Presenting Yourself in Social Media
advertisement

AUB
Nml
cycle – bleeding every 28 days
lasting 3-5 days 30-50 mL of blood loss
AUB is any departure from norm (too
much, too little, inappropriate schedule)
DUB – idiopathic heavy and/or irregular
bleeding that cannot be attributed to
another cause (anovulation or
oligoovulation)
Patterns of AUB
PALM-COEIN classification system of AUB
PALM (structural causes) – Polyps, Adenomyosis,
Leiomyomas, Malignancy/hyperplasia
COEIN (nonstructural causes) – Coagulopathy,
Ovulatory dysfunction, Endometrial, Iatrogenic,
Not Yet Classified
MENORRHAGIA
Excessive flw in duration (>7 days) or volume (>80 mL)
Caused by uterine fidrobids, adenomyosis, endometrial polyps; less
endometrial hyperplasia or cancer or cervical polyyps
Teans should be tested for primary bleeding d/o (von Willebrand dz, ITP,
platelet disfunction, thrombocytopenia from malignancy)
Test for CBC, platelet count, PT/PTT, factor VIII, von Willebrand factor antigen and
activity
Cryptorchidism
• 1% 1 y/o boys
• Complete or incomplete failure of the intra-abdominal testes to
descend into the scrotal sac
• U/l in most cases
• Characterized by an arrest in development of germ cells
associated with marked hyalinization and thickening of the BM
of the spermatic tubules
• In most patients the undescended testis is palpable in the
inguinal canal
• Condition is completely asymptomatic, found by patient or the
examining physiian only when scrotal sac is discovered not to
contain the testis
* Regularly timed menses with light flow
* Caused by hypogonadotropic hypogonadism
(anorexic pts and athletes); Asherman’s
syndrome (intrauterine adhesions), congenital
malformations, infection, intrauterine trauma,
OCPs/depo/progestin IUDs, endometrial
ablation all have atrophic endometrium; outlet
obstruction secondary to cervical stenosis or
congenital abn
*
Metrrrorrrrhagia – bleeding between regular
periods (less than normal)
Caused by cervical lesions, endometrial polyps,
carcinoma
Menometrrrorrrrhagia – excessive (>80 mL) or
prolonged bleeding at irregular intervals
Caused by uterine fibroids, adenomyosis,
endometrial polyps, hypereplasia, cancer
Metrorrhagia and
Menometrorrhagia
Oligomenorrhea
• Periods > 35 days apart
• Caused by disruption of hypothalamicpituitary-gonadal axis or systemic dz
(hyperprolactinemia and thyroid d/o); PCOS,
chronic anovulation, pregnancy, thyroid dz
Polymenorrhea
• Periods <21 days apart
• Usually caused by anovulation
Evaluation
History – timing of bleeding, quantity, menstrual hx/menarche, associated
symptoms, family hx
Physical – rectal, urethral, vaginal and cervical causes r/o; PCOS symptoms
(hirsutisum, acne, truncal obesity, acanthosis nigricans); thyroid dz
(thromegaly, skin changes, diaphoresis, increased pulse); bleeding d/o
(bruising, petechiae); PAP smear for cervical dysplasia and cancer; cervical
cultures for infection
Lab eval (tailored)
Light skipped cycles – preg test, TSH, PRL, FSH (menopaus/POI)
Heavy/frequent/prolonged – preg test, TSH, CBC
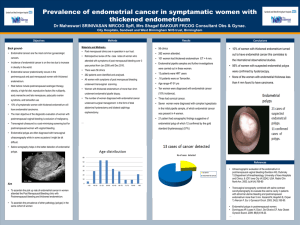
F >45 with AUB needs endometrial biopsy to r/o endometrial hyperplasia and
cancer (or obese if <45 – peripheral conversion of androgens into estrogens in
adipose cells)
Pelvic US for endometrial polyps, fibroids, hyperplasia, cancers, adnexal masses
Sonohysterogram to see intrauterine defects if pathology on pelvic US
MRI to distinguish adenomyosis from uterine fibroids
Hysteroscopy to visualize intrauterine cavity
D&C provides tissue for diagnosis
TREATMENT
Depends on underlying etiology
Sypmtomatic fibroids/polyps – resection/removal
Adenomyosis – hormonal regulation (OCPs, Mirena), endometrial ablation (done
bearing children)/resection, hysterectomy
Cervical polyps – polypectomy
Endometrial polyps – Hysteroscopy, polypectomy +/- D&C, endometrial ablation,
hysterectomy
Endometrial hyperplasia – progestin therapy, D&C, hysterectomy
Endometrial Cancer – Hysterectomy, BSO, radiation
