SVC Syndrome
advertisement

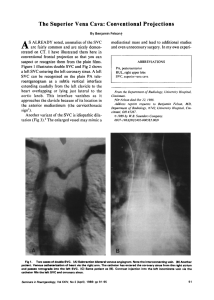
SVC Syndrome Sung Chul Hwang, M.D. Dept. of Pulmonary and Critical Care Medicine Ajou University School of Medicine Introduction • A medical entity where compression of SVC by various causes brings clinical symptoms and signs of facial, upper body edema, formation of collateral circulations, and causes cyanosis and dyspnea • 1757 William Hunter • Malignancy– most common • Fibrosing mediastinitis Etiology 1) 2) 3) 4) 5) 6) Malignancy 66/86 (YUMC) Mediastinal fibrosis 2 Thrombosis 1 Inflammatory 0 Radiation fibrosis 0 Unknown 31 Symptoms and Signs 1) 2) 3) 4) 5) 6) 7) 8) Suffusion Dyspnea Cough Pain Neck Vein Distention Venous engorgement Edema Cyanosis Diagnosis • • • • History Physical Examination X-rays and CT Scans Tissue Diagnosis Diagnostic Methods • • • • • • Bronchoscopy Lymph node biopsy Sputum cytology Pleural biopsy Thoracotomy Bone marrow biopsy Treatment of SVC Syndrome • Radiotherapy • Chemotherapy : Small cell Ca, Lymphoma • Diuretics • Corticosteroid • Endovascular Stents Prognosis • • • • Poor Inoperable Not treated : 3- 4 weeks If treated : about 10 months SVC Invasion by Lung Cancer SVC Invasion by Lung Cancer SVC Syndrome and the stents Lymphoma with SVC SD F/26 DOE for 2 months Lymphoma with SVC SD Lymphoma with SVC SD Fibrosing Mediastinitis • 20- 40 years • Cough, Dyspnea, or Hemoptysis • Most common cause of Benign SVC syndrome • Almost always remote Histoplasmosis • Plain X-rays may be normal or only minimal changes • Partially calcified Mass on CT is diagnostic Fibrosing Mediastinitis F/29 with SVC Syndrome by Histoplasmosis Fibrosing Mediastinitis F/29 with SVC Syndrome by Old Histoplasmosis