New Technologies for Rapid
Diagnosis of MDR TB:
Lab and Clinical Perspective
Gisela Schecter, TB Branch, CDPH
Grace Lin, MDL, CDPH
5-6-10
CTCA Annual Meeting
Long Beach
1
Outline
Case study: Rapid detection of MDR TB and
rapid initiation of appropriate therapy
Discussion of molecular methods
molecular beacons (MB)
• Test principle
• Performance characteristics of MB
Line probe assays
New CDC MDDR service
How to submit samples and turnaround time
2
Outline (2)
Review of indications for requesting MB
Impact of MB on TB patient management
Case study: Discrepant results of MB and
DST
Case study: Illustrate usefulness of MDDR
service
Discussion of silent mutations, mutations that do not
confer resistance
MDDR reporting (how to interpret the report)
Case study: Low level rifampin resistance
(advanced usage of MB)
3
Case 1
21 y/o Filipina woman with Type I DM recently
arrived from the Philippines
No TB screening at the time of immigration
History of treatment for TB with INH +/- RIF as a
child and, more recently, with INH, RIF, PZA
and EMB given by SAT the previous year
Presented with cough X 6 months, progressive
SOB/DOE x 6 weeks, pleuritic chest pain and
fever to 101 degrees
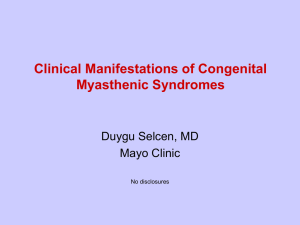
CXR and Chest CT were done
4
Case 1
5
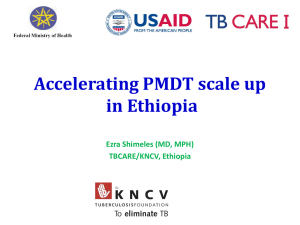
Case 1
6
Case 1
7
Case 1
Three
sputum specimens were AFB
smear positive and the patient was
begun on RIPE
Sediment was immediately sent for
molecular beacon (MB) testing
MBs found mutations conferring both
INH and RIF resistance
8
Case 1
Within 7 days of the first positive smear, the
patient was placed on:
Amikacin 870 mg IV five times weekly,
Moxifloxacin 400 mg po qd,
Cycloserine 500 mg po qd,
PAS 4 gm po bid,
EMB 15 mg/kg po qd,
PZA 25 mg/kg,
Vitamin B6 50 mg po BID
9
Case 1
Phenotypic susceptibility results showed
resistance to all first-line drugs and SM
EMB and PZA were discontinued and
linezolid added
Clinically did well and smear-converted
within 6 weeks
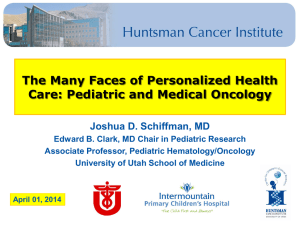
Repeat CXR 8 weeks later
10
Case 1
11
Case 1
Because
of the availability of a rapid test
for INH and Rifampin susceptibility, this
young woman was able to begin effective
therapy within days of TB diagnosis.
Infected contacts were not placed on
ineffective drugs
Appropriate isolation was maintained
12
Molecular Beacon Assay
(at MDL)
Target:
DNA
Realtime PCR
PCR to amplify target sequences
At the same time, Molecular beacon probes are
used to detect INH and RIF resistance mutations.
• 2 MBs for INH (targeting katG & inhA)
• 3 MBs for RIF (targeting core of rpoB)
13
Real-Time PCR
2 components
PCR to amplify target sequences.
A system to monitor PCR product.
• Fluorophore-labeled probes
• An optical device to detect fluorescence
• Software to record data
iCycler
IQ5
No post-PCR manipulations
Fast
• when PCR is done, results are ready for
interpretation.
No amplicon contaminations
14
What is a Molecular Beacon?
