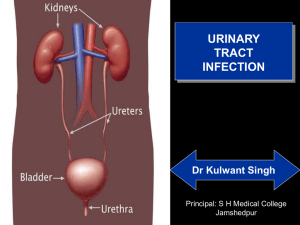
Lower Urinary Tract
advertisement

Lower Urinary Tract Outline Lower Urinary tract •Ureter •Bladder •Urethra Lower Urinary Tract Lower Urinary Tract: Several Similar morphological characteristics In spite of different embryonic origin All are lined by a special type of transitional epithelium(Urothelium)(Renal pelves,uretes,bladder and the proximal urethra) There are 3-5 layers of epithelial lining in the Ureters, while the layers in the bladder may be up to 7 layers. Lower Urinary Tract Lower Urinary Tract: There is a well developed basement membrane ,a distinct lamina propria as well a muscularis propria(detrusor muscle fibres) The Ureters are close to the uterine arteries in females and may be easily injured at surgery Lower Urinary Tract Lower Urinary Tract: The ureters insert into the bladder at an oblique angle creating an anatomic sphinteric mechanism that prevents Upward reflux of urine . The orifice of the ureter is usually at the bladder trigone which is lined by glycogenated squamous epithelium The close anatomic proximity of the female genital tract to bladder increases the incidence of spread of infection from one tract to the other. Lower Urinary Tract Ureter Congenital Anomalies •2-3% of all biopsies •Most are not clinically significant •Ureterovesical junction anomalies often predispose to VUR.( a common cause of pyelonephritis) 1. Double ureters: •Derived from a double or split ureteral bud •Associated with either double renal pelvis or with a large kidney with bifid pelvis., no significance. Lower Urinary Tract 2. Ureteroplevic junction obstruction: •Left ureters>Right •Boys>girls •Most common cause of hydronephrosis in children Lower Urinary Tract Inflammation of the ureter (Ureteritis): •Usually develops as a component of UTI Tumors of the ureter •Rare •Fibroepithelial polyps •Leimyomas •Primary malignant tumors are Transitional cell carcinomas Lower Urinary Tract Ureteral obstruction: Clinically important because it can cause pathology in the kidney. (hydroureters, hydronephrosis) •Ureteral stones •Stricture •Tumors •Blood clots •Neurogenic •Inflammatory lesions Lower Urinary Tract Urinary bladder: •Bladder diseases are usually a source of distress and discomfort. Congenital Anomal1ies 1. Diverticular: •A pouchlike evagination of the bladder •Due to a failure of development of the normal musculature or to urinary tract obstruction during fetal development. Lower Urinary Tract Congenital Diverticular: •Frequently multiple •May constitute sites of urinary stasis=> Infection and calculi formation. •May also predispose to VUR as a result of impingement on the ureters •Carcinomas may also arise within a diverticular(rare) Lower Urinary Tract Bladder Exstrophy: •Developmental failure of the anterior abdominal wall and bladder •The bladder communicates through a larger defect in the abdominal wall with the surface. •Increased risk of infection that may spread to the upper urinary tract or systemic infections. •Chronic infection often transforms the exposed mucosa to a stratified Squamous type. •Surgery corrects the situation. Bladder Exstrophy Lower Urinary Tract Vesicourethral reflux: •Common •Also clinically very important •It is a major contributor to renal infection and scarring. Especially with regards to pyelonephritis. •Caused by a shortening of the intravesical portion of the ureter.=>a more horizontal insertion of the ureters into the bladder. Lower Urinary Tract Urinary Bladder: Inflammations: Acute and Chronic Cystitis •Acute Cystitis: •Gram negative coliforms;E.Coli,Proteus,Klebsiella and Enterobacter. •Commoner in females because of the shorter urethra. Other non common causes :T.B,Candida(in immunocompromised),Chlamydia and Mycoplasma. Lower Urinary Tract Acute Cystitis cont: •Shistosomiasis is a common cause in Egypt and Sudan •Cyclophosphamide =>Hemorrhagic cystitis •Radiation of the bladder=>radiation cystitis. Morphology •Mucosal hyperemia, neutrophillic exudates. Lower Urinary Tract Chronic Cystitis: Persistence of infection leads to chronicity •Similar morphological features apart from the presence of lymphocytes in the exudates •The bladder wall shows evidence of fibrosis and in-elasticity Variants includes: Follicular cystitis(aggregation of lymphocytes into lymphoid follicles) and eosinophilic cystitis(submucosal eosinophils). Lower Urinary Tract Presentation of Cystitis: Triad of: •Frequency •Lower abdominal pain •Dysuria: usually burning pain on micturition •Cystitis may also predispose to developing acute pyelonephritis. Lower Urinary Tract Special Cystitis Interstitial Cystitis: •Etiology unknown •Painful chronic cystitis •Mast cells in the bladder wall. •Must rule out carcinoma Malacoplakia •Related to chronic infection with E.coli or immunosuppresion. Lower Urinary Tract Bladder Malacoplakia: It represents a bladder inflammatory reaction, Gross: soft, yellow,raised mucosal plaques. Histology: Foamy macrophages with occasional giant cells. There are interspersed lymphocytes. •Michaelis- Gutman bodies are seen. These are laminated mineralized concretions resulting from deposition of calcium in enlarged lysosomes. Mchaelis –Gutman bodies Lower Urinary Tract Neoplasms: •95% of bladder tumors are of epithelial origin •Mesenchymal tumors account for the rest. •Most Epithelial are composed of transitional epithelium and are known as transitional tumors or Urothelial tumors. Benign lesion, known as Papillomas are rare. •Transitional Cell Carcinomas: •May be seen anywhere that is lined by urethelium(renal pelvis to the distal urethra) Lower Urinary Tract Transitional cell carcinoma of the Bladder: Risk factors: •Smoking •B-Naphtylamine •Chronic Cystitis •Schistosomiasis •Cyclophosphamide Carcinoma of the Bladder :Commoner in male with a 3:1 ratio. • Presents with painless haematuria • May also cause CVA pain • Recurrence after surgery is common • Prognosis depends on tumor grade, differentiation and depth of invasion Carcinoma of the Bladder Morphology cont: • Flat • Papillary • Low grade • High grade. Low grade tumors are papillary and are usually not invasive tumors. Recurrence after surgery is common . Carcinoma of the Bladder Morphology Cont’D. • High grade tumor: Usually papillary, but may be flat. They occupy large area of the bladder and have a shaggier, necrotic appearance. • Higher grade tumor would have evidence of distal metastasis. Low Grade Urothelial carcinoma, orderly arrangement of thickened epithelium High Grade Papillary Carcinoma: Marked Cytologic atypia with pleocytosis Papillary Tumor Lower Urinary Tract Neoplasms: Other Carcinomas: •Squamous cell carcinoma •Mesenchymal tumors •Secondary tumors •Squamous cell carcinoma is seen with schistosomiasis.(endemic zones Egypt and sudan)