New Concepts in the Evaluation
and
Treatment of Dyslipidemia
Nathan D. Wong, PhD, FACC
Professor and Director
Heart Disease Prevention Program
Division of Cardiology
University of California, Irvine
Past President, American Society
for Preventive Cardiology
Lipoprotein Particles
VLDL
Density (g/ml)
0.95
Chylomicron
VLDL
Remnants
1.006
IDL
Chylomicron
Remnants
1.019
LDL-R
1.050
1.063
HDL2
Lp(a)
1.100
HDL3DL3
Only these lipoprotein particles
found in plaque at biopsy.
1.20
5
10
20
40
60
Particle Size (nm)
80
1000
High Plasma Apo B Lipoprotein
Levels Promote Atherogenesis
Rationale for therapeutic lowering of Apo B lipoproteins: decrease the
probability of inflammatory response to retention
Apo B lipoprotein
particles
Blood
Monocytes bind to
adhesion molecules
Smooth muscle
Inflammatory
response
Modification
Macrophage
Foam cell
Tabas I et al. Circulation. 2007;116:1832-1844.
Williams KJ et al. Arterioscler Thromb Vasc Biol. 1995;15:551-561.
Hoshiga M et al. Circ Res. 1995;77:1129-1135.
Williams KJ et al. Arterioscler Thromb Vasc Biol. 2005;25:1536-1540.
Merrilees MJ et al. J Vasc Res. 1993;30:293-302.
Nakata A et al. Circulation.1996;94:2778-2786.
Steinberg D et al. N Engl J Med. 1989;320:915-924.
Lipid Atherogenesis
HDL
Endothelial
injury
High plasma
LDL
LDL
+
VLDL
Adherence
of platelets
LDL infiltration
into intima
Release
of PDGF
Oxidative
modification
of LDL
Liver
Cholesterol
excreted
LCAT
APO-A1
Advanced
fibrocalcific
lesion
Other
growth
factors
+
Macrophages
Foam cells
Fatty streak
Unstable
lesion
lipid core
adventitia
Anti-atherosclerotic therapy
Stable
lesion
lipid core
adventitia
From Davies et al (1998
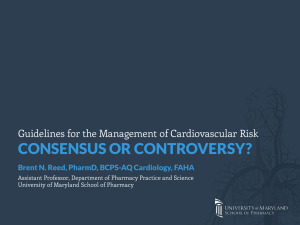
Total Cholesterol Distribution:
CHD vs Non-CHD Population
Framingham Heart Study—26-Year Follow-up
No CHD
35% of CHD
Occurs in
People with
TC<200 mg/dL
150
CHD
200
250
300
Total Cholesterol (mg/dL)
Castelli WP. Atherosclerosis. 1996;124(suppl):S1-S9.
1996 Reprinted with permission from Elsevier Science.
14-y incidence
rates (%) for CHD
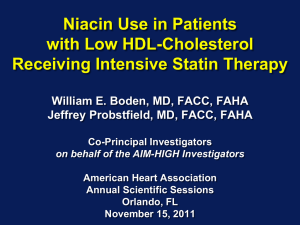
Low HDL-C Levels Increase CHD Risk Even
When Total-C Is Normal
14
12
10
8
6
4
2
0
< 40 40–49 50–59 60
HDL-C (mg/dL)
260
230–259
200–229
< 200
Risk of CHD by HDL-C and Total-C levels; aged 48–83 y
Castelli WP et al. JAMA 1986;256:2835–2838
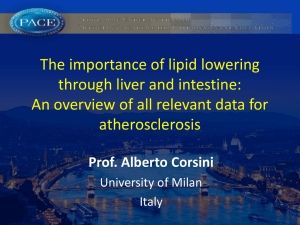
Triglyceride Level Is Significant CHD Risk Factor:
Recent Meta-Analysis of 29 Studies (n=262,525)
(Sarwar et al., Circulation 2007)
Groups
Duration of follow-up
CHD Cases
≥10 years
<10 years
CHD Risk Ratio* (95% CI)
5902
4256
Sex
N=262,525
Male
Female
7728
1994
Fasting status
Fasting
Nonfasting
7484
2674
Adjusted for HDL
Yes
No
4469
5689
1.72 (1.56–1.90)
Overall CHD Risk Ratioa
Decreased Risk
aIndividuals
1
Increased Risk
2
in top versus bottom third of usual log-triglyceride values, adjusted for
at least age, sex, smoking status, lipid concentrations, and blood pressure (most)
CHD=coronary heart disease
Sarwar N, et al. Circulation. 2007;115:450-458.
HDL=high-density lipoprotein
How Can Hypertriglyceridemia
be Atherogenic?
Triglyceride-rich lipoproteins carry cholesterol and promote
atherosclerosis*
Very–low-density lipoprotein (VLDL) is precursor to low-density
lipoprotein (LDL)
Hypertriglyceridemia (HTG) drives
Cholesterol esters enrichment of VLDL (more atherogenic)
↓ LDL size (small, dense LDL are more atherogenic)*
↓ LDL-C (small, dense LDL carry less cholesterol)*
↓ High-density lipoprotein (HDL) size (small, dense HDL are unstable)
HTG is linked to other proatherogenic states*
Insulin resistance
Proinflammatory state
Prothrombotic state
Prooxidative state
Endothelial dysfunction
*Reasons why non–HDL-C is stronger than LDL-C as predictor of cardiovascular disease
Elevated Triglycerides Are Associated With
Increased Small, Dense LDL Particles
More Particles
Fewer Particles
LDL=
130 mg/dL
Apolipoprotein
B
More
apolipoprotein B
Cholesterol
ester
Correlates with:
TC
198 mg/dL
LDL-C
130 mg/dL
TG
90 mg/dL
HDL-C
50 mg/dL
Correlates with:
TC
210 mg/dL
LDL-C
130 mg/dL
TG
250 mg/dL
HDL-C
30 mg/dL
Non–HDL-C 148 mg/dL
Non–HDL-C 180 mg/dL
Otvos JD, et al. Am J Cardiol. 2002;90:22i-29i.
TC=total cholesterol, LDL-C=low-density lipoprotein cholesterol,
TG=triglycerides, HDL-C=high-density lipoprotein cholesterol
Why Is Small, Dense LDL More
Atherogenic?
Cholesterol per particle, BUT
Subendothelial penetration
Subendothelial binding
Oxidized/modified
LDL-receptor clearance
LDL=low-density lipoprotein
Atherogenic Lipoproteins
Non-HDL; Apo B-100—containing
Non-HDL Includes All Atherogenic
Lipoprotein Classes
Very–low-density lipoprotein (VLDL)
VLDL
IDL
LDL
Made in the liver
Triglycerides (TG) >> cholesterol esters (CE)
Carries lipids from the liver to peripheral tissues
Intermediate-density lipoprotein (IDL)
• Formed from VLDL due to lipase removal of TG
• Also known as a VLDL remnant
Low-density lipoprotein (LDL)
• Formed from IDL due to lipase removal of TG
• CE >> TG
Lp(a)
Lipoprotein (a)
• Formed from LDL w/addition of apolipoprotein A
HDL
High-density lipoprotein (HDL)
• Removes cholesterol from peripheral tissues
• Atherogenic and prothrombotic
Lp(a) in Atherogenesis: Another Culprit?
