AnatomyHSR _2013
advertisement

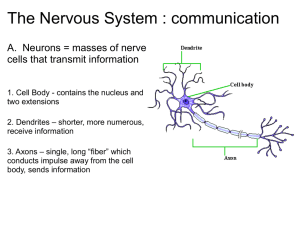
Anatomy for the Anesthetist Marianne Cosgrove, CRNA, DNAP, APRN Components of the Respiratory System The nose The pharynx The larynx The trachea The bronchi The lungs Conducting Portion of the Respiratory System nasal cavities oral cavity pharynx larynx trachea bronchial tree Lining of the Respiratory Tract Nonciliated stratified squamous epithelium – anterior nose, oropharynx, laryngopharynx Ciliated pseudostratified squamous epithelium – posterior nose, nasopharynx, laryngeal mucosa above cords Ciliated pseudostratified columnar epithelium – larynx below cords, trachea, bronchiolar tree Nonciliated cuboidal epithelium – terminals and respiratory bronchioles The Nose and Sinuses The external nose The internal nose – bony septum – nasal turbinates – posterior nares The paranasal sinuses – – – – maxillary frontal sphenoid ethmoid Functions of the Nose Warms inspired air Humidifies air Cleans inhaled air Organ of olfaction Resonator for speech The Pharynx …a musculomembranous tube extending from the undersurface of the skull to the level of C6 and lower border of the cricoid cartilage where it is continuous with the esophagus. The Pharynx Divisions – nasopharynx – oropharynx – laryngopharynx Innervation – sensory • via glossopharyngeal (cranial nerve IX) – motor • via vagus (cranial nerve X) Primary motor function – swallowing Divisions of the Pharynx nasopharynx – Behind posterior nares and above soft palate oropharynx – Extends from the soft palate to the base of the tongue Divisions of the Pharynx cont’d laryngopharynx – Extends from the base of the tongue to the opening of the esophagus – Contains the landmarks for endotracheal intubation: epiglottis, aryepiglottic folds, arytenoid cartilages Landmarks for Intubation Esophagus upper 1/3 striated muscle – voluntary – airway protection against regurgitation via the cricopharyngeus muscle (A.K.A. upper esophageal sphincter (UES)) • motor innervation via the RLN lower 2/3rds – involuntary; tone/contraction under ANS control distal 3-5 cm lower esophageal sphincter (LES) – A functional structure; may be manually opened with ~ 18 cm H2O pressure Classifications of the Airway Mallampati Cormack-Lehane The Larynx …consists structurally of a framework of articulating cartilages linked together by ligaments which move in relation to each other by the action of laryngeal muscles. The Larynx Location – adult • anterior neck at the level of C4-6 – child • anterior neck at the level of C3-5 The Larynx Blood supply – Arterial • subclavian artery to inferior thyroid artery to inferior laryngeal artery – Venous • inferior laryngeal vein to brachiocephalic vein to SVC The Laryngeal Cartilages Singular cartilages – thyroid – cricoid – epiglottis Paired cartilages – arytenoids – corniculates – cuneiforms Thyroid Cartilage Largest cartilage – Two broad sheets of cartilage which unite in a V shape anteriorly to form the “Adam’s Apple” – Attached to the hyoid bone by the thyrohyoid membrane – Attached to the cricoid cartilage by the cricothyroid membrane – Provides the anterior attachment for the vocal cords Cricoid Cartilage Consists of the only complete ring in the larynx which broadens into a plate like structure on the posterior aspect; A.K.A. “The Signet Ring Cartilage” forms the inferior and posterior borders of the larynx Is the narrowest portion of the pediatric airway Epiglottis Leaf like, elastic – Projects obliquely upward behind the tongue and in front of the entrance to the larynx • Functions to cover the glottic opening to prevent entrance of solids and liquids into the airway during swallowing Attached to the posterior surface of the thyroid cartilage above the vocal cords First cartilage encountered during laryngoscopy Arytenoid Cartilages Pyramidal in shape; sit on cricoid cartilage – Each has a muscular process which is the insertion of the posterior and lateral cricoarytenoids – Each has a vocal process which is the posterior attachment of the vocal cords Corniculate Cartilages Cone shaped structures situated in posterior