Decompensated cirrhosis * hospital perspective
advertisement

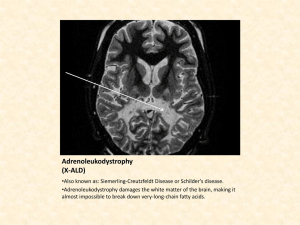
The Critically Ill Alcoholic – A Daily Challenge PERSONAL INTRODUCTION A DIFFICULT CASE MEDICAL AND ETHICAL FACTORS DISCUSSION & QUESTIONS Your speaker – Dr Philip Berry University of Bristol (qual. 1996) Roehampton, Kingston, St Thomas’, Sydney (ICU) SW Thames gastroenterology rotation MD at Kings College Hospital - Institute of Liver Studies Hepatology - Royal Free Hospital, University College Hospital Appointed FPH November 2010 Interests Decompensated cirrhosis and prognosis Critical illness, interface with ICU Advanced endoscopy Medical ethics General gastroenterology MW, 55 years old, known ALD 2010 VB, Ascites, recovered MW, 55 years old, known ALD 2010 VB, Ascites, recovered 2012 Jaundice Ascites Confusion MW, 55 years old, known ALD 2010 VB, Ascites, recovered 2012 Jaundice Ascites Confusion O/E Icteric++ Fever Large abdomen Aterixis MW, 55 years old, known ALD 2010 VB, Ascites, recovered 2012 Jaundice Ascites Confusion O/E Icteric++ Fever Large abdomen Aterixis Ix Bili 346 µmol/L INR 2.8 Hb 10.4 g/dL Creat 280 µmol/L Further Ix Tap – 460 PMN/ml MW, 55 years old, known ALD 2010 VB, Ascites, recovered 2012 Jaundice Ascites Confusion O/E Icteric++ Fever Large abdomen Aterixis Ix Bili 346 µmol/L INR 2.8 Hb 10.4 g/dL Creat 280 µmol/L Further Ix Tap – 460 PMN/ml Tx CVC Tazocin Albumin Terlipressin ADU MW, 55 years old, known ALD Later that night: Semi-comatose Hypotensive Oligoanuric ABG – acidosis Hypoxic ICU – full organ support ADU/HDU ceiling of care Ward – palliative care MW, 55 years old, known ALD Later that night: Semi-comatose Hypotensive Oligoanuric ABG – acidosis Hypoxic ICU – full organ support ADU/HDU ceiling of care Ward – palliative care Should he be admitted to ITU? Is it appropriate? Considerations: He will definitely die without organ support - Fact What is the chance of short term survival on ICU? What is the longer term outlook? What is the duration of therapy that will be required? Cost? – should we be asking ourselves this? Does he deserve another ‘throw of the dice’? – should we be asking this? National burden of decompensated CLD In the UK, between 1990 and 2003, admissions for chronic liver disease (CLD) rose by 71% in males and 43% in females. These changes were largely driven by alcohol related liver disease (ARLD) with rates more than doubling in all age groups. There has been a five-fold increase in progression to cirrhosis in 35-55 year olds over the last 10 years. Between 1996 and 2005 the percentage of ICU admissions in England and Wales with ARLD rose from 0.65% to 1.35%, the estimated number of bed days rising from 3100 to over 10000. Single rising cause of death The National Plan for Liver Services UK 2009 A Time to Act: Improving Liver Health and Outcomes in Liver Disease Experience of ALD at FPH 66 patients with decompensated cirrhosis leading to 154 admissions over 12 months ALD HCV HBV ALD ALD/Fluclox HFE/ALD NASH PSC First presentation Ongoing alcohol use Abstinence Experience of ALD at FPH In-hospital mortality: Ward - 5% HDU - 14% ICU - 36% LEVEL of CARE ICU HDU Ward 0 5 10 15 20 25 30 35 40 Length of Stay and Mortality 90 day mortality: Ward - 8% HDU - 21% ICU - 50% 50 45 40 35 30 25 Ward 20 HDU ICU 15 10 ICU 5 HDU 0 LOS (d) Ward In-hospital mortality (%) 90 day mortality (%) Therapeutic nihilism 100 cirrhotic patients requiring mechanical ventilation. Overall mortality rate was 89% 100% among patients with septic shock and/or superimposed acute hepatitis and/or severe cirrhosis defined with clinical signs: jaundice and/or ascites and/or spontaneous hepatic encephalopathy and/or severe malnutrition (Goldfarb 1983) Relative optimism! Secondary care data, which may reflect a less highly selected