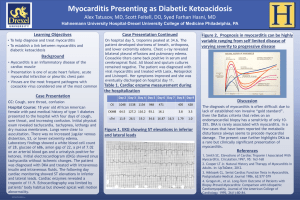
TEXTBOOK READING 1 2 “Any inflammation of the myocardium” External Triggers : 1. Viruses 2. Bacteria 3. Parasites 4. Toxins 5. Drugs 6. Mechanical trauma Internal Triggers : 1. Autoimmune activation 2. Ischemic damage 3. Genetic cardiomyopathies Cardiac injury Immunologic response Cardiac inflammation Destroy heart tissue acutely Persistent cardiac dysfunction Cardiac remodeling Dilated cardiomyopathy, heart failure, death Good news : most patients is self limited with proper support and follow up care 3 4 Prevalence rate Per 100.000 Global Burden of Disease Myocarditis Higher in the 1st year of life 9.21 8.04 Estimated 0.42 deaths per 100.000 1-14 years, males = females >15 years, males > females 1990 2019 Disability from Myocarditis - HEART FAILURE DCM SUDDEN CARDIOVASCULAR DEATH 2% of infants 5% of children 5-14% of young athletes 5 6 GIT/respiratory Mucosal surface Respiratory 7 Mechanism: 1. Direct infection 2. Activation of inflammatory myocardial dysfunction 3. Bloodstream infection metastatic foci in myocardium Pathogens: 1. Corynebacterium diphteriae 2. Streptococcal 3. Tuberculosis 4. Tropheryma whipplei 5. Borrelia burgdorferi Trypanosoma cruzi : Chagas disease 1. Trichinella 2. Echinococcus 1. Arsenicals and lithium myocyte necrosis 2. Physical agents: Radiation, excessive heat, hypothermia 3. Drugs: antiepileptic, antimicrobial, allopurinol, sulfa-based drugs, dobutamine, corticosteroids, clozapine, smallpox vaccination, chemotherapeutic 8 9 10 Myocarditis has a wide- ranging array of potential clinical presentations ASYMPTOMATIC ECG/ECHO ABNORMALITY Community viral outbreaks/influenza pandemics : Transient ECG/ echocardiographic abnormality Mostly cardiac asymptomatic few longterm squele CHEST PAIN CARDIAC DYSFUNCTION ARRHYTMIAS/ HEART FAILURE HEMODYNAMIC COLLAPSE Young children – teenagers acute/fulminant Chest pain in Adult subtle – insidious, DCM, HF myocarditis may resemble typical B19V : endothelial dysfunction angina and GCM : ventricular arrhythmias accompanied by ECG and heart block changes including STElevation. Also can mimic in pericarditis Sarcoidosis : Enlarged LN, CXR hilar adenopathy Drug/toxin : pruritic, maculopapular rash, eosinophilia 11 ACUTE MYOCARDITIS Nonspecific symptoms related to the Heart. Fatigue (82%), DOE (81%), arrhythmias (55%), palpitations (49%), and chest pain at rest (26%). Fever, chills, myalgias, and constitutional symptoms occurs in 20%- 80% FULMINANT MYOCARDITIS Hemodynamic compromise and hypotension. Abrupt onset, usually within 2 weeks of a viral illness. Echo: diffuse global hypofunction, cardiac dilation, thickening ventricular wall. EMB: typical diffuse myuocarditis GIANT CELL MYOCARDITIS EOSINOPHILIC MYOCARDITIS Heart failure, arrhythmia, or heart block, with standard medical therapy fails to improve. Improved with the use of immunosuppressive therapy. EMB: Giant cell, active inflammation, scar tissue. Often have other autoimmune: thymoma/crohn disease Allergic eosinophilic myocarditis : caused by a hypersensitivity reaction to a foreign antigen. Löffler endocarditis : systemic eosinophilic disorders, resulting in myocardial, endocardial, and Valvular involvement. Fulminant necrotic myocarditis. CHRONIC ACTIVE MYOCARDITIS PERIPARTUM CARDIOMYOPATHY Older adults. Insidious onset. moderate ventricular dysfunction (fatigue and dyspnea). EMB: active myocarditis, or borderline/fibrosis/myocyte droput. 