Grazie per aver scelto di utilizzare a
scopo didattico questo materiale
delle Guidelines 2011 libra.
Le ricordiamo che questo materiale è
di proprietà dell’autore e fornito
come supporto didattico per uso
personale.
New Treatment Options for Severe
Asthma
Modena, Italy
March 2011
Eric D. Bateman
MD, MBChB, FRCP, DCH
Professor of Respiratory Medicine, University of Cape Town
Director of University of Cape Town Lung Institute
Head, Division of Pulmonology, Cape Town
New Treatment Options for Severe Asthma
Outline
Defining the problem
Bronchodilators
• ICS/LABA and as-needed use
• Beta2-agonists (ultra-long acting)
• Anti-muscarinics
Anti-inflammatory drugs
• PDE4 inhibitors
• Inhaled corticosteroids
Bronchial Thermoplasty
Severe asthma requiring high intensity treatment
ATS / ERS Task Force Asthma Control and Exacerbations
Standardizing Endpoints for Clinical Asthma Trials and Clinical Practice
“Severe asthma is defined as the requirement for high intensity
treatment after modifiable factors and comorbidites have been
appropriately managed”
Good control on high
intensity treatment
Treatment
responsive, but
with persistent
problems e.g. poor
adherence,
smoking
Poor control despite high
intensity treatment
Persistent comorbidities e.g.
GE reflux, obesity
Treatment
resistant/
refractory asthma
Reddel H, et al, Amer J Resp Crit Care Med 2009;180:59-99
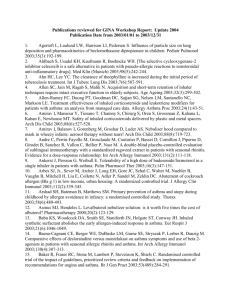
Levels of CONTROL achieved in GOAL
Total or Well Controlled* at 52 weeks
% of patients CONTROLLED
100
Fluticasone 500
Fluticasone 250
Salm/FP 500
Salm/FP 250
Fluticasone 100
Salm/FP 100
80
Relatively steroid-refractory?
Difficult to treat?
62%**
60
47%
40
20
0
Previously uncontrolled on
moderate doses of ICS
*GOAL definitions of control
**p<0.001 vs Fluticasone propionate
n = 1155
Bateman ED et al. Am J Respir Crit Care Med 2004; 170: 836–844
Patients (% per week) achieving GINA Controlled or Partly
Controlled weeks during Bud/Form M&R studies
Bud/Form M&R vs
Same-dose ICS/LABA
+ SABA1,3
Bud/Form M&R vs
High-dose ICS/LABA
+ SABA4,5
60
Controlled and Partly Controlled (%)
Controlled and Partly Controlled (%)
60
50
40
30
20
10
0
0
4
8
12 16 20 24 28 32 36 40 44 48 52 56
Week
Bateman ED et al, JACI 2010
50
56%
40
30
50% were on Salm/FP
50/500 b.i.d
20
10
0
0
4
8
12
16
20
24
28
Week
1. O’Byrne PM, et al. Am J Respir Crit Care Med 2005;171:129–136
2. . Rabe KF, et al. Lancet 2006;368:744–753
3. Kuna P, et al. Int J Clin Pract 2007;61:725–736
4. Bousquet J, et al. Respir Med 2007;101:2437–2446
Patients (% per week) experiencing exacerbations requiring
medical intervention
Higher-dose ICS/LABA
+ SABA vs Bud/Form M&R
Exacerbations in week (%)
Exacerbations in week (%)
Same-dose ICS/LABA
+ SABA vs Bud/Form M&R
3.6
3.2
2.8
2.4
2.0
1.6
1.2
0.8
0.4
0.0
3.6
3.2
2.8
2.4
2.0
1.6
1.2
0.8
0.4
0.0
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56
Week
50
40
30
20
10
Week
50
40
30
20
10
0
0
56
8 12 16 20 24 28
Increasing the dose of ICS
in the combination inhaler 60
Controlled and Partly
Controlled (%)
Controlled and Partly
Controlled (%)
60
4
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56
Week
Bateman ED et al, JACI 2010
0
4
8 12 16 20 24 28
Week
Ultra-long-acting (once daily) beta2-agonists
for asthma
•
•
•
*
*
Least squares mean FEV1
(L/min)
• Indacaterol
• Carmoterol
• Milveterol
• GSK-642444
• BI-1744-CL
• LAS-100977
• PF-00610355
1.5
*
*
1.4
1.3
1.2
Indacaterol Indacaterol Indacaterol Formoterol
300 µg
12 µg
600 µg
150 µg
(n = 49)
(n = 50)
(n = 50)
(n = 47)
Placebo
(n = 48)
BIG QUESTIONS
FDA requirements for safety studies
Exclusively in combination with ICS
What about as-needed use?
Cassola M, et al, Curr Opin Pulm Med 2010; 16: 6
New Treatment Options for Severe Asthma
Outline
Defining the problem
Bronchodilators
• ICS/LABA and as-needed use
• Beta2-agonists (ultra-long acting)
• Anti-muscarinics
Anti-inflammatory drugs
• PDE4 inhibitors
• Inhaled corticosteroids
Bronchial Thermoplasty
Tiotropium as Step-up Treatment in Asthma (TALC)
Trial design
**
*
* QVAR BDP 40µg b.i.d.
