Reason for Sentinel Node Biopsy- Dale Han, MD
advertisement

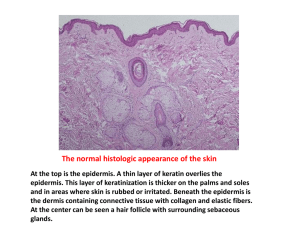
Surgical Treatment: Reason for Sentinel Node Biopsy Dale Han, MD Yale University School of Medicine Assistant Professor Department of Surgery Section of Surgical Oncology Yale University School of Medicine Prognostic Features Correlated with Melanoma-Specific Survival • Breslow thickness (T1-4) – Thin ≤1 mm (T1) – Intermediate >1 - ≤4 mm (T2, T3) – Thick >4 mm (T4) • • • • Ulceration (Ta/b) Mitotic rate in thin lesions (Ta/b)* Nodal status (N0-3) Distant metastasis (M0-1) Yale University School of Medicine Balch CM, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol 2009; 27(36):6199-206. Disease Status at Presentation, 2013 Melanoma of the Skin Yale University School of Medicine Siegel R, et al. Cancer Statistics, 2013. CA Cancer J Clin 2013;63:11-30. Nodal Status for Melanoma • Primary treated with wide local excision • Predilection for nodal spread – Nodal status prognostic for survival – Majority with no clinical evidence of nodal metastasis • Possibility for microscopic nodal spread? • Elective lymph node dissection once routinely performed to evaluate nodal status – Only 20% harbor nodal metastasis – Many unnecessarily exposed to risks and morbidity of lymphadenectomy without proven survival benefit Yale University School of Medicine Sentinel Lymph Node Biopsy • Morton et al. reported on sentinel lymph node biopsy (SLNB) for melanoma as a less invasive technique to evaluate nodal status • Hypotheses: – Each area of skin drains to specific lymph nodes – 1st draining nodes of a primary first to harbor nodal metastases and could be used to determine nodal status Yale University School of Medicine Morton DL, et al.: The sentinel lymph node and regional melanoma micrometastases. In: Cutaneous melanoma, 5th ed. Eds: Balch CM, Houghton AN, Sober AJ, Soong S, Atkins MB, Thompson, JF. Quality Medical Publishing, Inc., St. Louis, MO (2009). Sentinel Lymph Node Biopsy • Peri-tumoral and intradermal injection of localizing agents – Accumulates in interstitial fluid and drains via lymphatics into regional nodes – Accumulates in 1st order nodes which are traced intra-operatively Uren RF, et al.: Lymphoscintigraphy in patients with melanoma. In: Cutaneous melanoma, 5th ed. Eds: Balch CM, Houghton AN, Sober AJ, Soong S, Atkins MB, Thompson, JF. Quality Medical Publishing, Inc., St. Louis, MO (2009). • Radiotracer – Lymphoscintigraphy • Vital blue dye Yale University School of Medicine Tufaro AP, et al.: Neck dissection and parotidectomy for melanoma. In: Cutaneous melanoma, 5th ed. Eds: Balch CM, Houghton AN, Sober AJ, Soong S, Atkins MB, Thompson, JF. Quality Medical Publishing, Inc., St. Louis, MO (2009). Efficacy and Value of SLNB: Multi-center Selective Lymphadenectomy Trial - I Breslow thickness: - 1.2 – 3.5 mm - >3.5 mm Randomization: - WLE and observe - WLE and SLNB 1661 randomized - 1347 intermediate - 314 thick Positive SLN: - 16% intermediate - 32.9% thick Yale University School of Medicine Morton DL, et al. Final trial report of sentinel-node biopsy versus nodal observation in melanoma. N Engl J Med. 2014;370(7):599-609. doi: 10.1056/NEJMoa1310460. • Within SLNB group, MSS differed significantly between positive and negative SLN patients in both intermediate and thick groups Yale University School of Medicine Morton DL, et al. Final trial report of sentinel-node biopsy versus nodal observation in melanoma. N Engl J Med. 2014;370(7):599-609. doi: 10.1056/NEJMoa1310460. SLN status most powerful predictor of survival Significant prognostic value for evaluating SLN status for intermediate group Yale University School of Medicine Morton DL, et al. Final trial report of sentinel-node biopsy versus nodal observation in melanoma. N Engl J Med. 2014;370(7):599-609. doi: 10.1056/NEJMoa1310460. Efficacy and Value of SLNB: Sunbelt Melanoma Trial Over 3600 patients enrolled Breslow thickness: ≥1 mm All patients had SLNB Positive SLNB: 19.8% Yale University School of Medicine McMasters KM, et al. Lessons learned from the Sunbelt Melanoma Trial. J Surg Oncol. 