Prostate Cancer
Julian Mander
RPH Urology
Histological Incidence at Autopsy
Histological cancer in autopsy studies
27% Third decade
20% Fourth decade
32% Fifth decade
55% Sixth decade
64% Seventh decade
Sakr et al: In Vivo 8:439,1994
Histological Incidence at Autopsy
Incidental Prostate Cancer Found at Autopsy (Detroit, MI)
W.A. Sakr, et al. Eur.Urol. 30: 138, 1996.
Removed the prostate glands from 525 consecutive male trauma victims dying in Detroit during the early 1990s.
Causes of Death in Australia 2011
2.1 LEADING CAUSES OF DEATH , Australia - Selected years - 2002, 2006, 2011
Cause of death
2002 No.
Ischaemic heart diseases
Cerebrovascular diseases
Dementia and Alzheimer disease
Trachea, bronchus and lung cancer
Chronic lower respiratory diseases
Diabetes
Colon, sigmoid, rectum and anus cancer
Blood and lymph cancer (including leukaemia)
Heart failure
Diseases of the urinary system
Prostate cancer
Breast cancer
Influenza and pneumonia
Pancreatic cancer
Intentional self-harm
Skin cancers
Accidental falls
Hypertensive diseases
Cardiac arrhythmias
Cirrhosis and other diseases of liver
26 063
12 533
4 364
7 303
6 256
3 329
4 649
3 791
3 367
2 887
2 852
2 716
3 084
1 834
2 320
1 462
629
1 353
1 226
1 354
Prostate cancer deaths per 100,000 male population
35.5
Rank
1
2
6
3
4
9
5
7
8
11
12
13
10
15
14
17
38
20
21
19
2006 No.
23 132
11 479
6 550
7 353
5 463
3 669
3 857
3 700
2 902
3 197
2 951
2 643
2 711
2 077
2 118
1 648
1 288
1 500
1 280
1 416
~29
Australian Bureau of Statistics 2013
Rank
1
2
4
3
5
8
6
7
11
9
10
13
12
15
14
17
20
18
21
19
2011
No.
21 513
11 251
9 864
8 114
6 570
4 209
4 087
3 978
3 488
3 386
3 294
2 937
2 492
2 416
2 272
2 087
1 845
1 802
1 612
1 589
Rank
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
29.7
http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/3303.0Chapter42011
Australian Mortality Data 1985 - 2002
9.22 DEATH RATES(a) FROM SELECTED CANCERS
Males
Selected cancers
1985
1990
1995
2000
2002
0.2
0.3
0.4
0.2
0.2
Colorectal
37.9
35.2
33.9
30.5
27.7
Lung
77.2
68.5
63.9
54.7
53.3
Melanoma skin
6.8
7.6
8.1
7.4
8.0
Non-Hodgkin's
lymphoma
8.0
10.0
9.9
10.4
9.5
Non-melanocytic skin
3.1
3.6
3.8
3.2
3.2
Prostate
35.7
39.9
41.4
35.9
35.5
Breast
All cancers
287.3
277.7
270.6
246.6
241.3
(a) Rate per 100,000 population, age standardised to the 2001 population (persons).
Source: AIHW 2003.
Australian Bureau of Statistics
Yearbook Australia
1301.0 - 2005
Health - Article - Cancer Trends
Prostate Cancer & Death in Australia
2011 Australia
3,294 deaths from prostate cancer
4,959 male deaths from lung cancer
62% of prostate cancer deaths >75 years
41%
‘’
‘’
‘’
>80 years
Australian Cancer Incidence and Mortality Books (ACIM)
http://www.aihw.gov.au/cancer/data/acim_books/index.cfm
~3% Male deaths are from prostate cancer
Prostate Cancer Deaths in Australia 2011
Australian figures 2011
Prostate cancer deaths: 3,294
Deaths (Male) from MVA: 921
Australian Govt Dept Transport and Infrastructure
http://statistics.infrastructure.gov.au/atsb/login.do?guest=guest&tableId=user/atsbguest/Road%20Deaths%20by%20State%20and%20Territory.txd
Suicide (Male) deaths: 1,726
ABS Yearbook 2013
http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/F25E446E1BE6C931CA257B2E000D729C?opendocument
Western Australian Figures 2011
Mortality to incidence ratios (M/I):
Prostate cancer
Breast cancer
Lung cancer
Overall cancer (2005)
•
Males
0.12
Females
0.17
0.78
0.36
0.30
Western Australia Figures 2011
Prostate cancer – number diagnosed: 2,086 vs
Breast cancer (female)
1,423
Lung cancer (male)
595
Colorectal cancer (male)
774
number of deaths: 253 vs road toll: 126 (Male)
238
462
224
Western Australian Cancer Registry
http://www.health.wa.gov.au/wacr/statistics/stats_full.cfm
Prostate Cancer Incidence and Mortality Trends USA
Prostate Cancer Incidence and Mortality Trends USA
Prostate Cancer Incidence Rates* by Race and Ethnicity, U.S., 1999–2009
Prostate Cancer Death Rates* by Race and Ethnicity, U.S., 1999–2009
* USA Govt Centre for Disease Control and Prevention
http://www.cdc.gov/cancer/prostate/statistics/race.htm
Aetiology of Prostate Cancer
•
•
Testosterone
Promotes prostate cancer development
Prostate cancer does not develop in eunuchs
Testosterone supplements problematic in men with normal serum testosterone levels
Genetics
Mutations in BRCA1 (on chromosome 17) and BRCA2 (on chromosome 13), important risk factors for ovarian
cancer and breast cancer in women, have also been implicated in prostate cancer.
