Dr.Melville PE/Backboard August Training
advertisement

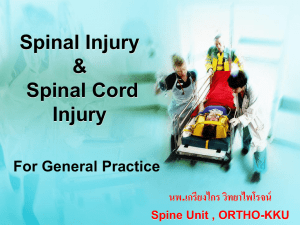
Procare Ambulance August Presentation Kraig Melville, MD, FACEP Pulmonary Embolism • Pulmonary embolism is a condition that occurs when one or more arteries in your lungs become blocked. In most cases, pulmonary embolism is caused by blood clots that travel to your lungs from another part of your body — most commonly, your legs • Globally more people die from PE than MI Pulmonary Embolism • Sources: – Lower: about 80-90% – Upper – Pelvis – Cardiac ventricle Pulmonary Embolism • Symptoms that should provoke a suspicion of pulmonary embolism: – – – – – – – – chest pain chest wall tenderness back pain, shoulder pain, upper abdominal pain Syncope Hemoptysis shortness of breath, painful respiration, new onset of wheezing any new cardiac arrhythmia any other unexplained symptom referable to the thorax. Pulmonary Embolism • The classic triad of signs and symptoms of PE (hemoptysis, dyspnea, chest pain) are neither sensitive nor specific. – occur in fewer than 20% of patients in whom the diagnosis of PE is made – most patients with those symptoms are found to have some etiology other than PE to account for them. – Of patients who go on to die from massive PE, only 60% have dyspnea, 17% have chest pain, and 3% have hemoptysis. Pulmonary Embolism Pulmonary Embolism Pulmonary Embolism • Treatment in the Ambulance – Oxygen – Pressure Support • IV fluids • Dopamine • (Dobutamine) – ?Aspirin – Avoid: NTG Cervical Spine Fracture in the Elderly • Mechanism: displacement may be anterior (hyperflexion) or posterior (hyperextension) – anterior displacement is associated with transverse ligament failure and atlanto-axial instability – posterior displacement by direct impact from the anterior arch of atlas during hyperextension (the “face plant”) Cervical Spine Fracture in the Elderly • Most common fracture of axis • Occur in bimodal fashion in elderly and young • patients elderly – common, often missed, and caused by simple falls – High risk due to fragility of bone – Canadian C-spine Rule lists age > or + to 65 as a high-risk patient Cervical Spine Fracture in the Elderly Cervical Spine Fracture in the Elderly Cervical Spine Fracture in the Elderly • Must maintain high level of suspicion and low threshold for spinal immobilization • Elderly patients difficult to clear by Nexxus Criteria – Dementia/ anxiety – High rate of distracting injuries – Medication effects Trauma Immobolization • Classic definition: – Rigid cervical collar, coupled with – Rigid backboard (note variation in type) Trauma Immobolization • Spinal immobilization can reduce untoward movement of the cervical spine and can reduce the likelihood of neurological deterioration in patients with unstable cervical spinal injuries following trauma. Immobilization of the entire spinal column is necessary in these patients until a spinal column injury (or multiple injuries) or a spinal cord injury has been excluded or until appropriate treatment has been initiated. While not supported by Class I or Class II medical evidence, this effective, timetested practice is based on anatomic and mechanical considerations in attempt to prevent spinal cord injury and is supported by years of cumulative trauma and triage clinical experience. • Source: ATLS Manual Trauma Immobolization • The variety of techniques employed and the lack of definitive evidence to advocate a uniform device for spinal immobilization, make immobilization technique and device recommendations difficult. It appears that a combination of rigid cervical collar with supportive blocks on a rigid backboard with straps is effective at achieving safe, effective spinal immobilization for transport. • Source: ATLS Manual Trauma Immobolization Trauma Immobolization • DO the right thing – If no contraindication, collar and back-board – Ask for written order – Avoid conflict: board them in the ambulance