Prostate Cancer Screening: Con - Dr. Petrylak

Prostate Cancer
Screening: Con
Daniel P. Petrylak, MD
Yale University Cancer Center
Prostate Cancer “Screening” Trials
Norrköping
Quebec Study (RCT)
Swedish Study (RCT)
– 1998
– 2004
Deviations / limitations
In statistical methods
Tyrol Study – Population comparison (+ screen effect)
PLCO
ERSP
Thought to be well designed RCT with appropriate controls and respected steering committees, reported from 2009-2012
Göteborg
• CAP and ProtecT (UK) are ongoing
Three Largest Randomized PSA
Screening Trials
ERSPC
– PSA every 4 yrs in 182,000 men
PLCO
– USA trial testing PSA every yr vs. no PSA screening in 76,693 men analyzed in ITT analysis
Göteborg
– Randomized 20,000 man screening trial showed
44% reduction in death with little press
– ERSPC subset
ERSPC = European Randomized Study of Screening for Prostate Cancer;
PLCO = prostate, lung, colorectal, ovarian; ITT = intent-to-treat.
Schroder et al, 2009; Andriole et al, 2009. Hugosson J, 2010
Two Conflicting Studies:
Originally Published Together
PLCO: No reduction in PCa mortality (76,000 USA)
– Large number pre-screened = contaminated control group
– Limited follow up w/ single cut point for PSA
– 85% of the screened group had a PSA but 52% of the nonscreened group had a PSA
ERSPC: 20% reduction in mortality (182,000 EU)
25% reduction in metastatic disease
– No DRE, multiple countries with variable criteria
– 41% reduced metastasis, more cancers, lower Gleason
– Screen 1410, treat 48 to benefit 1 death
PLCO: Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial
ERSPC: European Randomized Study of Screening for Prostate Cancer
Andriole G, et al. N Engl J Med . 2009;360:1310-
1319. Schröder F, et al.
N Engl J Med . 2009;360:1320-
1328.
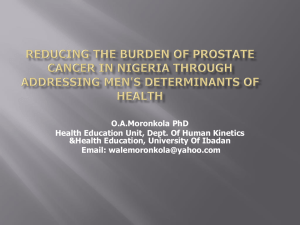
ERSPC: Cumulative Risk of Death
From Prostate Cancer
ERSPC demonstrates 20% reduction in prostate cancer death after
8.8 yrs of follow-up. The adjusted rate ratio for death from prostate cancer in the screening group was 0.8 (95% CI, 0.65
–0.98; p = .04).
CI = confidence interval.
Schroder et al, 2009.
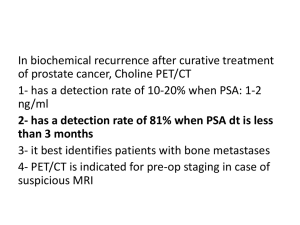
PLCO: Number of Prostate Cancers and Prostate Cancer Deaths
PLCO trial suggested that
PSA screening increases risk of cancer diagnosis but does not decrease risk of death
Andriole et al, 2009.
Pick level 1 evidence to make any point
No
PLCO: No reduction in prostate cancer mortality
Yes
ERSPC: 20% reduction in mortality
25% reduction in metastatic disease
Yes
Göteborg Trial: 44% reduction in mortality
Andriole G, et al. N Engl J Med . 2009;360:1310-1319.
Schröder F, et al. N Engl J Med . 2009;360:1320-1328.
PLCO reanalysis: improved PCSM when comorbidities were considered.
(22 v 38 deaths)
Crawford, D
JCO 2010
PLCO: no benefit for entire group
– “contaminated” control arm
– ~ 55% RRR for post-hoc defined subgroup.
ERSPC: 20% RRR; 25% reduction in metastatic disease
– reduces if Goteborg or Rotterdam participants removed
– improvements continue with time in
NNS, NNT
Principles of Screening
•
Finding disease is not a measure of success in screening
Increased survival is not a legitimate measure of success outside of a randomized clinical trial
Reduction of mortality in a randomized trial is the only true proof of effective screening
Cancer Screening
•
Well designed clinical studies have demonstrated the utility of:
•
Mammography and CBE for Breast Cancer
•
Stool Blood Testing, Sigmoidoscopy and
Colonoscopy for Colorectal Cancer
•
Pap and HPV testing for Cervical Cancer
Thoughts
• Screening doesn’t work for all cancers: Lung, neuroblastoma, and not all breast cancers
•
Need to separate diagnosis from treatment, clearly over treating men
•
But, need to remember that 28,000 men died in 2011 of CaP
•
We need to figure out who needs to be diagnosed and effectively treated.
