Acute and Fulminant Viral Myocarditis
advertisement

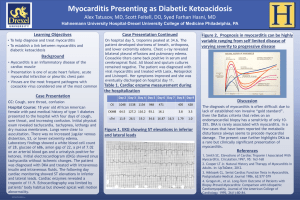
Case 1 17-year-old girl with a PMHx significant only for asthma presented with a chief complaint of fatigue. Her mother noticed she had been having unintentional weight loss of 10 pounds over 2 weeks and brought her to a doctor who diagnosed her with (asymptomatic) UTI and treated her with Bactrim. After 1 week, she represents with fever, abdominal pain, nausea and vomiting. 1 Case 1 A CT of the abdomen and pelvis showed no abnormalities and she is discharged with Keflex for pyelonephritis. She returns in 24 hours hypotensive with the following ECG. 2 Case 1 : Troponin 13 3 Case 1 On arrival to VCU she is hypotensive with a SBP in the 60-80s despite 4L IVF Dobutamine 5mcg/kg/min is running HR 140s Lactate 7.2 Troponin >50 4 QuickTime™ and a Microsof t V ideo 1 decompressor are needed to see this picture. 5 QuickTime™ and a Microsof t V ideo 1 decompressor are needed to see this picture. 6 Acute and fulminant VIRAL Myocarditis Frances Canet, MD Cath Conference August 18, 2011 7 Outline Definition Incidence Clinical presentation Etiologies Pathogenesis Diagnostics Treatment Prognosis 8 Definition of mycocarditis Inflammation of the heart muscle secondary to injury Ischemic damage Mechanical trauma Genetic cardiomyopathies Exposure to discrete external antigens ○ Viruses, bacteria, parasites, toxins drugs Internal triggers ○ Autoimmune activation against self antigens 9 Dallas criteria Active myocarditis: the presence of an inflammatory infiltrate of the myocardium with necrosis and/or degeneration of adjacent myocytes not typical of the ischemic damage associated with coronary artery disease (CAD). Borderline myocarditis: the presence of an inflammatory infiltrate of the myocardium without necrosis or degeneration of adjacent myocytes. 10 Incidence Difficult to ascertain, depends on criteria used Estimated 8 to 10 per 100,000 Unselected autopsy series as high as 1 to 4 per 100 Young adults with sudden cardiac death, estimated 8.6% Idiopathic dilated cardiomyopathy patients only 10-40% are secondary to myocarditis 11 Population Bimodal age distribution Young children and teenagers: acute presentation Exuberant response to initial exposure of antigen Older adults: Subtle and insidious symptoms of dilated cardiomyopathy and heart failure Mature immune system with greater tolerance 12 Clinical presentation Wide-ranging clinical presentation contributes to difficult diagnosis and classification Asymptomatic ECG or echocardiographic abnormalities Cardiac dysfunction, arrhythmias, heart failure and hemodynamic collapse 13 Acute Myocarditis Presentation Fatigue 82% Dyspnea on exertion 81% Arrhythmias 55% Palpitations 49% Chest pain at rest 26% 14 Acute Myocarditis Presentation Acute ischemic syndrome type symptoms Elevated troponin ST-segment elevation on ECG Segmental wall motion abnormalities on echocardiography Viral prodrome symptoms 20-80% Fever Chills Myalgias Constitutional symptoms 15 Fulminant Myocarditis Presentation Abrupt onset within 2 weeks of a viral illness Hemodynamic compromise Hypotension requiring pressors and mechanical support Echocardiogram reveals diffuse global hypofunction Thickening of the ventricular wall probably due to myocardial edema from myocardial inflammation and cytokine release 16 Case 1 QuickTime™ and a Microsof t V ideo 1 decompressor are needed to see this picture. 17 Endomyocardial biopsy in fulminant myocarditis Typical and diffuse myocarditis in each histologic section 18 Infectious Etiologies 19 Non-infectious Etiologies 20 Pathogenesis of viral myocarditis caused by coxsackievirus 21 Pathogenesis 22 Pathogenesis 23 Diagnostics: Expanded Criteria for Diagnosis of Myocarditis Category I: Clinical Symptoms Clinical heart failure Fever Viral prodrome Fatigue Dyspnea on exertion Chest pain Palpitations Pre-syncope or syncope 24 Category II: Evidence of Cardiac Structural or Functional Perturbation in the absence of Regional Coronary Ischemia Echocardiography evidence Regional wall motion abnormalities Cardiac dilation Regional cardiac hypertrophy Troponin release High sensitivity (>0.1 ng/mL) Positive indium In 111 antimyosin scintigraphy and Normal coronary angiography or Absence of reversible ischemia by coronary distribution