2004;86:212-223. False-Negative Rate of SLNB • Meta-analysis shows range of 0 to 34% • Overall FNR of 12.5% (95% CI 11-14.2%) Yale University School of Medicine Valsecchi ME, et al. Lymphatic mapping and sentinel lymph node biopsy in patients with melanoma: a meta-analysis. J Clin Oncol.2011;29:1479-1487. SLNB for Intermediate Thickness Melanoma • Primary group evaluated for SLNB are patients with intermediate thickness melanoma – SLN status powerful prognostic value in this population – Positive SLNB rate ~15-20% – Identifies who will need node dissection and spares node-negative patients morbidity of lymphadenectomy – False-negative rate ~10-15% – Complication rate ~5-10% • Lower number of harvested nodes allows for more rigorous evaluation of each node Yale University School of Medicine SLNB for Thick Melanoma • Controversy exists over use of SLNB for thick melanoma (≥4 mm) • 30-40% of patients with thick melanoma ultimately develop systemic metastases • Regional staging may have limited utility in patients who ultimately develop distant disease • For patients who do not develop systemic disease, staging of regional nodes may provide benefit since 25-40% of these patients will harbor SLN metastases Yale University School of Medicine SLNB for Thick Melanoma Morton et al. 2014 Yale University School of Medicine MSLT-I Significant difference in MSS by SLN status Gajdos C, et al. Is there a benefit to sentinel lymph node biopsy in patients with T4 melanoma? Cancer. 2009;115:5752-5760. SLNB for Thin Melanoma • 70% of newly diagnosed melanomas are thin melanomas (≤1 mm) • Most patients with thin melanoma have a good prognosis with 10-year survival rates of ~90% • Controversy exists – Subset of thin melanoma patients do poorly with 5-10% developing regional recurrences and these patients may benefit from nodal staging – Low incidence of nodal metastasis – Uncertain prognostic value • Several high-risk factors for nodal disease in thin melanomas reported with no consensus Yale University School of Medicine Studies Evaluating SLN Metastasis in Thin Melanoma N +SLN Han et al. 1250 Yonnick et al. Thick Clark Ulc 5.2% Yes Yes Yes 147 11% Yes Han et al. 271 8.1% Kesmodel et al. 181 5% Venna et al. 484 7% Ranieri et al. 184 6.5% Yes Yes Koskivuo et al. 56 5.4% Yes Yes Murali et al. 432 6.7% Yes Oliveiri et al. 77 7.8% Wright et al. 631 4.9% Yes Sondak et al. 42 9.5% Yes Olah et al. 89 13.5% Bedrosian et al. 71 5.6% Taylor et al. 135 5.2% Yale University School of Medicine Age MR Gender Regress TIL VGP LVI Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Guidelines for SLNB for Melanoma • SSO/ASCO and NCCN published guidelines – Intermediate thickness melanoma: SLNB is recommended for patients with intermediate thickness cutaneous melanoma (Breslow thickness 1-4 mm) of any anatomic site. – Thick melanomas: SLNB may be recommended for staging purposes and to facilitate regional disease control for patients with cutaneous melanomas that are T4 or >4 mm in Breslow thickness. – Thin melanomas: There is insufficient evidence to support routine SLNB for patients with melanomas that are T1 or <1 mm in Breslow thickness, although it may be considered in high-risk patients. Yale University School of Medicine Wong SL, et al. Sentinel lymph node biopsy for melanoma: American Society of Clinical Oncology and Society of Surgical Oncology joint clinical practice guideline. J Clin Oncol. 2012;30:2912-2918. Coit DG, et al. Melanoma clinical practice guidelines in oncology. J Natl Compre Cancer Netw. 2012;10:366-400. Why is CLND Recommended? • Gold standard is completion lymph node dissection (CLND) for positive SLNB and no evidence of distant disease • Rate of additional nodes with metastasis in CLND after positive SLNB: – Range: 15-32% – MSLT-I: 16%, Sunbelt: 16% – Meta-analysis: 20.1% • SSO/ASCO and NCCN guidelines recommend CLND for all patients with a positive SLNB Yale University School of Medicine Why is CLND Recommended? MSLT-I Yale University School of Medicine Faires MB, et al. The impact on morbidity and length of stay of early versus delayed complete lymphadenectomy in melanoma: results of the Multicenter Selective Lymphadenectomy Trial (I). Ann Surg Oncol. 2010;17:3324-3329 Does Every Positive SLN Case Require CLND: MSLT-II • 80-85% of positive SLN cases with no additional nodal metastasis outside of SLN disease • 70-80% of positive SLN patients only have 1 node with metastasis Yale University School of Medicine Morton DL, et al. Sentinel node biopsy for early-stage melanoma: accuracy and morbidity in MSLT-I, an international multicenter trial. Ann Surg. 2005;242:302-11; discussion 311-3. Summary • Sentinel lymph node biopsy – Recommended for intermediate and may be recommended for thick melanomas – May be considered for thin melanomas with high-risk features • Sentinel node status is prognostic for survival • Until results of MSLT-II are available, CLND is recommended for a positive SLNB Yale University School of Medicine Thank You