx. Co-codamol 30/500
• See again if worsens
Consultation No. 2 later that week
• The doctor said to come back if it got worse
• It has got worse, the co-codamol are not helping
• Examined: tenderness over the right side of upper
thoracic vertebra
• Outcome: Rx Tramadol. Refer for MRI Scan of
thoracic spine
• Differential diagnosis ?
• This Dr ordered an MRI scan to investigate, but what
would you do?
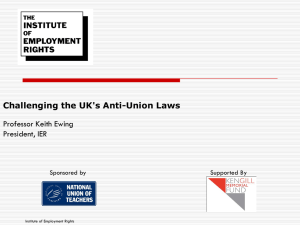
Myeloma: 2008-2010
Average Number of New Cases Per Year and Age-Specific Incidence Rates per 100,000 Population, UK
Please include the citation provided in our Frequently Asked Questions when reproducing this chart: http://info.cancerresearchuk.org/cancerstats/faqs/#How
Prepared by Cancer Research UK - original data sources are available from http://www.cancerresearchuk.org/cancer-info/cancerstats/
What is Multiple Myeloma?
• Plasma cell in Bone Marrow becomes
malignant
• Plasma cells are a type of WBC
• Plasma cells usually produce immunoglobulins
(antibodies)
• Plasma cell clones multiply and accumulate in
bone marrow
• Immunoglobulins (antibodies) are also known
as ‘paraproteins’
• The malignant plasma cells make vast
quantities of Ig’s = paraproteinaemia
Myeloma Disease Process
• The type of paraproteinaemia depends on
the type of plasma cell which became
malignant
• Commonest is IgG Myeloma
• The plasma cell tumours are known as
plasmacytomas, they spread and damage
bone affecting multiple areas of the
skeleton
• This causes hypercalcaemia
• The paraproteins cause renal damage
Myeloma can lead to.....
•
•
•
•
•
•
•
•
•
Pathological fractures
Nerve compression
Renal failure
Bone pain
Hypercalcaemia symptoms
Anaemia
Thombocytopaenia
Serious infections (only 1 type of Ig)
Hyperviscosity
MYELOMA SCREEN
• Full blood count
• ESR or plasma viscosity
• Urea, Creatinine, Calcium, Albumin
• Electrophoresis of serum and concentrated urine
including 24 hour Urine for Bence-Jones Protein
light chains (typical antibody = 2 light chains + 2
heavy chains)
• +/- Xray of painful region, lytic lesions,
pathological fractures
Dr Henry Bence-Jones
developed a light chain protein urine test in 1847
A crystal of BJ
Protein:
Ig light chains leak
into urine due to
renal failure
Chemist and Physician. 1813- 1873.
What is the Treatment for
Myeloma?
• Young patients who can tolerate aggressive
treatment – Stem Cell Transplant (autologous or
allogeneic)
• Following 6-9/12 treatment with:
• Chemotherapy + Steroids +Thalidomide
• Older patients >70: mephalan, pred &
thalidomide (MPT)
• Treatment for 12-18 months, 80% respond, well
for 2-3 years and then relapse
Thalidomide
• Recently approved for use in combination
with steroids for the treatment of newly
diagnosed Multiple Myeloma
• Interferes with signals affecting myeloma
cell multiplication and spread
• Inhibits new blood supply (angiogenesis)
• Patients must not become pregnant or
father children on treatment with
thalidomide
Victor Parker – Home Visit Request
2 weeks later at 11:30am
• His wife rang: ‘Can you come and see Vic,
He tried to get up to go to the loo this
morning and he says his legs are too
weak! He stumbled on the stairs
yesterday and he’s got pain in the bottom
of his back’
Victor Parker – Home Visit Request
The Doctor visits straight away:
• Back Pain: Unable to stand due to weakness
of legs. Unable to pass urine into container by
bed, ?bladder palpable. no ankle reflexes and
loss of sensation to perineum/perianally. Poor
anal tone. Spoke to Neurosurgeons at Hope
? Cauda Equina Syndrome
Victor Parker - Outcome
Radiology report in hospital
• L5 vertebral collapse causing compression
of cauda equina, partial compression
fracture of T6 noted, no cord compromise
at this level, multiple lytic lesions of spine
and ribs, consider myeloma as first
differential. report phoned to neurosurgery
team – for urgent decompression at L5/S1
Victor Parker - Outcome
•
•
•
•
•
Had decompression surgery
Spent 3 weeks in hospital
Still has leg weakness but normal bladder function
Myeloma was confirmed – chemo, steroids, thalidomide
Whilst in hospital appointment came through for MRI
arranged by GP
• Shortly after discharge his wife (and main carer) had
a sudden episode of drooping of left side of mouth
with an irregularly irregular pulse...