Identical to LDL particle except for addition of apo(a)
Plasma concentration predictive of atherosclerotic
disease in many epidemiologic studies, although
not all
Accumulates in atherosclerotic plaque
Binds apo B-containing lipoproteins and proteoglycans
Taken up by foam cell precursors
May interfere with thrombolysis
Maher VMG et al. JAMA. 1995;274:1771-1774.
Stein JH, Rosenson RS. Arch Intern Med. 1997;157:1170-1176.
Lp(a): An Independent CHD Risk Factor in Men of the
Framingham Offspring Cohort
10
5
2
RR
2.7
1.9
1.8
1.8
1.2
1
0.5
3.6
Lp(a)
TC
HDL-C
HT
0.2
0.1
RR=relative risk; HT=hypertension; GI=glucose intolerance.
Bostom AG et al. JAMA. 1996;276:544-548.
GI
Smoking
Placebo - Statin outcome trials
Continuum
of risk
Placebo MI rate per 100 subjects per 5 years
53.7
End stage
CORONA
GISSI-HF Heart failure
(rosuvastatin)
22.6 Secondary
prevention
4S
(simvastatin)
HPS
(simvastatin)
12.9
CARE
(pravastatin)
LIPID
8.44
7.9
2.8
High-risk CHD patients
(high cholesterol)
Majority of
CHD patients
(broad range of
cholesterol levels)
(pravastatin)
PROSPER
(pravastatin)
Primary
prevention
WOSCOPS
(pravastatin)
AFCAPS/TexCAPS
(lovastatin)
JUPITER
(rosuvastatin)
Patients at high risk
of CHD (high
cholesterol)
Patients at low
risk of CHD
(low HDL-C)
LDL cholesterol and benefit in clinical trials
Is lower better ?
30
4S - Placebo
25
Rx - Statin therapy
PRA – pravastatin
ATV - atorvastatin
Secondary Prevention
4S - Rx
20
15
LIPID - Placebo
CARE - Placebo
LIPID - Rx
CARE - Rx
Primary Prevention
HPS - Rx
TNT – ATV10 HPS - Placebo
PROVE-IT - PRA
WOSCOPS – Placebo
TNT – ATV80
PROVE-IT – ATV
AFCAPS - Placebo
TNT
10
5
JUPITER
6
AFCAPS - Rx
WOSCOPS - Rx
ASCOT - Placebo
ASCOT - Rx
0
40
(1.0)
60
(1.6)
80
100
120
140
(2.1)
(2.6)
(3.1)
(3.6)
LDL-C achieved mg/dL (mmol/L)
Adapted from Rosensen RS. Exp Opin Emerg Drugs 2004;9(2):269-279
LaRosa JC et al. N Engl J Med 2005;352:e-version
160
(4.1)
180
(4.7)
200
(5.2)
Cholesterol Treatment Trialists’ (CCT) Collaboration:
Efficacy and safety of cholesterol-lowering treatment:
prospective meta-analysis fo data from 90,056
participants in 14 randomized trials of statins
(The Lancet 9/27/05)
Over average 5 year treatment period (per mmol/L
reduction—approx 40 mg/dl in LDL-C):
12% reduction in all-cause mortality
19% reduction in coronary mortality
23% reduction in MI or CHD death
17% reduction in stroke
21% reduction in major vascular events
No difference in cancer incidence (RR=1.00).
Statin therapy can safely reduce 5-year incidence of major
coronary events, revascularization, and stroke by about
20% per mmol/L (about 38 mg/dl) reduction in LDL-C
HPS: First Major Coronary Event
StatinPlaceboType of Major
Allocated Allocated
Vascular Event (n = 10269) (n = 10267)
Coronary events
Nonfatal MI
357 (3.5%)
574 (5.6%)
Coronary death
587 (5.7%)
707 (6.9%)
Subtotal: MCE
898 (8.7%)
1212 (11.8%)
Statin Better
0.73 (0.670.79)
P < 0.0001
Revascularizations
Coronary
513 (5.0%)
725 (7.1%)
Noncoronary
450 (4.4%)
532 (5.2%)
Subtotal: any RV
939 (9.1%)
1205 (11.7%)
Any MVE
0.76 (0.700.83)
P < 0.0001
0.76 (0.720.81)
P < 0.0001
2033 (19.8%) 2585 (25.2%)
0.4
Placebo Better
0.6
0.8
Heart Protection Study Collaborative Group. Lancet. 2002;360:722.
1.0
1.2
1.4
HPS—Simvastatin:
Vascular Events by Baseline LDL-C
Baseline
LDL-C (mg/dL)
Statin
(n = 10,269)
Placebo
(n = 10,267)
<100
282 (16.4%)
358 (21.0%)
100–129
668 (18.9%)
871 (24.7%)
1083 (21.6%)
1356 (26.9%)
130
All patients
2033 (19.8%)
2585 (25.2%)
Event Rate Ratio (95% CI)
Statin Better Statin Worse
0.76 (0.72–0.81)
P < 0.0001
0.4 0.6 0.8 1.0 1.2 1.4
www.hpsinfo.org
HMG-CoA Reductase Inhibitor:
Secondary Prevention
Pravastatin or Atorvastatin Evaluation and Infection
Therapy (PROVE-IT)—TIMI 22 Study
4,162 patients with an ACS randomized to atorvastatin (80 mg) or pravastatin (40
mg) for 24 months
Recurrent MI or
Cardiac Death
30
Atorvastatin
Pravastatin
25
16% RRR
20
15
10
5
P =0.005
0
3
6
9
12
15
18
21
24
27
30
Follow-up (months)
ACS=Acute coronary syndrome, CV=Cardiovascular, MI=Myocardial infarction, RRR=Relative risk
reduction
Cannon CP et al. NEJM 2004;350:1495-1504
TNT: Rationale
Patients With CHD Events (%)
30
25
TNT
20
15
10
5
Screening
?
Atorvastatin 10 mg
Atorvastatin 80 mg
0
60
(1.6)
80
(2.1)
100
(2.6)
120
(3.1)
140
(3.6)
160
(4.1)
LDL-C, mg/dL (mmol/L)
Adapted from LaRosa et al. N Engl J Med. 2005:352:1425-1435.
180
(4.7)
200
(5.2)
TNT: Changes in LDL-C by
Treatment Group
160
Baseline
Atorvastatin 10 mg (n=5006)
3.5
120
Mean LDL-C level = 101 mg/dL (2.6 mmol/L)
100
3.0
2.5
80
2.0
60
P<.001
Mean LDL-C level = 77 mg/dL (2.0 mmol/L)
1.5
40
1.0
20
0.5
0
0
Screen 0 3
12
24
36
48
Study Visit (Months)
LaRosa et al. N Engl J Med. 2005;352:1425-1435.