Hair-pin structure
Loop (15-30 nt)
Stem (5-7 nt)
Fluorophore
Quencher
15
Detection of Mutations with a Molecular Beacon
(Loop portion containing wildtype SQ)
Mutant Sequence
Wildtype Sequence
+
Amplicon
Loop
Fluorophore
Fluorophore
Heat
Molecular
Beacon (off)
Courtesy of Dr. Probert
Quencher
Light
Hybrid (Molecular Beacon - On)
16
An Example of a Good MB
No mutations,
Susceptible
R
F
U
Threshold
Mutant,
Resistant
17
MB Data from the Initial Study
Phenotypic Results
Resistant
Susceptible
Mutations detected
105
0
No Mutations detected
22
69
RIF
Mutations detected
No Mutations detected
79
2
0
69
INH
18
MB Performance from the Initial Study
Sensitivity Specificity
PPV
NPV
INH
10% Resistance 82.67%
100%
100%
98.11%
RIF
2% Resistance
100%
100%
99.95%
97.53%
19
Data for INH
3 years after implementation
INH
Cultures & sediments
Combined data (186)
MB
Phenotypic results
R
S
Mutation detected
44
1
No mutations
6
129
Inconclusive
2
4
20
Data for RIF
3 years after implementation
RIF
Cultures & sediments
Combined data (186)
MB
Phenotypic results
R
S
Mutation detected
36
5
No mutations
0
139
Inconclusive
2
4
21
MB Performance (3-year data)
(Agreement between MB and phenotypic drug results)
INH
RIF
Cultures
98.4%
99%
Sediments
93.6%
94.9%
Overall
96.1%
97.2%
22
Drug Resistance Detected by MBs
(3 years)
INH-R
RIF-R
MDR
Sediments
22.9%
16.9%
14.5%
Cultures
24.3%
21.4%
15.5%
Overall
23.7%
19.4%
15.1%
23
Limitations
Limited genes & sites are targeted.
•
Some mutations are not detected.
Emerging resistance in mixed populations may not
be detected.
Some mutations do not confer resistance.
•
•
•
Rare occurring, but lead to wrong interpretation.
Silent mutation in rpoB: codon 514.
Not a silent mutation but only cause little change in MIC.
Available for INH and RIF only.
New MBs for other drugs not developed yet.
Phenotypic drug susceptibility testing is still needed.
24
Line Probe Assays
Target:
DNA
Traditional PCR (not realtime)
Amplify target sequences.
Reverse
hybridization
Amplicons hybridize to probes immobilized on
membrane (strip).
Colorimetric
detection of captured amplicons
on strip.
Observation of bands. One probe for one band.
25
Line Probes
Hybridization
and colorimetric detection
Amplicons bind to probes
Color reaction to form bands
26
MTBDR by HAIN Lifescience
Conjugate ctrl
MTBC
Universal ctrl
LiPA RIF.TB by
INNOGENETICS
marker line
MTBC
rpoB universal ctrl
rpoB wild-type, 5
segments
516
526
531
4 rpoB mutations
katG universal ctrl
katG wild-type
315
2 katG mutations
More probes are added in MTBDRsl to detected 2nd-line drug R-mutations.
27
Line Probes Features
Many controls; more objective
MTBDRsl (HAIN) added embB, gyrA, rrs (screen
for XDR).
Exact mutations are available for most prevalent
mutations only.
Some mutations are detected by lacking bands in
wild-type sequences.
Emerging resistance in mixed populations may not
be detected.
Phenotypic drug susceptibility testing is still
needed.
28
CDC MDDR
(Molecular Detection of Drug Resistance)
DNA sequencing
Loci examined are:
Amplify target SQ by PCR
Cycle sequencing
Line up SQ by sequencer
For INH: katG, inhA promoter—same as for MB.
For RIF: rpoB—same as for MB
For quinolone: gyrA
For aminoglycosides & Capreomycin: rrs, tylA, eis
promoter
CDC accepts cultures only
Growth from liquid or solid media.
MDDR
Criteria for submission:
Known MDR, screen for XDR.
Contact of MDR.
Advantages
Detect mutations associated with:
• quinolone and aminoglycoside/cyclopeptide drugs
Results will show mutations
• MB detects mutations, but does not know what mutations.
Disadvantages
Need to wait till culture grows; 2-3 weeks of wait time.
30
31
CDC MDDR Report
Interpretation
The report states the % of R-strains studied at CDC
having mutations in each locus.
Examples:
gyrA, no mutation,
• Cannot rule out fQ-R (86% of fQ-R isolates have a mutation at
this locus).
rrs, no mutation,
• Cannot rule out R to injectable drugs. (58% of KM-R and 88%
of AK-R have a mutation in rrs locus).
rpoB, mutation: TCG>TTG Ser531Leu
• RIF-R (100% of 254 isolates with this mutation are RIF-R)
32
Specimen type & submission
Assay
Specimen
type
Where
TAT
MB
Culture
sediment
MDL
LA
1-3 days
(Median: 1 day)
MDDR
Culture
CDC
1-3 days
Hain
Lipa
Culture
Sediment
Florida
2 days?
33
Who Is At Higher Risk of MDR-TB?
(And Needs MBs obtained)
History of previous TB treatment, particularly
if recent
Foreign-born patients from countries or
ethnicities with high prevalence of MDR
Hmong refugees
Tibetan ancestry
Cases from former USSR, China, Korea, Peru,
Honduras are disproportionately MDR
34
Who Is at Higher Risk of MDR-TB?