Mr Bob Peters 83, Type 2 DM
• 23 June 2014 – left-sided low back
pain and hip pain (chronic)
• Examination of hip and back
normal
• No bony tenderness
• OA lumbar spine likely
• Analgesia advice – add codeine to
paracetamol
21 July 2014
• Diarrhoea symptoms 1 month
• Loss of appetite
• Loss of 1 stone in weight in 1 month
• PR normal
• Abdo exam normal
• FH Bowel Cancer
• Referred for colonoscopy 2WW
13 August 2014
• Colonoscopy normal
•
•
•
•
•
17 August
Attended OOH GP – fever, malaise, dysuria
No urine to dip, T 37.8, tender suprapubically
Suspected UTI
Trimethoprim 200mg bd 7 days
22 August 2014
• Reviewed following OOH GP attendance
• Symptoms better but feels drained
• Urine dipstick normal, T 36.9
• No signs of ongoing infection
• Antibiotics finish today
• Recovering from illness
8 September
• Still not fully recovered from UTI, feels
lethargic
• Still has back pain, slightly worse.
• Bloods arranged inc PSA , Bone profile,
CRP, UE eGFR, FBC, HbA1c, LFT
24 September 2014
Blood results
• PSA 47 (< 6.70 ug/L)
• Hb 12.7
• HbA1c 48
• ALT 37.4 (<5)
• CRP 37.4 (<5)
• eGFR 63, creatinine 110 (62-124)
• ALP 141 (<130)
• Other blood tests parameters normal
26 September 2014
• Results discussed with patient
• Prostate Cancer likely
• Referred Urology 2WW
•
•
•
•
•
3 October
Emergency appointment
Severe left-sided back pain, loin to groin, colicky
Apyrexial, abdomen soft, feels pain in renal angle
Referred surgeons ? Renal colic
CT Scan during Admission
• Suggestive of prostate cancer with nodal involvement
• Filling defect in left sided renal pelvis
• Diagnosis: Ureteric obstruction secondary to
prostate cancer
• Biopsy done
• Started on Cyproterone and to have Zoladex in clinic
Managing Neuropathic Pain
NICE GUIDELINE CG96 (Health Technology Appraisal)
1. Amitriptyline or Pregabalin
2. Pregabalin (if 1st used was Amitriptyline or other TCA)
3. Refer to Pain Team and add or change to Tramadol
• Don’t start opoids other than Tramadol without specialist
assessment
LOCAL GMMMG GUIDELINE
1. Amitriptyline
2. Nortriptyline/imipramine to maximum doses
3. Gabapentin
4. Pregabalin (if started 1st and not effective go back to step 1)
5. Carbamazepine or other anticonvulsant
GMMMG Guidance
• GMMMG met and considered the NICE guideline
CG96. (without access to the evidence NICE
considered)
• NICE places products equally in the guideline when
there is an acquisition cost difference of 20 – 60 times
difference per month.
• Implementation of the guideline would have lead to
an additional financial pressure of £12.8 million
Drugs licensed for treatment of neuropathic pain
Amitriptyline
Not licensed for neuropathic pain
Duloxetine
Licensed for painful diabetic
neuropathy
Imipramine
Not licensed for neuropathic pain
Lidocaine (topical)
Licensed for post-herpetic neuralgia
Nortriptyline
Not licensed for neuropathic pain
Gabapentin
Licensed for neuropathic pain
Pregabalin
Licensed for central and peripheral
neuropathic pain
Tramadol
Licensed for moderate and severe
pain
Response from NICE
• NICE is aware that there have been concerns about the
associated costs that pregabalin may bring to the NHS
as one of the first line treatment options for adults with
neuropathic pain
• Therefore, NICE will fully update its clinical guideline in
order to address ongoing uncertainties regarding the
cost effectiveness of some of the recommended
treatment options
• Until a further announcement is made, the original
guideline (CG96) continues to represent best practice
for the NHS
The Back Book (RCGP)
• http://www.wsib.on.ca/files/Content/DownloadableFil
eTheBackBook/BackBookEnglish.pdf
Upcoming Sessions
• 11th November 2014: Confidentiality
and Consent (MDDUS)
• 25th November 2014: TBC
• 9th December 2014: COPD (Michaela
Bowden)