60
Final
Mean LDL-C (mmol/L)
Mean LDL-C (mg/dL)
4.0
Atorvastatin 80 mg (n=4995)
140
Proportion of Patients Experiencing
Major Cardiovascular Event
TNT: Primary Efficacy Outcome Measure: Major
Cardiovascular Events*
0.15
Atorvastatin 10 mg
Atorvastatin 80 mg
Relative
risk
reduction
22%
Mean LDL-C level = 101 mg/dL
0.10
0.05
Mean LDL-C level = 77 mg/dL
HR=0.78 (95% CI 0.69, 0.89); P<.001
0
0
1
2
3
Time (Years)
4
5
* CHD death, nonfatal non–procedure-related MI, resuscitated cardiac arrest,
fatal or nonfatal stroke.
LaRosa et al. N Engl J Med. 2005;352:1425-1430.
6
Recent Coronary IVUS
Progression Trials
Relationship between LDL-C and Progression Rate
Median change in percent
atheroma volume (%)
1.8
CAMELOT
placebo
1.2
0.6
REVERSAL
atorvastatin
0
-0.6
REVERSAL
pravastatin
ACTIVATE
placebo
A-Plus
placebo
ASTEROID
rosuvastatin
-1.2
50
60
70
80
90
100
110
120
Mean LDL-C (mg/dL)
Nissen SE, Nicholls S et al. JAMA 2006;295:1555–1565
Residual CVD Risk in Statin vs Placebo
Trials
Many CHD Events Still Occur
in Statin-Treated Patients
Patients Experiencing
Major CHD Events, %
40
30
20
25-40% CVD Reduction Leaves High Residual Risk
28.0
Placebo
Statin
19.4
15.9
12.3
10
0
N
LDL
4S1
4S
4444
-35%
LIPID2
LIPID
9014
-25%
Secondary
Group. Lancet. 1994;344:1383-1389.
Study Group. N Engl J Med. 1998;339:1349-1357.
3Sacks FM et al. N Engl J Med. 1996;335:1001-1009.
13.2
10.2
CARE3
CARE
4159
-28%
11.8
8.7
HPS4
HPS
20
536
-29%
High Risk
14S
4HPS
2LIPID
5Shepherd
7.9
10.9
5.5
6.8
WOSCOPS5 AFCAPS/TexCAPS6
AFCAPS
WOS
6595
6605 /
TexCAPS
-26%
-25%
Primary
Collaborative Group. Lancet. 2002;360:7-22.
J et al. N Engl J Med. 1995;333:1301-1307.
6 Downs JR et al. JAMA. 1998;279:1615-1622.
Potential Antiatherogenic Actions of HDL
Vasodilatory
Activity
Anti-inflammatory
Activity
Antithrombotic
Activity
Anti-infectious
Activity
Reverse
Cholesterol
Transport
Cellular
Cholesterol
Efflux
Apo A-I
Apo A-II
Chapman MJ et al. Curr Med Res Opin. 2004;20:1253-1268.
Assmann G et al. Annu Rev Med. 2003;53:321-341.
HDL
Antiapoptotic
Activity
Endothelial
Repair
Antioxidative
Activity
Should High-Density Lipoprotein
Be a Target of Therapy?
Change in % stenosis
per year
Change in Percent Diameter Stenosis
vs On-treatment HDL-C in QCA Trials
CCAIT
1.4
1.2
PLAC I
MARS
1
MAAS
CCAIT
0.8
PLAC I
0.6
0.4
MAAS
0.2
0
-0.2
-0.4
-0.6
-0.8
-1
40
45
LCAS
Placebo
Statin*
MARS
LCAS
ASTEROID
50
On-treatment HDL-C (mg/dL)
*ASTEROID
rosuvastatin
MARS lovastatin
MAAS simvastatin
LCAS fluvastatin
CCAIT lovastatin
PLAC I pravastatin
Ballantyne CM, Nicholls S et al. Circulation 2008; Online
Should High-Density Lipoproteins Be a
Target of Therapy ?
ATP III Guidelines on HDL-C:
“Current
documentation of risk reduction through controlled
clinical trials is not sufficient to warrant setting a
specific goal value for raising HDL-C” (Grundy SM et
al. Circulation. 2004;110:227-239)
Failure of ACCORD, FIELD, AIM-HIGH and the
experience with torcetrapib and dalcetrapib have
raised doubts re: the value of raising HDL-C
Still,
The one best study of niacin effects on CVD (HPS-
2/THRIVE) is ongoing—results early in 2013
Investigational CETP inhibitors greatly increase HDL-C
and might be shown to reduce CVD—clinical trials
ongoing, results after 2017
HDL-C Risk Factor vs Risk Marker?
Low HDL-C predicts high CVD Risk
High HDL-C predicts anti-atherogenic effects:
Anti-inflammatory
Antioxidant
Antithrombotic
Pro-endothelial
But clinical trials of HDL-C-raising agents so far
have failed to prove CVD benefit—suggesting
that HDL-C may be only a risk marker
Lifestyle Modifications to Raise HDL-C
Levels
• Smoking Cessation
− HDL-C levels are lower in smokers (by 7%-20%), and return
towards normal 1-2 months after smoking cessation
• Whole Food Plant Based Diet—dietary fiber blunts adverse
carb effect
• Weight Reduction
− For every 3 kg (7 lb) of weight loss, HDL-C levels increase
by 2-4%, but only after stabilization at new lower weight
• Exercise
− Aerobic exercise (40 min, 3-4 x weekly) may increase HDLC by 5-10%
Rössner S et al. Atherosclerosis. 1987;64:125-130.
Wood PD et al. N Engl J Med. 1988;319:1173-1179.
Ornish D et al. JAMA. 1998;280:2001-2007.
Cullen P et al. Eur Heart J. 1998;19:1632-1641.
Kokkinos PF et al. Arch Intern Med. 1995;155:415-420.
Kodama S et al. Arch Intern Med. 2007;167:999-1008.
Available Agents for HDL-C Raising
HDL-C ↑
Primary Use
Nicotinic acid
15-35%
Fibrates
5-20%
Statins
5-15%
Prescr. Om-3*
2-10%
Bile-acid resins*
2-5%
Ezetimibe*
1-3%
Pioglitazone*
5-20%
Estrogens*
10-25%
*Lacking FDA-approved indication for HDL-raising.
-blockers*
10-20%
Belalcazar LM, Ballantyne CM. Prog Cardiovasc Dis. 1998;41:151-174.
Insull W et al. Mayo Clin Proc. 2001;76:971-982.
McKenney
JM et al. Pharmacother. 2007;27:715-728.
Alcohol*
5-15%
Agent
HDL ↑
TG ↓
LDL ↓
TG ↓
LDL ↓
LDL ↓
Glucose ↓
Hot flashes
BPH
Social, etc.
