Christina Lewis, MN, RN, NP
Certified Dermatology Nurse
UCLA Arthur Ashe Student Health and
Wellness Center
May 31, 2012
1
Identify questions to review when presented
with a student that has a concern about
possible skin cancer
Compare and contrast the three most
common types of skin cancer
Explain how UV exposure can affect the skin
and how it may affect the Vitamin D levels of
the average college student
2
Skin cancer is the most common form of
cancer in the United States.
2003 there was more than one million new
cases of skin cancer in US and 9,800 will die
of the disease (Scarlett, 2003)
Incidence of skin cancer has doubled each
decade since the 1930’s (Wolf, 2003)
Who to screen? No randomized studies.
Discuss changes in behaviors with whom?
3
Increase to 75% proportion of persons who
use at least one protective measure that may
reduce risk of skin cancer:
◦
◦
◦
◦
avoid sun between 10-4
wear sun protective clothing
use sunscreen with SPF of at least 15
avoid artificial sources of UV light.
4
Family history of skin cancer
- Personal history of skin cancer
- Number of blistering sunburns in the
student’s lifetime
-Tanning bed use
-Where they grew up
-Changes to any area of the skin and when the
changes were noted. Including changes in
areas of past burns and keloids
-
5
Basal Cell-more common with intermittent
“recreational” exposure. Unclear if sunscreen
prevents BCC. Metastasis rate is less than 0.1%
Squamous Cell-more common with continuous
sun exposure such as outdoor workers. “regular
sunscreen can prevent SCC” (Lin, et al. 2003).
Metastasis rate is 2-6%
Melanoma-more common with intermittent
“recreational” exposure. Unclear if sunscreen
prevents melanoma (Lin, et al 2003)
6
7
8
9
10
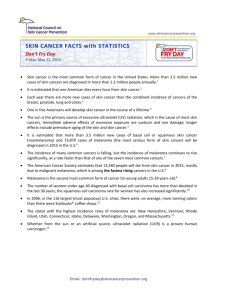
Dermnet images
11
Appears “black, pearly”
Pigmentation is present in >50%. Compared
to 5% in whites. (Bigler, et al, 1996)
BCC occurs most commonly after the 5th
decade (Maguire-Elsen, 2011)
12
13
Predisposing Factors
◦
◦
◦
◦
◦
◦
◦
◦
◦
◦
Precursor lesions (actinic keratosis, Bowen disease)
Ultraviolet radiation exposure
Ionizing radiation exposure
Exposure to environmental carcinogens- Arsenic,
Insecticides and herbicides, smoking/alcohol assoc with
oral SCC
Immunosuppression
Scars
Burns or long-term heat exposure
Chronic scarring or inflammatory dermatoses discoid
lupus, pilonidal cyst, hidradenitis superativa
Human papillomavirus infection (HPV 16-head and neck,
HPV 5)
Genodermatoses (albinism, xeroderma pigmentosum,
porokeratosis, epidermolysis bullosa)
14
15
Fitzpatrick Color Atlas
16
17
Surgical excision
Cryotherapy-97-99% cure rate in BCC
Mohs micrographic surgery
Topical chemotherapy (5-FU, interferon,
retinoids)
Systemic chemotherapy
Laser therapy
Electrodessication and Curettage
Curettage (for BCC only)
Photodynamic therapy-uses light, oxygen and a
photosensitizing chemical
18
• Different incidence, site distribution, stage
at diagnosis, and histological type. Acral
lentiginous melanoma is more frequent
(Cress, Holly, 1997)
Lower extremity:
◦ Hispanics-20%
◦ Asians-36%
◦ Blacks-50%
◦ Nonhispanic whites-9%
• Trunk is in all males but only in nonhispanic
whites among females. (Weir, 2011)
19
Male Hispanics in Florida had a 20% higher incidence
than male Hispanics in the U.S. Female Hispanics in
Florida had a lower rate than other areas of U.S.
Female Blacks had 60% higher incidence than the U.S
cohort. Total of 109,633 pts in study.(Rouhani, 2010)
Mucosa, palms, soles and nail beds are equally
frequent in whites and blacks and have remained
constant unlike melanomas in other body areas.
