Analysis of FcReceptor IIA and IIIA Polymorphisms:
Correlation with Outcome in Trastuzumab-Treated Her2/neu
Amplified Early and Metastatic Breast Cancer Patients
POSITIVE DISCLOSURES
Dr. Hurvitz received research/grant support from Genentech/Roche
Dr. Stern is an employee of Genentech and stockholder in Roche
Jeremy Stinson is an employee of Genentech and stockholder in Roche
Dr. Seshagiri is an employee of Genentech and stockholder in Roche
Dr. Robert receives research/grant support from Genentech and is on the
Roche Speakers’ Bureau
Dr. Valero receives research/grant support from Genentech/Roche and is on
the Roche Speakers’ Bureau
Dr. Crown receives research/grant support from Roche and is on the Roche
Speakers’ Bureau
Dr. Slamon is on the speakers’ bureau for Genentech
Analysis of Fc Receptor IIa and IIIa Polymorphisms:
Correlation with Outcome in Trastuzumab-Treated
Her2/neu Amplified Early and Metastatic Breast
Cancer Patients
Sara A. Hurvitz, David Betting, Howard M. Stern,
Emmanuel Quinaux, Jeremy Stinson, Somasekar Seshagiri,
Ying Zhao, Marc Buyse, John Mackey, Nicholas J. Robert,
Vicente Valero, John Crown, Adrian Driga, Valerie Bee,
Dennis J. Slamon, John M. Timmerman
Abstract 64
Trastuzumab: αHer2-Monoclonal IgG1 Antibody
Postulated Mechanisms of Action
1. Growth Factor Receptor Blockade
Inactivation of AKT signaling
Decreased Cell Proliferation
Induction of Apoptosis
Tumor Cell
FcR
NK Cell
Preclinical evidence for role of ADCC:
2. FcR engagement (e.g. AntibodyDependent Cellular Cytotoxicity, ADCC)
Efficacy of trastuzumab against breast
cancer xenografts was largely dependent
on FcR binding
Clynes et al. Nature Med. 2000;6:443-446
Human FcRIIIa (CD16) polymorphisms
• FcRIIIa is expressed on both NK cells and
macrophages; ADCC effectors in vivo
• Gene dimorphism encoding FcRIIIa:
phenylalanine (F) or a valine (V) at position 158
• This residue interacts with IgG1 Fc
• Human IgG1 binds more strongly to
homozygous V/V NK cells than to others
• Frequency of genotype in population:
158 V/V 13%, V/F 47%, F/F 40%
Wu et al, J. Clin. Invest.100:1059, 1997.
Lehrnbecher, Blood, 1999;94;4220-4232.
Human FcRIIa (CD32) polymorphisms
• Gene dimorphism encoding FcRIIa:
histidine (H) or arginine (R) at position 131
• Human IgG1 binds more strongly to
homozygous FcRIIa-131 H/H immune cells than
to H/R or R/R
• Frequency in general population:
131 H/H 21%, H/R 58%, R/R 21%
Wu et al, J. Clin. Invest.100:1059, 1997.
Lehrnbecher, Blood, 1999;94;4220-4232.
FcR Genotype: Outcome with Monoclonal Ab Therapy
Rituximab anti-CD20-antibody for non-Hodgkin’s lymphoma:
• FcRIIIa-158V/V and FcRIIa-131H/H genotypes associated with
improved response rates and PFS.
Question: Does FcR genotype play a role in the
response to trastuzumab?
Such an association would:
• provide evidence that the immune system plays a role in the antitumor activity of trastuzumab
• support the development of engineered monoclonal antibodies
with an increased affinity for FcR to improve drug efficacy
Cartron, Blood 2002;99:754-758.
Weng, W-Ki, et al. JCO 2003
Previous studies of FcR genotypes in trastuzumabtreated breast cancer: Discordant Results
Foster, et al1: No association between FcRIIIa genotype and response
in retrospective analysis of trial evaluating trastuzumab monotherapy
in relapsed MBC (N=63)
Musolino et al, 20082: Assessed role of FcR genotypes in predicting
efficacy of trastuzumab in 54 Her2+ MBC receiving trastuzumab +
taxane.