Fibrate Evidence:
Primary Prevention
Fenofibrate Intervention and Event Lowering in
Diabetes (FIELD)
9,795 diabetic patients randomized to fenofibrate (200 mg) or placebo
for 5 years
11% RRR
CHD Death or
Nonfatal MI (%)
9
6
5.9
5.2
3
0
P=0.16
Placebo
Fenofibrate
A fibrate does not provide significant additional benefit* in diabetics
CHD=Coronary heart disease, MI=Myocardial
infarction, RRR=Relative risk reduction
*Unadjusted for concomitant statin use
Source: Keech A et al. Lancet 2005;366:1849-61
Fibrate Evidence:
Primary and Secondary Prevention
Action to Control Cardiovascular Risk in Diabetes
(ACCORD) Lipid Trial
5,518 diabetic patients on statin therapy randomized to fenofibrate
(160 mg) or placebo for 4.7 years
8% RRR
CV death, nonfatal
stroke or nonfatal
MI (%/year)
3
2.4
2.2
2
1
0
P=0.32
Placebo
Fenofibrate
On a background of statin therapy, a fibrate does not reduce CV events
in diabetics
CV=Cardiovascular, MI=Myocardial infarction,
RRR=Relative risk reduction
Source: ACCORD study group. NEJM 2010;Epub ahead of print
Is Niacin Useful in Low HDL-C?
HATS: Percent Change in Stenosis
4.5
4.0
Change (%)
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
-0.5
-1.0
Placebo
Antioxidant
Vitamins*
Simvastatin/
Niacin†
*P = 0.16 for comparison with placebo; †P < 0.001; ‡P = 0.004.
HATS = HDL-Atherosclerosis Treatment Study.
Adapted from Brown BG et al. N Engl J Med. 2001;345:1583-1592.
Simvastatin /
Niacin/
Antioxidants‡
Patients Free of Events (%)
HATS: Patients Free of Events
Simvastatin-niacin
100
97%
90
All placebos
80
76%
RR = 0.10
P = 0.03
70
0
0
1
2
Years
HATS = HDL-Atherosclerosis Treatment Study.
Adapted from Brown BG et al. N Engl J Med. 2001;345:1583-1592.
3
Meta-Analysis: Effects of Nicotinic Acid
Pre-AIM-HIGH Trials: Major Coronary Events
Treatme
nt
n/N
Control
n/N
ARBITER-6HALTS
Guyton JR et al
2/187
9/176
1/676
1/272
AFREGS
0/71
1/72
ARBITER-2
2/87
2/80
HATS
1/38
5/38
UCSF_SCOR
0/48
1/49
STOCKHOLM
72/279
100/276
1/94
5/94
Study
CLAS
CDP
Peto OR
95% Cl
Peto OR
95% Cl
0.25 (0.08,
0.84)
0.35 (0.02,
7.56)
0.14 (0.00,
6.92)
0.92 (0.13,
6.65)
0.24 (0.05,
1.26)
0.14 (0.00,
6.96)
0.61 (0.43,
0.88)
0.25 (0.05,
1.29)
0.81 (0.69,
0.94)
287/1119 839/2789
Total
Test for heterogeneity: P = 0.24, I2 =
23.0%
Test for overall effect: P <0.0001
Subtotal excluding CDP
0.75 (0.65,
0.86)
0.1
0.2
0.5
Log scale
Many of these trials were tests of drug combinations that included niacin.
Bruckert E et al. Atherosclerosis. 2010;210:353-361.
1
2
5
10
0.53 (0.38,
0.73)
AIM-HIGH
Design
Purpose: “Rigorous test of the HDL hypothesis…”
(not designed to be a test of niacin)
Subjects: n=3414 men/women (85%/15%) w/ prior
CVD event and HDL-C 35 (<42/53) LDL-C 74
(algorithm), TG 163 (100-400) [median (range)]
Randomized Therapy
Extended-release niacin (1500-2000 mg hs) vs
“Placebo” (immediate-release niacin 100-150 mg hs)
Open-label titration/addition (keep LDL-C in 40-80
mg/dL)
AIM-HIGH Investigators. N Engl J Med. 2001;365:2255-267.
AIM-HIGH Investigators. Am Heart J. 2011;161:471-477.e2.
Simvastatin 5-80 mg/d
AIM-HIGH — Results
HDL-C at Baseline and Follow-up
Boden WE. N Engl J Med. epub 15 Nov 2011; doi 10.1056/NEJMoa1107579.
AIM-HIGH — Results
Primary Outcome
1o Endpoint: CHD Death, nonfatal MI, ischemic stroke, high-risk ACS,
hospitalization for coronary or cerebrovascular revascularization
Boden WE. N Engl J Med. epub 15 Nov 2011; doi 10.1056/NEJMoa1107579.
Fate of Niacin Beyond AIM-HIGH: HPS2THRIVE : December 2012 Update
HPS2-THRIVE evaluated extended-release
niacin/laropiprant plus statin therapy versus
statin therapy alone in patients at high risk for
cardiovascular events
HPS2-THRIVE did not reach the primary
endpoint to reduce coronary deaths, non-fatal
heart attacks, strokes, or revascularizations
This finding, supportive of AIM-HIGH, suggests
that niacin may not provide additional benefit to
reduce CVD risk when patients are well-treated
with statins
Emerging HDL-C Therapies
CETP Antagonism
Role of CETP in Atherosclerosis
LDL-R
LDL
VLDL
CE
CETP
Foam
cells
TG
ABC-A1
RCT
Bile
LIVER
HDL
PLASMA
Atherosclerosis
LDL
ABC-G1
Free
cholesterol
PERIPHERAL TISSUE
Human CETP deficiency is usually associated with marked ↑ in HDLC
CETP activity is inversely correlated with plasma HDL-C
Decreasing CETP activity has consistently inhibited atherosclerosis
in animal models
Barter PJ et al. Arterioscler Thromb Vasc Biol. 2003;23:160-167.
Contacos C et al. Atherosclerosis. 1998;141:87-98.
Guerin M et al. Arterioscler Thromb Vasc Biol. 2008;28:148-154.
CETP Inhibitors: 2 Down, 2 Remain
--------------------↑HDL-C---------------------~80%
~80%
~138%
~30%
Evacetrapib
↑CVD (25%)
but OK HDL
function
(off-target eff.?)
Barter et al. N Engl J Med. 2007;357(13):2109-2122.
http://www.ama-assn.org/ama1/pub/upload/mm/365/dalcetrapib.doc.
http://www.ama-assn.org/ama1/pub/upload/mm/365/torcetrapib.doc.
Qiu X et al. Nat Struct Mol Biol. 2007;14(2):106-113.
CETP
*No ↓CVD,
but OK HDL
function, +/- anti
athero?
http://www.ama-assn.org/ama1/pub/upload/mm/365/anacetrapib.pdf.
http://www.roche.com/media/media_releases/med-cor-2012-05-07.htm.
*Dalcetrapib development stopped May 7, 2012 due to lack of efficacy in the
Dal-Outcomes CVD endpoint trial.