cohort of patients with CLD, has demonstrated ICU and hospital mortality rates of only 38% and 47% respectively (Thomson et al, 2010) Recent analysis of 16,000 admissions to ICU O’Brien et al, 2012 Guidance “…organ support should be offered to those with pre-morbid MELD <15, but questioned if MELD is >30 and there is >/= 3 organ failure...” Guidance “…organ support should be offered to those with pre-morbid MELD <15, but questioned if MELD is >30 and there is >/= 3 organ failure...” MELD = 40 CVS RS Renal Don’t judge too soon Score Admission ROC 48hr ROC CPS 0.75 0.78 MELD 0.78 0.86 APACHE II 0.75 0.78 SOFA 0.81 0.88 FOS 0.79 0.85 Cholongitas et al, 2008 Self-inflicted pathology ‘Good Medical Practice’: “The investigations or treatment you provide or arrange must be based on the assessment you and the patient make of their needs and priorities, and on your clinical judgement about the likely effectiveness of the treatment options. You must not refuse or delay treatment because you believe that a patient's actions have contributed to their condition...”. Moral Responsibility ‘Recidivists’ cannot resist the urge to drink The power of the individual to resist cravings is equated, in the eyes of some authors, to their degree of ‘moral responsibility’. There is ample time during an alcoholic’s life to receive advice and comprehend the damage that it is doing; therefore the decision to continue must involve a personal acceptance that the individual will become ill. (Glannon, 1998) Moral Responsibility There is a responsibility that individuals should actively seek help once it becomes clear that alcohol addiction has developed and those who do not must bear some responsibility for this failure. Those who do, but for whom attempts to break the addiction fail, might be regarded in a more positive light. (Moss AH, 1991) Is help available? NICE has only recently published guidelines for identifying, treating and supporting alcohol addicted patients. The interventions suggested (pharmacological, psychological and psychosocial) demand the provision of many suitably trained staff. It is likely that many patients presenting now will have not had the benefit of such structured therapy. Factors beyond their power Gender Genes Cofactors Social factors Abuse Parental example ‘Gremlins’ Gremlins Dir. Paul Watson, 2007 The cost -The impact of organ dysfunction in cirrhosis: survival at a cost?- (Shawcross et al, 2012) Alcohol was the most common etiology (47%) and variceal bleeding (VB) the most common reason for admission (35%). Invasive ventilatory support was required in 74% of cases, vasopressors in 49%, and 50% required renal replacement therapy. Forty-nine per cent of non-transplanted patients survived to ICU discharge. Median ICU cost per patient was €14,139. Futility & Rationing “medical futility signifies that a treatment offers no therapeutic benefit to a patient…rationing specifically acknowledges that a treatment does offer a benefit, and the issue becomes how to distribute beneficial but limited resources fairly.” “To clarify the distinction further: futility decisions are made at the bedside of a specific patient, whereas rationing decisions, involving categories of patients or treatments or circumstances, inevitably should be made at a policy level in order to assure just distribution of resources.” (Jecker NS, Schneiderman LJ, 1992) Public Opinion Decision Time? Decision Time? o No snap decisions re. prognosis o Reversible factors? o Patient preference? o Family view o Recognise death wheh it is happening o Negotiation with ICU: • Don’t behave as if liver patients are ‘special’ • But if you don’t advocate for them who will? • Trial of therapy, 3-5 days • Restrict haemofiltration • Agreed withdrawal criteria • Prepare the ground with family