Other linked genes include the Hereditary Prostate Cancer Gene (HPC1) on chromosome 1, said to be responsible
for 3% of prostate cancers.
Dietary Factors
Little scientific evidence for dietary factors involved in the development of prostate cancer.
Relatively rare in South East Asian populations with diets high in phytoestrogens such as soy.
Pathology
Morphology
Adenocarcinoma 99%
cell of origin – basal cell most likely, not lumenal cell
Ductal carcinoma 0.141%
Mucinous adenocarcinoma 0.103%
Small cell carcinoma 0.056% (neuroendocrine)
Carcinosaroma 0.07%
Embryonal carcinosarcoma 0.06%
Differentiation = Gleason score
Based on morphological appearance (grade 1 – 5) where two most common morphologies are added to give a sum score (2 – 10)
Gleason 3 + 4 = 7 where 3 is the most common morphological pattern and 4 is the second most common pattern
If three morphological patterns, first number is most common pattern and second number is the pattern with the highest grade
Higher score = poorer differentiation = worse prognosis
Gleason 3
Gleason 4
Gleason 4
Gleason 5
Gleason Score and Prognosis
Gleason score is an independent prognostic indicator:
Gleason 5 - 6
moderate grade cancer
Gleason 7
intermediate grade cancer
Gleason 8 - 10
high grade cancer
The disease-specific mean survival (DSMS) in 305 men in Sweden diagnosed at TURP 1975 – 1990 who
had no curative treatment (no staging information used)
Gleason score 4-5
20 years
6
16 years
7
10 years
8-10
5 years
Gleason score and % cancer were independent predictors of DSMS (P < 0.001).
Prognostic Value of Gleason Score in Prostate Cancer
Egevad et al BJU Int 2002 Apr;89(6):538-42.
Clinical Management
Cancer screening and PSA
Diagnosis – TRUS biopsy and MRI
Prostate cancer prevention – “chemoprevention”
Expectant management
Curative therapy for Localized Disease (< T3 )
Surgery
“watchful waiting”.................
Perineal prostatectomy
Radical retropubic prostatectomy with dorsal vein ligation 1979 and neurovascular preservation 1982 by Patrick Walsh
Laparoscopic radical prostatectomy
Robotic laparoscopic radical prostatectomy
HIFU and Cryotherapy
Radiotherapy
External
Internal
External beam DXRT
Conformal external beam DXRT
IMRT Intensity Modulated Radiotherapy
IGRT Image Guided Radiotherapy
LDR brachytherapy ( I125 seeds)
HDR brachytherapy
P.S.A. - Prostate Specific Antigen
PSA is a Single chain glycoprotein.
237 amino acids long translated as a 261 AA prepropeptide from chromosome 19 gene designated LKLK 3.
Glycosylated PSA has MW 28,400 daltons.
Functions as a serine protease, recognized as a member of the human kallikrein family.
Functions to liquefy semen coagulum by breaking down gel forming proteins semenoglobulin I, semenoglobulin II and
fibronectin, releasing spermatozoa.
Originally identified in Japan in 1966 by Hara, who initially reported their findings on γ-seminoprotein in 1966 in
Nippon Hoigaku Zasshi, the Japanese Journal of Legal Medicine, and in 1971 were able to characterize this protein.
Although this antigen was later shown to be similar to PSA the original publications were in Japanese and
consequently not available to the English - speaking scientific community. This was early work on a forensic science
test for rape.
P.S.A. - Prostate Specific Antigen
Synthesized in prostatic ductal epithelium and acini and secreted into prostatic ducts to become a
component of semen.
Detected in female and male periurethral glands, apocrine sweat glands, some breast cancers, some
salivary gland cancers and breast milk.
Thought to diffuse across cells and basement membrane to enter bloodstream, diffusion increased in
inflammation and prostate cancer.
Half life 2.2 - 3.2 days.
Immunoreactive PSA subgroup
free PSA 1% - 30% of this group
bound PSA bound to alpha 1 antichymotrypsin.
PSA Levels Affected By :
Prostatitis - levels up to 120 recorded, resolving with antibiotics.
Urine retention - up to 6 fold increase.
Ejaculation - 0.2 ng/ml increase 24 hours later.
Ambulation - decreases PSA up to 20%.
Prostate biopsy - 8 ng/ml increase 4 - 24 hours later.
TURP - 6 ng/ml increase with median return to baseline at 18 days
Klein et al, The effects of prostate manipulation on PSA levels.
Urologic Clinics of North America May 1998.
PSA as a screening test
PSA is a poor screening test with high sensitivity but very poor specificity
Advocated screening with yearly PSA and DRE for men between 50 and 70 years of age
Earlier commencement of screening advocated for those at risk of hereditary cancer between 40 and
70 years of age
Recommended in some parts of the USA. A policy of the American Urological association.