on perfusion scan 25 Category III: Cardiac Magnetic Resonance Imaging Increased myocardial T2 signal on inversion recovery sequence Delayed contrast enhancement after gadolinium-DTPA infusion 26 Category IV: Myocardial biopsy – Pathologic or Molecular Analysis Pathology findings compatible with Dallas criteria Presence of viral genome of polymerase chain reaction or in situ hybridization 80-100% specificity when performed from myocardial biopsy 27 Enzyme biomarkers Elevated secondary to myocardial damage from inflammatory cell infiltrates, cytokine activation and virus- mediated cell death More useful when high sensitivity thresholds are used Troponin T threshold of >0.1mg/mL increases sensitivity from 34% to 53% 28 ECG Findings T wave inversions ST-segment elevation Bundle branch block Supraventricular arrhythmias Ventricular arrhythmias 47% sensitivity, indeterminate/poor specificity 29 Echocardiography Regional ventricular dysfunction Ventricular remodeling Chamber dilation Regional hypertrophy Regional wall motion abnormalities May not be able to distinguish from myocardial ischemia or infarction Useful as follow-up to monitor natural history and response to treatment Helps distinguish fulminant from acute myocarditis 30 Cardiac MRI Characterizes tissue according to water content and changes in contrast kinetics (T2 imaging) Can detect local patchy nature of myocarditic lesions Extracellular contrast agents such as gadolinium-DTPA distribute and clear differently in inflamed or scarred tissue compared to normal tissue (T1 imaging) 31 Cardiac MRI T2 weighted imaging has a sensitivity of 84% and specificity of 74% based on biopsy or natural history evidence of myocarditis Delayed enhancement increases diagnostic accuracy to 90% Deposition of collagen bundles in healing binds gadolinium and decreases its clearance 32 Cardiac MRI Helpful in guiding biopsy CMR suggests the lateral wall is a common location for lesion development (not the septum) 33 Case 2 34 Case 2 35 Case 3 36 Case 3 37 Case 4 38 Role of CMR in myocarditis 2009 Indications for CMR include New-onset or persisting symptoms suggestive of myocarditis Evidence of recent or ongoing myocardial injury or dysfunction Suspected viral or non-ischemic etiology 39 Criteria for myocarditis At least 2 of the following indicators of inflammation Regional or global myocardial signaling intensity increase in T2-weighted images Increased global myocardial early gadolinium enhancement between myocardium and skeletal muscle in gadolinium-enhanced T1 weighted images At least one focal lesion with non-ischemic regional distribution in inversion recovery prepared gadolinium-enhanced T1-weighted images 40 Myocardial Biopsy The Dallas criteria are the gold standard for diagnosis, however there are many reasons for insensitivity Patchy nature of disease Of postmortem hearts of patients with known myocarditis, only 25% of single endomyocardial biopsies showed myocarditis 66% if 5 biopsies were taken Most inflammation is in the lateral wall 41 The Role of Endomyocardial Biopsy AHA/ACC/European Society of Cardiology released a scientific statement in 2007 with 14 clinical scenarios Only the first 2 scenarios are class 1 recommendations with B level of evidence 42 Clinical Scenarios for Biopsy 1. New-onset heart failure of <2 weeks duration associated with a normal sized or dilated left ventricle and hemodynamic compromise 2. New-onset heart failure of 2 weeks to 3 months duration associated with a dilated left ventricle and new ventricular arrhythmias, second- or third-degree heart block, or failure to responds to usual care with 1-2 weeks 43 Risks of endomyocardial biopsy Complications occur in 2-5% of patients with a dilated cardiomyopathy Half of these are related to venous access Arterial puncture Pneumothorax Vasovagal reaction Bleeding after sheath removal 44 Risks of endomyocardial biopsy Related to the biopsy itself Arrhythmias Cardiac conduction abnormalities Cardiac perforation ○ Pericardial tamponade Death 45 Molecular evaluation of biopsy Combined with Dallas criteria, improves sensitivity of the biopsy as a diagnostic tool Detect viral myocarditis Delineate potential viral etiology In-situ hybridization, PCR PCR is limited by requirement of the viral pathogen must be declared in advance Helps