(Wolff, 2008)
Melanoma education to ethnic people may be
improved by using skin cancer photographs of early
melanoma in people with dark skin, providing
guidance on how to inspect hands and feet for
suspicious moles.(Robinson, 2011)
20
21
b
22
23
24
25
UV accounts for approximately 93% of skin
cancers (Gallagher, 2010)
UV light is addicting. UV light releases
endorphins
26
UVA penetrates the stratum corneum but is
poorly absorbed by DNA
◦ Has a longer wavelength
◦ Accounts for about 95% of UV rays that reach the earth
◦ More efficient than UVB in immediate and delayed
pigment darkening and delayed tanning. (Korak, 2011)
UVB-partially penetrates the stratum corneum
and is absorbed by DNA
◦ Primarily associated with erythema and sunburn
◦ Can cause immunosuppression and photocarcinogenesis
27
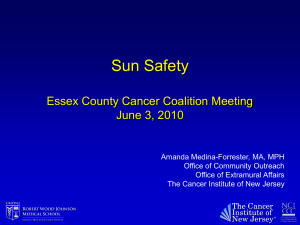
Ultraviolet
radiation
makes
chemical
change in
DNA
Change
in DNA
causes
mutation of
P53
Mutation
alters
function
of the
gene
Gene
function
leads to a
new cell
phenotype
DNA
UV
Mutation
lesion
Gene
The
abnormal
cell
expands
into a
clone
Cell
phenotype
The clone
becomes
the target
of further
DNA
damage
Clonal
expansion
Precancer or
carcinoma
28
◦
◦
◦
◦
◦
◦
◦
◦
◦
◦
◦
◦
Latitude
Altitude
Ozone-UVB
Season/cloudiness
Exposure time
Time of the day
Sunscreen
Shade
Tanning bed
Herbal preparations
Low fat diet
Behavioral Therapy
29
Latitudes above 35o have little UVB exposure
Squamous cell carcinoma appears to double with
each 8-10 degree decline in latitude
◦
◦
◦
◦
◦
◦
◦
◦
◦
◦
◦
Albuquerque, N.M.35
Birmingham, Ala.33
Bismarck, N.D.46
Boston, Mass.42
Charlotte, N.C.35
Chicago, Ill.41
Minneapolis, Minn.44
Nashville, Tenn.36
New York, N.Y.40
Philadelphia, Pa.39
Salt Lake City, Utah40
30
Affects UVB more than UVA
31
UVB is somewhat blocked by the ozone
32
In the summer, UVA is 96.5% of the UV rays
that reach the earth and UVB is 3.5%
Seasonal change accounts for about 1/5 of a
change in Vitamin D production (PerezLopez, 2010)
Clouds affect UVB more than UVA
33
High school white students who never wore
sunscreen when out in sun >1 hr, increased
from 57.5%to 69.4% from 1999-2009 (Jones,
2012)
34
UV is strongest between 10 am and 4 pm
2/3 of the UV radiation comes between 10
am and 2 pm
35
Used most common in women, less common
in black women. SPF 30 protects from 97% of
UVB
People in the U.S. only apply about 25% of the
recommended sunscreen (Thieden, et al,
2005)
Nambour (Queensland) sunscreen trial-first
randomized clinical trial with regular
sunscreen users and control group
36
17 approved agents in the U.S. (MaguireElsen, 2011)
Blocking sunscreen reflect UV rays
zinc oxide and titanium dioxide. Scatter
UV light. Good for sensitive skin, not skin
of color.
Chemical sunscreens absorb the UV rays
◦ Chemical sun blocks only block narrow regions of
the UV spectrum so they are used together. Most
block UVB.
37
“Broad spectrum” means UVA and UVB protection
Skin cancer/skin aging alert on sunscreens <15
Capped SPF value of 50+
“Sunblock”, “sweatproof”, and “waterproof” can not
be used.
◦ Clear time frames for “water resistant” (40 minutes)
and “very water resistant” (80 minutes)
◦ New Drug Facts box
◦ Will include “do not use on damaged or broken
skin”
◦
◦
◦
◦
38
UVA is not filtered by window glass (UVB is)
50% of exposure to UVA occurs in the shade
Shade use-most common in women-less
common in white women
Hat with brim, long sleeves
Clothing to the ankles-most common in men
Sunglasses with UV-absorbing lenses
Darker colors are slightly more protective.
◦ Plain white cotton T-shirt has about SPF 7
◦ Dark green T-shirt has about SPF 10
39
In the past, because UVA did not cause sunburn, only
tanning, it was not considered harmful to skin.
Tanning bed regular and early (high school and college)
use increases risk of skin cancer.