Lipid Effects of CETP
Inhibitors/Modulators
% Change from Baseline
CETP Agent
Dose
(mg/day)
HDL-C
(%)
LDL-C
(%)
TG (%)
Torcetrapib
60
61
-24
-9
Anacetrapib
100
138
-40
-7
Evacetrapib
500
129
-36
-11
Dalcetrapib
600
31
-2
-3
Adapted from Cannon C et al. JAMA. 2011;306:2153-2155.
Nicholls SJ et al. JAMA. 2011;306:2099-2109.
Torcetrapib: Increased Cardiovascular and
Patients Without Event (%)
Non-cardiovascular Morbidity and Mortality
100
98
96
94
92
90
0
Atorvastatin only
HR = 1.25
P = 0.0001
Torcetrapib plus atorvastatin
0
90 180 270 360 450 540 630 720 810
Days After Randomization
Is the toxicity of torcetrapib related to the mechanism or the molecule?
Barter PJ et al. N Engl J Med. 2007;357:2109-2122.
Torcetrapib Caused Off-target
Hyperaldosteronism
Torcetrapib arm of ILLUMINATE trial showed significant:1
↑ Systolic Blood Pressure:
Mean ↑5.4 mmHg
>15 mmHg ↑ SBP: 19.5% torcetrapib arm (vs 9.4% placebo
arm, P<0.001)
↓ serum potassium
↑ serum bicarbonate
↑ serum sodium
↑ serum aldosterone
Inverse relationship of CVD and on-Rx-HDL-C preserved
Conclusion: ↑ CVD in ILLUMINATE likely due to off-target actions of
torcetrapib, not related to CETP inhibition1,2
1. Barter PJ et al. N Engl J Med. 2007;357:2109-2122.
2. Rosenson RS. Curr Athero Rep. 2008;10:227-229.
HDL Cholesterol
(mg/dL)
dal-OUTCOMES Results: Isolated ↑HDL-C
7907
7910
7685
7663
7498
7402
7272
7196
6959
6871
6436
6333
3650
3599
LDL Cholesterol
(mg/dL)
No. at risk
Placebo
Dalcetrapib
No. at risk
Placebo
Dalcetrapib
7907
7910
7679
7657
7473
7382
Months
7265
7191
6947
6863
6427
6324
3640
3591
Schwartz GG et al.
N Engl J Med. 2012
Nov 5.
[Epub ahead of
print].
Cumulative Incidence of Primary Outcome
(% of patients)
dal-OUTCOMES Results: No ↓CVD
No. at risk
Placebo
Dalcetrapib
Year
7933
7938
7386
7372
6551
6495
Schwartz GG et al. N Engl J Med. 2012 Nov 5. [Epub ahead of print].
1743
1736
The Role of PCSK9 in the Regulation
of LDL Receptor Expression
For illustration purposes only
Impact of an PCSK9 mAb
on LDL Receptor Expression
For illustration purposes only
Change in Calculated LDL-C at 2 Weekly Intervals
from Baseline to Week 12
0
LDL-C Mean (SE) % Change from Baseline
BASELINE
WEEK 2
WEEK 4
WEEK 6
WEEK 8
WEEK 10
WEEK 12
∆ - 5.1%
-10
∆ - 8.5%
-20
∆ - 30.5%
-30
∆ - 39.6%
-40
-50
∆ - 53.6%
-60
∆ - 64.2%
∆ - 62.9%
-70
∆ - 72.4%
-80
Placebo
SAR236553 50 mg Q2W
SAR236553 100 mg Q2W
SAR236553 150 mg Q2W
Mean percentage change in calculated LDL-C from baseline to weeks 2, 4, 6, 8, 10, and 12 in the modified intent-to-treat (mITT) population,
by treatment group. Week 12 estimation using LOCF method.
LDL-C from Baseline to Week 12
by Treatment Group (mITT Population)
Intervention
Baseline LDL-C
(mg/dL)
Attained
LDL-C (mg/dL)
Placebo
130.2
120.5
SAR236553 50mg Q2W
123.2
73.2
SAR236553 100mg Q2W
127.0
46.0
SAR236553 150mg Q2W
123.9
34.2
SAR236553 200mg Q4W
128.2
71.1
SAR236553 300mg Q4W
131.6
66.0
HoFH Disease Overview
HoFH is a serious life-threatening genetic disease characterized by
extremely elevated blood LDL-C levels, premature atherosclerosis and
increased risk of CV morbidity and mortality.1
HoFH usually presents in childhood, but patients may go undiagnosed until
adulthood.2,3,4
Based on the genetic defect leading to LDL receptor dysfunction, patients
have minimal response to existing pharmacologic therapies.5
Diagnostic criteria for HoFH in the literature are variable and not universally
defined. However, the clinical diagnosis typically consists of the following:6
1.
2.
3.
4.
5.
6.
Significantly elevated levels of LDL-C
Cutaneous and tendon xanthomas and corneal arcus
Parental history of significant hypercholesterolemia and/or premature CVD
DNA confirmation can be used when diagnosis is unconfirmed
Goldberg AC, et al. Journal of Clinical Lipidology. (2011); 5(3 Suppl):S1-S8.
Raal FJ, et al. Circulation. (2011); 124(20):2202-2207.
Hoeg JM, et al. Atheroscler Thromb Vasc Biol. (1994);14(7):1066- 1074.
Taszner M, et al. 80th Eur Atherosclerosis Society Meeting. Milan, Italy. Abstract 1349
Rader DJ, et al. J Clin Invest. 2003;111:1796-1803
Raal FJ, Santos RD. Atherosclerosis. (2012); 223(2):262-268.
©2013 Aegerion Pharmaceuticals, Inc.
Patient with HoFH
•
•
•
•
28 year-old female
Cutaneous xanthomas beginning at age 3
Obstructive coronary artery disease and CABG at age 12
LDL cholesterol = 780 mg/dL
©2013 Aegerion Pharmaceuticals, Inc.
Clinical Characteristics FH
Corneal Arcus (<45yo)
Xanthelasma (<25yo)
Tendinous Xanthomas (any age)
HoFH Impact on the Patient
Consequences of Markedly Elevated LDL-C
in HoFH patients:
● Typically develop cardiovascular disease
before the age of 201
●
●
●
●
●
●
Coronary artery disease
Myocardial infarction
Severe aortic stenosis
Heart failure
Stroke
Sudden death
● Even with currently existing therapies,
the mean age of death is 33 years2
● Joint symptoms such as tendonitis or
arthralgias; unusual skin lesions - xanthomas
● Significant Unmet Medical Need
1. Goldstein, J. L. et al. (2001). The Metabolic and Molecular Basis of Inherited Disease.
2. Raal FJ, et al. Circulation. (2011); 124(20):2202-2207
©2013 Aegerion Pharmaceuticals, Inc.
LDL Apheresis is Current Recommended
Care for HoFH
Re-Priming
Solution
Heparin Pump
Regeneration
Solution
Regeneration
Pump
Blood Pump
Plasma Pump
Plasma
Separator
Blood Return
Schematic courtesy of D. Rader
Dextran sulfate
columns
Plasma Line
Waste Line
©2013 Aegerion Pharmaceuticals, Inc.