part of the aryepiglottic folds Each is attached to the apex of an arytenoid cartilage Cuneiform Cartilages Elongated structures located slightly posterior to the corniculates at the base of the epiglottis C3 C4 C6 The Laryngeal Cartilages Netter, Plate 71 Other Laryngeal Structures Aryepiglottic folds Ventricular folds (false vocal cords) Vocal folds (true vocal cords) The glottis – *The rima glottis is the narrowest portion of the adult airway cricothyroid membrane – palpated between the lower border of the thyroid cartilage and the cricoid ring – allows for easy surgical access to the airway via cricothyrotomy in “can’t ventilate, can’t intubate” scenario Muscles of the Larynx muscle action effect Posterior cricoarytenoids (2) Rotate arytenoids outward ABduction (widens rima) Lateral cricoarytenoids (2) Rotate arytenoids inward ADduction (approximates vocal cords) Transverse arytenoid (1) Approximate arytenoids ADduction (approximates vocal cords) Thyroarytenoids (2) Draw arytenoids forward Relaxes and shortens cords Cricothyroids (2) Draw up arch of cricoid and tilt lamina back Tenses and elongates cords Posterior, Lateral Views of Laryngeal Muscles Netter, Plate 72 Lateral Dissection of Laryngeal Muscles Netter, Plate 72 Superior View of Laryngeal Muscles Netter, Plate 73 Action of Posterior and Lateral Cricoarytenoids Netter, Plate 73 Action of Cricothyroid Muscles Netter, Plate 73 Action of Transverse Arytenoid, Thyroarytenoid Muscles Netter, Plate 73 Innervation of the Larynx Superior laryngeal nerve – A branch of the vagus nerve; contains internal and external branches • Internal branch supplies sensory innervation above the vocal cords *stimulation may precipitate laryngospasm • External branch supplies motor innervation to the cricothyroid muscles Innervation of the Larynx Recurrent laryngeal nerve – A branch of the vagus nerve – Supplies motor innervation to all muscles of the larynx except the cricothyroid muscles – Supplies sensory innervation to the larynx below the vocal cords – May be damaged during thyroid/parathyroid surgery Damage to the Recurrent Laryngeal Nerve Unilateral transection = hoarseness Bilateral damage from ischemia = complete airway obstruction from laryngospastic cords Bilateral transection = flaccid vocal cords – May have some passage of air Laryngeal Nerves Netter, Plate 74 The Trachea Cartilaginous and membranous tube extending from the vocal cords to the carina to form the right and the left mainstem bronchi Lies anterior to the esophagus and is protected anteriorly with cartilaginous rings Posterior wall is membranous The carina lies at the level of T5 Airway Measurements female Incisors to vocal 10-14 cm cords male 12-16 cm Incisors to carina 26-28 cm 24-26 cm The Bronchi Mainstem (A.K.A primary bronchus) – Right • Shorter, wider, and less acute angle off trachea – In adults, forms a 25 degree angle – In children less than 3 years old, forms a 50 degree angle • Divides into 3 lobar branches • Inhaled foreign bodies are more likely to enter the R mainstem bronchus The Bronchi Mainstem (A.K.A primary bronchus) – Left • Longer, narrower, more horizontal than right –In adults and children, forms a 40-60 degree angle off trachea • Divides into two lobar branches The Tracheobronchial Tree, Respiratory Bronchioles, and Alveoli Continued branching produces: – Segmental bronchi – Small bronchi – Bronchioles – Terminal bronchioles – Respiratory lobules The Terminal Bronchioles The tracheobronchial tree ends at the 16th level from the trachea at the level of the terminal bronchioles Diameter is <1 mm, cilia disappears, cartilage is absent This marks the end of anatomic dead space Anatomic Dead Space Equal to approximately 1cc/lb in both adults and children Examples: – 70 Kg pt = 155 lbs Approximate anatomic dead space = 155 cc - 4 kg infant = 9 lbs Approximate anatomic dead space = 9 cc The Respiratory Lobule Comprised of: – respiratory bronchiole – alveolar duct – alveolus (air sac) The Respiratory Bronchiole Where actual respiratory exchange begins Muscle layer of bronchial tree is thickest here (relatively