File
advertisement

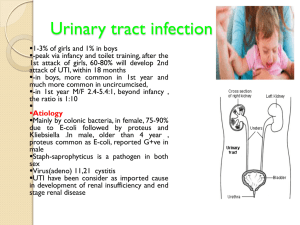
Dr MJ Engelbrecht Dept Urology University of Pretoria More common in girls Boys more common under 1 year Preputial aerobic bacterial colonization is the highest under 1 year Uncircumcised infants have a increased risk of UTI vs circumcised boys Diagnosis Urine bag Suprapubic aspiration Midstream urine specimen Interpretation Culture Midstream or urine bag collected specimen Single organism > 100000 organisms/ml Suprapubic aspiration Any number of organism is significant Which UTI should be investigated ALL FIRST INFECTIONS MUST BE INVESTIGATED Investigations Under 2 years U/S KUB VCUG Over 2 years U/S KUB VCUG only if Abnormal ultrasound Temperature more than 38 degrees Abnormalities found (50% of children) VUR Obstruction 85% of urinary tract abnormalities Posterior urethral valves PUJ Obstruction Primary obstructive megaureter Ureterocele Other Neurogenic bladder Calculi Flow of urine from the bladder into the ureters Normal anti reflux mechanism Pressure of urine in the bladder on the submucosal ureter. Therefore normal submucosal length is important. Primary reflux Short submucosal tunnel Secondary reflux N O T I C E - Neurogenic bladder Obstruction Trauma or surgery Infection Congenital ureteric abnormalities Ectopic ureteric openings 1-2 % of children 20 – 30 % of children with UTI Outosomal dominant genetic disorder 30% in siblings 50% in offsprings Reflux nephropathy Hypertension Chronic renal failure 20% of pediatric renal transplant patients have reflux nephropathy VCUG “gold” standard Done after the UTI has been treated Advantages Grades reflux Excludes secondary causes of reflux Indirect nuclear cystography Ultrasound VCUG Medical Natural history is spontaneous resolution 50% by 4 to 5 years 80% by puberty Therefore most patients are treated medically Treatment only to prevent renal scarring from infections Includes long term antibiotic prophylaxis and regular follow up (6 monthly ultrasound) Yearly assessment of the state of reflux with VCUG Surgical Indications Failure of medical treatment to prevent UTI’s Non compliance with medical treatment Severe reflux that is unlikely to resolve Associated pathology (Uretercele/Diverticulum) Persistent VUR in adolescent females (prevent problems during pregnancy) Endoscopic treatment STING (Subureteric injection of Teflon or Macrplastique) Open surgery Reimplantation of ureter into the bladder (>90% success) Obstruction of the ureter at the pelvic ureteric junction Primary Congenital intrinsic obstruction of the ureter Exstrinsic compression by a abnormal blood vessel Secondary In the lumen - In the wall - Stone or blood clot Stricture from infection or trauma Pyelonehritis Loss of normal renal function Renal failure if bilateral Calculi due to stasis The kidney is more prone to trauma Hypertension Pain due to obstruction Ultasound IVP First investigation Will show hydronehrosis with normal ureter Show dilated renal pelvis with normal ureter MAG 3 renogram Conservative If no complications and > 40% differential function Regular follow up with renal ultrasound Surgical Indications Decrease in differential function Complications UTI Renal failure Calculi Surgical Open surgical Pyeloplasty Endoscopic Endopyelotomy Balloon dilatation Laparoscopic Nephrectomy If non fuctioning kidney Thin membrane obstructing the urethra distal to the verumontanum This cause proximal urethral dilatation, severe bladder trabeculation and bilateral hydronephrosis The more severe the obstruction the earlier the patient presents 60% presents before 1 year of age Neonates presents with UTI Acute renal failure Failure to thrive Respiratory distress Palpable kidneys Urinary ascites Older children presents with Recurrent UTI Overflow incontinence Chronic renal failure Acute management Resuscitation Fluids Electrolytes Correct Acid base balance Treat UTI Urethral catheter Will relieve obstruction This will allow urosepsis and renal failure to resolve Ultrasound Will show bilateral hydronephrosis and hydroureter Thickened bladder wall Dilated posterior urethra VCUG Confirms the diagnosis Will show Dilated posterior urethra Trabeculated bladder VUR (Secondary reflux) Surgical treatment Endoscopic valve ablation (As soon as condition stabilized) Vesicostomy if persistent UTI or poor renal function Despite correct treatment 50% of these children will end up in end stage renal failure after puberty