inpatient blood glucose control

BLOOD GLUCOSE
CONTROL
A learning module for Staff
How to Use this Module
• Use this module to educate staff on glucose control.
• Sample slides have been prepared on identifying and managing patients with hyperglycemia.
• You may copy and paste your facility order sets and add your own key points to match your policy and protocols.
Blood Glucose Control
Objectives
1.
The importance of blood glucose control in surgical patients.
2.
Understand the pathophysiology related to hyperglycemia and safety.
3.
Educate staff to the policies, procedures, and protocols.
Why is Blood Glucose Control so
Important in the Perioperative Setting?
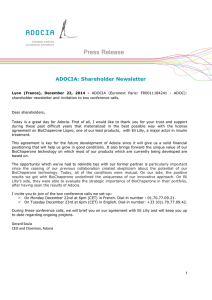
Hyperglycemia vs No Hyperglycemia
All Patients
16
14
12
10
8
6
4
2
0
30% of all hyperglycemic patients were not diabetic!
All p<0.01
Normal
Gluc>180
All Pts Bariatric Colectomy
SCOAP data courtesy of Sung (Steve) Kwon
Pathophysiology of Hyperglycemia
RECEPTOR DEFECT
GLUCOSE
INCREASED GLUCOSE
PRODUCTION
INSULIN
RESISTANCE
DECREASED INSULIN PRODUCTION
‘Stress’ Hyperglycemia-What Happens?
• Cytokines/inflammatory mediators contribute to:
• Inability of immunoglobulin to bind with surface of invading bacteria so decreased bacteriocidal capacity.
• Impaired platelet function 54% increased blood stream infections
59% increase acute renal failure requiring dialysis and 50% increase in blood transfusions.
• Relative hypoinsulinemia contributes to:
• Decreased insulin sensitivity.
• Unrestrained free fatty acids and hepatic fatty acids.
• Increased ketone bodies and metabolic acidosis.
• Impaired myocardial contractility and larger infarct sizes.
• Glycosuria induced osmotic diuresis and extracellular K+ shift.
Berghe, 2001; Goldberg & Inzucchi, 2005
Adapted from Whitman, 2012 WSHA Webcast
Resulting Complications of Hyperglycemia and Stress Hyperglycemia
Decreased tissue perfusion
Impaired metabolism
Pro-thrombotic state
Impaired cardiac function
Pro-inflammatory state
Decreased wound healing
Braitwaithe, et al. 2008; Adapted from Inzucchi, Magee, & O ’ Malley, 2010
Image retrieved from: http://pennstatehershey.adam.com/content.aspx?productId=42&pid=42&gid=000254
Adapted from Whitman, 2012 WSHA Webcast
Physiologic Insulin Secretion:
Basal/Bolus Concept
50 Nutritional Insulin
25
0
Basal Insulin
Breakfast Lunch Dinner
Suppresses Glucose
Production Between Meals
& Overnight
150
100
Nutritional Glucose
The 50/50 Rule
50
Basal Glucose
0
7 8 9 10 11 12 1 2 3 4 5 6 7 8 9
A.M.
P.M.
Time of Day
Adapted from
Maynard & Wesorick, Society of Hospital Medicine, 2008 J.
Whitman, Perioperative Glucose Control, Webcast 2012
Current Best Practices
• Insulin infusion:
• If NPO and unstable .
• Basal insulin:
• Covers the baseline insulin needs.
• Essential for all type 1 diabetics to prevent ketosis.
• In most cases should be given even if patient is NPO.
• Nutritional insulin:
• Covers increases in serum glucose after caloric intake.
• Correctional insulin:
• Additional to scheduled nutritional dose.
Wisse, 2012
Adapted from Whitman, 2012 WSHA Webcast
Oral Hypoglycemic Agents
STOP
Why Not Sliding Scale?