speaking) – Forms a thin band around the openings of the alveolar ducts – No muscle is found beyond this point Classification of airways by order of branching Common name Generation of airway Trachea 0 Main bronchi 1 Lobar bronchi 2-3 Segmental bronchi 4 Small bronchi 5-11 Bronchioles, terminal bronchioles 12-16 Respiratory bronchioles 17-19 Alveolar ducts 20-22 Alveolar sacs 23* Trachea and Major Bronchi The Lungs Lie free in the pleural cavity attached only at the hilum – The bronchi, major vessels, and lymphatics enter and leave here Each lung has a concave base – Rests upon the diaphragm Each lung has an apex The Right Lung Three lobes – Right – Middle – Lower Broader, shorter than the left lung due to elevation of the diaphragm from the liver – The right apex extends further above the clavicle than the left The Left Lung Two lobes – Upper – Lower Smaller than the right due to the position of the heart The Thoracic Cavity Three divisions separated from each other by partitions of pleura – Pleural space • Contains the lungs – Pericardial space • Contains the heart, pericardium – Mediastinal space • Contains the major vessels, lymphatics The Bronchial Circulation Feeds the parenchyma of lung Venous return to the pulmonic vein – Accounts for a normal 1-3% shunt (deoxygenated blood mixing with arterial blood) Not to be confused with pulmonary circulation – Where respiration occurs Shunt vs. Dead Space Shunt – perfusion without aeration Dead space – aeration without perfusion • A.K.A. an area of bi-directional air flow The Pleura A double layered serous membrane – Parietal • Lines the entire thoracic cavity, inner surface of ribs, superior surface of diaphragm – Visceral • Adheres to the surface of each lung – The pleural space is a potential space between the pleura • A small amount of serous fluid is present Muscles of respiration diaphragm – responsible for 70% of tidal volume accessory muscles of respiration: inspiration expiration sternocleidomastoid scalenes pectoralis major pectoralis minor serratus anterior serratus posterior superior upper iliocostalis external oblique internal oblique rectus abdominus lower iliocostalis lower longissimus serratus posterior inferior Cardiac Anatomy Coronary Arteries Other Zones of Anesthetic Interest… Major Nerve Plexuses A nerve plexus is a network of intersecting nerves which combine sets of spinal nerves that serve the same area of the body into one large grouped nerve Cervical plexus (C1-C5) A plexus of the ventral rami of the first four cervical nerves –Branches: • Lesser occipital nerve (C2) • Greater auricular nerve(C2,3) • Transverse cervical nerve (C2,3) • Supraclavicular nerves (C3-4) Supplies the skin behind the ear, at the angle of the jaw, in the anterior and lateral triangles of the neck to shoulder and below the clavicle Cervical Plexus, cont’d Branches, cont’d –Muscular • Ansa cervicalis • Hypoglosssal • Thyrohyoid, genohyoid Innervate the rhomboids, serratus anterior, SCM, trapezius, levator scapulae, and scalenus medius Cervical Plexus, cont’d –Communicating • From the SNS (superior cervical sympathetic ganglion) –C1 communicates with hypoglossal »supplies geniohyoid and thyrohyoid –C2 and C3 form ansa hypoglossi »supplies sternohyoid, sternothyroid, and omohyoid muscles Cervical Plexus, cont’d –Mixed (sensory, motor, and sympathetic) –Phrenic nerve (C5) diaphragm Cervical plexus contributes to brachial plexus The Brachial Plexus Supplies the upper limb with sensory and motor innervation A branching network of nerves derived from the anterior (ventral) rami (roots) of spinal nerves C5, 6, 7, 8, and T1 Brachial Plexus Divisions Roots (Randy) – C5-T1 Trunks (Travis) – Upper, middle, lower Divisions (Drinks) – Anterior, posterior Cords (Coffee) – Lateral, medial, posterior Branches (Black) The Brachial Plexus clavicle Distribution of terminal nerves cords lateral branches musculocutaneous median posterior axillary radial medial median ulnar innervation to UE flexors (m) lateral aspect forearm from elbow to wrist (s); *most difficult to block medial aspect forearm (s) see below shoulder (m,s) UE extensors (m) thumb, 2nd finger, inner medial 3rd finger (s) dorsal-distal half 2nd, 3rd fingers; medial ½ 4th finger (s) ventral-thumb, 2nd, 3rd, and ½ of 4th finger (s) 4th, 5th fingers, lateral hand (s) Brachial Plexus Block Four approaches: 1) Interscalene - Trunks emerge between anterior and middle scalenes; proximity of RLN, stellate ganglion, phrenic nerve, and vertebral artery predisposes to high rates of incidental blockade or intravascular injection 2) Supraclavicular (AKA subclavian) - Plexus is compacted here; provides excellent blockade; high incidence of pneumothorax (1-6%) 3) Infraclavicular - Risk for pneumo, hemo, chylo (L sided) thorax 4) Axillary - Remember the musculocutaneous nerve! 1) Visit www.nysora.com Celiac (solar) Plexus Formed (in part) by the greater and lesser splanchnic nerves of both sides, and also parts of the right vagus nerve includes a number of smaller plexuses which supply viscera: – – – – – – – – – hepatic splenic gastric pancreatic suprarenal renal testicular/ovarian superior mesenteric plexus inferior mesenteric plexus Lumbosacral plexus Lumbar plexus (T12-L4) – Main branches • iliohypogastric • ilioinguinal nerve • genitofemoral nerve – Dorsal divisions • lateral femoral cutaneous • femoral nerve adductors of hip, extensors of knee, and skin over medial surfaces of thigh and leg – saphenous is main branch – Ventral divisions. • obturator nerve adductors of hip and skin over medial surface of thigh • accessory obturator nerve Lumbar plexus, cont’d Sacral plexus (L4-S4) gluteal nerves adductors and extensors of hip and skin over posterior surface of thigh sciatic nerve (L4-S3) 2 nerves contained within a sheath common peroneal tibial – flexors of knee and ankle, flexors and extensors of toes, and skin over anterior and posterior surfaces of leg and foot – posterior and medial cutaneous nerve skin over medial surface of leg – pudendal nerve (S2-4) Sacral Plexus The Great Veins of the Neck Internal jugular – Right IJ best for cannulation and passage of a PA catheter External jugular – Beware of the large valve at the junction of the EJ and the subclavian Anterior jugular Subclavian The Great Veins of the Neck The Thoracic Duct Aortic Arch Brachiocephalic=Innominate The Antecubital Fossa The Circle of Willis …an anastomosis of the internal carotids and the vertebral arteries which is found at the base of the brain. All cerebral arteries are derived from this anastomosis. This circle is directly responsible for cerebral perfusion. During carotid X-clamping, collateral flow to the circle is via the contralateral carotid and the vertebro-basilar system. Cerebral Perfusion Pressure CPP = MAP - ICP or CVP, whichever is higher The Circle of Willis CSF circulation CSF secreted by choroid plexus to Lateral ventricles 1 & 2 to Foramen of Munro to 3rd ventricle to Aqueduct of Sylvius to 4th ventricle to Foramina of Luschka and Magendie to Subarachnoid space to Reabsorption by arachnoid villi The Cranial Nerves …with regard to their regions of innervation, are nerves of the head. They spread through the head-neck region, except for the parasympathetic portions of the vagus nerve which pass to the abdominal organs. Cranial Nerves I-VI Cranial nerves Type I. Olfactory S smell II. Optic S sight III. Oculomotor M eye movement, pupil constriction IV. Trochlear M eye movement V. Trigeminal B chewing, great sensory of face M eye movement (three branches) ophthalmic (S), maxillary (S), mandibular (M & S) VI. Abducens Function Cranial nerves VII-XII Cranial nerves Type Function VII. Facial B taste, great motor of the face S hearing, balance (five branches) temporal, zygomatic, buccal, mandibular, cervical VIII. Acoustic (A.K.A. vestibulocochlear) IX. B Glossopharyngeal swallowing, afferent carotid body and sinus X. Vagus B “Great Wanderer” afferent and efferent M larynx and pharynx tongue (branches: superior laryngeal and recurrent laryngeal nerves may be injured during intubation) XI. Accessory (A.K.A. spinal accessory) XII. Hypoglossal (may be injured during intubation) M The Spine Largest interspace is L5-S1 (A.K.A. Taylor’s space) Spinal cord Extends from the foramen magnum to the level of L1 (adults), L3 (children) – Terminates to conus medullaris and filum terminale • lower spinal nerves form the cauda equina – “Tuffier’s line” – the plane which crosses the iliac crests bilaterally • Approximately the L4 level in most individuals • Cord may extend below the L1 level in obese pts • Conus is at approximately L3 in children Tuffier’s Line ( ~T7) Spinal Cord termination Blood supply • Derived from a single anterior and paired posterior spinal arteries –Anterior spinal artery »formed from the vertebral artery »supplies anterior 2/3rds of the cord –Posterior spinal arteries »Arise from cerebellar artery Additional blood supply to the cord Intercostals (thorax) Lumbar arteries (abdomen) Artery of Adamkiewicz (great ventral radicular artery, arteria radicularis magna) – arises from the aorta – unilateral—usually from the L side – provides the major blood supply to the anterior, lower 2/3rds of the spinal cord Cross section of spinal cord Substantia gelatinosa Found in the dorsal horn of the spinal cord Plays a major role in processing and modulating nociceptive input from cutaneous nociceptors Major site of action for intrathecal opioids AKA “Rexed’s Lamina II” Vertebra—superior view Vertebra--lateral view Vertebra and disc Spinal Ligaments Spinal anesthesia Epidural Anesthesia Epidural Anesthesia Epidural Anesthesia epidural space venous plexus ligamentum flavum Epidural space widens as it descends the cord; widest at L2-3 Schematic of Spinal vs. Epidural Anesthesia Miscellaneous… Diaphragmatic Innervation Phrenic nerve (R & L branches) – Arises from C3, 4, 5 • This is the source of motor innervation (“C3,4,5 keeps a man alive”) – Sensory innervation • Lower 6 intercostal nerves Cardioaccelerator nerves Arise from T1-4 Bradycardia usually noted in quadriplegia or high level of spinal anesthesia Landmarks for Sensory Levels T4 Nipple T6 Xiphoid T7 Lower border of scapula T8 Lower border of rib cage T10 Umbilicus L4 Iliac crest Dermatome Man Peripheral Nerve Stimulation Most common site of placement of PNS is along the groove of the ulnar nerve – Elicits a response from the adductor pollicis brevis May use the facial nerve distribution for placement if arms are not accessible – Elicits a response from the • orbicularis oculi • corrugator supercilii Arterial Supply of the Hand Sites for arterial cannulation Radial artery – Most commonly selected site Ulnar artery – Major blood supply of the hand – Difficult to cannulate; deep, tortuous Brachial artery – Large, easy to cannulate – Risk of median nerve damage Axillary artery Femoral artery – Good to use in low flow states Dorsalis pedis artery – May have distortion of waveform; falsely high SBP 2º distance from aorta Positioning neuropathies following surgery are from: – stretching of nerves for sustained periods of time – pressure on nerves for sustained periods of time • leads to ischemia of the nerve neuropathy • alopecia of occipital area; particularly in low-flow states anesthetized pts are unable to compensate for awkward/painful positions – muscle relaxation allows for positioning that would otherwise not be tolerated by the pt proper positioning considered a “shared responsibility” among OR team (however…) Positioning upper extremity – *ulnar nerve is the most frequently damaged in pts in the supine position – neuropathy may manifest as sensory and/or motor deficit • usually transient – 70-90% of injured pts are male – other predisposing factors to development of injury: • • • • extremes of weight (particularly obese pts) extended bedrest (before and/or after surgery) long surgery preexisting neuropathy in the contralateral limb Brachial plexus injury most associated with median sternotomy – particularly with dissection of IMA • probably 2º uneven retraction of chest wall increased risk with – arm abduction > 90º from side • compounded if head is turned contralaterally – prone position with arms on rests beside head • may occur with arms at sides if shoulders allowed to prolapse forward with no support