Shoulder Girdle
advertisement

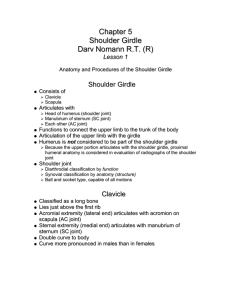
Shoulder Girdle Tanya Nolan Shoulder Girdle Formed by 2 bones Scapula Clavicle Function Connect upper limb to trunk Clavicle Long Bone Horizontal oblique plane Doubly curved for strength Function Fulcrum for movements of the arm Acromial Extremity Articulates with acromion process of scapula Sternal Extremity Articulates with the manubrium of sternum & 1st costal cartilage Scapula Flat Bone 2 surfaces 3 borders 3 angles Anterior Scapula Proximal Humerus Posterior Greater Tubercle Attachments Superior: Supraspinatus Middle: Infraspinatus Inferior: Teres Minor Lesser Tubercle Attachments Biceps Tendon Subscapularis Muscles Muscles Biceps Brachii Long Head Tendon Short Head Tendon Arises from superior margin of glenoid cavity Arises from coracoid process Muscle inserts into the radial tuberosity Bursa Small Subcoracoid Bursa Supraspinatus Muscle Long head of biceps muscle synovial filled sacs Relieves pressure and reduces friction Injury or age causes calcium deposits seen on x-rays Shoulder Girdle Articulations Scapulohumeral Ball and Socket Acromioclavicular Gliding Sternoclavicular Double Gliding AP Projection Shoulder (Anatomic Position, External Rotation) AP Projection Shoulder (Anatomic Position, External Rotation) Greater tubercle and Humeral head in profile Supraspinatus tendon insertion visualized AP Projection Shoulder (Neutral Rotation, palm against hip) AP Projection Shoulder (Neutral Rotation, palm against hip) Greater Tubercle partially superimposing the humeral head Posterior part of supraspinatus insertion demonstrated Profiles calcific deposits not otherwise visualized AP Projection Shoulder (Internal Rotation, posterior hand against hip) AP Projection Shoulder (Internal Rotation, posterior hand against hip) Lesser Tubercle in profile Proximal humerus in true lateral position Insertion site of subscapular tendon demonstrated Transthoracic Lateral Projection Shoulder (Lawrence Method) What do you do if the patient cannot sufficiently elevate the unaffected shoulder? Transthoracic Lateral Shoulder Inferosuperior Axial Projection Lawrence Method Degree of angulation of CR depends on abduction of arm Inferosuperior Axial Projection Lawrence Method Lesser Tubercle Humerus Coracoid Process Acromioclavicular Joint •Lesser Tubercle in profile •Coroacoid Process pointing anteriorly Acromion Scapulohumeral Joint Superoinferior Axial Projection Alternative to Supine Lawrence Method Place the patient in a chair at the end of the exam table and have them extend the shoulder over the table. Shoulder should be over midpoint of IR Tilt head away from IR Humeral epicondyles should be vertical CR 5-15 degrees toward elbow AP Axial Projection Trauma Shoulder CR 35 degrees Demonstrates relationship of humeral head to the glenoid cavity Useful in diagnosing posterior dislocation Scapular Y PA Oblique Projection The position of the arm is unimportant because it does not change the relationship of the humeral head to the glenoid cavity Scapular Y Scapular Y Useful in demonstrating dislocations Anterior Subcoracoid dislocation Head beneath the coracoid process Posterior Subacromial dislocation Head projected beneath acromion process AP Oblique Projection Glenoid Cavity (Grashy Method) RPO / LPO Position 35-45 degrees toward affected side Scapula parallel with the plane of the IR CR 2 in. medial and 2 in. inferior to superolateral border of the shoulder Open Glenoid Cavity in Profile Intertubercular Groove Tangential Projection CR: 10-15 degrees posterior Hand supinated Profiles the intertubercular groove free from superimposition of the surrounding shoulder structures. Acromioclavicular Articulations AP Projection: Bilateral SID: 72 inches Upright Position With and Without weights Demonstrates dislocation, separation, and the function of joints Acromioclavicular Articulations AP Projection: Bilateral What pathology does this image demonstrate? How do you know a patient is not rotated or favoring the injured side? Acromioclavicular Articulations Alexander Method AC Joint and Clavicle projected above the Acromion CR 15 degrees cephalic Clavicle AP Projection Clavicle PA Projection What would be the advantage of doing a PA Projection? AP Axial Projection Lordotic Position Thinner patients require more angulation to project the clavicle off of the scapula and ribs. Which position is easier for the patient? AP Axial Projection Lordotic Position How do you treat a fractured clavicle? Scapula AP Projection Scapula Lateral Projection Patient flexes elbow and places hand on posterior thorax Delineates the acromion and coracoid process Adjust body of scapula to be perpendicular to the IR Scapula Lateral Projection Arm brought across the chest grasping opposite shoulder Position of the arm determines what portion of the scapula will be superimposed by the humerus Scapula Lateral Projection Extending the arm upward demonstrates the body of the scapula best. Shoulder Arthrography Examination of a joint after the injection of contrast material that outlines soft tissue and joint structures. The most common purpose of shoulder arthrography is to rule out bursitis