Physical Therapy Intervention for the Treatment of AIS
advertisement

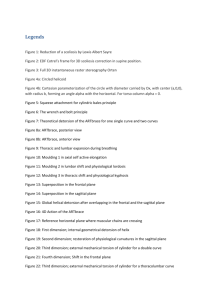
A 3-D Treatment Approach to Treating Scoliosis According to the Principles of C.L. Schroth Michelle Dwyer, DPT Schroth and SEAS Certified for the Treatment of Scoliosis and Spinal Deformities • Parents- Too much “wait and see” • Patients- Lack of knowledge regarding how to help themselves beyond bracing and waiting • Therapists- Inadequately educated and equipped in scoliosis treatment • Orthotists-Traditional bracing lacks 3-D corrections, resulting in flat back and other poor cosmetic changes • Doctors- Is there a way to help patients sooner? • • • • • Postural Awareness Stretching/ Strengthening Hip ROM Spinal Stability Body Mechanics • Schroth Based PT - Barcelona Physical Therapy School • SEAS - ISICO, Stephano Negrini MD, Milan, Italy • Team Approach PCP/ Pediatrician, Orthotist, Orthopedic/Neurosurgeon, Other? • Community Involvement Curvy Girls, Hope’s Closet, local meeting and support groups. • Primarily Adolescent Idiopathic Scoliosis Treatment • Deformities in the Sagittal Plane ( Scheurmann’s, Hyper-Kyphosis and Hyper- Lordosis • Curve Specific • Cognitive, sensory- motor, kinesthetic, neuromuscular exercises to reduce scoliosis posture History and Goals Correct scoliosis posture Germany 1921 Inpatient Spain 1968 Outpatient USA 2005 First certified therapists 2011 First US course held Steven’s Point, WI Reduce risk of progression Strengthen asymmetrically Improve respiration Diminish functional limitations Reduce pain Improve body mechanics Improve self image and quality of life Precautions: • Osteoporosis • Post- Surgery • Juvenile Hypermobility Syndrome (JHS) • Osteogenesis Imperfecta • Spondylolisthesis Contraindications: • Reactive Scoliosis (tumor, disease, etc) • Inflammatory diseases- during active phase • Psychiatric Issues May be treated but with limitations: • Syndromic and Neuromuscular Scoliosis • Post – Surgery • Adult Degenerative Scoliosis • Infantile (Age 0-3), Juvenile (age 4-9) * * SRS Classification Risk of Progression Factor Patient Age Risser Score Cobb Angle Age patient is first seen • • • • • • • • • Screening- Adam’s Test Angle of Trunk Rotation- (ATR) Using Scoliometer • >5 ° in sitting = + Screen Postural- Frontal, Sagittal and Aerial X- Ray- Cobb, Apex, Rotations, CSL, Risser Height Measurement – Sitting and Standing Vital Capacity Thoracic Function Pain Quality of Life – SRS 22, SRS 36, TAPS, QLSPD Schroth Exercises Semi-Hanging Sagittal Plane Prone on Knees-Transverse Plane Anterior Gravity Assisted Schroth Exercise Supine Gravity Assisted- Transverse Plane Standing 3D Correction Assessment Photos Assessment Photos In Brace Correction Pre/ Post Brace Comparison Pre Brace X-Ray In Brace X- Ray Sagittal Plane Correction Visit 1 Visit 3 Exercises Using Schroth Principles Exercises Using Schroth Principles Visit 1 - Uncorrected Visit 3 - Corrected Posture Exercises – Sport Specific and In-Brace Sport Specific Training In Corrected Posture Case Study Visit 1 Visit 1 Sagittal Visit 1 Visit 2 Sagittal Plane Correction Sagittal Correction Psoas Stretch Stretching- Stabilization Supine Hamstring Stretch Scapular / Core Stability Sagittal Correction Visit 1 Visit 6 - 2 month follow up Patient Follow Up Visit 1 2 Month follow up PT Treatment Options Local Program Basic Program 2x wk- 8wks Progression Monthly, Quarterly, Bi- Annually Until Risser 5 Immersion Program Basic Program for 5 consecutive days Progression First yr every 3 months Bi-Annually to Risser 5 Assistants