Targeting HER family receptors
in breast cancer
Prof. Sabino De Placido
Dip. di Endocrinologia ed Oncologia Molecolare e Clinica
Università Federico II --- Napoli, Italia
Targeting HER2: Key points
HER2 gene amplification and/or overexpression
occurs in about 20% of breast cancers and is
associated with more-aggressive disease and, until
the advent of HER2-targeted agents, a worse outcome
The monoclonal antibody, trastuzumab (which targets
HER2), and the small molecule tyrosine kinase
inhibitor, lapatinib (which targets HER1 and HER2),
have considerable efficacy in HER2-positive breast
cancer
Adjuvant Setting
What we know
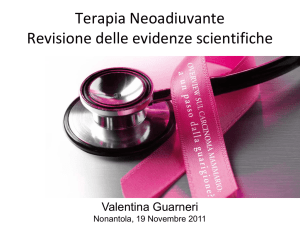
Trastuzumab has changed the
natural history of early HER2+ BC
Adjuvant Trastuzumab predicted to prevent
recurrence in almost 28,000 patients over a
10-year period in the 5 major EU countries
Patients, 20,000
n
18,000
No. of patients prevented from developing metastases
Incidence of MBC without Herceptin
Herceptin introduced
16,000
14,000
27,737
12,000
10,000
8000
6000
4000
2000
0
2000
2005
2010
2015
Year
Weisgerber-Kriegl et al, ASCO 2008
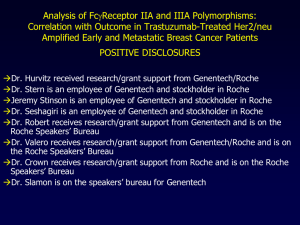
More than 14.000 patients were recruited
in 4 international clinical trials
HERA (ex-USA)
BCIRG 006 (global)
Observation
IHC / FISH
(n=5,090)
FISH
(n=3,222)
1 year
1 year
2 years
1 year
NCCTG N9831 (USA)
IHC / FISH
(n=3,505)
NSABP B-31 (USA)
1 year
IHC / FISH
(n=2,030)
1 year
1 year
Standard CTx
Doxorubicin +
cyclophosphamide
IHC, immunohistochemistry
FISH, fluorescence in situ hybridisation
CTx, chemotherapy
Docetaxel
Docetaxel +
carboplatin
Trastuzumab
Paclitaxel
Piccart-Gebhart et al 2005
Romond et al 2005; Slamon et al 2006
Neoadjuvant setting
What we know
Adjuvant setting
What we do not know
Small, node negative tumors are under
represented in clinical trials
Studies investigating clinical outcome of pT1pN0 tumors by
HER-2 and hormone receptors (HRs) status. Results
• Overall
7,164 pts. with pT1pN0 tumors
– median follow-up 4.5 - 12.4 yrs.)
– 600 pts. with HER-2 + tumors
• % HER-2 + disease
– ranging between 7 and 10%
• Absolute risks of distant relapse HER2+
– 5 yrs. ± 10-15%
– 10 yrs. 22-28%
• Increased risk of disease relapse if HER-2 +
– hazard ratios ranging between 2.4 and 8.99
Reviewed by Oakman C et al, Educational book – ESMO meeting, Milan – October 2010
Studies investigating clinical outcome of pT1pN0 tumors by HER-2
and hormone receptors (HRs) status. Caveats and Conclusions
• Caveats
- heterogeneity in adjuvant therapies
- HRs status not always centrally revised
- in 3 out of 7 studies pT1c tumors were eligible
- only 2 out of 7 studies evaluate outcome by combination of
HER-2 and HRs status
• “Take-home” messages
- there is a substantial degree of concordance in considering
HER-2 + patients with pT1pN0 tumors at increased risk of
relapse compared to the HER-2 negative population (2 to 9
fold increase)
Reviewed by Oakman C et al, Educational book – ESMO meeting, Milan – October 2010
Key question
Is proportional benefit from
adjuvant systemic therapies
dependent on disease stage ?