LDL-C Levels Decrease and then Rebound
Following Apheresis
Start of LDL apheresis
Baseline LDL
LDL CHOLESTEROL
Pre-treatment
LDL level
2-week
interval
Post-treatment
LDL level
TIME
Adapted from Thompsen J & Thompson PD. Atherosclerosis. 2006;189: 31-8.
©2013 Aegerion Pharmaceuticals, Inc.
New Lipid-Lowering Therapies
Approved in the US for Use in HoFH
Drug and dosage
Indication in HoFH
Lomitapide 1
Approved Dec 2012
5 mg orally, once daily- starting dose
Dose can be escalated gradually
based on acceptable safety and
tolerability
60 mg orally, once dailymaximum recommended dose
As an adjunct to a low-fat diet and other lipid lowering treatments, including LDL
apheresis where available, to reduce low-density lipoprotein cholesterol (LDLC), total cholesterol (TC), apolipoprotein B (apo B), and non-high-density
lipoprotein cholesterol (non-HDL-C) in patients with homozygous familial
hypercholesterolemia (HoFH).
Mipomersen2
Approved Jan 2013
200 mg subcutaneous injection
once weekly
Limitations of Use
• Safety and effectiveness have not been established in patients with
hypercholesterolemia who do not have HoFH;
• Effect on cardiovascular morbidity and mortality has not been determined
As an adjunct to lipid-lowering medications and diet to reduce low density
lipoprotein-cholesterol (LDL-C), apolipoprotein B (apo B), total cholesterol (TC),
and non-high density lipoprotein-cholesterol (non HDL-C) in patients with
homozygous familial hypercholesterolemia (HoFH).
Limitations of Use:
• Safety and effectiveness have not been established in patients with
hypercholesterolemia who do not have HoFH.
• Effect on cardiovascular morbidity and mortality has not been determined.
• Use as an adjunct to LDL apheresis is not recommended.
1.
2.
Juxtapid™ (lomitapide) capsules [US prescribing information]. Cambridge, MA: Aegerion Pharmaceuticals; 2012.
Kynamro™ (mipomersen sodium) Injection [US prescribing information]. Cambridge, MA: Genzyme Coorporation; 2013.
©2013 Aegerion Pharmaceuticals, Inc.
Microsomal Triglyceride Transfer Protein
(MTP)
• MTP is an intracellular lipid-transfer protein found in the lumen of the endoplasmic
reticulum (ER) responsible for binding and shuttling individual lipid molecules between
membranes1
• Normal concentrations and function of MTP are necessary for the proper assembly and
secretion of apo B-containing lipoproteins in the liver and intestines2
Intestinal
Epithelial Cell
Liver Cell
Cytoplasm
Cytoplasm
ER
ER
Lumen
MTP
1. Hussain M, et al. Journal of Lipid Research. 2003:44;22-32.
2. Liao W, et al. Journal of Lipid Research. 2003:44;978-985.
Lumen
MTP
©2013 Aegerion Pharmaceuticals, Inc.
MTP Inhibitors – Mechanism of Action
MTP inhibitors1,2
Prevent the assembly of apo B-containing
lipoproteins in hepatocytes and
enterocytes. This inhibits the synthesis of
VLDL and chylomicrons.
The inhibition of the synthesis of VLDL and
intestinal chylomicron
secretion lowers plasma lipids.
1. Wetterau JR, et al. Science. 1998:282;751-754.
2. Hussain MM, et al. Nutrition Metabolism. 2012:9;14.
©2013 Aegerion Pharmaceuticals, Inc.
Phase 2 Study Design
•
•
•
•
Single arm, open label study
16-week treatment duration - lomitapide as monotherapy (no background lipid-lowering
therapies)
Dose escalated from a low starting dose (mean doses at each of the four titration steps
were: 2.0, 6.7, 20.1, and 67.0 mg/day)
Low-fat diet (prescribed diet of <10% energy from fat)
6 Patients
Lomitapide
0.03 mg/kg
Lomitapide
0.1 mg/kg
Lomitapide
0.3 mg/kg
Lomitapide
1.0 mg/kg
Washout
4 weeks
4 weeks
4 weeks
4 weeks
4 weeks
Key Inclusion Criteria:
- Patients aged 18-40 yrs.
- Clinical Diagnosis of HoFH and one of the following
- documented functional mutation in both LDL receptor alleles
OR
- skin fibroblast LDL receptor activity <20% normal
OR
- TC >500 mg/dl + TGs <300 mg/dl + both parents with TC >250mg/dl
Cuchel, M. et al. NEJM 2007; 356:148-56.
©2013 Aegerion Pharmaceuticals, Inc.
Phase 2 HoFH Study: Efficacy
51% Reduction in LDL-C
51%
Reduction
p<0.001
Mean
Dose (mg):
2.0
6.7
20.1
67.0
Cuchel, M. et al. NEJM 2007; 356:148-56.
©2013 Aegerion Pharmaceuticals, Inc.
Antisense Oligonucleotides and
Apo B Synthesis Inhibition
Brautbar A and Ballantyne CM. Nat Rev
Mipomersen and LDL Lowering in
Homozygous FH
n=17
n=34
Baseline LDL-C: 405 mg/dl
200mg SC/Q week
Raal F. Lancet
What’s New in the Cholesterol Guideline?
1)
2)
3)
4)
5)
6)
Focus on ASCVD reduction: 4 Statin Benefit Groups
New Perspective on LDL-C and/or Non-HDL-C
Treatment Goals
Global Risk Assessment for Primary Prevention
Safety Recommendations
Role of Biomarkers and Noninvasive Tests
Future Updates to Guidelines
New Perspective
on LDL–C & Non-HDL–C Goals
• Lack of RCT evidence to support titration of drug
therapy to specific LDL–C and/or non-HDL–C goals
• Strong evidence that appropriate intensity of statin
therapy should be used to reduce ASCVD risk in
those most likely to benefit
• Quantitative comparison of statin benefits with statin
risk
• Nonstatin therapies – did not provide
ASCVD risk reduction benefits or safety profiles
comparable to statin therapy
Why Not Continue to Treat to Target?
Major difficulties:
1. Current RCT data do not indicate what the
target should be
2. Unknown magnitude of additional ASCVD risk
reduction with one target compared to another
3. Unknown rate of additional adverse effects
from multidrug therapy used to achieve a
specific goal
4. Therefore, unknown net benefit from treat-totarget approach
4 Statin Benefit Groups
Clinical ASCVD*
LDL–C >190 mg/dL, Age >21 years
Primary prevention – Diabetes: Age 40-75 years, LDL–C
70-189 mg/dL
Primary prevention - No Diabetes†: ≥7.5%‡ 10-year
ASCVD risk, Age 40-75 years, LDL–C 70-189 mg/dL,
*Atherosclerotic cardiovascular disease
†Requires risk discussion between clinician and patient before statin initiation.
‡Statin therapy may be considered if risk decision is uncertain after use of ASCVD
risk calculator.