Prostate cancer screening is not currently recommended by Government health authorities in either
Australia or the UK.
PSA as a screening test
Australian Health Technology Advisory Committee (AHTAC) review 1996 - Australian Government
Publishing Service 1996.
“As a result of the evaluation of prostate cancer screening against established criteria, AHTAC
recommends against the screening of asymptomatic men for prostate cancer.”
“AHTAC recommends:
that the use of PSA continue to be supported in the monitoring of men known to have prostate
cancer and in patients selected for active treatment for BPH; and that men being offered, or
requesting the PSA test must be fully informed of the limitations of the available tests and the
possible further diagnostic and treatment choices with which they may be faced should they decide
to proceed with the test.”
Total PSA screening studies
PSA > 4ng/ml
Incidence of cancer detection on prostate biopsy based on DRE findings and PSA.
PSA ng/ml
0-4
4 - 10
>10
Overall cancer detection rate
1.5% - 4.1%
DRE negative
4 - 7%
24 - 25%
31 - 42%
PPV
33% mean
DRE positive
10 - 13%
41 - 62%
67 - 77%
Arcangeli et al Urologic Clinics of N. America, May 1998
PSA Density and Screening
PSA density = Total PSA ng/ml / TRUS determined prostate volume in ml
>0.15 with PSA 4 - 10
reduces number of biopsies 50%
misses 50% of cancers
Catalona et al : J Urol 153:2031,1994
PSA Velocity and Screening
This is shown to be higher in men with prostate cancer than in BPH
PSA slope cut off 0.75 ng/ml per year with PSA <4 ng/ml
sensitivity 79%
specificity 66%
Smith and Catalona: J Urol 152:1163, 1994
Difficult because there is a 15% short term variation in PSA levels
Stamey et al: J Urol 155: 1977,1996
Age Specific Reference Ranges in PSA
Oesterling et al 471 men in Olmstead County, Minnesota had DRE, PSA and TRUS . Found to have
increasing PSA with age at a rate of 0.04 ng/ml per year.
Oesterling et al: JAMA 270:860, 1993
Catalona however found that 30% of organ confined histologically significant cancers in men older
than 60 would be missed if age related reference ranges were used.
Catalona et al: J Urol 152:2037, 1994
Age related reference ranges improve specificity at the cost of sensitivity.
Free/Total PSA Ratio in Screening
Note that there are over 50 commercially available PSA assays available and all should have
different reference ranges, such is the complexity of the assay.
Measurement of free PSA is difficult and F : T ratios should be validated for each individual test.
Standardisation of these tests is difficult and not yet universal.
%Free PSA falls as prostate cancer develops.
Study
PSA range
F : T Ratio
Sensitivity loss
Specificity gain
Luderer
4 - 10
<20%
5%
15%
Catalona
>4
<20%
10%
38%
Free/Total PSA - Netherlands Schroder Study
9,600 men 54 - 76 years old screened with PSA, DRE and TRUS
4.3% cancer detection rate
5.1 biopsy to cancer ratio
64% of cancers specimen confined at radical prostatectomy
Best sole predictor of prostate biopsy is total PSA
Specificity of PSA in range 4 - 10 is improved with F : T ratio
F : T ratio < 20 in total PSA range 4 - 10
reduces biopsies by 38%
misses 12% of cancers
Schroder et al: Urologic Clinics of North America, May 1998
Years of Life Saved by Screening
Sensitivity analysis of years of life saved by prostate cancer screening using various estimates of the
natural history of prostate cancer.
Grade of disease
Years of life saved
without QOLA
Years of life saved
with QOLA
well differentiated
1.35
1.01
moderately ‘’
2.58
2.41
poorly
2.78
2.68
‘’
Chodak metanalysis: Urologic Clinics of North America May 1998
The years of life saved using assumptions of the natural history of prostate cancer compare favorably
to the years of life saved by other cancer screening programs.
Cost Effectiveness of Prostate CA Screening & Rx
Estimates used because no randomized controlled studies of the effectiveness of prostate cancer
screening have been done.
Years of life lost because of prostate cancer age 65 - 74 years
Grade
Well differentiated
Moderately ‘’
Poorly
‘’
Years of life lost
2.2
4.9
7.1
Cost per year of life saved by prostate cancer screening and Rx
Age range
50 - 69
60 - 69
50 - 69
Saving $US DRE + PSA
2339 - 3005
3905 - 5070
3574 – 4627
Benoit & Naslund: Urologic Clinics of North America, May 1998
Cost per Year of Life Saved By Various Interventions
Intervention
Smoking cessation counseling
Hypertension control
CABG
Renal dialysis
Liver transplantation
Screening mammography
Cervical cancer screening
Colon cancer screening
Cost per year of life saved $US
5,249 - 15,833
32,600
62,900
42,000 - 80,300
225,000
20,000 - 50,000
33,572
28,848 - 113,348
For prostate cancer, cost per year of life saved through PSA and DRE screening programs compares
extremely favorably with that for breast, cervix and colon cancer screening.
Benoit & Naslund: Urologic Clinics of North America, May 1998
Conclusion on the socio - economic implications of PSA Screening
Benoit and Naslund, Urologic Clinics of North America, May 1998
“Although men aged 50 - 75 years will potentially benefit the most from PSA screening, this benefit will
not be realised until these men are in their seventh and eighth decade of life.”
