Emergency Childbirth - Silver Cross Emergency Medical Services
advertisement

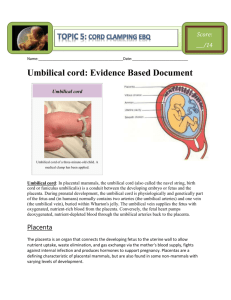
Silver Cross EMS EMD CE November 2011 This presentation is set up as if you were on scene, assisting with a delivery. You will go over the questions to ask, things to look for, possible complications and assisting with a delivery. Hopefully this will help you picture the scene and better understand why you are asking certain questions and give more effective instructions. Your EMDPRS will be updated soon, with some new information and pre-arrival instructions. Childbirth is a normal, natural part of life. Your part of the process involves helping, guiding, and supporting the infant as it is born. After the birth, you should ensure the infant is breathing adequately and being kept warm. Two indicators of an impending birth: Frequency of the contractions Crowning As you prepare to assist the mother in the delivery, keep two things in mind: Calm the woman: Delivery is a natural process. Calm yourself: You are there to help or coach. This lecture has some graphic pictures of childbirth and emergency delivery. There will also be an option to click on a link to view an actual childbirth video. Viewer discretion advised. The external opening is called the birth canal (vagina). The developing infant (fetus) is encased in an amniotic sac for support and floats in amniotic fluid. The placenta is the organ of exchange between mother and child. The umbilical cord connects the baby to placenta. Opening of the Uterus is the Cervix. •Placenta – develops early in pregnancy & performs important functions Exchanges respiratory gases – Transports nutrients from mother to fetus – Excretes waste – Transfers heat – Active endocrine gland produces several important hormones – Attached by umbilical cord •Amniotic pregnancy sac – develops early in Consists of membranes that surround & protect developing fetus – Amniotic fluid cushions fetus & provides stable environment – – Umbilical cord – attaches fetus to placenta • Contains one vein & two arteries – Vessels in umbilical cord similar to pulmonary circulation – • Arteries carry deoxygenated blood • Veins carry oxygenated blood Newborn cord is about two feet long – First stage of labor: the pregnant woman’s body prepares for birth Characterized by these conditions: Initial contractions occur. The bag of waters breaks. The bloody show occurs. (loss of protective mucous plug from cervix) The infant’s head does not appear during contractions. This is the longest stage but is shorter for each pregnancy. Second stage of labor: the birth of the infant Contractions are close together, 2-3 minutes apart. Mother will have the urge to push. You will see the infant’s head crowning during contractions. There is no time for transport, you will need to assist with delivery. Third stage of labor: delivery of the placenta (afterbirth) Mom will start to have contractions again and will usually delivery the placenta within 20-30 minutes. Your focus should be caring for mom and newborn. Is this the woman’s first pregnancy? Has the woman experienced a bloody show? A woman experiencing her first labor will usually have more time to reach the hospital. Loss of mucous plug. Has the bag of waters broken? The bag of waters usually breaks toward the end of the first stage of labor. How frequent are the contractions? Contractions less than 2 minutes apart usually indicate that delivery will occur very soon. Contractions are timed from the start of one to the start of the next. Does the woman feel an urge to move her bowels? When the infant’s head is in the birth canal, it presses against the rectum. Do not allow her to go to the toilet. Is the infant’s head crowning? Head is visible in the birth canal Is transportation available? Is the ambulance responding? How far is it to the hospital? Will bad weather, a natural disaster, or traffic prevent prompt arrival of transportation? ? What additional information do you want to know? You will not be able to maintain sterile conditions. Attempt to be as clean as possible. Wash your hands thoroughly. If you do not have a sterile delivery kit, use household items to prepare for delivery. Use shoestrings or strips of cloth to tie the cord. Have plenty of clean towels ready. There will be lots of fluids, so protect yourself. Place the patient on a firm surface that is padded with blankets, folded sheets, or towels. Elevate the woman’s hips 2" to 4" with pillows and blankets. Place the woman on her back with knees bent and feet flat on the surface beneath her. Remove clothing below the waist. In a normal birth: The infant will turn to its side by itself after the head emerges. The rest of the body will be delivered spontaneously. The