Potential options for adjuvant treatment of
endocrine-resistant pT1b pN0 tumors
HER-2 +
• Docetaxel-Cyclophosphamide (TC) x 4 + Trastuzumab*
Trastuzumab
(lack of phase III data)
• Docetaxel-Carboplatin-Trastuzumab (TCH) x 6
(BCIRG 006 data)
* concomitant trastuzumab > sequential trastuzumab
Trastuzumab
Treatment decision:
a multi-factorial process
Tumor* :
Size
Patient :
Co-morbidities
Vascular invasion
Ki-67
Patient :
Expectations
Age
Preferences
Treatment
decision
Adjuvant setting
What we do not know
Duration of Trastuzumab
Adjuvant trials with different duration of
trastuzumab administration
• HERA (PI M. Piccart): sample size ~34001
– 12 vs 24 months of H following adjuvant CT
• Phare (PI X. Pivot): sample size ~34002
– 6 vs 12 months of H following adjuvant CT
• Persephone (UK-NCRI): sample size ~40003
– 6 vs 12 months of H following adjuvant CT
• Hellenic Oncology Group (Greece): sample size 4784
– 6 vs 12 months of H with ddDoc after FEC
• SOLD (PI H. Joensuu): sample size ~30006
– HD 3-wkly x3 ->FE75C x3
vs
– HD 3-wkly x3 ->FE75C x3 -> H 3-wkly x14
• ShortHER (PI PF. Conte): sample size ~12505
– D 3-wkly x3 + H weekly x 9 -> FE60C x3
vs
– AC or EC x 4 -> HD or HP 3-wkly x4 -> H 3-wkly x14
Metastatic Disease
Overall Survival
by Trastuzumab Treatment Groups
Overall Survival Probability
1.0
Negative
No Trastuzumab
Trastuzumab
HER2+ /
Herceptin
0.8
0.6
HER20.4
HER2+ /
0.2
No Herceptin
0.0
0
12
24
36
Months from Diagnosi
48
60
What we Know
The first line
HERNATA Study
HERNATA study : results
Time to Progression
Overall Survival
Andersson JCO 2010
HERNATA study: results
Time to Treatment Failure
Andersson JCO 2010
HERNATA study : safety profile
Andersson JCO 2010
What we Know
The second line
Tyverb plus capecitabine: significantly
longer TTP in difficult to treat population
(EGF100151, independent assessment)
Cumulative progression-free (%)
Tyverb + capecitabine
Capecitabine
HR: 0.57 (95% CI: 0.43, 0.77)
p=0.00013
18.6 wks
27.1 wks
(4.3 mos)
(6.2 mos)
1. Cameron et al. Breast Cancer Res Treat 2008;[Epub ahead of print].
Figure Adapted from Cameron D, Casey M, Press M et al. A phase III randomized comparison of lapatinib plus capecitabine versus capecitabine
alone in women with advanced breast cancer that has progressed on trastuzumab: updated efficacy and biomarker analyses. Breast Cancer Res
Treat, 2008 Epub ahead of print, with kind permission of Springer Science and Business Media.