“Society must decide if the years of life saved in these men warrants the use of limited health care
resources.”
“This decision will be easier when randomised controlled trials are available to quantify the costs and
benefits of PSA screening.”
PSA screening – large trial results
Mortality Results From a Randomized Prostate-Cancer Screening Trial
Andriole et al NEJM 2009 360:13 1310-19
Randomized trial on 76,693 men, annual PSA screening on 38,343 men vs no screening on 38,350 between 1993 – 2001.
After 7 years, the incidence of prostate cancer per 10,000 person-years was 116 (2820 cancers) in the screening group
and 95 (2322 cancers) in the control group.
The incidence of death per 10,000 person-years was 2.0 (50 deaths) in the screening group and
1.7 (44 deaths) in the screening group.
Conclusion: After 7 to 10 years of follow up, the death rate from prostate cancer was very low and did not differ
significantly between the two study groups.
PSA screening – large trial results
Screening and Prostate Cancer Mortality in a Randomized European Study
Schroder et al NEJM 2009 360:13 1320-28
182,000 men between ages 50 – 74 years in seven European countries randomized to two groups with one group receiving PSA screening and the
other group not having PSA screening, recruited between 1991 and 2003.
During a median follow up of 9 years, the cumulative incidence of prostate cancer was 8.2% in the screening group and 4.8% in the control group.
The rate ratio for death from prostate cancer in the screening group as compared with the control group was 0.8.
The absolute risk difference was 0.71 deaths per 1,000 men.
This means that 1410 would need to be screened and 48 additional cases of prostate cancer would need to be treated to prevent one death from
prostate cancer.
Conclusion: PSA based screening reduced the rate of death from prostate cancer by 20% but was associated with a high risk of overdiagnosis.
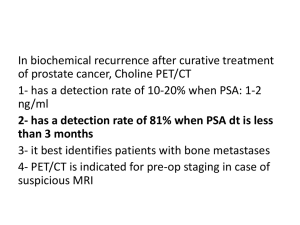
End of the PSA Era?
Diagnosis – TRUS Biopsy
Prostate biopsy is required for diagnosis, generally 11 biopsies taken
Transperineal prostate biopsy using trans rectal U/S (TRUS) and 18F “Biopty” guns originally developed by Jim
Anderson, interventional radiologist at RPH in 1989 using freehand technique.
All TRUS biopsies done by Jim Anderson using this technique under local anaesthetic up to around 2000 with no
antibiotic prophylaxis used. Rare septicaemia if patient had UTI/prostatitis at the time of biopsy (handful of cases over
10 years and around 18,000 TRUS biopsy episodes).
TRUS biopsy largely taken over by urologists around 2000 using trans rectal approach under general anaesthetic.
“Lists of TRUS biopsies”.
3% Gram negative septicaemia rate with transrectal biopsy despite antibiotic prophylaxis.
Now a move nationally by urologists over the last 12 months to move on to transperineal biopsy because of concerns
over septicaemia and antibiotic prophylaxis.
Many urologists have this technique from brachytherapy seed placement anyway but this is now being workshopped
by urologists in the Eastern States.
Diagnosis - Prostate “Multiparametric” MRI
New computer software enhancement of contrast MRI is providing more accurate assessment with
“Multiparametric” MRI scanning:
“Dynamic Contrast Enhanced” imaging DCE
“Diffusion weighted imaging” DWI - Difference in Brownian motion of water molecules in cancer
vs normal tissue.
Currently at RPH, 1.5 Tesla external MRI with multiparametric processing, DCE and DWI.
1.5 Tesla vs 3.0 Tesla – possibly not as important as image processing and analysis.
Endorectal coil 3.0 T claimed up to 98% specific and up to 86% PPV with DCE.
MR Spectroscopy up to 93% PPV
Current role seen as a localising test for targeted biopsy after negative biopsy with ongoing PSA rise.
CURRENTLY SHOULD NOT BE USED AS A DIAGNOSTIC TEST WITH AN ABNORMAL PSA TO
AVOID BIOPSY.
Diffusion Imaging
(Brownian motion)
T2 Axial NAD
Colour map
T2 Axial Slightly
More rostral
Colour map
graph
DWI
ADC
Axial Ultrasound
Lesion visible Hypoechoic
11 oc ext ant
Transperineal systematic cores (11 systematically) additional 2 cores from presumed index
lesion at 11 oclock (13 cores in total) 8mm,13mm and 10 mm acinar Adenocarcinoma 11 oclock
(Slide courtesy of Jim Anderson)
Prevention
Castrate all adolescent males - prostate cancer unknown in eunuchs in China.
Diets high in phytoestrogen - SE Asian populations and low cancer incidence.
African americans - high testosterone and high incidence of prostate cancer.
“Chemoprevention” – 5 alpha reductase inhibitors finasteride and dutasteride
Effective but caution due to relative increase in high grade prostate cancer incidence FDA warns:
The results of the PCPT trial showed that men on the finasteride arm had a 24.8% overall lower risk of being diagnosed with
prostate cancer when compared to the placebo arm (p<0.0001). The reduction in risk of prostate cancer was limited to Gleason
score (GS) 6 or lower prostate cancers. However, there was an increased incidence of GS 8-10 prostate cancers with finasteride
versus placebo (1.8% versus 1.1%, respectively).