(And Needs MBs obtained) (2)
Poor response to standard 4-drug treatment
Culture remains (+) after 2 months treatment
Known exposure to MDR-TB case
Recent arriver (<1 year in US)
HIV (+)
Higher incidence of Rifampin mono resistance
35
History of Prior TB Treatment
RVCT Data 2005-2009
166
MDR-TB cases reported
29.5% had hx of previous TB disease
644
culture (+) cases had a history of prior
TB disease
623 had DST to I/R
7.7% had MDR-TB
36
High incidence countries
of origin and ethnicities
RVCT Data 2005-2009
Hmong:
20.8% MDR-TB
Former Soviet Union: 7.5% MDR-TB
Laos: 12.5% MDR-TB
China, Korea, Guatemala: 2-2.5% MDR
Mexico and PI: < 2% MDR-TB
Recent arrivers: 2.7% MDR-TB
37
HIV/AIDS
Data is from the TB/AIDS registry match, 2001-2007
Mono INH
Resistant
Mono Rif
Resistant
MDR
TB without HIV
coinfection
TB with HIV
coinfection
1,338 (8%)
67 (7%)
32 (0.2%)
9 (0.9%)
227 (2%)
10 (1%)
38
Contacts and Treatment Failures
Not
captured in RVCT surveillance
Examples:
Day laborer with MDR TB.
• 3 contacts with active disease found over 1 year span.
All with MDR TB, same strain.
Older woman with DM,
• unreported vomiting after meds due to gastroparesis.
• Still culture positive at 5 months, now with MDR TB.
39
Impact of MB testing
The
median time to beginning an MDR
regimen for patients with MDR TB was 41.5
days earlier when MBs were obtained.
Total treatment duration and time to culture
conversion were both shorter when MBs
were used.
When MDR TB was NOT present, patients
were spared from an expanded MDR
regimen.
40
Any problem
with MB testing?
41
Case 2
45 year old man from PI with poorly controlled
diabetes.
History of 2 previous episodes of TB in the PI,
treated by SAT.
Presented with mild, persistent cough
Sputum was AFB smear +.
Molecular Beacons were ordered and showed
Rifampin resistance mutations but no INH
mutations were seen.
42
Case 2
Because
isolated Rifampin resistance is
unusual without HIV infection, the patient
was begun on an MDR TB regimen.
Surprise!
Phenotypic DST results showed INH and
PZA resistance, and Rifampin sensitivity.
How often does this happen?
43
INH-R detection Rate
Genes
katG, inhA, ahpC, ndh, etc.
About 85-90%
katG
associated with INH resistance
& inhA promoter
In California: 83%
With a 10% INH-R rate, when no mutations
detected by MB or MDDR, the likelihood that
the isolate is INH-S is about 98%.
RIF-R Detection Rate
Genes associated with RIF-Resistance
rpoB: >96%
In CA, we detected about 97.5%
With 1.5% RIF-R, when MB or MDDR does not
detect mutation, the chance for RIF-S is >99.9%.
BUT, some mutations do not confer resistance.
It is rare, but it exists.
Silent mutation does not confer resistance.
• An MB was designed to detect 514 silent mutation. Less a
problem now.
Few mutations in rpoB do not confer resistance.
45
Some mutations in rpoB
associated with RIF resistance
MB 531 (59.3%)
MB 516 (12.3%)
MB 526 (28.4%)
GAGCCAAT T CAT GGACCAGAACAACCCGCT GT CGGGGT T GACCCACAAGCGCCGACT GT CGGCGCT GGGG
513 514
516
522
526
531
533
AAA K
GTC
V
TTG L
T AC Y
TTG L CCG P
CCA P
T AC Y
CTC L
T GG W
CTA L
GAG E
AAC N
CCG
GAC D
GCG
TTT F
CGC R
TTC F
GGC G
T GT C
CCC P
CAA Q
T GC C
Most common mutations
TCG531TTG (S531L)
CAC526TAC (H526Y)
GAC516GTC (D516V)
Silent mutation
TTC514TTT
(F514F)
Mutations not confering resistance
(MDL findings)
CTG533CCG (L533P)
CAC526AAC (H526N)
46
What Happened to Case 2
It’s a bad combination that can happen in MB testing
No mutations detected in katG and inhA promoter.
Mutations occur somewhere that MBs do not target.
A mutation in rpoB was found, which was in codon 526
(CAC to AAC).
• MB detected a mutation, but did not know which mutation.
• It happened to be the one that does not confer resistance.
• It occurred 2X. Add a new MB to detect this mutation?
