kda--curved canals 2014
advertisement

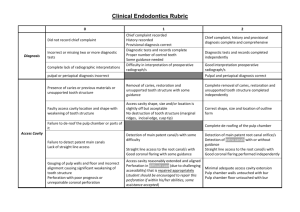
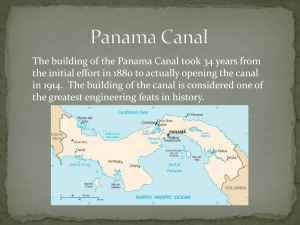
BDS(NBI), CIBRD(KASADA), MDSc-Endo(Mal), Cert. In Oral Implantology (Mal) SPECIALIST ENDODONTIST,IMPLANT PRACTITIONER AND LECTURER Dept of Conservative Dentistry University of Nairobi Practice limited to Endodontics and implantology E-Mail: tomdienya@uonbi.ac.ke or tomdienya@yahoo.com Introduction and Lit review The goal of endodontic therapy is the prevention and/or elimination of pathosis of endodontic origin Correct diagnosis SUCCESFULL RCT Complete obturation Cleaning and Debridement (European Society of Endodontology Consensus, 1994, Omer et al., 2004, , FDI World Dental Press, 2005 ). Introduction and Lit Review cont.. Detailed Knowledge of ROOT CANAL SYSTEM Inadequate understanding Of Root Canal Systems Improper shaping And Inadequate Cleaning SUCCESSFUL ROOT CANAL Poor Obturation Omer et al.,2004,Mikrogeorgis et al.,1999,Al-Nazhan,2007 Treatment Failure Carrotte,2004 INTRODUCTION CONT.. A tooth with a straight root and a straight root canal is an exception rather than being normal because most teeth show some curvature of the canal (weinne,scheinder,kyomin). Tomes, in 1848, called such curvatures as dilacerations Dilaceration: Defination It refers to an angulation or a bend or a curve in the root or crown of formed tooth or a deviation or in the linear relationship of a crown of a tooth to its root. Epidemiology In most studies,prevalence of curvature ranged between 80 to 100%. Dienya et al 2009 in a study of 400 maxillary and mandibular 1st molars in a Kenyan population got 91% curvature. Dr Schaffer in Germany examined 1163 root canals and found that 980 (84%) were curved and 65% showed an angle > 27 degrees with radii < 40 mm. CAUSE The condition is thought to be due to trauma during the period in which tooth is forming. The result is that the position of the calcified portion of the tooth is changed and the remainder of the tooth is formed at an angle Types of curvatures Curved canals can be: Gradual curvature of the canals in the coronal,middle or apical third; Acute curvature in the apical third; Curvature throughout the canal; S-shaped root canal. Mandibular 1st molar with GRADUAL distal curvature of the mesial root Maxillary molar with the DB root showing ACUTE curvature in the apical third Buccal curvature at the tip of a palatal root Mandibular 1st molar with an S-curvature of the D root Combination of S-shaped canals and gradual shape THE STAIR CASE CURVE THE DECEIVING CURVE --distal root curves lingually THE CONSEQUENCES 1) EXCESSIVE FLARING 2) LEDGING 3) APICAL TRANSPORTATION 4) APICAL PERFORATION SHORT OBTURATION- due to inability to negotiate curvature Common to all curvatures: • Instruments break unexpectedly • Separated apical part is difficult to remove Instruments separation just at the beginning of the curve Missed canal in maxillary 1st molars Note : Canal was missed probably due to it being hidden at the beginning of the curve presence of lamina dura—indicates canal presence pain Management Start with accurate diagnosis preoperative radiographs taken with parallelling technique with at least two different views-SLOB RULE: UPPER TEETH-normal buccal view,then use rule MMMM LOWER TEETH—normal buccal view then use the rule DMMD or use CBCT OR DIGITAL X-RAYS Paralleling technique in the lower jaw Parallel periapicals Root canal configurations obtained with CBCT Type I Type V Type II Type VI Type III Additional Canals 1 Addition al canal 2 Type IV Additiona l Canal 3 Make a good access cavity Pitfalls of inadequate access Inadequate acess easily leads to ledging Remnants of pulp roof removed by slow speed round bur Straight line access achieved Determine the DEGREE OF curvature Before initiation of treatment, an estimate should be made as to the degree of curvature of canals by seeing the radiograph, probing OR schneiders method The interior angle is formed by intersection of the straight line from the orifice through coronal portion of the root and another straight line from apex through apical portion of canal Take an impression of the canal S-shaped c-shaped J--shaped Merging canals USE CROWN DOWN TECHNIQUE Divide the root into three Flare coronal one third and open up orifice-use orifice shapers Or 25/07 in mtwo system or sx in protaper system—Do not use gates glidden. ENDOFLARE 1 Before ENDOFLARE® filing - Pronounced dentinal overhang 2 ENDOFLARE® filing (penetration < coronal third) 3 After ENDOFLARE® filing - Elimination of the coronal strains BEFORE AFTER Pr. CALAS Working length Working length-practical determination Use apex locators—such as raypex 6 or vdw motor No direct measurements on file Direct measurements are likely to introduce errors MEASURE CURVATURE by tracing rules R>160------stainless steel handfiles can be used R—140—160---consider precurving stainless steel files or use rotary R –100—140—rotary with initial glide path;use highly flexible files with radial lands or use rotary in straight portion and hand files apically R –90—100—niti hand files with high flexibility; orifice shapers only coronally R—90 or less—consider apicoectomy and reverse filling,aggressive use of hand niti management USE OF HAND NITI FILES Tedious..some files can break due to torsional stress PRECURVING STAINLESS STEEL FILES Crown Down Technique Crown Down Technique Coronal third Middle third Apical third Orifice shapers 0.06 taper rotary 0.04 OR 0.02 taper hand or rotary FILES TO USE HERO Shapers Red sequence Red sequence for average difficult cases 25 6% 2/3 WL 25 4% WL 30 4% WL 2/3 WL WL + + HERO Shaper Yellow sequence HERO Shaper Yellow sequence Yellow sequence for difficult cases 20 6% 20 4% 25 4% 30 4% 2/3 WL WL WL WL 2/3 WL WL + + + Preparation of coronal third Preparation of middle third Preparation of the apical third Prepare to actual working length Use 0.04 taper NiTi hand files in sequence smaller to larger Preparation of apical third Irrigation needle should have side opening to opening to preven driping of irrigant fluid hence pain Acoustic streaming around a file in free water (left) and a schematic drawing (right). cases Extensive Amalgams-can be very painful necessitating endo-therapy