Tanning 4 times a year increases risk of non-melanoma
cancer by 15% and melanoma by 11% (Sun & Skin News,
2011)
One tanning session a year in high school increased risk of
BCC by 10%. (Zhang)
6.7% of high school males and 25.4% of females use
indoor tanning.(MMRW 2010)
WHO recommended minors be prohibited. 36 states have
put into law as of April, 2012.
No protective benefit to getting an artificial tan before
exposure to natural light (Miyamura, 2011)
40
Herbs and herbal preparations protect from
UV exposure generally through their
antioxidant activity
Plant peptides protect skin proteins (our
natural sun blockers). Topical application of
sesame oil blocks 30% of UV rays. Coconut,
peanut, olive and cottonseed oil block about
20%, mineral oil does not block UV.
41
Proanthocyanidin-grape seed (DNA mutation
inhibitor)
Resveratol -grapes, wine, cranberries,
peanuts
Quercetin-many fruits and vegetables-is the
most common flavonol
Apigenin-cumin, fruit, and vegetables
(carrots), marigolds
Silymarin-milk thistle
Curcumin-tumeric
42
Vitamin E-(tocopherol)-in wheat germ,
pumpkin seeds.
Vitamin C-rosehip seed extract
Carotonoids-(sea buckthorn, fruit oil [ie Avocado oil],
fish oil). Fish oil may increase sun protective effect in
some cases up to SPF 5.
43
◦
◦
◦
◦
◦
◦
◦
◦
Green tea and black tea
Aloe vera
Walnut extract
Krameria triandra (Kameria triandra root extract)
Borage oil
Evening primrose oil
Tea tree oil (increases blood flow only)
Porphyra (red algae)
44
Low fat diets. High fat diets shorten the time
between UV exposure and tumor formation
45
Behavioral counseling can increase sun
protection by decreasing:
◦ Indoor tanning
◦ Objectively measured pigmentation in college
students
◦ midday sun exposure
◦ increase sunscreen use in young adults
(Lin,2003)
46
Vitamin D insufficiency (range being 20 or
30) is common among:
Elderly
Institutionalized
Dark skinned
Wearing of protective clothing or consistent use of
sunscreen causing limited effective sun exposure
◦ Obese
◦ Malabsorption issues (Dawson-Hughes, 2012)
◦
◦
◦
◦
47
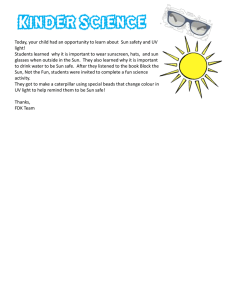
7-dehydrocholesterol
UV light
skin
Diet/supplements
Ergocalciferol (Vitamin D2)
Cholecalciferol
(Vitamin D3)
Liver
48
Grant (2009) supported sun exposure.
“Although a few thousand extra deaths per
year might occur from melanoma and skin
cancer, the avoided premature death rate
could be near 400,000/year.”
49
Recommendation for short (15 minute) sun
exposure, outdoor sport and leisure activities
is needed as a vitamin D rich diet generally
provides only about 10% of the needed
vitamin D (Perez-Lopez, 2010)
The difference in the sunlight can be made up
with supplements.
50
◦ Correlates with reduced risk of about 14 types of
cancer including Hodgkin lymphoma, colon, breast
and prostate cancer, and colon cancer
◦ Correlates with reduced incidence and/or mortality
rates of type 2 DM, coronary heart disease, and
congestive heart failure
51
International Agency for Research on Cancer
(IARC) concluded that data does not support
any form of intentional UV exposure
52
Uptodate recommends for high risk (dark
skin/sunscreen/protective clothes users)
measurement of serum 250HD is useful but
for regular low risk adults, suggest they take
600-800 iu/day
53
Main questions to review with patients:
◦ Family history of skin cancer
◦ Personal history of skin cancer or biopsies and
results
◦ Number of blistering sunburns in the patient’s
lifetime, tanning bed use
◦ Any changes or specific skin concerns the patient
has noted.
◦ Students of color, location and presentation of
melanoma.
54
Three most common skin cancer
◦ Basal cell
◦ Squamous cell
◦ Melanoma
55
Correlation of UV exposure and skin cancer
Sunscreen and other interventions to
decrease UV exposure (concern about
possible low Vitamin D)
56
Bigler, C et al. “Pigmented basal cell carcinoma in Hispanics” j am acad
dermatol 34:751-2.