47
Case 3
22
year old Peruvian woman, Class B1
immigrant
Hx of previous treatment
Left upper lobe resection for MDR TB in Peru
Second line meds (Kanamycin, Ofloxacin,
PAS, Cycloserine and Ethionamide) for 18
months
Smear
negative, but culture +
48
Case 3
Is
this patient at risk for XDR or pre-XDR?
49
Case 3
Is
this patient at risk for XDR or pre-XDR?
Yes
Is this a candidate for CDC’s MDDR
service?
50
Case 3
Is
this patient at risk for XDR or pre-XDR?
Yes
Is this a candidate for CDC’s MDDR
service?
Yes, patient has seen both an injectable
drug and a quinolone.
We need to know if she has mutations that
confer quinolone and injectable resistance
51
Case 4
35
year old Hispanic man with extensive
bilateral cavitary, smear positive
tuberculosis
Initially did not give hx of prior TB rx
Begun on RIPE, but DST at county lab
showed Res to INH and PZA, with “some
growth” in the Rif MGIT tube
Now hx of extensive prior TB rx elicited
Culture sent to MDL for MBs
52
Case 4
Mutations
for both Rifampin and INH
resistance detected (rpoB and katG).
MDR TB Regimen begun but including
Rifampin.
53
Case 4
Summary of Susceptibility Results
Lab
INH
Rif
EMB
PZA
County
R: 0.1
R: 0.4
S: 1.0
“Some growth”
S: 5.0
R: 100
S: 5.0
R: 100
MDL MBs katG +
CDC
R: 0.2
R: 1.0
rpoB +
(detected by MB 516)
Rifampin: 1.0 50%
growth
Rifabutin: Susc.
54
Mutations Associated with
RIF Resistance
MB
assay detects 97.5% RIF-R:
MB 531 (529-534)—59.3%
• most common: S531L (ser to leu)
• RIF MIC: >64 g/ml
MB 526 (523-529)—28.4%
• Most common: H526Y (his to tyr)
• RIF MIC: >64 g/ml
MB 516 (511-518)—12.3%
• Most common: D516V (asp to val)
• RIF MIC lower than that of S531L & H526Y.
55
Rifamycins
Rifamycins
Rifampin (RIF)
Rifapentine (RFP)
Rifabutin (RFB)
Cross-resistance:
Very common
• with most prevalent mutations (S531L, H526Y, etc)
Less common
• with mutations in 511,516, 519, etc
• RFB has higher potency than RIF & RFP
References:
JAC, 1995;35:345-348
AAC, 1998;42:1853-1857
56
Rifampin-R but Rifabutin-S
7
cases identified.
122 RIF-R isolates, 73 tested with RFB.
• Rate for RIF-R but RFB-S: 5.7-9.6%
• Disclaimer: review of existing data, not a study.
Cross resistance between RIF & RFB is
very high (90-94%).
57
Mutations Detected for the 7 Cases
Found to Be RIF-R but RFB-S
Case
#4
Wild-type Codon
Mutant
Amino acid changes
GAC (D)
516
GTC (V)
Aspartic acid to valine
GAC (D)
516
GTC (V)
Aspartic acid to valine
GAC (D)
516
TTC (F)
Aspartic acid to
phenylalanine
CAC (H)
526
CTC (L)
Histidine to Leucine
RIF MIC=2
CAC (H)
526
CTC (L)
Histidine to Leucine
CAC (H)
526
GGC (G)
Histidine to Glycine
AAG (K)
527
AGG (R)
Lysine to arginine
58
Can MB Assay Predict RFB-S?
Predictive values have not established.
MB516 detects mutations btwn 511-518.
RBF may test S with mutations: D516V, D516Y, etc.
• Are strains with those mutation always S to RFB? NOT KNOWN.
• Shall we do RIF MIC? (RFB testing not available at MDL).
MB531 detects mutations btwn 529-534.
S531L confers high RIF-R. Cross-R to RFB anticipated.
MB526 detects mutations btwn 523-529.
H526Y—2nd most frequent mutation in rpoB with high MIC.
Other mutations in 526 may confer low RIF-R or not confer
RIF-R. Low frequency; exact prevalence not surveyed.
59
Conclusions
MB is useful for MDR screening, can be done on a smear +
specimen, has a fast turnaround time, and is cost-effective.
95-97% agreement with phenotypic DST
When mutations not detected, it provides confidence for using RIPE to
treat.
When mutations detected, proper treatment and prophylaxis can be
initiated in a timely fashion.
If pre-XDR or XDR is suspected, MDDR service is valuable with
excellent TAT. But, need to wait till cultures grow.
A study may be warranted to investigate clinical efficacy for low level
RIF resistance, since RIF is essential to short course therapy.
When a mutation is detected by MB 516, it may be useful to test RIF
MIC. If MIC is low (<=4), RIF or RFB may have clinical efficacy?
60
 0
0