with prognosis and to guide therapy 46 Treatments/Therapeutic Approaches Supportive Therapy Immunosuppression Interferon Intravenous Immune Globulin Immune Adsorption Therapy Hemodynamic Support Vaccination 47 Supportive Therapy First-line therapy Only a small proportion of patient require hemodynamic support Treat this group same as for clinical heart failure Diuretics IV Vasodilators: Nitroglycerin, Nesiritide ACEi, ARBs, B-blockers when stable ○ Anti-inflammatory properties 48 Immunosuppression Unproven hypothesis No shortage of short trials, limited by High degree of spontaneous improvement in the control and treatment arms Small sample size with heterogenous population Patchy nature of myocardial biopsy Lack of relationship between pathologic abnormalities and clinical prognosis 49 NIH-sponsored Myocardial Treatment Trial 50 Interferon Type 1 interferons (IFN- and IFN- phosphorylate interferon-stimulated genes in the host innate immune systemdegradation of foreign viral RNA and interfere with accumulation of viral RNA 2003, Kuhl et. Al. evaluated 22 patients with dilated cardiomyopathy and biopsy evidence of viral persistence 24 weeks of IFN- Eliminated the viral genome in all 22 patients LVEF improved from 44.6% to 53.1% in 15 of 22 patients. NYHA class also improved 51 Intravenous Immune Globulin Passive immunization with IVIG 2001 Controlled trial of IVIG in recentonset dilated cardiomyopathy, McNamara et. Al. 62 patients IVIG or Placebo LVEF improved 25 to 41% at 6 months LVEF improved to 42% at 12 months Same improvement seen in both IVIG and Placebo group 52 Intravenous Immune Globulin No primary indication except: Pediatric population Patients refractory to immunosuppressive therapy Need to obtain viral studies prior to administering 53 Immune Adsorption Therapy Plasmapheresis of peripheral blood Cytokines, circulating antibodies may target specific components of the myocyte under stress Beta-adrenergic receptor ATP carrier Myosin molecule Leads to cell dysfunction and cell death 54 2001 Immunohistological changes in dilated cardiomyopathy induced by immunoadsorption therapy and subsequent immunoglobulin substitution, Staudt at. al 34 patients, randomized Standard therapy or immune adsorption therapy aimed at removal of antibodies against the beta-adrenergic receptor After 1 year, treatment group LVEF improved from a mean of 22 to 38%. 55 Hemodynamic Support Patients with fulminant myocarditis and cardiogenic shock may require Intra-aortic balloon pump Ventricular assist devices Extracoporeal membrane oxygenation (ECMO) 56 Vaccination Targeted vaccination in the future Patients genetically susceptible to myocarditis After the mumps vaccination Disappearance of endocardial fibroelastosis causing dilated cardiomyopathy 57 Prognosis Most patients with acute myocarditis and mild cardiac involvement recover without long-term sequelae Patient with advance cardiac dysfunction, varied outlook Patients with severe hemodynamic collapse at presentation actually have a good prognosis 93% transplant-free survival in 11 years 30% of those with chronic myocarditis may recover 58 Prognosis Several studies have looked at clinical variables that predict adverse outcomes (death and transplantation) Syncope Bundle branch block EF <40% Other factors NYHA Class III or IV PCWP <15mmHg Immunopathologic evidence of myocardial inflammation Failure to use B-blockers BiV failure Giant cell or viral genome on biopsy 59 Other poor prognostic signs Dilated cardiomyopathy with positive enteroviral genome Viral genome persistence on myocardial biopsy Excessive apoptosis Myocardial expression of Fas ligand or tumor necrosis factor receptor 1 showed minimal recovery 60 Good prognosis Echo evidence of small left atrial and LV size was predictive of recovery in one small study 61 Summary Myocarditis is a model study of host injury and repair Diagnosis was classically dependent on Dallas criteria Newer modalities of testing such as cardiac MRI and PCR will help pinpoint diagnosis thus facilitating treatment and prognosis 62 Summary Understanding the pathophysiologic mechanisms of infection and injury has led to new treatments. Interferon and immune-modifying agents as well as advanced modes of hemodynamic support will offer patients the best chances of full recovery. 63