infant will be wet and slippery. Keep the infant’s head at about the level of the woman’s vagina. Encourage the mother to breath deeply between contractions and push with contractions. • • • • • • • Support head with gentle pressure Check and see if cord is wrapped around baby’s neck— attempt to loosen (more on that later) Apply gentle downward pressure on shoulder & head After anterior shoulder has delivered, apply gentle upward pressure. Once shoulders are out the rest of body will follow quickly. Suction or wipe out mouth & nostrils (in that order) when head appears Once delivered, stimulate infant if it does not breathe (info to follow) Put two clamps on umbilical cord & cut 6 inches from navel between clamps, after the cord stops pulsating Follow this link to a childbirth video, starting with crowning and ending with stimulation of the infant and awaiting the afterbirth. This baby had Nuchal Cord. http://www.youtube.com/watch?v=80T89vBR_k •During first stage of labor amniotic sac usually breaks, expelling amniotic fluid • If sac is still covering infant’s head when head appears, use a finger to pierce sac •Very tough membrane •Note color & character of amniotic fluid • Fluid can be clear or straw-colored (which is normal) • Tainted, discolored, thick or “pea soup-like” (which indicates meconium staining or a bad intra-uterine infection) •Baby could be in distress • • • • • • Once head delivers, have mother to stop pushing so you can check to see if the cord is wrapped around infant’s neck If cord looks like it is wrapped tightly, you will need to loosen it Gently slip cord over baby’s head by placing two fingers under cord at back of neck Bring cord over shoulders & head Cord is durable, but it can tear if handled roughly so don’t use excessive force Too tight to loosen, clamp cord in two places two inches apart and cut cord between clamps • • • • • • After the baby is out, remember to keep baby level with birth canal until the cord is clamped and cut Position infant on it’s side for drainage Re-suction or wipe out the baby’s mouth & nostrils Dry & wrap baby in a warm blanket — cover its head If baby is not breathing, try to stimulate it by gently but vigorously rubbing the infant’s back with you fingertips or flick the soles of it’s feet If no response • begin CPR CPR technique for the infant that is not breathing, after stimulation Place infant on a firm, flat surface Find compression site which is just below nipple line on middle or lower third of sternum Wrap your hands around upper abdomen with your thumbs on compression site Use your thumbs to deliver gentle pressure against sternum, pressing ½ to ¾ inch into chest at rate of 100 per minute 30:2 compressions to breaths Continue to observe the mother and infant and keep both warm. Bleeding should stop after placenta delivers. Observe mother for excessive bleeding and treat for shock If baby is doing well and mother wants to breastfeed, this will help slow bleeding down by contracting uterus Cord presentation Limb presentation Breech (buttocks or feet) Shoulder Dystocia (stuck at shoulders) Premature or Stillborn Multiples Drug or alcohol abuse Underlying medical problems with mother or child Can your questioning help identify possible problems and better prepare responders? Most can not be delivered safely in the field. Elevate mother’s hips to relieve pressure on birth canal and advise her not to push. Have her focus on her breathing and wait for responders. Any bleeding during pregnancy could be the sign of a serious problem Ectopic Pregnancy (outside uterus) Miscarriage Placenta problems Uterus rupture • • • Some women develop diabetes during pregnancy (Gestational Diabetes) Diabetics can have problems maintaining their blood sugar levels during pregnancy Supine hypotensive syndrome occurs when increased weight of uterus compresses inferior vena cava while a patient is on her back • Position mother on her left side to avoid this • Variety of signs and symptoms including: Hypertension – Abnormal weight gain – Edema – Headache – Protein in the urine – Epigastric pain – • If untreated, preeclampsia can progress to eclampsia •Eclampsia, also called toxemia, most serious manifestation of hypertensive disorders of pregnancy • Characterized by grand mal seizures • Often preceded by visual disturbances such as flashing lights or spots before the eyes •Eclampsia patients often experience swelling of hands & feet & markedly elevated blood pressure • If eclampsia develops, death of mother & fetus frequently results • Treat by lying mother on her side, maintaining airway and monitor until help arrives Childbirth is a natural process with a small percentage of complications. Follow your scripted protocol for imminent births.