** Tiotropium HandiHaler ®
Peters S, et al, N Engl J Med 2010; 363: 1715
Tiotropium as Step-up Treatment in Asthma
TALC Study Demographics (n = 210)
Mild- moderate, reversibility and FEV1 >40% pred.
Less than 10 pack-years and non-smoking
Demographic feature
Value
Male sex (%)
33%
Atopy (one or more SPT +ve)
87%
Age (years)
42.2
FEV1 (pre-bronchodilator) (L)
2.31
FEV1 (post-b.d.)(L)
2.62
FEV1 (Pre-b.d.) % predicted
71.5
FEV1 reversibility (albuterol)
14.9
FEV1 reversibility (ipratropium)
12.4
Asthma control days (%)
21.2
ACQ (Total score)
1.64
Peters S, et al, N Engl J Med 2010; 363: 1715
Tiotropium as Step-up Treatment in Asthma (TALC)
Outcome variables
Morning PEF
Evening PEF
Pre-b.d FEV1 (L)
Asthma Control Days
(No./14 days)
Peters S, et al, N Engl J Med 2010; 363: 1715
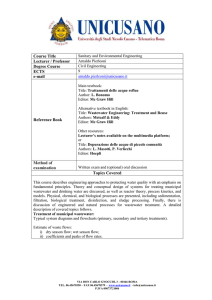
Tiotropium as Step-up Treatment in Asthma
Responder analysis: Asthma Control Days
50
Percentage patients
45
40
Overall response rates:
• Tiotropium
= 41.5%
• Salmeterol
= 44.5%
• Double dose ICS = 34.9%
38
35
30
25
20
17.5
15
11.4
10.2
10
5
7.4
5.4
4.8
0
Peters S, et al, N Engl J Med 2010; 363: 1715
7.2
5.4
New Treatment Options for Severe Asthma
Outline
Defining the problem
Bronchodilators
• ICS/LABA and as-needed use
• Beta2-agonists (ultra-long acting)
• Anti-muscarinics
Anti-inflammatory drugs
• PDE4 inhibitors
• Inhaled corticosteroids
Bronchial Thermoplasty
Roflumilast in Asthma
Inclusion criteria:
• Patients with chronic, stable asthma
• Age 15 to 70 years
• FEV1 50% and 85% of predicted value
• Reversibility FEV1 15% or PEF variability 15%
Run-in
period
Double-blind
Open-label extension
period
Roflumilast
500 µg/day
Placebo
2-agonist
p.r.n.
Roflumilast
250 µg/day
250 µg/day
Roflumilast 500 µg/day
Roflumilast
100 µg/day
100 µg/day
1-3
weeks
Randomization
12 weeks
40
weeks
Bateman ED, et al. Efficacy and safety of roflumilast in the treatment of asthma.
Ann Allergy Asthma Immunol 2006;96:679-86.
Roflumilast in asthma – a dose-ranging study
12-week study
Roflumilast
100, 250, 500 µg
40-week study
Roflumilast
500 µg
Patients (N)
693
456
Median age in years
(range)
40 (16 – 70)
42 (17 – 71)
Male / Female (%)
48 / 52
49 / 51
Mean FEV1 ± SD (L)
100 µg: 2.43 ± 0.61
250 µg: 2.38 ± 0.63
500 µg: 2.47 ± 0.68
2.79 ± 0.83
FEV1 ± SD (% predicted)
73 ± 9
85 ± 17
Previous ICS (%)
39.4
43.6
Smokers/Ex-smokers (%) 26
Bateman ED, et al. Ann Allergy Asthma Immunol 2006;96:679-86.
25
Roflumilast in asthma: FEV1
12-week, Dose-Ranging and 40 week extension study
*
400
300
*
*
200
100
0
100
250
Roflumilast (µg/day)
*p < 0.0001 for change vs baseline
LOCF analysis
1
500
100
Change vs baseline (L / min)
(LSMean and SEM)
Change vs baseline (mL)
(LSMean)
p = 0.0017
80
60
40
20
0
12
Bateman ED, et al. Ann Allergy Asthma Immunol 2006;96:679-86.
16
26
39
Time (weeks)
52 Endpoint
1
Roflumilast in COPD: Concurrent with ICS
M2-111 and M2-112 pooled post hoc analysis
Martinez FJ, Calverley PMA, Goehring UM, et al. COPD7 2010; abstract 12. Available at: www.copdconferences.org
Roflumilast in COPD: Concurrent with LABA
Pre-specified analysis of exacerbation rate in LABA subgroup
Hanania NA, Brose M, Larsson T, et al. Am J Respir Crit Care Med 2010;181:A4435. Abstract.
Bateman E, Calverley PMA, Fabbri L, et al. Eur Respir J 2010;36:P4003.
Roflumilast in COPD Concurrent with Tiotropium
Pre-bronchodilator FEV1
Post-bronchodilator FEV1
Fabbri LM, Calverley PMA, Izquierdo-Alonso JL , et al. Lancet 2009;374:695-703.