4 Statin Benefit Groups (Revised Figure)
IA
IA
IB
IA
IIaB
1
Clinical Flow (Revised Figure-con’t)
Intensity of Statin Therapy
*Individual responses to statin therapy varied in the RCTs and should be expected to vary in clinical
practice. There might be a biologic basis for a less-than-average response.
†Evidence from 1 RCT only: down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (Pedersen et
al).
‡Although simvastatin 80 mg was evaluated in RCTs, initiation of simvastatin 80 mg or titration to 80 mg is
not recommended by the FDA due to the increased risk of myopathy, including rhabdomyolysis.
Primary Prevention
Global Risk Assessment
• To estimate 10-year ASCVD* risk
New Pooled Cohort Risk Equations
White and black men and women
More accurately identifies higher risk individuals
for statin therapy
Focuses statin therapy on those most likely to
benefit
You may wish to avoid initiating statin therapy in
high-risk groups found not to benefit (higher
grades of heart failure and hemodialysis)
*10-year ASVD: Risk of first nonfatal myocardial infarction,
coronary heart disease death, nonfatal or fatal stroke
Risk
Reduction
as Related
to 5-year
Risk
Categories
Cholesterol
Treatment
Trialists’
Collaboration,
The Lancet 2012
Primary Prevention
Statin Therapy
• Thresholds for initiating statin therapy
derived from 3 exclusively primary
prevention RCTs
• Before initiating statin therapy, clinicians
and patients engage in a discussion of the
potential for ASCVD risk reduction benefits,
potential for adverse effects, drug-drug
interactions, and patient preferences
• Calculators don’t write Rx, physicians do!
Individuals Not in a Statin Benefit Group
In those for whom a risk decision is uncertain:
These factors may inform clinical decision making:
•
•
•
•
•
Family history of premature ASCVD
Elevated lifetime risk of ASCVD
LDL–C ≥160 mg/dL
hs-CRP ≥2.0 mg/L
Coronary artery calcium (CAC) score
≥300 Agaston units
• Ankle brachial index (ABI)<0.9
Their use still requires discussion
between clinician and patient
Monitoring Statin Therapy
I IIa IIb III
Adherence to medication and lifestyle, therapeutic
response to statin therapy, and safety should be
regularly assessed. This should also include a fasting
lipid panel performed within 4 to 12 weeks after
initiation or dose adjustment, and every 3 to 12
months thereafter. Other safety measurements should
be measured as clinically indicated.
Optimizing Statin Therapy
The maximum tolerated intensity of statin should be
used in individuals for whom a high- or moderateintensity statin is recommended, but not tolerated.*
* Several RCTs found that low and low-moderate intensity statin therapy reduced
ASCVD events. In addition, the CTT meta-analyses of statin trials have shown that each
39 mg/dL reduction in LDL-C reduced CVD events by 22%. Therefore, the Panel
considered that submaximal statin therapy should be used to reduce ASCVD risk in
those unable to tolerate moderate- or high-intensity statin therapy.
Insufficient Response to Statin Therapy
I IIa IIb III
In individuals who have a less-than-anticipated
therapeutic response or are intolerant of the
recommended intensity of statin therapy, the
following should be performed:
Reinforce medication adherence.
Exclude secondary causes of hyperlipidemia.
Reinforce adherence to intensive lifestyle
changes.
Insufficient Response to Statin
Therapy (cont.)
It is reasonable to use the following as indicators of
anticipated therapeutic response to the recommended
intensity of statin therapy. Focus is on the intensity of
the statin therapy. As an aid to monitoring:
High-intensity statin therapy† generally results in an
average LDL-C reduction of ≥50% from the untreated
baseline; (recommendation cont. below)
†In those already on a statin, in whom baseline LDL-C is unknown, an LDL-C <100
mg/dL was observed in most individuals receiving high intensity statin therapy.
Insufficient Response to Statin
Therapy(cont.)
(recommendation cont.)
Moderate-intensity statin therapy generally results in
an average LDL-C reduction of 30 to <50% from the
untreated baseline;
LDL-C levels and percent reduction are to be used
only to assess response to therapy and adherence.
They are not to be used as performance standards.
Insufficient Response to Statin
Therapy (cont.)
In individuals at higher ASCVD risk receiving the
maximum tolerated intensity of statin therapy who
continue to have a less-than-anticipated
therapeutic response, addition of a nonstatin
cholesterol-lowering drug(s) may be considered if
the ASCVD risk-reduction benefits outweigh the
potential for adverse effects.
(recommendation cont. below)
Insufficient Response to Statin
Therapy (cont.)
Higher-risk individuals include:
Individuals with clinical ASCVD‡ <75 years of age
Individuals with baseline LDL-C ≥190 mg/dL
Individuals 40 to 75 years of age with diabetes
Preference should be given to nonstatin cholesterollowering drugs shown to reduce ASCVD events in
RCTs.
‡ Clinical ASCVD includes acute coronary syndromes, or a history of MI, stable or
unstable angina, coronary or other arterial revascularization, stroke, TIA, or peripheral
arterial disease presumed to be of the atherosclerotic origin.
Insufficient Response to Statin
Therapy (cont.)
I IIa IIb III
In individuals who are candidates for statin
treatment but are completely statin intolerant, it
is reasonable to use nonstatin cholesterollowering drugs that have been shown to
reduce ASCVD events in RCTs if the ASCVD
risk-reduction benefits outweigh the potential
for adverse effects.
Safety
• RCTs & meta-analyses of RCTs used to identify
important safety considerations
• Allow estimation of net benefit from statin therapy
o ASCVD risk reduction versus adverse effects
• Expert guidance on management of statin-associated
adverse effects, including muscle symptoms
• Advise use of additional information including
pharmacists, manufacturers prescribing information,
& drug information centers for complex cases
Management of Muscle Symptoms
on Statin Therapy
• It is reasonable to evaluate and treat muscle
symptoms including pain, cramping, weakness,
or fatigue in statin-treated patients according to
the management algorithm
• To avoid unnecessary discontinuation of
statins, obtain a history of prior or current
muscle symptoms to establish a baseline
before initiating statin therapy
Management of Muscle Symptoms
on Statin Therapy (con’t)
If unexplained severe muscle symptoms
or fatigue develop during statin therapy:
• Promptly discontinue the statin
• Address possibility of rhabdomyolysis
with:
CK
Creatinine
urine analysis for myoglobinuria
Statin-Treated Individuals
Nonstatin Therapy Considerations
Use the maximum tolerated intensity of statin
Consider addition of a nonstatin cholesterol-lowering
drug(s)
• If a less-than-anticipated therapeutic response persists
• Only if ASCVD risk-reduction benefits outweigh the
potential for adverse effects in higher-risk persons:
Clinical ASCVD <75 years of age
Baseline LDL–C ≥190 mg/dL
Diabetes mellitus 40 to 75 years of age
Nonstatin cholesterol-lowering drugs shown to reduce
ASCVD events in RCTs are preferred
Non-Statin Therapies
1) Ezetimibe – Additional 15% lowering of LDL-C –
No known benefit for reducing CVD events beyond
statin therapy – awaiting IMPROVE-IT clinical trial
2) Bile Acid Resins
3) Niacin
4) Fibrates (Fenofibrate)
5) Therapies for HoFH (Lomitapide, Mipomersin)
Emerging Therapies in Development
1) CETP Inhibitors (Anacetrapib and Evacetrapib)
2) PCSK9 Inhibitors
Three Principles
Do not focus on LDL–C or non-HDL-C
cholesterol
levels as treatment goals
o Lipid panel to monitor adherence
For those shown to benefit, use statins –
inexpensive (5 of 7 generic) medications proven to
reduce ASCVD risk
In primary prevention decisions, use a clinicianpatient discussion to determine:
global risk reduction strategy
potential for benefit and harms of statin therapy
Patient preferences (shared decision making)
Lifestyle management remains the
cornerstone for reducing
cardiovascular disease risk
including achieving and maintaining
optimal lipid levels
What’s New in Lifestyle?