What we Know
Beyond the second line
Lapatinib in combination with trastuzumab
significantly prolonged PFS compared with
lapatinib alone (EGF104900)
Cumulative progression-free (%)
100
Lapatinib
Lapatinib +
trastuzumab
n=145
n=146
Progressed or died, n
128
127
Median, wks
8.1
12.0
80
60
HR (95% CI)
0.73 (0.57, 0.93)
p value
40
0.008
6-month PFS
28%
20
13%
0
0
10
Subjects at risk:
Lapatinib 148
53
21
13
5
0
73
42
27
8
2
Lapatinib + 148
trastuzumab
20
30
40
Time from randomisation (weeks)
50
60
Updated overall survival in ITT
Cumulative % alive without progression
(EGF104900)
100
80%
Died, n (%)
80
Median, months
Hazard ratio (95% CI)
70%
60
L
n=145
L+T
n=146
113 (78)
105 (72)
9.5
14
0.74 (0.57, 0.97)
Log-rank p value
.026
56%
6 month OS
40
41%
20
L+T
L
12 month OS
0
0
Patients at risk
L
148
L+T
148
5
10
121
102
88
65
15
20
25
Time from randomization (months)
64
47
43
28
25
13
30
1
35
Lapatinib effect on ErbB2 accumulation at cell
membrane: novel mechanism for enhanced
effects of combined anti-ErbB2 therapy
Lapatinib has been shown to enhance antitumour effect of
trastuzumab in vitro and in clinical studies
This study explored the mechanism for this effect by
investigating impact of lapatinib and trastuzumab on receptor
expression and signalling
Treatment:
lapatinib,
trastuzumab,
or both
ErbB2-positive BC cells
(SKBR3 and MCF7-HER2)
In vitro assays:
Receptor expression,
phosphorylation, signalling,
tumour growth
Mouse xenograft
Scaltriti et al., J Clin Oncol ASCO Annual Meeting Proceedings 2008; 26(Suppl.): Abstract 3594 and poster
Scaltriti et al., Oncogene 2009; www.nature.com/onco
What we Know
HER2+ and HR+
HER2 and hormone receptor-positive BC
Clinical trials to assess therapy
Cortes Nat Rev Clin Oncol 2010
HER2 and hormone receptor-positive BC
Clinical trials to assess therapy
Overall response rates (%)
100
Combination with
chemotherapy
80
60
H0648g
M77001
Combination with
Aromatase inhibitors
40
EGF30008
TAnDEM
20
0
Trastuzumab
+
anastrozole
Lapatinib
+
letrozole
Trastuzumab Trastuzumab
+
+
paclitaxel
docetaxel
Drug regimen
Figure 1: Overall response rates in HER2-positive and hormone receptor-positive metastatic breast cancer. Anti-HER2
therapy was combined either with chemotherapy or aromatase inhibitors in four pivotal trials. The combination with
chemotherapy showed higher overall response rates. 8.10-12
Cortes Nat Rev Clin Oncol 2010
What else we Know
The Future
Trastuzumab + Pertuzumab
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6-10, 2011
Pertuzumab and trastuzumab have complementary
mechanisms of action
Pertuzumab
HER2
HER1/3/4
Trastuzumab
Subdomain IV
Dimerization
domain
Trastuzumab:
Pertuzumab:
• Inhibits ligand-independent HER2
signaling
• Inhibits ligand-dependent HER2
dimerization and signaling
• Activates ADCC
• Activates ADCC
• Prevents HER2 ECD shedding
ADCC, antibody-dependent cell-mediated cytotoxicity; ECD, extracellular domain
Copyrights for this presentation are held by the author/presenter. Contact them at JBASELGA@PARTNERS.ORG for permission to reprint and/or distribute.
35
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6-10, 2011
CLEOPATRA: a Phase III trial of trastuzumab +
pertuzumab in the 1st-line setting
n=406
Patients with
HER2-positive MBC
centrally confirmed
(N = 808)
Placebo + trastuzumab
PD
Docetaxel*
≥6 cycles recommended
1:1
Pertuzumab + trastuzumab
n=402
PD
Docetaxel*
≥6 cycles recommended
• Randomization was stratified by geographic region and prior treatment
status (neo/adjuvant chemotherapy received or not)
• Study dosing q3w:
− Pertuzumab/Placebo:
− Trastuzumab:
− Docetaxel:
840 mg loading dose, 420 mg maintenance
8 mg/kg loading dose, 6 mg/kg maintenance
75 mg/m2, escalating to 100 mg/m2 if tolerated
* <6 cycles allowed for unacceptable toxicity or PD; >6 cycles allowed at investigator discretion
MBC, metastatic breast cancer; PD, progressive disease
Copyrights for this presentation are held by the author/presenter. Contact them at JBASELGA@PARTNERS.ORG for permission to reprint and/or distribute.
