rosacea
advertisement

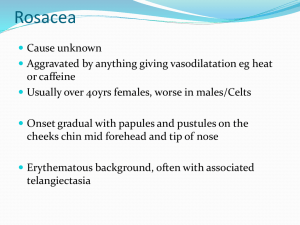
ROSACEA By Dan Ladd, D.O. Texas/KCOM Dermatology Residency Program Program Director Bill V. Way, D.O. CC: ITCHY RASH ON FACE • • • • “STINGS” “BURNS” ONSET 2 DAYS TOPICAL CREAMS NOT HELPFUL • PMX: NONE • NO NEW MEDS • NO NEW SOAPS OR PERFUMES WHAT IS ROSACEA? • • • • • • • VARIABLE DEGRESS OF….. CENTROFACIAL ERYTHEMA TELANGIECTASIAS PAPULES PUSTULES NODULES EDEMATOUS PLAQUES EARLY ROSACEA (STAGE I) • • • • “FLUSHER-BLUSHERS” OFTEN < AGE 20 NOSE/CHEEKS RECURRENT EPISODES OF BLUSHING. • ERYTHEMA PERSISTS • FEW TELANGIECTASIAS STAGE I - TELANGIECTASIAS STAGE I • TELANGIECTASIAS BECOME PROGRESSIVELY PROMINENT, FORMING SPRAYS ON THE NOSE, NASOLABIAL FOLDS, CHEEKS AND GLABELLA STAGE II PAPULES & PUSTULES BEGIN, INCREASED ERYTHEMA AND TELANGIECTASIAS STAGE III DENSE ERYTHEMA PAPULES, PUSTULES, NODULES. TELANGIECTASIAS SEVERE, DIFFUSE VARIABLE PLAQUE-LIKE EDEMA ROSACEA VS. ACNE • • • • • • ADULTS PAPULES PUSTULES NO COMEDONES ERYTHEMA TELANGIECTASIAS • • • • • • TEENS PAPULES PUSTULES COMEDONES NO ERYTHEMA NO TELANGIECTASIAS WHAT CAUSES ROSACEA? • “VIRTUALLY NOTHING IS KNOWN ABOUT • • • • CAUSATION……….THE INFLUENCE OF HEREDITY IS MOOT, AS IS ALMOST EVERYTHING THAT HAS BEEN WRITTEN ABOUT ETIOLOGY” --A. Kligman Vasomotor lability? Hypertension? Demodex mite infestation? Solar damage? Heat? Caffiene? Lymphatic obstruction? Emotional stress? Found within follicular infundibula & sebaceous ducts… Commensal organisms…. NOT Pathogenic organisms…. TRIGGERS • • • • • • HOT LIQUID BEVERAGES, SOUPS ALCOHOL / CAFFEINE SPICY FOODS SUN EXPOSURE IRRITATING COSMETICS/OTC HEAT – EXERCISE IN COOL AREAS. COMPLICATIONS • • • • COMPLICATIONS: RHINOPHYMA – DISFIGURING, NOSE OPHTHALMIC ROSACEA LESS COMMON VARIANTS: GRANULOMATOUS, STEROID, GRAMNEGATIVE, CONGLOBATA, FULMINANS RHINOPHYMA - EARLY RHINOPHYMA MODERATE SEVERE RHINOPHYMA • OCCURS EXCLUSIVELY IN MEN. • PROGRESSIVE INCREASE IN CONNECTIVE TISSUE, SEBACEOUS GLAND HYPERPLASIA, ECTATIC VEINS AND CHRONIC DEEP INFLAMMATION. • MAY OCCUE WITH STAGE III ROSACEA, BUT SURPRISINGLY, PATIENTS WITH RHINOPHYMA MAY ONLY HAVE MILD ROSACEA. Treatment – Cosmetic Repair OCULAR ROSACEA OCULAR ROSACEA COMMON, MAY BE FIRST SIGN OF ROSACEA VARIABLE PRESENTATION OCULAR ROSACEA • • • • • • BLEPHARITIS CONJUNCTIVITIS PAIN, PHOTOPHOBIA IRITIS, IRIDOCYLITIS, KERATITIS MAY NEED OPHTHALMOLOGY CONS KERATITIS MAY LEAD TO BLINDNESS TREATMENT - MILD • • • • SUNSCREENS TOPICAL SULFACETAMIDE/SULFUR TOPICAL METRONIDAZOLE ORAL TETRACYCLINE, DOXYCYCLINE, MINOCYCLINE Topicals- Sulfacetamide/Sulfur • • • • • • Klaron 10% Lotion Rosula Lotion (with Urea) Sulfacet R Rosanil Cleanser Ovace Cleanser Plexion Cleanser, Suspension and SCT Topical Metronidazoles • • • • Noritate 1% cream, Once a Day Metrocream 0.75% BID Metrolotion 0.75% BID Metrogel 0.75% BID Tetracyclines • Tetracycline 250-500mg QD or BID • Very cheap, but must take 1 hour before or • • • • 2 hours after meals, less compliance Doxycycline 50-75-100mg QD or BID Generic, Doryx Pellets, Adoxa. Minocycline 50-75-100mg QD or BID Generic, Vectrin, Dynacin, Minocin Tetracyclines • Not for children due to teeth discoloration, may cause hyperpigmetation at sites of trauma in adults, stop medication if worsening headache occurs (pseudotumor cerebri) • Photosensitivity reactions rare if patients on sunscreens TREATMENT – SEVERE • ORAL METRONIDAZOLE • CLONIDINE 0.1mg QD or BID FOR FLUSHING HELPS • PREDNISONE TAPER • ISOTRETINOIN (ACCUTANE) A SIMPLE REGIMEN FOR THE VAST MAJORITY OF ROSACEA PATIENTS • WASH FACE GENTLY WITH CETAPHIL • • • • DAILY FACIAL CLEANSER APPLY KLARON LOTION QAM APPLY SUNSCREEN WASH FACE AGAIN AT NIGHT APPLY NORITATE CREAM QHS A GOOD START…. • KLARON LOTION, 4oz., apply qAM to face • NORITATE CREAM, 30g, apply qHS to face EXPECTATIONS • TELL THEM TO EXPECT IMPROVEMENT IN 4-6 WEEKS • TELL THEM TO CONTINUE REGIMEN UNTIL NEXT VISIT • MAY GIVE ORAL TETRACYCLINES FOR FLARES • INFORM THEM THERE IS NO CURE FOR ROSACEA!!!!!!!!!!!!!!!!!!!! QUESTIONS