Urethral Stricture
my treatment algorithm
Sanjay Kulkarni
Prof of Urology
KULKARNI Urethroplasty Centre
Pune, India.
Urethra is Urethra, Penis is Penis
Don’t touch Penis
Italian Patient to Guido Barbagli
Genital skin flaps are used rarely now
Retrograde Urethrography and MCU
Site
•Penile
•Bulbar: Proximal
Mid to Distal
•Posterior
Urethro- Cystoscopy 6Fr URS
Non-obliterative
Obliterative
Management
Cure
DVIU
Trauma
Anastomotic
Dilation
Bulbar
Posterior
CIC
Stent
Long gaps
To Create Stable urethra of
Normal Caliber
Penile 1 Asopa
2 Kulkarni- Barbagli
3 Two stage BMG
Bulbar
Proximal -Ventral BMG
Mid-Distal- Dorsal BMG
Long ObliterativeDouble Face BMG
Pan Urethral-Kulkarni
Diversion
Augmented Substitution
Perineal
Anastomosis Oral Mucosa Flap
Urethrostomy
Management
• Dilatation rarely cures a stricture
• Results of Dilation and DVIU are same
• DVIU followed by CIC should NEVER be
the first line of treatment
• CIC- Unfit pt.
Pt. refuses surgery
Multiple failed urethroplasties
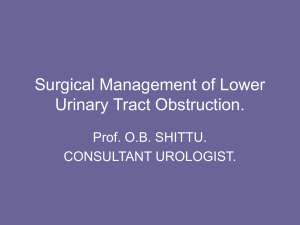
Injury -Posterior urethra plucked away
Surgery -Bulbar urethra mobilized
Management of the patient with
Pelvic fracture urethral injury
Resuscitation of the
patient to preserve life
Supra Pubic Catheter
Preserve the
bladder neck
Avoid jeopardizing
sexual function
residual to the trauma
SPC
MCU+ RGU
Impotence due to Posterior Urethral
Injuries
Duplex Color Doppler
Posterior urethral injury
The goal of surgery
Tension free Bulbo-Membranous anastomosis
Instruments
Lithotomy with Allen stirrups
Posterior urethral trauma
Simple
•
•
•
•
•
•
•
•
•
Complex
Failed urethroplasty
Boys
Girls
Recto urethral fistula
Long gap > 4cm
BN incompetence
Impotence
Bulbar urethral ischemia
Abscesses and fistulae
Approaches
Perineal 1. Bulbar urethral mobilization
2. Crural separation
Elaborated perineal (Webster)
3. Inferior pubectomy
4. Supra-crural rerouting of urethra
Perineo abdominal (Turner Warwick)
5. Total pubectomy
6. Omental wrap
Simple perineal repair
1.Bulbar urethra mobilized
2.Crural separation
Ancilliary procedures
3.Inferior pubectomy
4.Supra-crural rerouting
Abdominal Approach
5.Total Pubectomy
6.Omental Wrap
Omental wrap
SPC-Flexible cystoscopy
Veru Montanum
SPC Flexible cystoscopy
During surgery
Prostate apex and pubic bone
Prostate low
Step 1: Bulbar urethra mobilized
Prostate high
Step 3: Inferior pubectomy
Prostate back
Step 2: Crura separation
The most unpredictable part of the surgery is the ease with which the
proximal urethra can be identified and spatulated-AR Mundy
Bulbo-prostatic gap
Bulbar urethral length
Less than 1/3
Less chance of pubectomy
More than 1/3
More chance of pubectomy
MM Koraitim, J Urol 2008, 179: 1879-81
Anastomotic urethroplasty for
posterior urethral trauma
Arezzo
Italy
Pune
India
Patients
18
172
Inferior
pubectomy
4
22%
0
Transpubic
100
58%
28
17%
75%
Success rate of Anastomotic urethroplasty
for posterior urethral injuries
Primary 95%
Redo
85%
Multiple failed urethroplasties
Incontinenent
Anastomosis to a False passage
Recto Urethral fistula
Urethral injury in a Girl
Penile Urethra: Normal Penis
1. Asopa
2. Kulkarni-Barbagli
Penis not normal,HypospadiasCripple -2 stage BMG
Bulbar urethra: Trauma 1-2 cm
Anastomotic urethroplasty
Bulbar urethra-Proximal
Ventral Onlay BMG
Bulbar Urethra
Transection
•
•
•
•
•
•
Trauma
Anastomotic
Success-90%
Recurrence-Obliterative
Augmented Anastomosis
5%Impotence
No Transection
•
•
•
•
•
•
•
•
No Trauma
Dorsal BMG
Success 85%
Recurrence- Non Obliterative
Ventral BMG
2% Impotence
Andrich,Mundy
2003 JUrol Vol 170,1,90-92
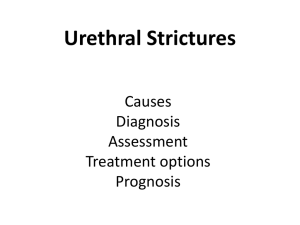
Long obliterative Bulbar urethral stricture
Trauma-Augmented Anastomosis
Long Obliterative Bulbar urethral stricture
No Trauma-Double face BMG
Double Face BMG
Bulbar Mid-Distal
Kulkarni-Barbagli Dorsal BMG
Bulbo-Spongiosus muscle preserved
One side dissection
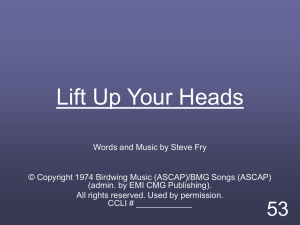
Pan urethral stricture repair
Kulkarni-Barbagli
Harvesting oral mucosa:
Buccal
Lip
Lingual
Fellowship in Reconstructive Urology
GURS
13 Centers in USA, London, Pune
Indian School of Urethral Surgery
www.strictureurethra.com