FcRIIIa
1. Foster, Ostland, Mass, et al. Proceedings ASCO, 2002. 21(Abstract No: 227)
2. Musolino et al. J Clin. Oncol. 2008: 26
FcRIIa
Purpose
Determine whether FcRIIIa 158 V/F and/or FcRIIa
131 H/R genotypes are associated with disease free
survival (DFS) in large cohort of patients with
Her2/neu-amplified early stage breast cancer
treated with trastuzumab.
In a separate cohort of Her2+ metastatic breast
cancer patients treated with trastuzumab, determine
whether FcRIIIa158 V/F and/or FcRIIa131 H/R
genotypes are associated with time to progression
(TTP).
Methods
• Serum & whole blood samples from breast cancer patients
treated in the BCIRG-006 study who signed optional
consent to have samples taken
• Genotype (FcRIIIA 158V/F and FcRIIA 131 H/R) was
determined by Sanger sequencing and Sequenom mass
spectrometry
• DFS was calculated by Kaplan-Meier and compared using
log-rank test using data from third planned analysis
BCIRG 006
4 x AC
4 x Docetaxel
60/600 mg/m2
100 mg/m2
4 x AC
4 x Docetaxel
60/600 mg/m2
100 mg/m2
ACT
Her 2+
(Central FISH)
N+
or high
risk N-
ACTH
1 Year Trastuzumab
6 x Docetaxel and Carboplatin
N=3,222
Stratified by Nodes
and Hormonal
Receptor Status
75 mg/m2
AUC 6
TCH
1 Year Trastuzumab
Slamon et al. SABCS 2006
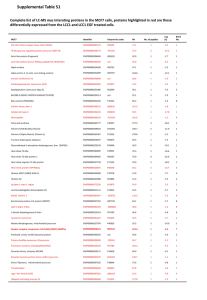
BCIRG 006 Subpopulation
Enrolled in BCIRG 006 (N=3,222)
Did not consent or provide sample
(N=1,936)
Patients signed optional consent and samples sent in (N=1,286)
FcR IIIA
FcRIIA
Genotyping failed
(N=97)
Genotyping failed
(N=68)
FcR IIIA (N=1,189)
FcR IIA (N=1,218)
Arm
Total in Trial
FcγR IIIA
FcγR IIA
AC-T
1,073
381 (36%)
387 (36%)
AC-TH
1,074
406 (38%)
415 (39%)
TCH
1,075
402 (37%)
416 (39%)
Total
3,222
1189 (37%)
1218 (38%)
BCIRG 006 Disease Free Survival
3rd Planned Analysis – Overall Population (N=3222)
% alive and disease-free
1
0.9
0.8
0.7
0.6
Patients Events HR (95% C.I.)