The results of the REDUCE trial showed that men on dutasteride had a 23% overall lower risk of being diagnosed with biopsy
detectable prostate cancer when compared to men on placebo (p<0.0001). This overall risk reduction was limited to a decrease
in GS 6 or lower prostate cancers. In contrast, there was an increased incidence of GS 8-10 cancers with dutasteride versus
placebo (1% versus 0.5%, respectively).
Prevention - Finasteride
USA Prostate cancer prevention trial 1993 – 2003
18,882 men with PSA < 3 and normal DRE enrolled.
5 mg of Finasteride per day or placebo.
Study closed 15 months before planned closure because overwhelming evidence that
the primary end point (prostate cancer prevalence) had been met.
24.8 % reduction in prostate cancer risk.
Increased proportion of high grade prostate cancers diagnosed from 1.1% to
1.8%raised (and more likely cause of early closure). Prompted FDA warning.
Subsequent analysis suggests finasteride “improved sensitivity of PSA for cancer
overall, and especially for high grade cancer”.
The Influence of Finasteride on the Development of Prostate Cancer.
Thompson et al
NEJM 2003; 349: 215
Expectant Management
“Watchful waiting” PSA between 4-10, do repeat PSA at regular intervals, 3 to 6 monthly, act when
certain parameters breached.
Pre biopsy - lower chance of cure with higher PSA due to interval progression, significant drop in
cure rates once PSA>10.
Post biopsy - little rational basis, chance of successful curative therapy must drop over time (albeit
slowly in many cancers).
However, ~50% chance of death from prostate cancer over 10 years without treatment in stage T1c
prostate cancer Gleason 7, few +ve biopsies.
Patients should have management options discussed and have a clear course of action in their
minds prior to having PSA test.
Ask “what if ?” prior to PSA testing.
Expectant Management
Albertsen et al
Cancer
Competing Risk Analysis for Men Aged 55 to 74 Years at Diagnosis Managed Conservatively for Clinically Localised Prostate
JAMA 280(11), 975 1998
Radical Prostatectomy
Cure 80% PSA 4-10, Gleason < 7, Stage T1c (Positive margin rate average
30% in Perth)
This group of patients have 10 - 20 % mortality from prostate cancer without any
treatment over 10 year time frame, depending on age (see previous).
Cure 50% PSA 10-15, generally higher stage.
Morbidity 10% incontinence
80% impotence
0.5% death
blood transfusion, rectal injury, lymphocoele
“PSA recurrence” = not cured
Rx radiotherapy (? 1/3 cured)
hormonal manipulation
? Better local control ? Better survival in this group
Puboprostatic Ligaments and Endopelvic Fascia
Dorsal Vein Ligation
Neurovascular Bundles
Neurovascular Bundle preservation
Radical Prostatectomy
•
Open radical retropubic prostatectomy
Now 4 – 5” midline incision
3 – 4 days hospital stay
2 – 3 weeks indwelling catheter
Laparoscopic radical retropubic prostatectomy
2” incision + port sites
2 – 3 days in hospital
1 – 2 weeks indwelling catheter
More rapid return to work
•
Cancer outcomes the same for open vs laparoscopic radical prostatectomy
•
Slightly lower impotence rate for laparoscopic radical prostatectomy
•
Slightly higher complication rate for laparoscopic radical prostatectomy, including rectal injury
•
Robotic radical prostatectomy
Robotic Radical Prostatectomy
Da Vinci robot developed through the 1990’s and given approval by US FDA in 2000.
Installed SJOG Subiaco in 2008.
Purchase cost $3 million in Australia with $300,000 yearly maintenance fees.
Cost $4,000 per case in disposable instruments.
Patient out of pocket costs $7,000 - $8,000 per procedure in Perth.
Four interactive robotic arms controlled from the console.
Endoscopic camera with two lenses gives the surgeon full stereoscopic vision from the console.
Da Vinci Robot
Robotic Radical Prostatectomy
2012 in USA 367,000 robotic operations performed (all, including prostate).
1,400 hospitals in USA have at least one Da Vinci robot.
Cancer outcomes no different.
Complication rate the same as manual laparoscopic radical prostatectomy.
Incontinence
7% vs 2% open radical prostatectomy Lepor et al Reviews in Urology 2005 Summer; 7(3): 115–127
Impotence
25% vs 30% “
“
“
“
Rectorethral fistula 0.53% overall with no good comparison laparoscopic/robotic/open
“
Hospital stay the same as manual laparoscopic radical prostatectomy, all lapararoscopic
prostatectomy 1 – 2 days shorter hospital stay than open radical prostatectomy.
Radiotherapy – External Beam
Results suggest efficacy equal to radical prostatectomy, but staging difficulties and poor data.
Comparison of the efficacy of local therapies for localized prostate cancer in the prostate-specific antigen era: a large single-institution
experience with radical prostatectomy and external-beam radiotherapy.
Kupelian et al Cleveland Clinic J Clin Oncol 2002 Aug 15;20(16):3376-85.