36
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6-10, 2011
Primary endpoint: Independently assessed PFS
Progression-free survival (%)
n = 433 PFS events
100
Ptz + T + D: median 18.5 months
90
Pla + T + D: median 12.4 months
∆ = 6.1 months
80
70
60
50
40
HR = 0.62
95% CI 0.51‒0.75
p<0.0001
30
20
10
0
0
5
10
15
20
25
30
35
40
Time (months)
n at risk
Ptz + T + D 402
345
267
139
83
32
10
0
0
Pla + T + D 406
311
209
93
42
17
7
0
0
D, docetaxel; PFS, progression-free survival; Pla, placebo; Ptz, pertuzumab; T, trastuzumab
Stratified by prior treatment status and region
Copyrights for this presentation are held by the author/presenter. Contact them at JBASELGA@PARTNERS.ORG for permission to reprint and/or distribute.
37
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6-10, 2011
Overall survival: Predefined interim analysis
Median follow-up: 19.3 months, n = 165 OS events
100
Overall survival (%)
90
80
70
HR = 0.64*
95% CI 0.47‒0.88
p = 0.0053*
60
50
40
30
Ptz + T + D: 69 events
20
Pla + T + D: 96 events
10
0
0
5
10
15
25
30
35
40
45
31
4
0
0
Time (months)
n at risk
Pertuzumab + T + D 402
20
387
367
251
161
87
Placebo + T + D
406
383
347
228
143
67
24
2
0
0
* The interim OS analysis did not cross the pre-specified O’Brien-Fleming stopping boundary (HR ≤0.603; p ≤0.0012)
D, docetaxel; OS, overall survival; Pla, placebo; Ptz, pertuzumab; T, trastuzumab
Copyrights for this presentation are held by the author/presenter. Contact them at JBASELGA@PARTNERS.ORG for permission to reprint and/or distribute.
38
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6-10, 2011
Cardiac tolerability
Placebo
Pertuzumab
+ trastuzumab + docetaxel + trastuzumab + docetaxel
(n = 397)
(n = 407)
Investigator-assessed
1.8%
1.0%
Independently adjudicated
symptomatic LVSD*
1.0%
1.0%
Fall in LVEF to <50% and by
≥10 percentage points from
baseline
6.6%
3.8%
symptomatic LVSD*
* LVSD was defined as NYHA class III/IV
LVEF, left ventricular ejection fraction; LVSD, left ventricular systolic dysfunction
Copyrights for this presentation are held by the author/presenter. Contact them at JBASELGA@PARTNERS.ORG for permission to reprint and/or distribute.
39
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6-10, 2011
Adverse events (all grades)
≥25% incidence or ≥5% difference between arms
Placebo
+ trastuzumab + docetaxel
(n = 397)
Pertuzumab
+ trastuzumab + docetaxel
(n = 407)
Diarrhea
184 (46.3)
272 (66.8)
Alopecia
240 (60.5)
248 (60.9)
Neutropenia
197 (49.6)
215 (52.8)
Nausea
165 (41.6)
172 (42.3)
Fatigue
146 (36.8)
153 (37.6)
Rash
96 (24.2)
137 (33.7)
Decreased appetite
105 (26.4)
119 (29.2)
Mucosal inflammation
79 (19.9)
113 (27.8)
Asthenia
120 (30.2)
106 (26.0)
Peripheral edema
119 (30.0)
94 (23.1)
Constipation
99 (24.9)
61 (15.0)
Febrile neutropenia
30 (7.6)
56 (13.8)
Dry skin
17 (4.3)
43 (10.6)
Adverse event, n (%)
Copyrights for this presentation are held by the author/presenter. Contact them at JBASELGA@PARTNERS.ORG for permission to reprint and/or distribute.
40
San Antonio Breast Cancer Symposium – Cancer Therapy and
Research Center at UT Health Science Center – December 6-10, 2011
Summary and conclusions
• CLEOPATRA met its primary endpoint and demonstrated a
statistically significant and clinically meaningful improvement in PFS
(HR = 0.62) in patients with HER2-positive MBC
– Median PFS increased by 6.1 months from 12.4 to 18.5 months
– The PFS improvement was consistent across subgroups and
supported by the secondary endpoints of ORR and OS (immature)
• The combination of pertuzumab and trastuzumab plus docetaxel
increased rates of diarrhea, rash, mucosal inflammation, febrile
neutropenia, and dry skin
– These adverse events were primarily grades 1‒2, manageable,
and occurred during docetaxel therapy
– There was no increase in cardiac adverse events or LVSD
• This new regimen may be practice-changing in HER2-positive
first-line MBC
Copyrights for this presentation are held by the author/presenter. Contact them at JBASELGA@PARTNERS.ORG for permission to reprint and/or distribute.
