44-SYMPATHETIC-OPHTHALMIA
advertisement

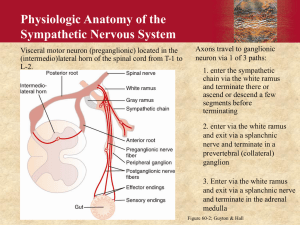
SYMPATHETIC OPHTHALMIA Dr.Rajesh Babu B MS, FMRF, MSc (CEH) DLSHTM, UK Consultant Uveitis & Ocular Immunology Ocular Epidemiology & Community Eye Health Narayana Nethralaya , Bangalore SYMPATHETIC OPHTHALMIA • • • • • • • • • • • • Definition Epidemiology Theories of pathogenesis Clinical manifestations Symptoms Examination findings Complications Pathology Differential diagnosis Fluorescein angiography findings Treatment Prognosis Definition • Sympathetic ophthalmia is defined as a bilateral granulomatous panuveitis that occurs after the uvea of one eye is subjected to a penetrating injury due to either accidental trauma or surgery. • The term “sympathetic ophthalmia” was coined by Mackenzie in the first half of the 19th century. Epidemiology • Incidence: – Prior to 1950 ~ 2% (16% during Civil War) – Retrospective studies: 0.2 - 0.5% after penetrating trauma and 0.01% after intraocular surgery. – Prospective study: 0.03/100,000 • Inheritance: No proven role. Postulated correlation of HLA DRB1, DQA1 reported in Japanese and UK series • Gender: M = F postsurgical; M > F traumatic • No racial predisposition • All ages, possibly increasing in the elderly Albert D, Diaz-Rohena R. A historical review of sympathetic ophthalmia and its epidemiology. Survey Ophthalmology 1989; 34: 1–14. Kilmartin D, Dick A, Forrester J. Prospective surveillance of sympathetic ophthalmia in the UK and Republic of Ireland . Br J Ophthalmology 2000; 84: 259–63. Prevalence • Difficult to measure because it has always been a relatively rare disease; as a result of improvements in modern surgical and medical treatment, it has become even more uncommon. • Changing Trends in Sympathetic Ophthalmia TREND HISTORICAL CURRENT Cause Post trauma Post surgery (esp. vitreoretinal) Patients Males and children (reflecting trauma peaks) No gender preference (reflects positive impact of injury prevention programs) and increasingly elderly patients (reflects impact of ocular surgery) Incidence Considered disappearing 30 years ago Probably increasing (under-diagnosed?) Onset For 65%, within 2-8 weeks; for 90% < 1yr Many delayed presentations as well Presentation Granulomatous panuveitis Any clinical uveitis Inciting Eye Enucleation within 2 weeks of trauma for prevention of SO Enucleation solely for the prevention of SO is questionable Visual Prognosis Poor Reasonable due to modern immunosuppression Theories of pathogenesis • It has long been thought that uveal pigment is somehow released by trauma and incites an inflammatory reaction. • Neurogenic (extension from one eye to the other through the optic nerves or via the ciliary nerves) • Infectious theory: tuberculosis, Actinomyces, Rickettsia, virus • Combined ciliary nerve and bacterial theories • Allergic or Anaphylactic theory: Autoimmunity against uveal melanin, uveal melanocytes, retinal pigment epithelium, or retinal antigens (S & IRBP) • Role of Ocular Immune Privilege Role of Ocular Immune Privilege • • • • • • Not all cases of ocular injury progress to SO Ocular immune privelege has a role to play Antigen released by the trauma induces ACAID An Immunosupressive Microenvironment Evolutionary protective mechanism Thwarts any process that endangers vision •Streilein JW (ed):Ocular Immune Privilege-Protection that preserves sight. Karger Gazzete. The eye in focus. No.64 http://www.karger.ch/gazette/64/streilein/index.htm accessed 1 Feb 2010 •Streilein JW (ed): Immune Response and the Eye. Chem Immunol. Basel, Karger, 1999, vol 73. Clinical manifestations • The interval between ocular injury and the onset of sympathetic ophthalmia has been reported to be as short as 5 days or as long as 66 years. • In general, 65% of sympathetic ophthalmia cases occur 2 weeks to 2 months after injury • 90% occur before 1 year. Clinical manifestations • The traumatized eye in SO, either from an accidental penetrating injury or following intraocular surgery, characteristically exhibits a persistent granulomatous inflammatory reaction. • SYMPTOMS • THE EARLIEST SYMPTOM MAY BE DECREASED ACCOMMODATION AND THE EARLIEST SIGN, RETROLENTICULAR FLARE AND CELLS IN THE FELLOW EYE. • • Irritable red eye with or without decreased vision. • Other symptoms include photophobia & transient hyperopia. • Cutaneous and neurologic changes (alopecia, poliosis, vitiligo, dysacousia, tinnitus, vertigo, and cells in the cerebrospinal fluid), which are classically associated with Vogt-Koyanagi-Harada syndrome, may rarely accompany SO. • On examination Bilateral granulomatous panuveitis: • Mutton fat keratic precipitates, • Cells and flare in the anterior chamber, vitreous cells, • Isolated or confluent patches of yellow-white choroidal infiltrates. • If undetected it eventually progresses to panuveitis with exudative retinal detachment. Dalen Fuch Nodules • Although not pathognomonic, are quite suggestive of SO and may indicate a more severe stage of SO. • Dalen-Fuchs nodules are small, discrete, yellowish infiltrates at the level of the RPE that are most often seen and are largest in the retinalchoroidal periphery. Complications • Extensive anterior and posterior synechiae, pupillary membrane formation. • Rubeosis, glaucoma, cataract • Papillitis, optic atrophy • Exudative retinal detachment, • Chorioretinal scarring, • Choroidal neovascularization, • Phthisis. Pathology • The inflammatory changes in the exciting and sympathizing eyes are the same, except for features of trauma in the exciting eye. • Granulomatous Uveitis – • The minimal and classic changes for the histopathologic diagnosis of sympathetic ophthalmia are diffuse lymphocytic infiltration of the uveal tract with epithelioid cell nests, pigment phagocytosis by the epithelioid cells, absence of necrosis, and sparing of the retina and choriocapillaris by the granulomatous process. CASELLA, Antônio Marcelo Barbante et al. Sympathetic ophthalmia - histopathological correlation with fluorescein and indocyanine green angiography: case report. Arq. Bras. Oftalmol. [online]. 2008, vol.71, n.6 [cited 2010-01-31], pp. 886-889 http://www.scielo.br/img/revistas/abo/v71n6/a25fig02.jpg • The uveal tract is usually diffusely thickened (massively in some) by an infiltration of lymphocytes in which various numbers of nests of epithelioid cells displaying pigment phagocytosis are present. Dalen-Fuch's nodules • • • • • Small, deep-yellow white lesions called Dalen-Fuch's nodules in the choroid. These nodules occur mostly in the periphery and consist of epithelioid cells located just internal to Bruch's membrane. Histopathologically they are nodular aggregations of lymphocytes and epitheloid cells with proliferation of retinal pigment epithelium. Dalen-Fuchs nodules are composed of a mixture of histiocytes, depigmented retinal pigment epithelial cells with lipofuscin and desmosomes, and small numbers of T lymphocytes of the suppressorcytotoxic subset THE CHORIOCAPILLARIS IS TYPICALLY SPARED. Eosinophils are a feature of sympathetic uveitis, especially in early cases. ATYPICAL PATHOLOGIC FEATURES – Focal nongranulomatous to diffuse nonnecrotizing granulomatous infiltrate – Focal choriocapillary involvement – Chorioretinal adhesions – Retinal detachment – Optic atrophy – Retinal perivasculitis – Mild inflammatory involvement of the meninges – Preferential anterior segment inflammation • Multiple areas of Early Hyperfluorescence and leakage at the level of the RPE (Dalen-Fuchs nodules) and the choroid (choroidal granuloma) in most cases, very similar to those seen in Harada's disease. • These sites (“window defects”) correspond to the Dalen-Fuchs nodules observed clinically. Presumably the hyperfluorescent or hypofluorescent nature in the early phase is determined by whether the Dalen-Fuchs nodules have an intact or a disrupted overlying RPE. FLUORESCEIN ANGIOGRAPHY If there is a serous retinal detachment, pooling of dye in the late frames of the angiogram can be observed. The FFA of the eye with inactive S.O will characteristically have scattered multiple window defects. CASELLA, Antônio Marcelo Barbante et al. Sympathetic ophthalmia - histopathological correlation with fluorescein and indocyanine green angiography: case report. Arq. Bras. Oftalmol. [online]. 2008, vol.71, n.6 [cited 2010-01-31], pp. 886-889 Hyperemic disc with blurred disc margins and tortuous dilated vessels Disc hyperfluorescence with blurring of margins in late phase (C and D) FFA showing multiple areas (encircled) of pinhead-sized leaks (arrow) Sampangi R, Venkatesh P, Mandal S, Garg SP. Recurrent neovascularization of the disc in sympathetic ophthalmia. Indian J Ophthalmol 2008;56:237-9 DIFFERENTIAL DIAGNOSIS • • • • • Vogt-Koyanagi-Harada syndrome Phacoanaphylactic uveitis Sarcoidosis Chronic idiopathic uveitis Other granulomatous uveitis induced by mycobacteria or fungi Differences between SO & VKH Sympathetic Ophthalmia Vogt-Koyanagi-Harada Syndrome Age All ages 20-50 years of age Racial predisposition None Asian and Black Penetrating trauma Almost always present Absent Skin changes Uncommon or unrelated Common (60-90%) CNS findings Uncommon Common (85%) Hearing dysfunction Uncommon Common (75%) Retinal serous detachment Uncommon Frequently seen Choriocapillaris involvement Usually absent Frequently seen CSF findings Usually normal Pleocytosis (84%) Treatment • Role of Enucleation of the Inciting Eye – Conventionally said to prevent SO if within 2 weeks of inciting event – Controversial whether enucleation is of benefit once SO develops • Pharmacological Therapy – Current: • Corticosteroids - oral, periocular, intraocular, topical • Steroid-sparing agents - Imuran, Cellcept, Cyclosporine A • Prophylactic steroids do not prevent sympathetic uveitis but can improve the visual outcome and can alter the histopathologic features. Prognosis • The relapsing nature of SO and the potential toxicity of treatment modalities warrant a careful long-term follow up of patients with this disease. • Spontaneous improvement rarely occurs and if left untreated, SO leads to loss of vision and phthisis bulbi. • The use of corticosteroid and other immunosuppressive agents together with the advancements in microsurgical techniques for wound repair have improved the prognosis of SO, • 50% of patients achieving a final visual acuity of 20/40 or better in at least 1 eye. • Cataract, secondary glaucoma, and chronic maculopathy are the major causes of visual loss. Thank You drrajeshbabu@yahoo.com