CONCLUSION:
Eight-year biochemical failure rates were identical between radiotherapy and surgery in any subgroup. Outcome is
determined mainly by pretreatment PSA levels, bGS, clinical T stage, and, for RT patients, radiation dose.
MD Anderson data shows external beam DXRT much better outcomes with higher doses, around 76 Gray, hence newer image guided
radiotherapy should be more effective
Six week treatment
Morbidity
Pretreatment hormonal manipulation 6 months appears to improve cure rate.
•
2% radiation proctitis
2% radiation cystitis
- 50% impotence within first year, increasing thereafter
- insignificant incontinence
Bladder cancer in 0.58% of 342,937 men treated for CA prostate, twice as likely in DXRT vs
radical prostatectomy
Secondary Bladder Cancer After Radiotherapy For Localized Prostate Cancer
Abern et al Chicago, IL
(AUA presentation) J Urology 185, No. 4S, Supplement May 2011
Image Guided Radiotherapy IGRT and IMRT
Image guided linear accelerators used to target the prostate.
IMRT Intensity modulated therapy advanced 3DCRT is now further refined.
Gold seed fiducial markers placed trans perineally using trans rectal U/S.
CT scan imaging data used for planning.
Cone beam flat panel CT used for targeting.
Allowing dose escalation to 78 – 86 Gy (? Use of hydrogel spacer for rectal separation).
Reduced risk of significant complication to 1- 2%.
Long term outcome data not available but early biochemical control (PSA) improved.
IGRT
LDR Brachytherapy - Seeds
I125 seeds implanted in prostate with transperineal needle application.
Survival Among Men With Clinically Localized Prostate CancerTreated With Radical Prostatectomy
or Radiation Therapy in the Prostate Specific Antigen Era Kibel et al J Urology
187, Issue 4, April 2012,1259-1265
The adjusted 10-year prostate cancer specific mortality was ;
1.8% (95% CI 1.6–2.1) Radical prostatectomy 6, 485 patients
2.9% (95% CI 2.6–3.3) External beam DXRT
2,264
“
2.3% (95% CI 2.0–2.6) LDR Brachytherapy
1,680
“
10,429 consecutive patients with localized prostate cancer in 2 centres,
Cleveland Clinic and Barnes-Jewish Hospital (St Louis)
~ 70% Stage T1C, 25% T2
~ 75% Gleason 6, 25% Gleason 7
(External beam DXRT generally higher stage and grade)
$18,000 cost currently in Perth (SCGH).
Brachytherapy - HDR
Control rod needles positioned under GA with TRUS day before
Stabilizing template sutured to perineum, dosimetry figured by physicists/radiotherapist, needles connected to HDR
machine
Iridium 192 radioactive wire source inserted via established needles, with dwell time and location governed by pre
programmed HDR machine
Time on machine relatively short – minutes
Template and needles removed at the end of procedure
High doses of radiotherapy delivered with low morbidity
Generally given an external beam “boost”
Treatment at SCGH, generally reserved for high grade, poor prognosis localized disease (high risk)
High Dose Rate (HDR) Brachytherapy with Conformal Radiation Therapy for Localized Prostate Cancer
Deger et al
Five-year progression free survival:
European Urology Volume 47, 4, April 2005, Pages 441–448
81% in the low risk group,
65% in the intermediate risk group
59% in the high risk group
HIFU
High Intensity focused ultrasound with TRUS targeting.
Acoustic energy converted to heat in tissue with thermal tissue injury.
Outpatient procedure lasting 1 – 3 hours.
Cancer outcomes:
Fourteen-year oncological and functional outcomes of high-intensity focused ultrasound
in localized prostate cancer.
538 patients
Ganzer et al
BJUI August 2013 112,3 322–329
mean follow up 8.1 years mean age 67.7 years 490 ≤ Gleason 7 221 stage T1 296 stage T2
TURP performed 4 -6 weeks prior to HIFU if prostate > 30 gm
Actuarial BDFS 5 years: 81%
Biochemical disease free survival Phoenix criteria (PSA nadir+2 ng/mL)
10 years: 61%
Mean PSA nadir 0.4
297 patients biopsied 25.6% biopsies showed cancer
Cancer specific deaths 3.3%
Complications:
rectorethral fistula
bladder outflow obstruction
urine incontinence
impotence @ 12 months
0.7%
28%
2.8%
75%
Not as yet available in WA but available in Melbourne and Sydney
4 patients
HIFU
2 machines available:
Sonotherm and Ablatherm
HIFU
Clinical Management
Palliative therapy for metastatic disease
Hormonal manipulation
Castration
Estrogens
LHRH analogues
Antiandrogens
Intermittent hormone manipulation
Abiraterone
Ketoconazole
Chemotherapy
Mitoxantrone
Docetaxel
Carbazetaxel
Immunotherapy
Sipileucel T
Injectable radiotherapy
Strontium
Radium
Targeted therapy ?
Palliative Hormonal Manipulation - Castration
Studies on Prostatic Cancer I.