41
What else we Know
The Future
T-DM1
Trastuzumab emtansine (T-DM1): the firstin-class HER2-targeted antibody-drug
conjugate
Target expression: HER2
Monoclonal antibody: trastuzumab
Cytotoxic agent: DM1
Highly potent chemotherapy
(maytansine derivative)
Linker
T-DM1
Systemically stable
Breaks down in target cancer cell
43
Study Design
TDM4450g: ongoing Phase II study of T-DM1 vs trastuzumab +
docetaxel in first-line HER2-positive MBC
Trastuzumab
8 mg/kg loading dose;
6 mg/kg q3w IV
HER2-positive,
recurrent locally
advanced breast
cancer or MBC
(N=137)
1:1
PDa
+ Docetaxel
75 or 100 mg/m2 q3w
Crossover to
T-DM1
(optional)
(n=70)
T-DM1
3.6 mg/kg q3w IV
PDa
(n=67)
• Randomized, phase II, international, open-label studyb
• Stratification factors: World region, prior adjuvant trastuzumab therapy, disease-free interval
• Primary end points: PFS by investigator assessment, and safety
• Data analyses were based on clinical data cut of Nov 15, 2010 prior to T-DM1 crossover
• Key secondary end points: OS, ORR, DOR, CBR, and QOL
aPatients
bThis
were treated until PD or unacceptable toxicity.
was a hypothesis generating study; the final PFS analysis was to take place after 72 events had occurred.
44
Progression-Free Survival by Investigator
Randomized Patients
Median
PFS, mos
Proportion progression-free
1.0
Trastuzumab
+ docetaxel (n=70) 9.2
T-DM1
(n=67) 14.2
Hazard
ratio 95% CI
0.594
0.364–
0.968
Log-rank
P value
0.0353
0.8
0.6
0.4
0.2
0.0
0
2
4
Number of patients at risk
T+D 70
66
63
T-DM1 67
60
51
6
8
10
Time (months)
12
14
16
18
20
53
46
43
42
12
22
4
15
2
6
2
3
0
0
27
35
Hazard ratio and log-rank P value were from stratified analysis.
45
Duration of Response by Investigator
Patients with Measurable Disease at Baseline with an Objective Response
Median
DOR, mos
Proportion progression-free
1.0
Trastuzumab
+ docetaxel (n=40)
T-DM1
(n=43)
9.5
NRa
95% CI
6.6–10.6
–
0.8
0.6
0.4
0.2
0.0
0
2
Number of patients at risk
T+D 40
40
T-DM1 43
41
4
38
38
6
8
10
12
Duration of objective response (months)
32
33
19
27
8
19
2
12
Kaplan-Meier estimates are shown.
aNR, not reached; longer follow-up is needed to estimate the duration of response in the T-DM1 arm.
14
16
18
1
6
1
3
0
0
46
Incidence of Nonhematologic Adverse Events:
≥30% (All Grade) and/or ≥5% (Grade ≥3) of Patientsa
All grade, n (%)
AE
Alopecia
Fatigue
Nausea
Diarrhea
Peripheral edema
Increased AST
Pyrexia
Headache
Back pain
Increased ALT
Pneumonia
Trastuzumab +
docetaxel
c
(n=66)
T-DM1
c,d
(n=69)
44 (66.7)
30 (45.5)
29 (43.9)
30 (45.5)
29 (43.9)
4 (6.1)
15 (22.7)
12 (18.2)
20 (30.3)
4 (6.1)
1 (1.5)
3 (4.3)
34 (49.3)
33 (47.8)
11 (15.9)
7 (10.1)
27 (39.1)
27 (39.1)
25 (36.2)
18 (26.1)
16 (23.2)
6 (8.7)
b
Grade ≥3 , n (%)
Trastuzumab +
docetaxel
c
(n=66)
T-DM1
c,d
(n=69)
e
e
3 (4.5)
0
2 (3.0)
3 (4.5)
0
1 (1.5)
0
3 (4.5)
0
0
3 (4.3)
2 (2.9)
0
0
6 (8.7)
0
0
1 (1.4)
6 (8.7)
4 (5.8)
Green represents those AEs with ≥20% difference between treatment arms.