60% DCM of unknown LV dysfunction in the last month of pregnancy or within 5 months of delivery, no preexisting cardiac dysfunction and no recognized cause of the cardiomyopathy. EMB: high freq of myocarditis 12 CLINICAL SUSPICION LABORATORY CRITERIA LABORATORY TESTING • • • • • Elevated cardiac troponin Elevated creatine kinase–MB In children with fulminant myocarditis, higher serum creatinine, lactate, and aspartate transaminase (AST) levels are associated with increased inhospital mortality rates. NT- pro- BNP is predictably elevated in children with acute DCM due to myocarditis HIgher interleukin-10 and soluble Fas concentrations are associated with an increased risk of death IMAGING MODALITIES ECG • • • • Nonspecific repolarization changes and sinus tachycardia are common PR- segment depression and diffuse ST- segment elevation may accompany a clinical presentation of myopericarditis. The presence of a QRS width greater than 120 milliseconds in duration and Q waves is associated with a great risk of cardiac death or need for heart transplantation. HISTOLOGIC ECHOCARDIOGRAPHY • • • • Acute cardiomyopathy : dilated, spherical ventricle with reduced systolic function Heart failure due to fulminant myocarditis : small cardiac chambers and mild and reversible ventricular hypertrophy from inflammation Segmental wall motion abnormalities often are present early A pericardial effusion usually signifies myopericarditis. 13 CLINICAL SUSPICION LABORATORY CRITERIA IMAGING MODALITIES HISTOLOGIC CMR • • • Myocardial necrosis can be detected by late gadolinium enhancement (LGE) T1- weighted, myocardialdelayed enhancement technique can quantitate regions of damage and possibly predict the risk of cardiovascular death and ventricular arrhythmias after myocarditis T2- weighted imaging can be used to detect myocardial edema 14 EMB • • • Low sensitivity due to the patchy nature of the inflammatory infiltrates in the myocardium and the reluctance of clinicians to perform an invasive diagnostic procedure GCM : diffuse or multifocal inflammatory infiltrate of lymphocytes and multinucleated giant cells in the absence of granuloma. Eosinophi (+) Cardiac sarcoidosis : giant cells are located within the granuloma, at the edges of the inflammation, where myocyte damage is present. Fibrosis (+) Acute myocarditis with widespread lymphocytic and histiocytic infiltrate (arrow) and associated myocyte damage (arrowhead). 15 Varies in relation to the clinical scenario and degree of left ventricular dysfunction at presentation 15% of patients with myopericarditis may develop recurrent myopericarditis There is a risk of late heart failure due to diastolic dysfunction years after the apparent resolution of acute myocarditis The presence of viral genomes on EMB may portend a poor outcome 16 The first- line therapy for all patients with myocarditis and heart failure is supportive care Routine treatment of mild to moderately severe acute myocarditis with immunosuppressive drugs is not recommended for adults Treatment of viral infection may be helpful in the management of posttransplantation viral heart disease in children adult patients with chronic DCM and viral genomes detected by PCR in heart biopsy tissues, one trial series suggests that 6 mIU of IFN- β three times per week improves enteroviral or adenoviral heart infection 17 Tailored Immunosuppression in Inflammatory Cardiomyopathy (TIMIC) trial, 85 patients with chronic inflammatory cardiomyopathy without persistent viral infection were randomly assigned to receive either prednisone and azathioprine or placebo. Immunosuppressive treatment was associated with an increase in the left ventricular ejection fraction from 26% to 46% and an improved quality of life. Patients with ventricular arrhythmias or heart block due to acute myocarditis should be hospitalized for electrocardiographic monitoring. Arrhythmias usually resolve after several weeks. The indications for an implantable cardiac defibrillator (ICD) are the same as with nonischemic DCM Mechanical circulatory support or extracorporeal membrane oxygenation may allow a bridge to transplantation or recovery in patients with cardiogenic shock despite optimal medical care. 18 19