part_ii_-_ladis_com_june_2014
advertisement

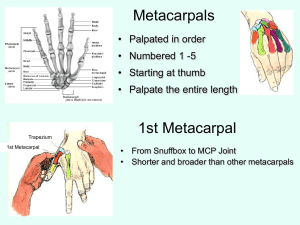
Bilateral Forelimb Lameness in an 11 year-old Thoroughbred Drs. Karyn Labbe and Beth Biscoe, Washington State University Dr. John Mattoon, Washington State University Bilateral forelimb lameness in an 11 year-old Thoroughbred • Patient is a previous racehorse acquired by the owner with the intended use of barrel racing • History of intermittent lameness in both forelimbs noticed by the owner 9 months prior • No improvement was seen with a prolonged period of stall rest Primary Veterinarian Workup • Injection of both fore coffin joints resulted in transient lameness improvement for 3 months • Referring radiographs of the left front foot revealed moderate navicular bone degeneration Lameness evaluation at presentation • Patient showed a grade II/V left fore lameness, which was exacerbated by left circling • Left fore palmar digital nerve analgesia resolved the left fore lameness and resulted in the horse displaying a grade III/V right fore lameness • Right fore palmar digital nerve analgesia improved the RF lameness greater than 75% Further Imaging • The decision was made for MRI of both fore feet • Nail screening radiography prior to MRI identified a type II fracture of the right fore third phalanx Advanced Imaging MRI Left Front Foot Region • MRI Proton Density (PD) transverse images shown • Distal to proximal • 2 vitamin E capsules were placed along lateral side MRI Left Front Foot Region Sagittal Plane • Proton Density sagittal plane • Lateral to medial MRI Findings Left Front Foot Region • Multifocal areas of hyperintensity associated with both lobes of the deep digital flexor tendon • Symmetrical biaxial lobes of tissue isointense to the DDFT that span from the palmar margin of the distal navicular suspensory ligament proximally and axially to merge with the DDFT lobes/fibrocartilaginous dorsal DDFT border • Hypointense tissue in the navicular bursa between the navicular suspensory ligament and dorsal-axial margin of the DDFT lobes, likely represent adhesions MRI Findings (continued) • Enlargement and heterogenous intensity of the impar ligament • Avulsion fragment of the distolateral border of the navicular bone at the impar attachment • Marked thickening of the distal digital annular ligament Follow-Up • Due to the poor prognosis for competitive use as a barrel horse, the patient was retired Commentary • This case was selected because of the described biaxial symmetrical lobes of tissue between the navicular suspensory ligament and the DDFT • A symmetrical finding was found in the contralateral forelimb • Due to the bilateral symmetry, the tissue likely represents a congenital anatomic variant Right Front, PD transverse Commentary (continued) • It is considered that the relationship of the tissue connecting the DDFT dorsal border and the navicular suspensory ligament may have altered the biomechanics of the distal limb (especially with extension of the DIP joint) • This may have placed additional strain on the DDFT distal to the site of tissue attachment, predisposing it to tendinopathy Commentary (continued) • The palmar carpal ligament extends distally to form the accessory ligament of the DDFT (inferior check ligament). No reports of additional DDFT accessory ligaments or a tripartite DDFT at the level of P2 were found in a literature search but are considered present in this horse, discovered in both the left and right forelimbs Commentary (continued) • The “T ligament” is described anatomically as vascular connective tissue separating synovial structures in the palmar foot, including palmar pouch of the coffin joint, proximal recess of the navicular bursa and distal recess of the digital tendon sheath • Although the observed tissue in the sagittal images was in a similar location as the T ligament, the tissue displayed hypointense signal similar to dense collagen connective tissue comprising tendons and not the typical “T ligament” Commentary (continued) • Fibrinous adhesions can form between the navicular suspensory ligament and DDFT. Over time collagen can be deposited resulting in a fibrous adhesion. However, due to the biaxial symmetry as well as bilateral symmetry of the discrete bundles discovered in this horse, fibrous adhesions are thought a less likely explanation Commentary (continued) • It was also interesting to evaluate the right fore type II third phalanx fracture on MRI • The bone margins at the fracture site were PD hypointense consistent with sclerosis, but did not demonstrate hyperintensity on STIR sequences Commentary (continued) • Characteristics of this fracture on MRI support a chronic fracture that has healed by a fibrous union, associated with the vestigial periosteum of the coffin bone (Butler JA, Colles CM, Dyson SJ, Kold SE, Poulos PW. Clinical Radiology of the Horse, 3rd ed., p.88, 2008, Wiley-Blackwell) • This case demonstrates the potential advantage of utilizing additional imaging diagnostics like MRI to evaluate soft tissue structures in the foot for a cause of lameness even though obvious bony lesions were identified on radiographs Right Front, Type II P3 fracture Transverse, PD Transverse, STIR Right Front, Type II P3 fracture Dorsal, 3D Right Front, Type II P3 fracture 60-degree dorsoproximalpalmarodistal oblique Lateral 45 degree proximalmedial distal oblique