Insulin
Insulin
Insulin
Insulin
Target range
Theoretical glucose levels with SSI
Adapted from Whitman, 2012 WSHA Webcast
Perioperative Blood Glucose Control
Protocols and Standing Orders
Perioperative Blood Glucose Control Protocol
Insulin Pump Standing Orders
SQ Insulin Standing Orders
Pre-Operative Period
• ALL patients with a blood glucose of 180mg/dl and greater.
• Regardless of diabetes diagnosis or not.
• NOT to be used on OB patients, 23 hour admits or those admitted with
DKA or HHS
(hyperglycemic crises)
Review the protocol
Intra-operative Glucose Control
Period
• Measure BG at induction and 1h into case.
• Anesthesia associated with hyperglycemia even in non-diabetic subjects.
• Measure BG every 1h in Type 1 DM patients.
• Method of glycemic control intra-operatively.
• IV insulin (DM1, critically ill, neurosurgery,
TBI).
• Basal insulin with bolus correction doses.
• Some hospitals have placed glucometers on every anesthesia cart.
Wisse, 2012
Post-Operative Period
• Initiate for BG >140 mg/dL x2 or >180 mg/dL range
• Goal range 110-180 mg/dL
• Standard infusions are regular insulin
100ml/100 units on a dedicated line
Post-Operative Period
(cont)
• Check BG every hour until at goal
• Then decrease BG checks to every 2 hours
• Hourly checks should always be resumed if patient falls outside of goal range
Key Steps in Transitioning Off the
Insulin Pump Suggested Criteria
• BG range 90-140 mg/dL .
• Do know criteria for transitioning off insulin pump
• Stable insulin infusion rate.
• Nutrition intake is current or anticipated.
• DO overlap SC and IV Insulin. Minimize
• Need last four hours of insulin drip data.
hyperglycemia because of short ½ life of IV insulin.
• DO use rapid analogs (Apidra) after meal if uncertain patient will eat.
• DO expect basal and nutritional insulin if patient is eating.
• DO ensure adequate food intake when switching patients with ketotic diabetes to SC insulin
• DO arrange for follow-up post hospitalization even if insulin is temporary.
Carlson, et al., 2006
Adapted from Whitman 2012 WSHA Webcast
Transition Algorithm
SKAGIT REGIONAL HEALTH
SKAGIT VALLEY HOSPITAL
SKAGIT REGIONAL CLINICS INSULIN SUBCUTANEOUS PROTOCOL
Attention Physician: All must be checked to initiate order • Transition any time of day.
• Give basal insulin 2hrs
Blood Glucose (BG) Goals:
Pre-meal Goal - 90-150mg/dL or HgA1C
Goal Postprandial BG:
HS Goal 90-180mg/dL or
Goal for BG @ 3 am or every 6 hours if NPO
Blood Glucose (BG) Monitoring Frequency:
Before meals & at bed time 2 hours after meals 2-3AM
• If transitioning from IV insulin see Transition Protocols
Basal Insulin: Give units of Glargine (Lantus)
• prior to stopping IV
Nutritional
Post-Breakfast
Give units of
Post-Lunch
Give units of
Post-Dinner
Give units of
Bedtime
Give units of
Insulin Glulisine (Apidra) Glulisine (Apidra) Glulisine (Apidra) Glulisine (Apidra) insulin.
• TDD of SC basal insulin =
Correction Algorithm for Hyperglycemia: To be administered IN ADDITION TO the scheduled insulin dose to correct pre-meal BG.
• Administer correctional insulin immediately post meal Low Medium High Individualized Algorithm
• Give full dose if 50-100% of meal eaten
• Give half dose if less than 50% of meal eaten
• If BG check is every 6 hours for NPO patient, use the pre-meal Algorithm Insulin doses
• Correction insulin type will be the same type as nutritional insulin
IV units insulin used last
MANDATORY BG CHECK AT 3AM IF BEDTIME CORRECTIONAL INSULIN GIVEN. IF 3AM BG > 150mg/d USE BEDTIME BG DOSING
4 hrs x 5.
