Diuretics
Moustafa K.Soltan
Diuretic
is substance that increases the urine excretion by kidney so decrease body fluids
mainly the extracellular fluids.
*the functional unit in the kidney is the nephron and each kidney has about one
million nephron.
*To increase water excretion, a diuretic has to increase Na+ secretion from blood
to nephron lumen, Or decrease Na+ reabsorption from lumen to blood.
*Natriuretic is substance increase Na+ excretion,
Saliuretic is substance increase Na+ and Cl- excretion,
Kaliuretic is substance increase K+ excretion.
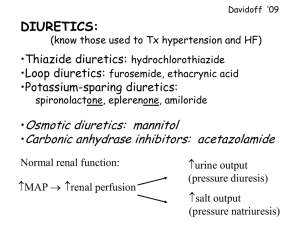
General used of diuretics:
1)treatment of all types of edema associated with congestive heart failure, liver
dysfunction or cirrhosis,
Renal failure and during pregnancy.
2)used in treatment of hypertension either alone if hypertension is mild or in
combination with antihypertensive drug if severe hypertension.
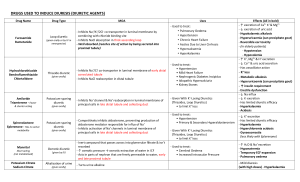
I] Classification due to site of action:
A} Agents that exert their effects in the proximal (convoluted) tubules:
Mercurial drugs, thiazides, osmotic diuretics, xanthines.
B} Agents that affect the loop of Henle (high ceiling or loop diuretics)
Mercurial drugs, thiazides, frusemide, ethacrynic acid.
C} Agents that exert their action on the distal (convoluted) tubules:
Potassium sparing diuretics (SPIRONOLACTONE), potassium excreting agents
THIAZIDES.
II] Classification duo to chemical structure
A} Water and osmotic agents (urea, mannitol).
B} Acidifying salts ( NH4Cl, NH4NO3).
C} Mercurial agents: mersalyl sodium.
D} α,β-unsaturated ketones: Ethacrynic acid.
E} Purine or xanthine diuretics: aminophylline.
F} Pyrimidines ( uracil derivatives): Aminometradin, amisometradin.
G} Sulphonamides: I] Carbonic anhydrase inhibitors:
Acetazolamide, methzolamide, dichlorophenamide.
II] Benzothiadiazine derivatives ( thiazides) :
Chlorothiazide, hydrochlorothiazide, bendrofluazide, trichlormethiazide,
benzthiazide, cyclothiazide,cyclopenthiazide, altizide, polythiazide.
III] Quinazoline derivatives:
Quinethazone, metolazone,.
IV] Phthalimidine derivatives:
Chlorothalidone.
V] Sulphamyl benzoic acid derivatives and their related
compounds:
Frusemide, clopamide, mefruside, indapamide.
H} Steroidal diuretics: Spironolactone.
G}Miscellaneous compounds: Triamterene, amiloride.
α,β-unsaturated ketones
HOOC
Cl Ethacrynic acid
O 1
3 Cl
CH2
CH3 HOOC
synthesis
Cl
Cl
O
Cl
4
O
2,3-dichloro-4-(2-methylene
butanoyl)phenoxyacetic acid
Mannich RXN
HCHO / (CH3)2NH
HOOC
AlCl3
O
(CH2)2CH3 F.C.acylation
O
-HCl
ClCl
+
(CH2)2CH3
O
Butanoyl Cl-
MOA:
it inhibit Na+ reabsorption in ascending loop of Henle, and in distal tubule and
commonly called
( Loop diuretic ), thus increase also Cl- excretion so cause systemic alkalosis.
Uses:
used in refractory edema.
Purine or xanthine diuretics
O
H 3C
O
N
NH 3
N
N
N
CH 3
NH 3
2
Aminophylline
***Assay: 1) for ethylene diamine: dissolve in water and then titrate with
standard acid and methyl orange indicator.
2) for theophylline: to the above neutral solution add Kn xss of
AgNO3, which pricipitate theophylline as insoluble silver salt
liberate equivalent amount of HNO3 titrated with st base,
indicator , or determine residual AgNO3 by st SCN-, ferric alum
aminophylline used as diuretic and bronchodilator
Sulphonamides.
1-Carbonic anhydrase inhibitors
General mechanism of action: they act mainly in proximal tubules.
they have SONH2 group which is structurally similar to carbonic acid so inhibit
carbonic anhydrase enzyme which catalyze the following process:
H2O + CO2
carbonic anhydrase
H2CO3
HCO3 + H+ enter to the tubular urine while Na+
enter the cell ( Na+ / H+ exchange)
When carbonic anhydrase is inhibited, the H+ conc. is decreased what will
decrease Na+ / H+ exchange,
Increasing Na+ excretion, decreasing its reabsorption so cause diuresis.
*** It decrease H+excretion so cause systemic acidosis that make inhibitors of
carbonic anhydrase ineffective,
So drug administration should be stopped till acid-base balance is returned.
O
O
H3 C
S
S
HN
N
NH2
O S O
NH 2
O
N
Acetazolamide
Cl
Cl O
O
S
NH2
Dichlorophenamide
Uses.1)reduces intraocular pressure so useful in treatment of glaucoma.
2) diuretic but less useful than other agents why?