aIn
either treatment arm.
adverse events listed were grade 5.
cTwo patients mistakenly received a dose of T-DM1 and were thus included in the T-DM1 arm for safety analyses.
dIncludes 3 patients who received at least 1 dose of trastuzumab alone or trastuzumab plus docetaxel.
eNational Cancer Institute Common Terminology Criteria for Adverse Events v.3 only categorizes alopecia as grade 1 or
grade 2; there is no grade ≥3 for this AE.
bNo
47
Cardiac Safety
• Cardiac function was assessed locally and centrally based on cardiac ECHO/MUGA
• Prior anthracycline in the adjuvant setting was 44.8% and 48.6% in the T-DM1 and
trastuzumab + docetaxel arms, respectively
• Asymptomatic LV dysfunction
Trastuzumab +
docetaxel
T-DM1
Patients assessed
65
67
Patients with post-baseline LVEF ≤40%
2a
0
Patients assessed
60
65
Patients with post-baseline LVEF ≤40%
1b
0
LVEF assessment
Local assessment
Central assessment
• There were no clinically significant cardiac events reported
aBoth
patients had prior anthracycline therapy in the adjuvant setting; 1 patient received prior trastuzumab therapy in the
adjuvant setting.
bThis patient did not receive prior treatment with an anthracycline.
48
Summary and Conclusions
• This is the first randomized study to evaluate an antibody-drug conjugate for HER2positive MBC
• First-line treatment of HER2-positive MBC with T-DM1, compared with trastuzumab
+ docetaxel was associated with:
– A significant improvement in PFS (14.2 vs 9.2 mos; HR=0.594; P value=0.0353)
– Similar ORR but more durable responses (64.2%, median duration not reached vs. 58.0%,
median duration 9.5 months)
– A lower rate of grade ≥3 AEs (46.4% vs 89.4%)
• These results validate the hypothesis that the unique properties of T-DM1 may lead
to an improved therapeutic index
– Improved PFS with T-DM1 may result from improved tolerability/duration of
treatment/response and intrinsic potency of HER2-targeted DM1
• T-DM1 is being evaluated in phase III randomized clinical trials for HER2-positive
MBC
49
TDM4370g (EMILIA) Phase III Study: T-DM1 vs
Capecitabine + Lapatinib in HER2-Positive MBC
• HER2-positive LABC or MBC
(N=980)
• Previously received
trastuzumab-based therapy
•
•
•
•
T-DM1 (3.6 mg/kg) q3w
1:1
Lapatinib (1250 mg/day, days
1–21)
+ capecitabine (1000 mg/m2,
days 1–14) q3w
Multicenter, randomized, open-label study
Treatment continues until progressive disease/unacceptable toxicity
Primary end points: PFS by IRF, OS, 1-y and 2-y survival rates, Safety
Secondary end points: PFS by INV, ORR, CBR, DoR, QOL, TTF
www.clinicaltrials.gov. NCT00829166.
MARIANNE:
Trastuzumab + taxane
(n=364)
HER2-positive progressive or
recurrent locally advanced BC or
previously untreated MBC
(n=1092)
T-DM1 + pertuzumab
(n=364)
T-DM1 + placebo
(n=364)
• Primary efficacy objective:
– PFS assessed by an independent review facility
• Primary safety objective:
– To compare the safety of T-DM1 + pertuzumab or T-DM1 + placebo
vs trastuzumab + taxane
BC = breast cancer; MBC = metastatic breast cancer; PFS = progression-free survival
51