akupunktur und riechen
advertisement

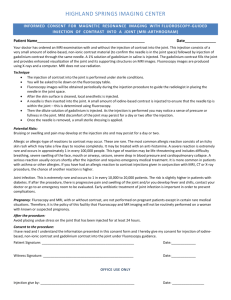
Do you know where your fillers go? An ultrasonographic investigation of the lips Julia Vent 1, F. Lefarth 2a, Th. Massing 2b, W. Angerstein 2a 1) University of Cologne Medical Center, Department of Otorhinolaryngology, Head and Neck Surgery, Cologne, Germany 2a) University of Duesseldorf Medical Center, Department of Phoniatrics and Pedaudiology, Duesseldorf, Germany 2b) University of Duesseldorf Medical Center, Department of Phoniatrics and Pedaudiology, Medical Acoustics and Audiology Unit, Duesseldorf, Germany Fig. 1: lips of Nefertiti, Berlin, 2012 Page 1 Vent et al.: European Academy of Facial Plastic Surgery, Rome, May 9-12, 2012 HNO Background Augmenting the perioral region with injectable fillers is most often performed by experience and palpation, without knowing the exact, final position of the injected material. To date, there are no in vivo investigations on the exact positioning of injectable hyaluronic acid fillers within the lips, and severe complications such as lip hematoma or thromboembolism were rarely published 2,4. The lips, and especially the modiolar region, have vivid blood supply. Thus, it was our aim to define the exact position of hyaluronic acid in the lips immediately after injection, and 18 days postinjection. Page 2 Fig. 2: blood supply of the lips1 HNO Vent et al.: European Academy of Facial Plastic Surgery, Rome, May 9-12, 2012 Material and Methods All 9 patients were history injectedtaking, with Juvederm Ultra III® and Ultra After a ®thorough photo-documentation was Smile , andA7status additionally with unlinked hyaluronic acid performed. quo via ultrasonography as well as ® . (Juvederm Hydrate ) The exact amounts, locations and informed written consent were obtained. recorded. • injection Includedtechniques in this pilotwere study were volunteers who agreed to have the lower third of the face augmented. Photographic documentation, as high resolution • Excluded were subjects who as had well undergone augmentation ultrasonography were performed. A Hitachi Hi Vision Avius in the past 6 months, with known allergies/ intolerance ultrasound system and with who linearsuffered scannerfrom (frequency range: 6against lidocaine, coagulopathies. 14 MHz) supplied images of the instable orbicularis oris muscle and Dysmorphophobic and psychic persons were also the surrounding lip tissue. Blood vessels were detected by discouraged to have injection augmentation. colour Doppler flowage mapping. Nine females (mean 55.0 years, range 41.2-66.1 years) participated in this pilot study. Three women were 6 hadperformed previouslybefore, received injectable after filler Theinjectable-naive, examinations were immediately augmentations. and 18 days after injection in 5 patients. Due to time constraints, 4 patients were examined only once on day 1 and on day 18. Page 3 Vent et al.: European Academy of Facial Plastic Surgery, Rome, May 9-12, 2012 HNO Ultrasound T cutis S muscle S air in vestibulum S S S T teeth Fig. 4: transverse B-mode scan of augmented lower lip, orbiculars oris muscle relaxed Fig 3 Fig. 3: systematic B-mode ultrasonography of the lips 1. static, at seven defined points (bars, T= transverse plane, S= sagittal plane) 2. dynamic (from midline to right and from midline to left modiolus) 3. Doppler sonography for identification of flow and vessels Page 4 Vent et al.: European Academy of Facial Plastic Surgery, Rome, May 9-12, 2012 HNO Results • Injected material distributed well within the lip tissue, and no embolism or a 2 bb * * * * * * 3 Fig. 5: paramedian, sagittal sonography scan of the right upper lip on day 1: a) before and time b) immediately after, time injection, with multiple intramuscular filler deposits; 1: during injection 2: day of injection, muscle structure and thickened by injected material (female timebulged 3: days 1-4 post injection (pi), time 4: days 5-9 pi, time 5: dayspatient, 10-14 pi aged 64 years). Orbicularis oris muscle: 1) superficial and deep layer [divided into 2) pars peripheralis and 3) pars marginalis], * filler deposits. Page 5 Vent et al.: European Academy of Facial Plastic Surgery, Rome, May 9-12, 2012 cavum oris cavum oris • thrombosis Minor bruising occurred.occurred, which resolved within 7 to 9 days. No hemorrhage could bedeposited detected ondeep daylayer 18. (pars peripheralis) of • Some of this filler material was in the orbicularis oris muscle. • the Patients showed no dysfunction of the lips, and pain only • However, the injected came up to 1 mm close to the arteries and veins of immediately aftermaterial injection. the lips. • All 9 patients were satisfied with the results and would come cutis back for injection therapy. cutis of side effects on a • Graph 11 shows these patient ratings 2 1 visual analogous scale (VAS): 3 HNO Conclusions and Discussion • In our 9 patients, no compression of lip structures occurred, nor did any severe complications result from injection. • It is crucial to know the exact anatomy to minimize complications and risks when injecting fillers. Position of injectables depends on the technique such as depot, channel or tower ². • Adverse events such as bruising or thrombosis can be avoided by ultrasonographic control. One should always have hyaluronidase as a rescue medication at hand. • When in doubt, the exact location of injected fillers should be controlled by Doppler ultrasound to avoid injury of arteries or veins. • Maybe intramuscular depots cannot be so well massaged and distributed as depots in connective tissue. Acknowledgements: • In ourHitachi opinion, intramuscular injectionsand are not absolute contraindications We thank for providing the ultrasonograph Allergan for providing Juvederm Ultra ®. al. ³. They may sometimes be necessary for an as®, stated by ®Lemperle III Ultra Smile and Hydrateet effective augmentation. References: • Because it was never monitored before, there are no limits or guidelines 1. R. Wesker: Dasand Gesicht. Bildatlas klinische Anatomie,may KVM, Berlin 2012 yetRadlanski, as to K. how deep how much substance be injected. Further 2. G. Sattler, B. Sommer: Bildatlas the der ästhetischen Augmentationsverfahren mit Fillern, KVM, Berlinfiller 2010 studies must quantify exact depth and the amount of injected 3. G. Lemperle, by P. Rullan, N. Gauthier-Hazan: Avoiding and Treating Dermal Filler Complications, Plastic materials simultaneous ultrasonography during injection. 4. Reconstr Surg 2006 (Sept, Suppl1) 92S-107S J. Niamtu III: Complications in Fillers and Botox, Oral Maxillofacial Surg Clin N Am 21 (2009) 13-21 Page 6 Vent et al.: European Academy of Facial Plastic Surgery, Rome, May 9-12, 2012 HNO