AC-T
1073
257
1 (reference)
AC-TH 1074
185
0.64 (0.53 - 0.78)
TCH
1075
214
0.75 (0.63 - 0.90)
0.5
0.4
0
12
24
36
Time (months)
48
60
P
< 0.001
0.002
72
BCIRG 006
Slamon et al, SABCS 2009
0 .6
0 .4
0 .2
Patients
Events Treatment
414
88
AC-T
436
85
AC-TH
436
83
TCH
0 .0
P ro b a b ility
0 .8
1 .0
Disease free survival:
Subset of patients who were genotyped
0
6
12
18
24
30
36
42
48
Months
54
60
66
72
78
84
90
0 .6
Stratified for major prognostic factors: age, LN, hormone
receptor status, size, surgery type:
0 .4
HR 0.74 [0.56, 0.98] p=0.036
0 .2
Patients
Events Risk group
414
88
AC-T
872
168
AC-TH+TCH
0 .0
P ro b a b ility
0 .8
1 .0
Disease free survival (DFS):
Genotyped patients with stratification
0
6
12
18
24
30
36
42
48
Months
54
60
66
72
78
84
90
Patient Characteristics
• Prognostic factors among the 3 FcRIIIA and 3 FcRIIA
genotypes were well balanced for:
• Lymph node status
•
•
•
•
•
ER/PR status
Menopausal status
Tumor size
Age
Her2/neu FISH ratio
DFS Trastuzumab Arms FcRIIIa genotype
0 .6
0 .4
Log Rank p=0.98 (VV vs. VF vs. FF)
Patients
0 .2
113
322
373
695
Events Risk group
20
63
74
137
V/V (14%)
V/F (40%)
F/F (46%)
F carriers
0 .0
P ro b a b ility
0 .8
1 .0
No statistically significant difference by genotype
0
6
12
18
24
30
36
42
48
Months
54
60
66
72
78
84
90
0 .6
0 .4
Log Rank p=0.76 (H/H vs. H/R vs. R/R)
Patients
0 .2
213
415
203
618
Events Risk group
41
85
39
124
H/H (26%)
H/R (50%)
R/R (24%)
R carriers
0 .0
P ro b a b ility
0 .8
1 .0
DFS: Trastuzumab arms by FcRIIa genotype
No statistically significant difference by genotype
0
6
12
18
24
30
36
42
48
Months
54
60
66
72
78
84
90
DFS: Trastuzumab Arms
0 .6
0 .4
Log Rank p=0.67
0 .2
Patients
Events Risk group
277
51
V/V and/or H/H
595
117
Others
0 .0
P ro b a b ility
0 .8
1 .0
FcRIIIa-158V/V and/or FcRIIa-131/HH vs Others
0
6
12
18
24
30
36
42
48
Months
54
60
66
72
78
84
90
Metastatic breast cancer cohort:
Retrospective analysis
•
Prospectively collected DNA from 53 women with Her2/neu
amplified and/or overexpressed metastatic breast cancer
treated with trastuzumab-based regimen
•
FcRIIIA 158V/F and FcRIIA 131H/R genotypes determined
•
Time to progression calculated from start of first exposure
to trastuzumab to time of disease progression or death
• Compared genotypes survival curves using log rank test
• Cox proportional hazards regression model used for HRs
•
Prior therapies in metastatic setting before receiving
trastuzumab
• 43 patients had no prior chemo
• 10 pts had 1-4 prior chemo regimens
Time to Progression by FcR Genotype
No significant differences in TTP according to FcR genotypes
among 53 MBC patients treated with trastuzumab
FcRIIIa
N=6
N=25
N=21
FcRIIa
N=15
N=26
N=12
Summary
•
BCIRG 006 Early Breast Cancer Cohort
• Largest FcR genotyping analysis of trastuzumabtreated breast cancer patients to date,
• We found no statistically significant correlation between
FcRIIIa and FcRIIa genotypes and DFS.
•
Limitations of study
• Incomplete genotyping of entire study population
• Trastuzumab benefit less robust in cohort of patients
with serum/whole blood available for genotyping
• Despite this limitation, there appears to be no statistically
significant difference in outcome among genotypes
•
Metastatic cohort
•
In 53 women with Her2/neu positive metastatic breast
cancer, we found no significant correlation between
FcR genotypes and TTP
Conclusions
In contrast to the Musolino study, but similar to
the Foster study, we saw no difference in clinical
outcome based on FcR genotypes in both early
and metastatic breast cancer cohorts.
These data do not support the hypothesis that
polymorphism-related differences in FcR affinity
cause differential outcome to trastuzumab therapy
Acknowledgements
Dennis Slamon, MD, PhD
John Timmerman, MD
Jan Tillisch, MD
Mark Pegram, MD
Yiou Tseng
Mark Sliwkowski, PhD
Anne Blackwood-Chirchir. MD
Mona Shing, MD
Fan Zhang, PhD
Deepali Bhatt
ASCO Foundation, Young Investigator Award 2007
NIH Loan Repayment Program
Genentech Research Grant
Patients
 0
0