Also give nutritional insulin if timing with a meal .
LOW DOSE ALGORITHM
(For patients requiring less than 40 units insulin/day)
Premeal BG
150-199
200-249
Additional Insulin
1 unit
2 units
250-299
300-349 greater than 349
Bedtime / 3am BG
150-199
200-249
250-299
300-349 greater than 349
3 units
4 units
5 units
Additional Insulin
None
1 units
2 units
3 units
4 units
MEDIUM DOSE ALGORITHM
(For patients requiring 40 to 80 units insulin/day)
Premeal BG
150-199
200-249
Additional Insulin
1 unit
3 units
250-299
300-349 greater than 349
Bedtime / 3am BG
150-199
5 units
7 units
8 units
Additional Insulin
200-249
250-299
300-349 greater than 349
None
2 units
3 units
5 units
7 units
HIGH DOSE ALGORITHM
(For patients requiring more than 80 units insulin/day)
Premeal BG Additional Insulin
150-199
200-249
250-299
300-349
2 units
4 units
7 units
10 units greater than 350
Bedtime / 3am BG
150-199
200-249
250-299
300-349 greater than 349
12 units
Additional Insulin
None
2 units
5 units
7 units
10 units
INDIVIDUALIZED ALGORITHM
(For patients requiring an individualized protocol)
Premeal BG Additional Insulin
150-199
200-249
250-299
300-349 greater than 350
Bedtime / 3am BG
150-199
200-249
250-299
300-349 greater than 349
Additional Insulin
Hypoglycemia Protocol for blood glucose less than 70mg/dL
A. If pt can take PO, give 15 grams of fast-acting carbohydrate (120mL apple/orange juice, 240mL nonfat milk)
B. If patient cannot take PO, give 25mL of D50 as IV push
C. Check finger-stick glucose every 15-20 minutes until BG above 100mg/dL
Date: Time: Provider Signature:
S5194
02/23/2012
Page 1 of 1
Signs and Symptoms of Hypoglycemia
• Sweating
• Hunger
• Irritability
• Pallor
• Anxiety
• Dizziness
• Shakiness
• Headache
• Confusion
• Tachycardia
• Trembling
• Weakness
Hypoglycemia can occur without symptoms, so it is important to check blood glucose levels regularly.
Adapted from Whitman, 2012 WSHA Webcast
Treating Hypoglycemia: 3 Steps
Give 15g of glucose or Wait 15 mins Recheck BG – give another fast-acting another 15g if carbohydrate necessary
• 4oz (1/2 cup) fruit juice * Assess for cause
• 8 oz (1 cup) milk
• 1 Tbsp honey
• IV Dextrose
Goal to restore BG above 100
Avoid overtreatment (excessive amount of glucose), which may result in significant hyperglycemia over next 4-6 hrs.
Adapted from Whitman, 2012 WSHA Webcast
PATIENT CARE FLOW SHEET:
Blood Glucose Section
The section of this documentation form is appropriate for all nurses to review whether they are on Med/Surg, Telemetry, or
Critical Care units.
Documentation of blood glucose control issues include documenting the hyperglycemia and hypoglycemia as well as the treatment. Look closely at this section:
Smooth Transition:
Inpatient to Outpatient
• If discharging patient new to insulin:
• Make the decision as early as possible.
• Teach, teach, teach.
• Early follow-up a must.
• Pens vs. vial/syringe.
• If changing outpatient regimen significantly:
• Communicate with PCP.
• Document rationale.
• Educate patient.
Wisse, 2012,
Adapted from Whitman 2012 WSHA webcast
THE FINISH LINE!!!
CONGRATULATIONS!
You have finished the
Surgical Glucose Control:
Policies, Procedures, and Protocols
Learning Module
If you have any questions, please contact your Clinical Educator, your unit’s Diabetes Champion, or one of the Diabetes Educators.