Prevention and Treatment of Infection in Knee and Hip Arthroplasty
advertisement

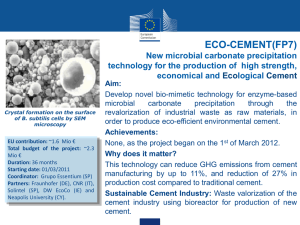
Prevention and Management of Infected Joint Replacements Jim Nairus, MD New England Baptist Hospital Financial Disclosure I have received no funding from any sources related to topics of this discussion Three Major Sources of Infection Patient Surgical Team Hospital Environment Incidence With Prophylaxis 0.5% to 2% with primary joint replacements 3-5% after revision joint replacements Incidence lowered with perioperative antibiotics Controversial: Antibiotic Cement, UV lights, space suits, laminar flow, less traffic in operating room Ramifications Most devastating complication High cost to hospital and patient $15,000 to $30,000 loss to hospital per patient Barrack CORR 1996 3 mos to 1 year out of life Very debilitating Organisms 75% caused by staph Staph epidermidis (non-aureus) most common, followed by staph aureus and then MRSA 10% strep usually viridens 10% gram negatives Not as bad as previously thought 5% Others Optimizing Patient Lose weight Obesity with increased infection rate due to longer surgical time, greater surgical dissection, and high calorie poor nutrition diet Namba et al in 2005 showed obese patients 6.7% higher risk of infection Control perioperative blood sugar in diabetics Stop TNF Alpha Antagonists one dosing cycle prior to surgery Optimizing Patient Pre-operative staph screening Molecular DNA studies have shown majority of infecting strains are part of resident’s nasal flora PCR test for staph aureus and MRSA Nasal Bactroban if nares positive for MSSA or MRSA Rao in 2008 showed reduced infections from 2.6% to 1.5% Vancomycin and isolation precautions for MRSA Antibiotic Prophylaxis The Most Important Factor in Lowering Infections Charnley lowered infection rate from 7% to 0.5% Want highest blood concentration of antibiotic at time of incision Should be completed within 20 to 60 minutes prior to incision Should be repeated if surgery lasts more than 2 hours or when patient loses more that 30% of blood volume (1.5L) Should be continued for 24 hours post-op No evidence of efficacy beyond 24 hours Kefzol Considered by many to be best Bactericidal Excellent tissue penetration, rapid (within minutes) and good bioavailability Broad spectrum (active against all skin flora including gram negatives) Disadvantage: does not cover MRSA or MRSE Patients weighing greater than 80 kg should get 2 gr Vancomycin Should be administered to patients colonized with MRSA or MRSE Not best for MSSA Disadvantage: needs to be administered over 1 to 1.5 hours and is oftentimes not timed correctly Does not cover any gram negatives Probably best for revisions JBJS ’04 – 30% of pos revision cultures resistant to Kefzol Penicillin Allergic Patients 5% of individuals allergic to penicillin are allergic to cephalsporins (Kefzol) Can give test dose of Kefzol Especially if allergy is rash Probably not with anaphylaxis or swelling Should never give Clindamycin Bacterostatic only Consider Vancomycn Kefzol and Vancomycin Covers almost all organisms Controversial because of development of resistance especially to Vancomycin Consider in high risk patients Obesity, revisions, anemia, diabetes, smokers, immunocompromised, prior surgeries Antibiotic Impregnated Cement Advantages: Lower incidence of infection Norwegian Arthroplasty Registry (10,611 THR’s) and Swedish Joint Registry (92,675 THR’s) Disadvantages Higher incidence resistant organisms (Swedish Registry, Kendall JArthrop ’96) Structural support (can use up to 2g per 40g bag of cement) Cost Cost Bag of cement approximately $60 Tobramycin cement as high as $300 Usually use two bags of cement Adding Vancomycin to cement only costs extra $10 to $20 Unfortunately have to mix at time of surgery Costs time and ?sterility Chiu et al, JBJS 2001 Prospective randomized study (340 TKR’s) 0 infections in atbx cement group and 5 (3.1%) infections in non-atbx group Chiu et al, JBJS 2002 showed 5 cases of infection were all in diabetics Personal Preference Tobramycin cement in all revisions not replanted for infection Vancomycin cement in all replant TJR’s after infection Tobramycin cement in TJR’s in diabetics, rheumatoid’s, UTI’s, and immunocompromised Non-antibiotic cement in all others Operating Room Environment Multiple studies show contamination from people present in OR (surgical team, anesthesia team, patient) People shed from 1,000 to 10,000 bacteria per minute Bacterial contamination not shown to be prevented by surgical gowns although switching from cloth to plastic gowns lessened bacterial shed Laminar Flow and Ventilated Suits Swedish registry > 150,000 TJR’s No decrease risk for infection with