Bronchial Thermoplasty for Severe Asthma: AIR 2
Study design:
•
Randomised, double-blind, sham-controlled
•
•
2 active:1 control
Alair Bronchial Thermoplasty (Asthmatx)
Baseline
Follow-up
BT
BT
BT
Assess
3mo.
4 weeks
>3 weeks
Assess
6mo.
Assess
9mo.
Assess
12mo.
>3 weeks
N = 288 (ITT)
Castro M, et al, Am J Respir Crit Care Med 2010; 81 : 116
Bronchial Thermoplasty for Severe Asthma
Inclusion criteria:
•
•
•
•
•
•
•
•
•
•
Aged 18 – 65 years
ICS >1000g/day BDP or equiv. + LABA
Plus controllers: LTRA, omalizumab, OCS <10mg/day
Stable for 4 weeks
AQLQ <6.25
Pre-b.d. FEV1 >60% pred.
PD20 M <8mg/ml
Symptoms on 2 days in 28 days
Non-smoker for at least 12 months and <10 pack-years
Exacerbations: <3 hospitalizations, lower respiratory infections
and <4 OCS bursts in last year
Castro M, et al, Am J Respir Crit Care Med 2010; 81 : 116
Bronchial Thermoplasty for Severe Asthma
Demographics
BT (n=190)
Sham (98)
Age (years)
40.7
40.6
Sex (male)
57.4
61.2
PC20 Methacholine (mg/ml) geometric mean
0.27
0.31
Pre-bronchodilator FEV1 % predicted
77.8
79.7
ICS (µg/day) (mean)
1960
1834
AQLQ (mean)
4.30
4.32
% symptom-free days
16.4
16.8
Oral corticosteroids (%)
3.7
1.0
Methylxanthines (%)
3.2
5.1
LTRA (%)
24.7
18.4
Omalizumab (%)
1.1
3.1
Other maintenance medications
Castro M, et al, Am J Respir Crit Care Med 2010; 81 : 116
Bronchial Thermoplasty for Severe Asthma
Primary Endpoint : Change in AQLQ score over 12 months
6.0
Average score
*
5.80
5.71
*
AQLQ Score
▲
5.5
5.49
5.71
▲
■
5.48
▲ Bronchial Thermoplasty
N = 173
5.68
▲
■
■
5.40
■
5.56
Sham
N = 95
5.0
3 months
6 months
* Posterior probability of superiority = 95%
3 months
12 months
Castro M, et al, Am J Respir Crit Care Med 2010; 81 : 116
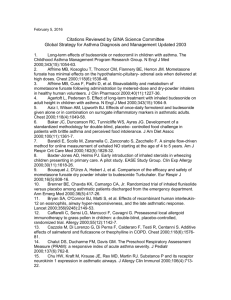
Bronchial Thermoplasty for Severe Asthma:
Primary Endpoint - % patients achieving change in AQLQ over 12 months
Bronchial Thermoplasty
Sham
100
*
90
80.9
Percentage of Subjects
80
Other conclusions:
70
•
63.2
60
•
50
40
•
29.5
30
16.2
20
10
Big placebo effect
Side-effects significant in first
week
Limited efficacy: no effect on
asthma control, rescue
use, ACQ, BHR,
7.4
2.9
0
< - 0.5
> - 0.5 to < 0.5
< 0.5
Change from baseline in average AQLQ Score
* Posterior probability of superiority = 100%
Castro M, et al, Am J Respir Crit Care Med 2010; 81 : 116
Bronchial Thermoplasty for Severe Asthma
Exacerbations and healthcare utilisation over 12 months
100
Bronchial Thermoplasty
Rate (Events/ subject/ yeear
90
Sham
80
*
70
60
50
*
40
30
16.2
20
10
0
7.4
Severe
exacerbations
Unscheduled
Physician Office
Visits
* Posterior probability of superiority = 95%
EU visits
Hospitalizations
Castro M, et al, Am J Respir Crit Care Med 2010; 81 : 116
Bronchial Thermoplasty for Severe Asthma
On the basis of the AIR2 data, does it make sense to offer
bronchial thermoplasty to patients with severe asthma?
For patients with uncontrolled asthma who have not been submitted
to a rigorous treatment protocol, the answer is no.
For the remaining patients, the AIR2 results might offer some hope.
...... benefit on the quality of life and severe exacerbations.
Severe asthma has many phenotypes , and at present we have no
clue which phenotype will benefit the most.
Long-term clinical and morphological research in various severeasthma phenotypes is still needed to obtain the required information
for clinical decisions
Bel E, Am J Respir Crit Care Med 2010; 81 : 116
New Treatment Options for Severe Asthma
Summary
Severe asthma remains difficult to treat
Several new treatment options are already available
Standardization of definitions and phenotyping will assist
the positioning of treatments
More trials testing various combinations are needed
Will the “Asthma cocktail” comprise ICS/LABA (once-
daily) and as-needed, anti-muscarinics, combinations of
anti-inflammatory drugs, and bronchial thermoplasty???