The Effect of Castration, of Estrogen and of Androgen Injection on Serum Phosphatases in
Metastatic Carcinoma of the Prostate*
Charles Huggins, M.D., and Clarence V. Hodges,M.D. Chicago, Illinois
Cancer Res 1941;1:293-297
“3. In prostatic cancer
with marked elevation of acid phosphatase, castration or injection of large amounts of estrogen caused a sharp
reduction of this enzyme to or towards the normal range. Alkaline phosphatase values rose following castration and then decreased, but
more slowly than acid phosphatase. In certain cases, these values reached and were maintained in a normal range during the period of
observation, 180 days, while in other patients the values were slightly above normal.”
Huggins awarded Nobel Prize in Medicine in 1966 for his work on prostate cancer
Response rate:
80% respond with biochemical and clinical remission
Response duration:
Catalona and Scott J Urol 119, 1-8 1978
Most patients with metastatic disease demonstrate hormone manipulation resistance within 18 – 24 months
Average survival 3 – 5 years on hormone manipulation when presenting with metastatic disease
Early vs delayed hormonal manipulation:
VACURG study 1967 showed no survival difference with early vs delayed therapy
Palliative Hormonal Manipulation - Estrogens
•
Estrogen therapy shown to be effective in Huggins and Hodges 1941 study with stilbestrol 1 mg I/V
or estradiol 1.66 to 3.32 mg I/V Cancer Res 1941;1:293-297
Estradiol (given I/M and orally) shown to be more effective palliation than castration in palliation of
metastatic prostate cancer with ~ 25% better survival at 2 years in high grade cancer, but with
higher cardiovascular mortality in the estrogen treated group.
Haapiainen et al BJU (1986) 58, 528 - 533
Thromboembolism risks
Stibestrol used as an alternative to castration up until the arrival of LHRH analogues (1993 PBS Aus)
dosage 1mg – 3mg per day
•
Some resurgence in the 1990’s as second line hormonal manipulation
Palliative Hormonal Manipulation – LHRH Analogues
•
•
•
•
Goserelin (Zoladex) was the first LHRH analogue licensed for use FDA 1989 TGA 1991
initially 3.6 mg monthly S/C pellet injection, later 10.8 mg 3 monthly S/C pellet injection
Synthetic analogue of LHRH, now also Leuprorelin (Lucrin) and Triptorelin (Diphereline available as 6 months dose)
Works by binding to the LHRH receptor cells in the pituitary gland leading to an initial increase in production of
luteinizing hormone which gives an initial increase in the production of testosterone, with potential tumour flare.
Initial flare may be treated by co-prescribing/co-administering antiandrogen (CPA, Bicalutamide etc).
After a period of about 14–21 days, production of LH is greatly reduced due to receptor downregulation, and
testosterone is reduced to castrate levels.
•
Same efficacy as castration in management of metastatic prostate cancer
•
Side effects: impotence, hot flushes, weight gain, depression, osteoporosis (same as for castration)
•
Cost is $1108.97 for a 10.8 mg injection to the government ($4,435.88 per year), on PBS either $5.90 ( for concession
holders) or $36.10 to the patient.
Palliative Hormonal Manipulation - Antiandrogens
Steroidal antiandrogens directly affect gene expression due to their fat-soluble nature that allows
them to diffuse through the plasma membrane’s phospholipid bilayer and prevent the binding of
testosterone and dihydrotestosterone (DHT) to androgen receptors inside the cancer cell.
Cyproterone acetete 100 mg bd as monotherapy may preserve sexual function whilst controlling prostate cancer, but
mainly used to prevent “flare” on initiation of LHRH analogues or as second line hormonal manipulation with “hormone
resistance” (failure of LHRH analogue or castration) –
Non-steroidal antiandrogens counter androgens and have no steroidal effects. Antiandrogens act by
blocking androgen receptors on the cancer cell surface
Flutamide, Nilutamide and Cosudex
Second line hormonal manipulation (adding to LHRH analogue or castration) can lead to a PSA
response of 50% or greater in 4%–50% of patients. The median duration of response is between 4.0
and 11.0 months.
Rotation through steroidal and non steroidal antiandrogens can give prolonged remission in some
Palliative Hormonal Manipulation – Intermittent Hormonal Manipulation
•
Bruchovsky from Vancouver first published on this in 1990
Large multicenter trial of intermittent hormonal manipulation (IADT) vs continuous hormonal
manipulation (CADT) in 383 patients published in 2012 showed no statistical difference in either
overall survival or progression free survival between intermittent or continuous therapy and no
difference in quality of life scores. Poor study with some randomized and some non randomized.
Intermittent hormonal therapy in the treatment of metastatic prostate cancer: a randomized trial
Mottet et al
•
BJUInternational 2012 | 110, 1262–1269
One small trial in 2002 suggested benefit but subsequently several large trials showing no real
benefit. Some subjective improvement in quality of life thought to occur.
•
Anecdotally useful in low bulk disease, i.e. failure of curative therapy for localized disease
•
Problematic in advanced symptomatic disease
•
In high bulk disease, treat until PSA nadir achieved (average ~ 7 months) then observed without
treatment until predetermined PSA rise reached – predetermined PSA rise different in different
centres (PSA 10 in the above study)
Chemotherapy - Docetaxel
Randomized trial of Docetaxel vs Mitoxantrone (both with prednisolone) published in NEJM 2004
The median survival was 16.5 months in the mitoxantrone group vs 18.9 months in the group given
docetaxel every 3 weeks.