Hormonal Problems
Anovulation – menstrual regulation with estrogens/progestins and weight loss
Hypothyroidism – thyroid hormone replacement
Hyperprolactinemia – DA agonists
DUB
No pathologic cause of AUB identified
Most pts with are anovulatory (ovary produces estrogen but no corpus
luteum is formed and no progesterone is produced); continuous
estrogenic stimulation of the endometrium without the usual
progesterone-induced bleeding – endometrium continues to proliferate
until it outgrows its blood supply, breaks down, sloughs of in irregular
fashion
Occurs in hypothyroidism, hyperprolactinemia, hyperandrogenism,
POI/PMOF, adolescence, perimenopause, lactation, pregnancy
Determine if pt is ovulating by basal body temp OR 21-23 serum
progesterone
Tx – NSAIDs for chronic, hormonal therapy (OCPs, OrthoEvra Patch,
Nuva Ring)
• If estrogen CI (HTN, thrombophilias, hx DVT/PE, >35 y/o and smoke)
can use progestin only options (depo, Mirena, Implanon)
• D&C, hysterectomy
Most Common Power Point
Mistakes
http://www.youtube.com/watch?v=GxSQ-0FWHNk
Objectives
Learn how to structure and give a strong
presentation
Learn some techniques that will allow you to
communicate effectively
Learn some personal etiquette rules to follow
Power Point Structure
Introduction
Content
Conclusion
Introduction
Objectives
Motivation
Prerequisite knowledge
Agenda
Content
Overview/Advanced Organizer
Content matches stated learning objectives
Skills/tasks to be learned were demonstrated
effectively
Current guidelines, recommendations, or
studies incorporated
Conclusion
Summary
References
Slides
Easily digestible portions of information
Directed attention at important information
Font size/style made easily readable
Color scheme/background appealing and not
distracting
Images/charts large enough to read easily
Delivery
Room and materials set up according to needs
of lesson
Speak and enunciate well
Body language should convey meaning and
should not be distracting
Personal Presentation
Speech
Appearance
Tone
Tone
Monotone vs. Emotion
Should match your speech and body language
Speech
Filler Words
Speed
Pronunciation
Enunciation
Appearance
Body language
Stance
Eye Contact
Gestures
Etiquette Fun Facts
At social events, keep right hand free for shaking hands
Always say your full name
Always stand when being introduced
Handshake (practice)
10 second Elevator Speech about yourself and why you are at an event
If you are at the dinner table you drop anything, don’t pick it up
Business Cards
Dinner Etiquette
B and D Fingers
Turn cup over if you
don’t want coffee or
tea
Fork and knife at end of
meal
Fold napkin on chair
when leaving table
Place hand bags on the
floor
Cut food as you eat it
Bread and Butter
Don’t drink while your
mouth is full of food
Passing around the
table
Don’t hand your plate
to the waiter
Summary
Keep your presentation simple and well
organized
Start practicing how you present yourself NOW,
however often you want!
Keep in mind there are some rules of etiquette
for different situations and try to follow them.
We gave you some but there are plenty of
resources to continue learning from!
Professionalism
“Professional competence is
the habitual and judicious use
of communication,
knowledge, technical skills,
clinical reasoning, emotions,
values, and reflection in daily
practice for the benefit of the
individual and community
being served.”
•
• Representing one’s
profession by encouraging
trust from patients in their
physicians.
Inter-professionalism
• The first priority of interprofessional education is to
create an inter-professional
team approach to
healthcare and overall
health care delivery. This is
theorized to help increase
communication, bring a
better understanding of
individual professional roles,
decrease duplication, and
improve patient care and
outcomes.
Social Media/Electronic
Information
Emails and Texts
• Professional Communication
•Err on the side of formality.