USPSTF Prostate Cancer History
•
2002: insufficient evidence to recommend for or against routine screening
•
2008: against testing any man over age 75 years and gives “ I ” rating for prostate-cancer screening , (current evidence is insufficient to assess the balance of benefits and harms, for men younger than 75.
•
2011: no healthy man undergo PSA screening unless symptoms of prostate cancer
•
Open to public comment until 11/8/2011 (NEW since 2009 mammography controversy)
Urology USPSTF Replies
•
Marberger EAU: "Clearly mortality is reduced by PSA screening, but it has to be done in younger and fit patients who have a life expectancy for whom this slow growing cancer can really be a threat, ”
•
Lacy AUA: "We are concerned that the task force's recommendations will ultimately do more harm than good to the many men at risk for prostate cancer, both here in the US and around the world.
“
"Until there is a better widespread test for this potentially devastating disease, the USPSTF -- by disparaging the test -- is doing a great disservice to the men worldwide who may benefit from the PSA test."
Concern #1: Everybody Has Prostate
Cancer —You Die with It Not of It
Look at the prevalence of prostate cancer!
PIN=prostatic intraepithelial neoplasia
Sakr WA, et al. J Urol . 1993;150:379-385.
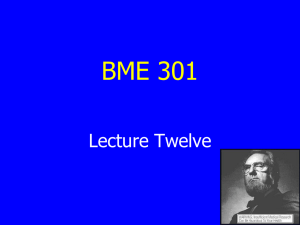
Concern #2: You Don ’t Help Most Men with Prostate Cancer When You Find It
Death from prostate cancer
Metastatic disease develops
Cancer spreads to lymph nodes
Cancer spreads beyond prostate
Cancer detectable: PSA >4 ng/mL
Prostate cancer develops
Patient D
Patient C
Zone of detection when cure is possible
Patient B
Patient A
Annual PSA and DRE
Concern #2: You Don
’
t Help Most Men with Prostate Cancer When You Find It
(cont
’
d)
Death from prostate cancer
Metastatic disease develops
Only this man benefits
Patient C
Cancer spreads to lymph nodes
Cancer spreads beyond prostate
Zone of detection when cure is possible
Cancer detectable: PSA >4 ng/mL
Prostate cancer develops
Annual PSA and DRE
Concern #2: You Don
’
t Help Most Men with Prostate Cancer When You Find It
(cont
’
d)
Death from prostate cancer
Metastatic disease develops
Patient D
These three guys do not benefit
Cancer spreads to lymph nodes
Cancer spreads beyond prostate
Zone of detection when cure is possible
Patient B
Cancer detectable: PSA >4 ng/mL
Prostate cancer develops
Patient A
Annual PSA and DRE
Concern #3: It Costs Too
Much!
Cost
•
Initial estimates of screening men age 50 –70 for prostate cancer
•
$25 billion during first year alone
•
Many countries don ’t encourage it, fearing screening will “break the bank” (eg, England,
Australia…)
Expenditures
•
Prostate- 8 billion 11.2%
•
Lung- 9.6 billion 13.3%
•
Breast 8.1 billion 11.2&
Concern #4: High Risk of Morbidity of Screening
•
Risks of screening: anxiety
•
Risks of biopsy: bleeding, infection, painful
•
Risks of treatment: impotence, incontinence, death, proctitis, cystitis, stricture
•
Risk of recurrence: as many as 1/3 of men will require a secondary treatment
And the Final Concern: No Proof that It
Really Works in Reducing Deaths
•
Screening evaluated in two trials
•
Prostate, lung, colorectal, ovarian (PLCO) screening study in the US (148,000 men and women randomized to screening or community standard of follow-up)
•
Europe: Rotterdam screening trial
•
Results of both: PLCO –Negative. ERSPC-? positive
Conclusions
•
A more rational policy is to screen appropriate men and treat only those with significant PCa.
•
The USPHSTF findings should be viewed as an opportunity to implement the above
•
Policy makers must consider risks and benefits to the USPHSTF recommendations on prostate cancer screening.