Positioning lower extremity – lithotomy position carries a high risk of perioperative nerve injury • usually mild/self limiting • severe footdrop – common peroneal nerve • *most commonly injured nerve in the lower extremities • relatively superficial – wraps around the head of the fibula on the lateral aspect of the knee Lower extremity nerves, cont’d sciatic nerve – adjacent to the hamstrings – stretch from hyper flexion of the hip, especially when coupled with an extended leg/flexed foot femoral nerve – more commonly injured with deep, lower abdominal retraction • sustained compression of the iliac or femoral arteries leads to ischemia – pronounced abduction of thigh (frog leg) Lower extremity nerves, cont’d obturator – injured with pronounced abduction of the thigh – neuropathies are usually sensory (numbness inner aspect of thigh) lithotomy position caveats: – padding of bony prominences is essential – position changes of the LEs must be made simultaneously 1º risk factor for the development of neuropathy following lithotomy is obesity Supine position minimal circulatory and ventilatory changes noted – FRC may be slightly due to cephalad displacement of diaphragm/abdominal contents – stress on lower back • may be attenuated with mild knee flexion – pressure on heels – legs crossed: sural (upper leg) and peroneal (lower leg) pressure – upper extremities should be neutral • if supinated, abduction from body not to exceed 90º • pronation may cause undue pressure on the ulnar groove • individualize to each pt Trendelenburg head down; associated with many physiologic changes – pulmonary compliance, FRC from diaphragmatic displacement – myocardial O2 demand • from preload, slight impedance of forward LVSV – may ultimately CO – ICP, IOP • leads to facial, scleral edema; possible retinal detachment, POVL – ? R mainstem intubation vs. extubation – risk of passive regurgitation; possible aspiration – arms should be secured if abducted – shoulder braces should be placed on acromio-clavicular processes with padding Prone face down; head and neck should remain in a neutral position – turned head may obstruct vertebral artery flow and jugular drainage upper extremities are best placed at sides – should not be abducted > 90º if extended alongside the head physiologic changes include – FRC with intraabdominal pressure • ***FRC may actually be unchanged or facilitated in absence of increased IAP – intraabdominal pressure • may impede venous return via IVC; thereby reducing preload/CO • collaterals via epidural vessels; may see intraoperative blood loss from congestion • pulmonary compliance – pooling of blood in lower extremities – facial/ocular edema • retinal artery occlusion may lead to blindness – risk compounded by overhydration with crystalloid, prolonged periods of hypotension, direct pressure on the orbits, EBL > 2.5 l, prolonged surgery – pressure on breasts, genitalia – risk for airway compromise during position changes or intraoperatively • pt should be log rolled after induction with neck maintained in a neutral position Sitting venous air embolism (VAE) is the 1º complication associated with this position – occurs when the operative site is above the level of the heart • treatment: – – – – have the surgeon flood the operative site with saline discontinue N2O aspirate air through a central venous catheter resuscitate with fluids, ionotropic support, (+) pressure ventilation other effects of sitting include: – BP, preload, CO from pooling – CPP (brachial reading underestimates pressure at the Circle of Willis!) – intrathoracic blood volume; V/Q mismatching Lateral decubitus side lying; physiologic changes generally pulmonary; overall V/Q mismatch from: – pulmonary compliance with perfusion to the upper lung dead space – pulmonary compliance and FRC with perfusion to the dependent lung shunt compression of IVC pressure on axilla on dependent side – brachial plexus injury common – pulse oximetry on dependent hand recommended to assess perfusion – Axillary roll – a misnomer! pressure on medial aspects of knees potential injury to dependent eye/ear