Buller, DB, et al. “Prevalence of sunburn, sun protection and indoor
tanning behaviors among Americans: review from national surveys and
case studies in 3 states” j am acad dermatol. 2011, Nov,65(5 Suppl 1)
S114-23.
Center for Disease Control and Prevention. “Preventing Skin Cancer”
MMWR Morb Mortal Wkly. Oct 17, 2003, 52(RR15);1-12.
Center for Disease Control and Prevention. “Sunburn and Sun Protective
Behaviors Among Adults Aged 18-29 Years-United States, 2000-2012”.
MMWR Morb Mortal Wkly. May 11, 2012, 61(18); 317-322
Crest, R, Holly E. “Incidence of Cutaneous Melanoma among nonHispanic whites, Hispanics, Asians, and Blacks: an analysis of California
Cancer Registry Data 1998-1993” Cancer Cause Control. 1997
Mar;8(2):246-52.
Dawson-Hughes, B “Treatment of vitamin d deficiency in adults”
uptoDate 2012 www.uptodate.com.
Gallagher, RP, et al “Ultraviolet radiation” Chronic dis Can. 2010;29
Suppl 1:51-68.
Grant, W. “In Defense of the Sun” Dermatoendocrinol. 2009 JulAug:1(4):207-214.
Jones, SE, et al, “Trends in sunscreen use among us high school
students: 1999-2000” j Adolesc Health 2012 Mar,50(3):304-7.
57
Korac, R and Khambholia, K. “Potential of herbs
in/skin protection from Ultraviolent Radiation”
Pharmacogn Rev. 2011 Jul-Dec;5(10): 164-173.
Lin, JS, Ederm M. et al. “Behavioral counseling to
prevent skin cancer: Systemic evidence to review to
update the 2003 U.S. Preventative Services Task Force
Recommendation”
Maguire-Elsen, M. :”Food and Drug Administration’s
final ruling on sunscreens” Journal of the
Deermatology Nurses’ Association. 2011, October
3(5):255-9.
Miyamura, et al. “The deceptive nature of UVA
tanning versus the modest protective effects of UVB
tanning on human skin” Pigment Cell and Melanoma
Research. 24(1), 136-7
MMRW Surveill Summ 2010;59: 1-142)
Murphy, et, al. “Predictors of Serum Vitamin D levels
in African American and European American Men in
Chicago” Am J Mens Health. 2012 Mar 8.
58
Perez-Lopez, et al. “Vitamin D and adolescent health” Adolescent Health,
Medicine, and Therapeutics. 2010 (1):1-8.
Pichon, L, et al. “Measuring skin cancer risk in /African Americans: is the
Fitzpatrick skin type classification Scale Culturally Sensitive”. Eth Dis.
2010 Spring:20(2):174-9.
Porcia, T. “Skin Cancer in Skin of Color” Dematol Nurs. 2009 Julaug;21(4): 170-178.
Rouhani, P., et al. “Increasing rates of melanoma among nonwhites in
Florida compared with the United States” Arch Dermatol. 2010
Jul;146(7):741-6.
Robinson, et al. “Melanoma knowledge, perception and awareness in
ethnic minorities in Chicago: recommendations regarding education”
Psychooncology. 2011 Mar;20(3):313-20.
Scarlett, WL. “Ultraviolet radiation: sun exposure, tanning beds, and
vitamin D levels. What you need to know and how to decrease the risk
of sun cancer” J Am Osteopath Assoc 2003 Aug, 103(8)271-5.
Sun & Skin News. 2011, winter, 28(4). www.SkinCancer.org.
Thieden, et al. “Sunscreen use related to UV exposure, age, sex, and
occupation based on personal dosimeter readings and sun –exposure
behavior diaries” Archives of Dermatology. 2005, 141(8):967-973.
Weir, et al. “Melanoma in adolescents and young adults (ages 15-39
years): United States, 1999-2006” J Am Acad Dermatol. 2011 Nov;65(5
Spppl 1):S38-49
Wolff, et al. Fitzpatrick Dermatology, 7th edition, 2008. Chapter 112.
Carcinogenesis: ultraviolet radiation
59
American Academy of Dermatologywww.add.org
CDC.gov/cancers/skin
Sunwise program www.epa.gov
SkinCancerNet
www.skincarephysicians.com/skincancernet/s
kin_of_color.html
http://www.skincancer.org/skin-cancerinformation/basal-cell-carcinoma
http://www.dermnet.com/images/BasalCell-Carcinoma-Face/photos/2
60