Esophagrams (Barium Swallow)
advertisement
")
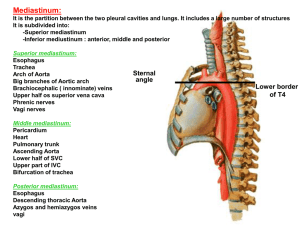
RDSC 233 Unit 8 Radiography of the pharnyx & esophagus Bontrager pp. 443-445: 458-460: 469-473 Anatomy of the pharnyx & esophagus Film Critique Radiographic anatomy Exposure Factors Positioning of: Soft tissue neck AP and lateral soft tissue neck RAO, LAO esophagus Left lateral esophagus AP, PA esophagus Radiographic Pathology Atlas of Human Anatomy Second edition (60) Need to know Nasopharynx, oropharynx, laryngopharynx, esophagus Soft palate, uvula Buccal cavity Epiglottis Piriform fossa (recess) Atlas of Human Anatomy Second edition (57) Need to know Soft palate, uvula Epiglottis Adnoids Nasopharynx, oropharynx, laryngopharynx, esophagus Vocal folds Esophagus Atlas of Human Anatomy Second edition (25x) Need to know Mucosa, submucosa, & muscular layers Zigzag (Z) line Diaphragmatic hiatus Abdominal part of esophagus Examinations of the esophagus Two procedures are done, one for the throat and one for the esophagus Barium Swallow (Esophagram) or modified barium swallow (MBS). For both the pharynx and esophagus the exam begins under fluoroscopy, in the upright position. Filming is typically done using a spot film camera or digital fluoroscopy. 90 mm cut film 105 mm roll film Spot film camera films, or photospots A similar procedure is done after a person has had a stroke or other disabling affliction to the muscles of speech. Examinations of the pharnyx With filtration Without filtration This is typically done by a speech pathologist, using barium paste, and is the one procedure commonly recorded on video tape. This procedure is also called a barium swallow. Photos from Bontrager Examinations of the pharnyx and esophagus Contrast Media Like the other examinations of the alimentary track, barium sulfate is used unless there are contraindications to barium. Both thin and thick barium are used. Thin barium is useful to outline the esophagus quickly. When administered in the upright position is empties into the stomach in seconds. It is also used to diagnose reflux when using the water test, (shallow LPO), compression, or the toe-touch maneuver. Thick barium (barium paste) is mixed with one part water to 3-4 parts barium powder. Commercial products are often packaged in a tube. Thick barium coats and adheres to the mucosa. It may be mixed with cotton balls, marshmallows, or other foods. No patient preparation is need for an esophagram, unless it is to be followed by an UGI Examinations of the pharnyx and esophagus Esophagrams begin under fluoroscopy, in the upright position. The patient holds a cup of barium, with a straw, in the right hand. The radiologist instructs the patient to patient to drink, and films in the AP, RPO, and LPO positions. The patient is often put into an RAO before the table to lowered to horizontal. The examination continues in the recumbent position. Overhead films are taken per the radiologist’s routine. The trick to overhead filming is to fill the esophagus, from the pharynx to the cardiac orifice of the stomach, and make the exposure before the esophagus empties. To do this the patient is instructed to take three large bolus swallows. On the fourth, breathing is suspended and the exposure is made at the moment the patient swallows. A shallow trendelenburg position will help keep the esophagus full. A large diameter straw is needed, and care must be taken that the end of the straw does not become vacuum sealed to the bottom of the cup. Radiographic Positioning of the x Positioning of: Soft tissue neck AP and PA of esophagus RAO and LAO esophagus Right lateral esophagus including Film Critique Soft tissue neck Expose during inspiration Positioned the same as an AP & Lateral C-spine: ½ the mAs. Done to assess the patency Nasopharynx Adnoids Oropharynx Hyoid bone Esophagus Trachea of the airway * masses * foreign bodies * enlarged adnoids (kids) * epiglottitis (kids) Routine Esophagus Positioning Preparation 1. Evaluate the order 2. Greet the patient 3. Take History What is pertinent Hx? chest pain, heartburn, dysphagia (difficulty swallowing), odynophagia (pain on swallowing) 4. Remove jewelry, check attire, snaps, pins, NG tubes, etc. 5. Explain the exam in layman’s terms 6. Questions? 7. Set technique before positioning Routine AP, PA Positioning Steps 1. 14” x 17” lengthwise (7” x 17” are also used) 2. Prone or spine. Head turned to side to allow drinking. 3. CR 1” inferior to sternal angle (Top of film 2”above shoulders). Critique criteria for frontal projections of the esophagus Entire esophagus filled with barium, in an unrotated frontal projection. When there is inadequate filling of the esophagus, under-penetration, and/or insufficient density, the esophagus is difficult to visualize against the mediastinum. Good filling, contrast, and density, demonstrating a condition called presbyesophagus Routine RAO or LAO Positioning Steps 1. 14” x 17” lengthwise (7” x 17” are also used) 2. 350-450 RAO position. (Spine must be as straight as possible, especially with tight collimation.) 