Suspensory Ligament Injury in Horses: Diagnosis & Treatment
advertisement

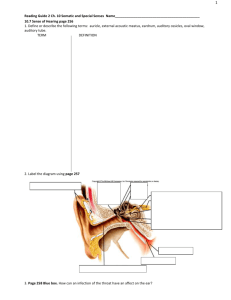
Injury to the Suspensory Ligament: A Suspenseful Affair Injury, Diagnosis, and Treatment By Dr. Kara Spillman Forelimb Hindlimb Drawings by Dr. Kara Spillman Your horse has become lame. You have the vet out and they have diagnosed a “suspensory”. What does this mean, and what can be done about it? The suspensory ligament refers to a structure located on the back of all four limbs that functions to support the lower limb as part of the “stay apparatus”. Although it is mostly comprised of collagen (ligamentous) tissue, it is interspersed with muscle fibers in the upper portion, particularly in the hindlimb. This mixture of muscle and ligamentous tissue can be especially tricky in ultrasounding the proximal suspensory area of the hindlimb. The suspensory ligament is shorter in length in the forelimb than the hindlimb, originating from the lower part of the back of the knee (carpus) and from the back of the cannon (metacarpal) bone. In the hindlimb it originates from the back of the lower hock bones and also the back of the upper part of the cannon bone, as shown in red in the above drawings. The uppermost portion of the ligament is referred to as the “origin of the suspensory” and will often cause lameness if injured. Generally the onset of lameness is gradual compared to other injuries lower down on the ligament, but can become quite significant over time. Moving further down the leg, the suspensory portion is referred to as the “body of the suspensory”, and it is generally much less common to incur an injury within this area of the suspensory compared to the origin or branches. About two thirds of the way down the cannon bone area, the suspensory body splits into two branches that ultimately attach onto their respective sesamoid bones at the fetlock. These branches can readily be seen in a normal horse’s limb. Injury to the branches can be quite painful, particularly if the attachment to the sesamoid bones is compromised. Generally radiographs are included in the work-up of a suspensory branch lesion to rule out boney changes in the fetlock region. A small extension of the suspensory can usually be seen externally on the horse crossing obliquely over the lower leg bones to join an extensor tendon in the front (the extensor tendon is shown in blue in the pictures). These extensions may become more apparent when they are stressed from workload, poor conformation, or injury that has compromised the stay apparatus of the limb. Generally injury to the extensor portions of the suspensory ligament do not cause significant lameness and are less concerning than an injury to the body or branches of the suspensory ligament. The first step after assessing the gait of a horse during a lameness exam is palpation and visual assessment of the structures of the leg. There may be heat, swelling, and pain noted that may point to a particular area of the suspensory that seems to be affected. It is very important to note that palpation of the suspensory ligament can be very subjective and diagnosis of a suspensory lesion should almost always be verified with appropriate diagnostics, such as regional nerve blocks and ultrasound examination. Once a suspensory lesion has been identified, treatment is focused on decreasing inflammation and promoting good fiber repair within the ligament. The majority of positive effect on ligament and tendon healing is rest, anti-inflammatory medication, supportive bandaging, and cold therapy. It is crucial to develop a proper rehabilitation program to bringing the horse back into work slowly, with constant monitoring of the ligament via visual and tactile aids. Repeated ultrasound examinations are strongly advised to make sure that any increase in workload is not causing further damage to the ligament. In addition to the good old-fashioned therapies, there are an increasing number of modalities to support proper healing within the ligament structure. Ligaments and tendons are generally fairly avascular, meaning that they do not have a good blood supply. Blood is necessary for oxygenation and repair of tissues. Shockwave treatment can be used to promote angiogenesis, the growth of blood vessels, to the area. Another key aspect to recovery is the promotion of anti-inflammatory effects. Modalities such as PRP, IRAP, and stem cell therapies have shown promise for treatment of many injuries, including the suspensory apparatus. These modalities use the body’s own cellular components to create an anti-inflammatory effect and promote proper healing and fiber alignment. Fiber alignment is important because the closer the fibers align in their original orientation and strength, the closer the ligament returns to its original function. An up-and-coming modality that is making its way to the equine world is elastic taping. This modality has become popular with human athletes and physicians worldwide, and was seen being used extensively during the summer Olympic Games. Working with Dr. Beverly Gordon and The Horse In Motion, Athletic Equine is now able to offer this supportive technique with Equi-tape™, elastic tape designed specifically for horses. Below demonstrates a taping performed by Dr. Gordon that supports an injured suspensory ligament. Athletic Equine is proud to offer this non-invasive, drug-free technique in conjunction with shockwave, PRP, IRAP, and in Florida locations, stem cell therapy (coming soon to Long Island!) to help improve healing for an injured athlete. For more questions concerning the suspensory ligament, injuries, and treatments, please contact Dr. Kara Spillman on her website www.drkara.biz, or call her at 561-316-8381.