Peri-operative and Consultative Medicine
advertisement

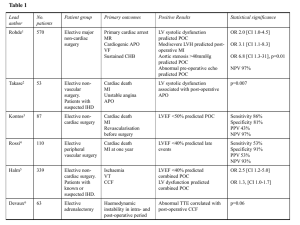
Perioperative and Consultative Medicine Pamela J. Pride MD, FHM Medical University of South Carolina 2/7/2012 Overview Role of consultant Cardiac risk assesment Perioperative beta blockade Preop pulmonary assesment and postop risk reduction Objectives Describe the risk factors for perioperative complication. Explain ACC risk stratification for surgery. Describe the evidence supporting prophylactic perioperative Beta Blockers. Use algorithms, when available, to assess and risk stratify patients. Reassess patients for postoperative complications and make medical recommendations when needed. Key Messages Limited role for routine preoperative coronary revascularization Perioperative beta blockers for high risk pts, need to be titrated Preoperative PFTs have limited role Role of the Consultant Evaluate and optimize patient’s medical status Treat modifiable risk factors Estimate and manage cardiac risk Recommend measures to attenuate all perioperative complications What Not to Do Recommend for or against surgery Tell anesthesiologists how to do their job Recommend the obvious “Clear” the patient Say nothing Pre-operative Cardiac Risk Assessment To Stress or Not to Stress ACC/AHA guidelines ACC Guidelines-Getting Started Define “Active Cardiac Syndromes” ACS HF (Class 4 or newly found) Significant arrhythmias (VT, symptomatic bradyarhythmias, rhythms requiring pacing, uncontrolled svts) Severe Valvular disorders (severe AS, symptomatic MS) ACC Guidelines-Getting Started Define “Clinical risk factors” Prior MI CKD Hx of CHF DM CVA ACC Risk Stratification for Surgery High: (cardiac risk >5%)-Emergency surgeries, aortic and major vascular, prolonged surgeries with large fluid shifts or blood loss Intermediate: (cardiac risk <5%)-CEA, ENT, intra peritoneal and intra thoracic, orthopedic, urologic Low: (cardiac risk <1%)-endoscopic, superficial, breast, cataract Metabolic Equivalents What is 4 mets? Walking 3 miles/hour, yoga, water aerobics Scrubbing floors, yardwork Carrying groceries in from car Competitive table tennis Dancing ACC Algorithm for Non-Cardiac Surgery American College of Cardiology Foundation, et al. J Am Coll Cardiol 2009;54:e13-e118 Copyright ©2009 American College of Cardiology Foundation. Restrictions may apply. Estimating Cardiac Risk Revised Cardiac Risk Index Circulation 1999;100:1043-1049 1. 2. 3. 4. 5. 6. High risk surgery History of CAD CHF CVA DM CKD # risk factors % complication 0…………………..0.4-0.5% 1…………………..0.9-1.3% 2……………………..4-7% ≥3……………………9-11% Perioperative Beta Blockers The Controversy Multiple early RCTs showed benefit The bandwagon rolls out AHRQ list ACC recommends ACP recommends More recent studies equivocal Perioperative Beta Blockade NEJM July 28,2005 Perioperative Beta Blockers The POISE Trial Lancet May 31, 2008 High risk pts undergoing non cardiac surgery Randomized to perioperative beta blockade vs. placebo Drug started hours before surgery and continued for 30 days post op Primary endpoints included cardiac death, nonfatal mi and non-fatal cardiac arrest The POISE Trial Results Poise Trial Results 6 5 4 Placebo metoprolol 3 2 1 0 30d nonfatal mi all cause mort cva Peri-operative Beta Blockers What should we do? Continue beta blockers for all pts on them chronically Start and titrate beta blockers preop for pts with Known CAD + ischemia on stress test High cardiac risk profile Unclear utility in pts with low cardiac risk profiles Do not use in absence of titration (goal hr 60-80) What about statins? Several observational studies suggest benefit from peri-operative statins. Randomised trials less clear Bottom line-prescribe only if statin is indicated regardless of surgery Preoperative Pulmonary Assessment and Postoperative Risk Reduction Patient Factors Advanced Age Poor functional status COPD CHF Tobacco abuse OSA Low albumin Surgical Factors Aortic, thoracic, upper abdominal Prolonged surgery General anesthesia Emergency surgery Routine NG tube placement Preoperative Pulmonary Function Testing Indicated for all lung resection patients Fail to consistently predict pulmonary complications Abnormal exam, CXR, and Goldman risk index more predictive Low rate of complications in patients with severe obstruction Use the “if they walked into my office” principle Evaluate unexplained dyspnea Establish baseline for patients with known lung disease Reducing Postoperative Pulmonary Complications Incentive Spirometry Selective NG decompression after general surgery Cigarette cessation* Medically optimize COPD Avoid sedating meds Neuraxial anesthesia Reference List Derivation and Prospective Validation of a Simple Index for Prediction of Cardiac Risk of Major Noncardiac Surgery . Circulation 1999;100:1043-1049 September 7, 1999 Perioperative Beta-Blocker Therapy and Mortality after Major Noncardiac Surgery. N ENGL J MED 2005; 353:349-361 July 28, 2005 Effects of extended-release metoprolol succinate in patients undergoing noncardiac surgery (POISE trial): a randomised controlled trial. Lancet, 5/31/2008, Vol. 371 Issue 9627, p1839-1847 Risk of Pulmonary Complications After Elective Abdominal Surgery Chest September 1996 110:3 p744-750 2009 ACCF/AHA Focused Update on Perioperative Beta Blockade Incorporated Into the ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery, J Am Coll Cardiol, 2009; 54:13-118