(***) acetazolamide just used
for 2-3 days as after this it becomes ineffective due to compensatory mechanism
of
the kidney to overcome
systemic acidosis results
from the drug that must be stopped till acid base
balance is returned.
SAR of carbonic anhydrase inhibitors:
1) the amino group in the SO2NH2 group should be primary and free,
substitution of one or the two sulfonamide hydrogens will abolishes
activity.
2) aromatic sulfonamides are more active than aliphatic ones.
3) 1,3,4-thiadiazolesulfonamides are 100 times as active as sulfanilamide,
ex acetazolamide.
4) methylation of acetazolamide leads to methazolamide has the same
activity as acetazolamide.
5) p-carboxybenzenesulfonamide is several times more active than
sulfanilamide.
6) introduction of another SO2NH2 group will increase activity, addition of
another Cl atom will increase potency
as in dichlorophenamide.
7) if acyl group is removed from the nitrogen atom, activity is decreased.
8) highly ionized agents are more firmly bound to carbonic anhydrase
enzyme so have more diuretic activity
II] Benzothiadiazine derivatives ( thiazides) :
Cl
H2NO2S
H
N
R
O
SO2NH2
4
Cl 6 5
-H2O
H2NO2S
N
3
1 NH 2
7
8
S
O O
MOA:
Inhibit Na+ reabsorption in proximal tubule and ascending loop of Henle what
cause diuresis.
They have SO2NH2 so has certain degree of carbonic anhydrase inhibition
SAR: 1) Cl, F, CF3 in the position 6 activates the nucleus.
2) substitution on the position 5 or 8 reduces the activity.
3) free sulfamoyl group is essential for activity, removal or replacement of
one of the two hydrogens of sulfamoyl group by methyl group abolishes activity
4) free sulfamoyl group in position 7 is equal in activity to that in position
5, if in position 6 it will reduce the activity
5) substitution of ring nitrogens in position 2 or 4 will reduce the activity, but if
by lower alkyl group as methyl in the position 2, it will enhance the activity.
6) saturation of the double bond in the position 3-4 give 10 fold increase in the
activity as in hydrochlorothiazide.
7) substitution in the position 3 by hydrophobic group like alkyl, cycloalkyl,
haloalkyl and aralkyl will increase the activity, α hydrogen is essential for
activity.
H 2NO2 S
Cl
O O
S
NH
N
Chlorothiazide
H2 NO 2S
Cl
O O
S
NH
N
H
Hydrochlorothiazide
H 2NO2 S
F3 C
O
O
S
NH
N
H
Bendrof luazide
Uses: 1) oedema associated with heart failure and hepatic or renal disorders.
2) hypertension alone or with other antihypertensives.
Phthalimidine derivatives
O
1 2
NH
3
OH
O
NH4OH
O
SOCl2
O
Cl
Cl
O
O
heat
OH
Cl
Cl
OH
Chlorothalidone SO2NH2
chlorophthalide SO2Cl
SO2Cl
*3-hydroxy-3-(3--sulfamoyl-4--chlorophenyl) phthalimidine
**1-oxo-3-(3--sulphamoyl-4--chlorophenyl)-3-hydroxy-2,3-dihydro-1H-isoindole
***Assay: as in hydrochlorothiazide
**** potent, long acting, orally effective diuretic and antihypertensive.
O
Cl
SO2Cl
benzophenone2-carboxylic
acid derivative
Sulphamyl benzoic acid derivatives
COOH
O
H2NO2S
Cl
N
H
H2N
COOH
O
H2NO2S
Cl
ClO2S
Cl NH4OH
Cl
COOH
COOH
Cl
ClSO3H
Cl
Cl
NaHCO3
Frusemide
*4-chloro-N-furfuryl-5-sulfamoylanthranilic acid
**Assay: non aqueous titration as weak acid.
***MOA: highly effective saliuretic agent that has rapid diuresis in short duration of action (6-8) hours,
it acts as loop diuretic, inhibit Na+ reabsorption in loop of Henle, it promotes K+ excretion also, so it is
used with potassium supplements or pot. sparing diuretics to avoid hypokalemia.
Steroidal diuretics: Spironolactone
(STEROIDAL POTASSIUM SPARING DIURETICS)
MOA:
aldosterone stimulate Na+ reabsorption and K+ excretion so cause hypokalemia
and decrease diuresis,
Spironolactone antagonize the effects of aldosterone in the collecting duct so as
to decrease Na+ rabsorption and also decrease K+ excretion so called potassium
sparing diuretic and it has steroidal structure.
** spironolactone is metabolized to an active metabolite which is canrenone.
Miscellaneous compounds: NON STEROIDAL POTASSIUM SPARING
DIURETICS)
Triamterene
8
H2N 7 N
6
N
5
N1
Amiloride O
NH2
2
4 N3
NH2
2,4,7-triamino-6phenylpteridine
Cl
N
H2N
N
N
H
NH2
NH
NH2
3,5-diamino-N(aminoiminomethyl)-6chloropyrazine-2-carboxamide
MOA:1) act in the late distal convoluted tubule and in the early collecting duct.
2)It exerts the same action of spironolactone but without any relation to the
aldosterone.
3) it is really mild natriuretic, saliuretic and antikaliuretic.
Uses: 1) mild edema associated with congestive heart failure or liver cirrhosis.
2)not enough alone in treatment of hypertension.
3) mainly used with hydrochlorothiazide to prevent associated hypokalemia of
the latter.
 0
0