•Read/Edit/Spell-check
•Avoid excessive formatting.
•Forward with caution.
•Responding to sensitive or
emotionally charged emails
• Rotations!
Social Media
Who is your audience?
Legal Precedent/Guidelines
• Slow but evolving
• Based on jurisdiction
• Free speech?
School Policies
• 10% of LCME medical schools have policies in their
student handbooks.
• Cyber bullying/stalking
Hospitals/Health
Networks
• Many large hospitals and networks have media
policies that tend to be more strict then schools.
Organizations/Profession
•
COSGP
• “I do hereby affirm that I will represent and serve my fellow students in
good judgment and diligence, always striving to uphold the principles of
the osteopathic oath, so entrusted to me as a future physician.”
•
Profession
• You represent yourself AND the organizations/groups/communities that
you are affiliated with.
• Your professional status is reaffirmed daily. You are responsible for
protecting that professional reputation.
What is concrete?
Tough Call
• A patient friend requests a
medical student.
o This is almost always inappropriate unless the Dr./medical
student- pt relationship has ended. Even after the Dr. pt
relationship has ended it would be inappropriate to discuss
health related info.
• A medical student tweets that he just finished rounds
with the residents on a pt and describes the clinical
findings of that patient.
-
It’s difficult to be certain that info disclosed on twitter is not
identifiable to that particular patent. The best types of posting
would include very general information. Other posts by the
same student could have indicated their medical school and
current rotations leading to circumstances that indirectly
indentify the pt. such as by naming a distinct disease or
symptom.
Tough Call
•
•
A med student writes in her blog naming an attending who did minimal
teaching on rounds and recommending that other students not take clinical
electives with that physician OR Med student posts to wall that half the class
slept during student doctor Liu’s lecture.
• Legitimate critique of an education activity is appropriate so long as
professionalism is maintained. There are ore effective and less public
mechanisms for relaying this type of info and the student may be
counseled accordingly.
Med student posts photo of patient with good intentions and receiving the
patients’ verbal ok.
• Without written consent this is a clear violation of patient confidentiality
even if the pt is not named and no other identifiable info is used.
Tough Call
•
Med student posts about how the hospital’s equipment they are rotating at should
have been replaced years ago and is unreliable.
• The public disclosure of such info increases the liability for the hospital health
system and is clearly unprofessional. There are legitimate and confidential
mechanisms for improving quality at the hospital.
•
Medical student posts that her teacher/attending wears too much cologne, has bad
taste in clothes, has a gross mustache, and takes overly long lunch breaks.
• Inappropriate forum and set of comments and demonstrates
unprofessional behavior by the student. There are legitimate and
confidential mechanisms for addressing valid concerns in schools and
the workplace.
•
Medical student wearing a Mayo Clinic Tee-shirt has a picture posted of them at a
bar clearly inebriated.
• 1) Hospital logo indentifies the affiliation to the institution and
• 2) The unprofessional behavior of the student is available for all to see, including
future employers and patients. The med student did not post the photo but
should do everything possible to have the photo removed and remove the
tagging link to the students own Facebook page.
Ten Recommendations
1)
Use good judgment.
• Think about how you want the public to view you as a person
and as a medical professional since you represent your
profession at all times.
• Don’t want to undermine your credibility or the reputation of
your colleagues and affiliations.
• Think before you post if there are people you wouldn’t want
to see what you are posting, liking, photos, etc.
2) Privacy Settings
Many can view your Facebook so go to settings and click view
as to see your profile as a random non-friend individual.
•
3) Check your school’s policy and that of the hospitals you rotate at.
4) Seek expert guidance.
•
Some schools have a specific person to contact if you have any
question about what is allowed and what is not.
5) Protect patient privacy.
Ten Recommendations
6) Respect work commitments (make sure not interfering with work
commitments).
7) False and unsubstantiated claims and inaccurate or inflammatory postings
may create liability for you.
8) Consider using a disclaimer such as the views expressed on this {post, blog, etc}
are my own and do not reflect the views of my {school, rotation site, etc}.
However this is not fool proof.
9) Respect copyright and fair use laws.
10) Protect propriety information.