3. CR to T5-6 (Top of film 2” above shoulders), several inches left of the spinous processes. Critique criteria for RAO & LAO esophagus Like the RAO stomach, which is the single best projection, the RAO is also best for the esophagus. The heart provides a homogeneous background to contrast it against, and the distal esophagus, traversing the esophageal hiatus, is laid out in profile. The RAO should demonstrate the entire barium filled esophagus. The abdominal portion is more important than the pharyngeal portion, which may be evaluated by direct inspection. Critique criteria for LAO esophagus The LAO may provide valuable diagnostic information, but contrasts the esophagus against the hilar area of the right lung and foreshortens the abdominal esophagus at the gastroesophageal junction. Photo from Bontrager The RAO & LAO should both demonstrate the entire barium filled esophagus. The abdominal portion is more important than the pharyngeal portion, which may be evaluated by direct inspection. Routine Right lateral Positioning Steps 1. 14” x 17” lengthwise (7” x 17” are also used) 2. Right lateral. C-spine “coextensive” to T-spine. 3. CR to T5-T6 (Top of film 2”above shoulders) in the midcoronal plane. 4. The arms may be raised and superimposed (like a lateral chest position), or the left shoulder may be rotated posteriorly for a “swimmers lateral.” Swimmers lateral Humerus Critique criteria for lateral esophagus Entire barium filled esophagus projected posterior to heart, and anterior to the T-spine Soft tissue of arm Why does the esophagus extend so far below the diaphragm, and yet the cardiac orifice is not seen? The caval opening is in the left hemidiaphragm. The right hemidiaphragm is typically higher than the left due to the liver. In this case the difference between them is extreme. Exposure Factors From the “Rules of Thumb” Based on: 3 phase, 100 RS film, 12:1 or 16:1 grid, 40” SID Because the esophagus is in the mediastinum, technique calculations are the same as for the abdomen. Because the contrast is barium, the lower kVp range is the same as for the single contrast UGI or colon: over 100 for penetration. Because the diameter of the esophagus is small compared to the stomach or colon, the upper range is 110 kVp. In summary: Abdomen technique calculations in 100-110 kVp range Significant Pathologies of the esophagus and their Radiographic Appearances TE fistula Foreign body Diverticulum Esophageal CA Presbyesophagus Treacheoesophageal (TE) fistula A congenital or ulcerative opening (fistual tract) between the esophagus and trachea. Radiographic examinations of fistulas are fistulagrams, or sinograms (sinus tract). Barium in the bronchial tree may result from a TE fistula, or aspiration of barium. Foreign bodies in esophagus Radiolucent FBs, such as chicken or fish bones, may require a swallow of barium to demonstrate. Diverticulum Rotary blades from an electric razor. One stuck in the proximal esophagus, and one in the pyloric canal. Esophageal Cancer Colon used to replace the esophagus after it was removed in a cancer operation. Note the haustrations Presbyesophagus An old esophagus Presby, meaning old, is used to describe the dilatation and scalloping of the esophagus that occurs with age. 43. What is the name, and acronym, for a functional study of the bladder and urethra? 44. What is the term that describes contrast media that has escaped from (out of) the bladder, due to a leakage or rupture? 45. What medical specialist (i.e. gynocologist, podiatrist, etc.), inserts the cystoscope in the performance of a retrograde cystogram? 46. When the male urethra can not be catheterized due to obstruction or trauma, what is the name of the procedure used to fill the urethra with contrast? 43. What is the name, and acronym, for a functional study of the bladder and urethra? voiding cystourethrogram (VCUG) 44. What is the term that describes contrast media that has escaped from (out of) the bladder, due to a leakage or rupture? extravasation 45. What medical specialist (i.e. gynocologist, podiatrist, etc.), inserts the cystoscope in the performance of a retrograde cystogram? urologist 46. When the male urethra can not be catheterized due to obstruction or trauma, what is the name of the procedure used to fill the urethra with contrast? injection urethrogram 47. A barium swallow for examination of the muscles of speech, usually following a stroke, utilizes a recording medium used almost solely for this exam. What is that medium? 48. If a good lateral c-spine were done at 10 mAs, what would be be used for a soft tissue neck? 49. A supine position in which the head is lower than the feet is called the position. 50. What oblique position, and degree of obliquity best demonstrates the barium filled esopagus. 47. A barium swallow for examination of the muscles of speech, usually following a stroke, utilizes a recording medium used almost solely for this exam. What is that medium? Video tape 48. If a good lateral c-spine were done at 10 mAs, what would be be used for a soft tissue neck? 5 mAs 49. A supine position in which the head is lower than the feet is called the position. Trendelenburg 50. What oblique position, and degree of obliquity best demonstrates the barium filled esopagus. 35-45 RAO The End