ventilated suits or laminar flow as long as prophylactic antibiotics used New Zealand Registry showed higher incidence of infection with both laminar flow and space suits Operating Room Ritter has shown that number of bacteria cultured at surgical site and on surgical table directly proportional to number of people in operating room Number of times door opens directly proportional to number of bacteria present Avoid Overuse of Antibiotics Wound drainage Temperatures Erythema Can mask deep infection where antibiotics are not helpful and change classification from acute to chronic infection Persistent Wound Drainage Established Knee Infections 17-50% have persistent wound drainage beyond 3-4 days Krakow ’93 J Arthroplasty 8/597 (1.3%) – Persistent Drainage All taken back to OR Average 12.5 days post-op Two (25%) had positive deep cultures None developed clinical infection Conclusions: Persistent drainage = impending infection Aggressive operative treatment recommended Etiology ½ infections introduced at the time of surgery or immediately post-op 1/3 are hematogenous Remainder not sure Classification All based on the duration of signs and symptoms Acute Post-operative Within 4 weeks of surgery Hematogenous Within 4 weeks of symptoms Chronic More than 4 weeks from surgery or symptoms Diagnosis Labs X-rays Bone scan Aspiration Intra-op Frozen section Intra-op culture Labs CBC Rarely positive Sed rate Very sensitive but not specific Usually > 35 Takes 1 yr to return to normal after surgery C-reactive Protein Peaks 48 hrs post-op and declines to normal 2-3 weeks later Used to monitor treatment Can be elevated with CAD Plain Radiographs Only positive with osteolysis in chronic infections Bone scan Positive with aseptic loosening and infection Need tagged WBC scan to be more specific May not be reliable Aspiration False positive in 015% False negative when organisms have poor vitality Should be selective and use with labs Get cell count with it Cell Count Cut-off value shown to be 1,100 to 3,000 WBC Lower glucose than blood glucose Differential with 60-80% Neutrophils Definitely not the 50,000 WBC for native knee Higher value for recently operated on knee With these parameters shown to be very good test Intra-op Frozen Section Intra-op Gram stain Poor sensitivity and poor predictive value Morgan JBJS 2009 Can get false positives from debris Using 5 PMN’s/PHPF 84% sensitive and 96% specific Lonner suggests 10 PMN’s/PHPF Should always use when replanting after infection or when highly suspicious Intra-op Cultures Gold standard Send 5 samples (2/5 for positive) 6-13% false positive Correlate with pathology Treatment Based on Classification Need to know duration of symptoms Need to do in a timely fashion Acute Early Post-op Surgical debridement with change of anything easily removable Then treat with at least 6 wks of IV antibiotics 10 to 50% success rate No role for arthroscopy Late Chronic Resection with or without antibiotic cement spacer Staged revision with frozen section after normal labs and aspiration (80% to 96% successful) Recurrence rate 10% Use antibiotic cement in knees 1 stage exchange not as successful 58% to 83% Acute Hematogenous Surgical debridement and change easily removable parts and 6 wks IV atbx Surgical emergency 80% success rate if done within one week of onset of symptoms 10 to 50% success rate if done within four weeks of symptoms Surgical Debridement and Component Retention Results improve with urgency of procedure Need one-year or lifetime oral suppressive antibiotics after 6 wks IV antibiotics 1 yr failure rate 54% 2 yr failure rate 69% Girldestone Resection Arthroplasty For Poor medical candidates Those unable to comply with post-op rehab Immunosuppressed Excellent success rate Pain-free and some younger patients can ambulate with assistive devices Arthrodesis Instead of resection arthroplasty in knee Wichita Nail, plates, or external fixator PROSTALAC for Hips Allows better patient mobilization Control over limb length discrepancy Easier second surgery 90-97% success rate Cultures more likely to be positive if infection still present Longer O.R. time My Results 28 PROSTALAC’s 4 cement coated Austin Moore, 24 Depuy 2 failures for recurrent infection Both in same patient 3 failures for dislocation or failure of acetabular component 7 reimplantations after Girdlestones 2 late dislocations No infections Knee Antibiotic Cement Spacer Cement spacer or PROSTALAC Should have at least 3g vanco powder per 40g bag of cement Tobramycin cement not good enough PROSTALAC in KNEES Advantages Able to mobilize with less scarring Easier second surgery Disadvantages Components do not fit well Some studies have shown longer persistent drainage Thank You