Recommendations based on in-depth systematic
reviews. Previous reports used different methods
and structure. More depth, less breadth.
More emphasis on dietary patterns
More data provided to support
• saturated and trans fat restriction
• dietary salt restriction
Evidence to support dietary cholesterol restriction in
those who could benefit from LDL-C is
inadequate.
LDL-C: Advise adults who would benefit
from LDL-C lowering* to:
I IIa IIb III
Consume a dietary pattern that emphasizes intake of
vegetables, fruits, and whole grains; includes low-fat dairy
products, poultry, fish, legumes, nontropical vegetable oils
and nuts; and limits intake of sweets, sugar-sweetened
beverages, and red meats.
• Adapt this dietary pattern to appropriate calorie
requirements, personal and cultural food
preferences, and nutrition therapy for other medical
conditions (including diabetes).
• Achieve this pattern by following plans such as the
DASH dietary pattern, the U.S. Department of
Agriculture (USDA) Food Pattern, or the AHA Diet.
*Refer to 2013 Blood Cholesterol Guideline for guidance on who would benefit from
LDL-C lowering.
LDL-C: Advise adults who would benefit
from LDL-C lowering* to: (cont.)
I IIa IIb III
Aim for a dietary pattern that achieves 5% to 6%
of calories from saturated fat.
I IIa IIb III
Reduce percent of calories from saturated fat.
I IIa IIb III
Reduce percent of calories from trans fat.
*Refer to 2013 Blood Cholesterol Guideline for guidance on who would benefit from
LDL-C lowering.
Physical Activity
I IIa IIb III
Lipids:
In general, advise adults to engage in aerobic
physical activity to reduce LDL-C and non–HDL-C: 3
to 4 sessions a week, lasting on average 40 minutes
per session, and involving moderate- to vigorousintensity physical activity.
I IIa IIb III
BP:
In general, advise adults to engage in aerobic
physical activity to lower BP: 3 to 4 sessions a week,
lasting on average 40 minutes per session, and
involving moderate- to vigorous-intensity physical
activity.
……even modest weight loss (3-5% of body weight) can result in
clinically meaningful benefits for triglycerides, blood glucose,
glycated hemoglobin, and development of diabetes (type 2)….
Lipid Management
Recommendations
For all patients
I IIa IIb III
Start dietary therapy (<7% of total calories as saturated
fat and <200 mg/d cholesterol)
I IIa IIb III
I IIa IIb III
Adding plant stanol/sterols (2 gm/day) and viscous fiber
(>10 mg/day) will further lower LDL
Promote daily physical activity and weight
management.
Encourage increased consumption of omega-3 fatty
acids in fish or 1 g/day omega-3 fatty acids in capsule
form for risk reduction.
Therapeutic Lifestyle Changes
Nutrient Composition of TLC Diet
Nutrient
Recommended Intake
Saturated fat
Less than 7% of total calories
Polyunsaturated fat
Up to 10% of total calories
Monounsaturated fat
Up to 20% of total calories
Total fat
25–35% of total calories
Carbohydrate
50–60% of total calories
Fiber
20–30 grams per day
Protein
Approximately 15% of total calories
Cholesterol
Less than 200 mg/day
Total calories (energy)
Balance energy intake and expenditure
to maintain desirable body weight
Possible Benefits From Other Therapies
Therapy
Result
• Soluble fiber in diet (2–8 g/d)
(oat bran, fruit, and vegetables)
LDL-C 1% to 10%
• Soy protein (20–30 g/d)
LDL-C 5% to 7%
• Stanol esters (1.5–4 g/d)
(inhibit cholesterol absorption)
LDL-C 10% to 15%
• Fish oils (3–9 g/d)
(n-3 fatty acids)
Triglycerides 25% to 35%
Jones PJ. Curr Atheroscler Rep. 1999;1:230-235.
Lichtenstein AH. Curr Atheroscler Rep. 1999;1:210-214.
Rambjor GS et al. Lipids. 1996;31:S45-S49.
Ripsin CM et al. JAMA. 1992;267:3317-3325.
Dietary Adjuncts
TLC for patients with LDL-C = 160
Dietary Component
Low saturated fat/dietary cholesterol
Viscous fiber (10–25 g/d)
Plant stanols/sterols (2 g/d)
Total
LDL-C (mg/dL)
–12
–8
–16
–36 mg/dl
Walden CE et al. Arterioscler Thromb Vasc Biol 1997;17:375-382.
Jenkins DJ et al. Curr Opin Lipidol 2000;11:49-56.
Cato N. Stanol meta-analysis. Personal communication, 2000.
w-3 Fatty Acids Evidence:
Effect on Lipid Parameters
27 patients with hypertriglyceridemia and low HDL-C treated
with w-3 fatty acid (4 grams/day) for 7 months
Triglyceride
% Reduction
0
Total
Cholesterol
-10
-20
-21*
-30
-40
-50
-46*
HDL-C=High-density lipoprotein cholesterol
*P<0.05
Source: Abe Y et al. Arterioscler Thromb Vasc Biol 1998;18:723-731
w-3 Fatty Acids Evidence:
Primary and Secondary Prevention
Japan Eicosapentaenoic acid Lipid Intervention
Study (JELIS)
18,645 patients with hypercholesterolemia randomized to EPA (1800 mg)
with a statin or a statin alone for 5 years
Years
w-3 fatty acids provide CV benefit, particularly in secondary prevention
CV=Cardiovascular, EPA=Eicosapentaenoic acid
*Composite of cardiac death, myocardial infarction, angina, PCI, or CABG
Source: Yokoyama M et al. Lancet. 2007;369:1090-8
CONCLUSIONS
Many persons with normal total or LDL-C levels still
suffer CHD events.
While statin-based clinical trials significantly reduce risk
of CHD, residual risk still exists.
Non-HDL-C, which reflects all the atherogenic lipid
fractions, appears to be a stronger predictor of CHD
events than LDL-C.
The measurement of non-HDL-C and its use as a
secondary therapeutic target is warranted to better
address residual CHD risk.
Lifestyle therapies as well as pharmacologic
approaches, particular combination therapy with statins
and other agents, are important for optimizing the entire
lipid profile.