Among these two groups, 32 percent vs 45 percent of men, respectively, had at least a 50 percent
decrease in the serum PSA level (P<0.001 for both comparisons with mitoxantrone)
22 percent vs 35 percent (P = 0.01) had predefined reductions in pain
13 percent vs 22 percent (P = 0.009) had improvements in the quality of life
Adverse events were also more common in the groups that received docetaxel
Docetaxel plus Prednisone or Mitoxantrone plus Prednisone for Advanced Prostate Cancer
Tannock et al
NEJM 351;15 October 7, 2004
New Palliative Therapies For Advanced Disease
ABIRATERONE
Developed at the Institute for Cancer Research (starting with ketoconazole), Royal Marsden and patented in 1993.
Inhibits 17 α-hydroxylase/C17,20 lyase (CYP17A1)
CYP17 catalyzes two sequential reactions:
(a) the conversion of pregnenolone and progesterone to their 17-α-hydroxy derivatives by its 17 α-hydroxylase activity
(b) the subsequent formation of dehydroepiandrosterone (DHEA) and androstenedione respectively, by its C17,20 lyase activity
Current intracrine and paracrine theory for failure of hormonal manipulation.
2010 interim results of phase III clinical trial in previously treated docetaxel overall survival was increased by 3.9 months (14.8 months
versus 10.9 months for placebo).
70% show significant PSA reduction.
Works better in men with ERG proto-oncogene = ETS (erythroblast transformation- specific) related gene
ERG protein is a transcription regulator
Approved by the FDA in April 2011
Placed on PBS Australia August 2013 for failed hormone manipulation followed by failed chemotherapy with Docetaxel
Annual cost ? $40,000
Single daily tablet 1gm (on empty stomach) administered with prednisolone 5mg b.d.
Side effects:
hypertension, fluid retention, CCF and hypokalemia
adrenal insufficiency
elevation of ALT and AST
New Palliative Therapies For Advanced Disease
CABAZITAXEL
A semi-synthetic derivative of a natural taxoid.
It was developed by Sanofi-Aventis
Approved by the U.S. Food and Drug Administration (FDA) for the treatment of
hormone-refractory prostate cancer in June 2010.
It is a microtubule inhibitor.
Phase III trial with 755 men for the treatment of hormone-refractory prostate cancer
median survival was 15.1 months for patients receiving cabazitaxel versus 12.7
months for patients receiving mitoxantrone.
Used with prednisolone.
Approved by TGA but rejected PBS listing in 2011 for patients with metastatic
hormone refractory prostate cancer having failed docetaxel as well.
New Palliative Therapies For Advanced Disease
SIPULEUCEL-T
Immunostimulant therapy.
A course of Sipuleucel-T treatment consists of three basic steps:
1. A patient's own white blood cells, primarily antigen-presenting cells (APCs), also called dendritic cells, are
extracted in a leukapheresis procedure.
2. The blood product is sent to the factory and incubated with a fusion protein (PA2024) consisting of two parts,
a) The antigen prostatic acid phosphatase (PAP), which is present in 95% of prostate cancer cells, and
b) An immune signalling factor granulocyte-macrophage colony stimulating factor (GM-CSF) that helps the
APCs to mature.
The activated blood product (APC8015) is returned from the factory to the infusion center and re-infused into the
patient to cause an immune response against cancer cells carrying the PAP antigen.
A complete Sipuleucel-T treatment repeats three courses over the span of a month, with two weeks between
successive courses.
IMPACT trial served as the basis for licensing approval of Sipuleucel-T by the FDA in 2010. This trial enrolled 512
patients with asymptomatic or minimally symptomatic metastatic HRPC randomized in a 2:1 ratio. The median
survival time for Sipuleucel-T patients was 25.8 months comparing to 21.7 months for placebo-treated patients.
Overall survival was statistically significant The longer survival without tumour shrinkage of change in progression
may suggest the effect of an unmeasured variable.
A course of treatment in Australia apparently $120,000.
New Palliative Therapies For Advanced Disease
RADIUM-223 CHLORIDE
Phase III clinical trials showed a 2.8 months increase in median overall survival due to the drug as compared to
placebo (the increase was from 11.2 months to 14.0 months) in 922 patients.
May 2013 FDA approval as a treatment for failed hormonal manipulation with symptomatic bone metastases and
without known visceral disease.
Alpha radiation from radium-223 decay to kills prostate cancer cells. Radium-223 targets to bone tissue by virtue of its
chemical similarity to calcium. Alpha radiation has an effect over a range of 2-10 cells, which is short-range when
compared to current intravenous radiation therapy which is based on beta or gamma radiation, and, therefore, causes
less damage to surrounding healthy tissues. Radium-223 has a half life of 11.4 days, making it suitable for cancer
treatment.
(Strontium 89 (Metastron) has been in use since 1992 for the same circumstances but 50 day half life – Beta radiation).
Side effects
Nausea, diaorrhea, vomiting and swelling of the leg, ankle or foot. The most common abnormalities detected during
blood testing were anaemia, lymphocytopenia, leukopenia, thrombocytopenia and neutropenia. Excreted by the gut.
In clinical trials, radium-223 chloride was administered by intravenous injection once a month for 4 or 6 months.