Pelvic exam across the life
span
Anne Moore, DNP, APN, FAANP
Objectives
• 1.
1.Evaluate current guidelines for pelvic
examination and screening for women across the
lifespan (pediatrics to geriatrics)
2.Rationalize the use of components of the pelvic
examination based on age-related and cultural
variables.
3.Evaluate techniques of the pelvic exam to
accommodate age-related and cultural variables.
Basic principles
• Tools for history include: calendar, pelvic diagrams,
gestation calculator
• Greet her while she is dressed & obtain her history
History: Essential Issues
• Do not make assumptions about sexuality
• Too old to be sexual
• Heterosexual
• Satisfied with sex life
• Not at risk for pregnancy/STI’s
History: Essential Issues
• Ask about continence (urine & stool)-dribbling, urgency,
wetness
• Wears pads? Activities she avoids?
Preparing for the Pelvic Exam
• What are her previous experiences?
• Tell her you will stop the exam if she asks
• Discuss cues for pain
Discussion
“A pelvic exam should not be painful, pressure is
normal, but pain is not. Let me know what you’re
feeling and we can stop at any time if it’s too
uncomfortable. “
Pelvic Exam with Older Women
• May take longer
• Positioning more challenging
• Smaller specula necessary
• Topical analgesic use
• Pain control, pain
vs. pressure
Preparing the Older Woman
• Provide estrogen creams, suppositories, rings directly to
the vagina to facilitate ease of speculum insertion.
•
• Consider oral (NSAID) & topical analgesics. Lidocaine to KY?
Tools of Your Trade
• Good light
• Older women can’t adjust to temperature change as
well. Consider fan in room
• Warm specula in a variety of sizes-pediatric size
• Long handled mirror
• Non-latex gloves-in your size
Tools for the Pelvic
• Cotton swabs
• Pap smears
• Scopettes or ring forcep + cotton balls
• pH paper
• Gc + CT tests or urine tests
• Warmed lubricant
• Various sized specula
YES You Can Use Lubricant Before Paps
and Infection Testing
• Griffith-Uni Texas Southwestern 2005
• Randomized study 9,500 women ages 20-44
yrs.3,460 Paps & 5,535 DNA assays
• Dime sized water soluble bacteriostatic gel
lubricant
• Does not effect Pap testing nor Gc or CT tests
Tools for the Pelvic
• Biopsy materials: lidocaine 1% w/o epinephrine
• Small syringe with TB needle or 25g
• Cleansing liquid-iodine
• Biopsy container with formalin-lid off & labeled
• Cervical biopsy forceps or other tool
Beginning the Pelvic Exam
• Positioning on table
• Drape up or down? Watch reactions, assess
discomfort
• Tell her what you are going to do, explain sounds
• Use positive terms, tell her what you see
Positions for Exam
• Decreased abduction of hips-side lying, assistant
supports anterior leg & knee-chest on floor with
specula upside down
• Obese-knee chest, or place abdominal hand
under panniculus
• Ultrasound
Inguinal Lymph Nodes
• Assess inguinal nodes-enlarged nodes-herpes,
perineal infections, inflamed hemorrhoids
• Infections of feet & legs, DM, stasis ulcers=
inguinal nodes
• nodes may indicate systemic disease, infection,
lymphoma
The Vulva
• Evaluate the hair distribution- sparse, gray,
hypoestrogenic
• Inspect skin of the vulva carefully-VIN
• Look for signs of scratching from pruritus
• Cancer is a great imitator
The Clitoris
• Inspect & retract prepuce
• Dry skin, smaller clitoris =E
• Clitoris 1 cm wide abnormal
• Pale pink, mobile, agglutination suggests lichen
planus
• 10% vulvar cancers occur on clitoris
Urethra and Skene's
Ducts
• Erythema- urethritis, prolapse
• Milk anterior vaginal area for discharge (D/C)
• Milk lat. vaginal introitus for D/C from Skene's
ducts
• Palpate Bartholin gland for swelling or
tenderness
Urethral Prolapse
Sx: dyspareunia at introitus, dysuria; post-menopausal
bleeding
Palpating the Vagina of an Older
Woman
• Often small, narrow, atrophic
• Assess vaginal tone: anterior –cystocele &
posterior- rectocele
• Have her grip your fingers- assess pelvic
musculature
Palpating the Vagina and Cervix
• Palpate vaginal walls for cysts (Gartner duct cystsnormal variation, common along lateral vaginal
walls)
• Abnormal texture (HPV, cancer) & vaginal septum
Find the Cervix (Cx) Before Speculum
Exam!
• Assess consistency- hard suggests cancer, nodular cx
suggests Nabothian cysts or cancer
• Note position-up, down, lateral? How far from introitus?
Don’t bump into it!
The Cervix
Insertion of Speculum in Elderly
Woman
• Viscous lidocaine, before exam
• 2-3 weeks of E cream before exam
• Use smallest speculum
• Spread labia to see introitus, insert gently &
obliquely
Cervix & Vagina of the Older Woman
• Cervix is small, os closed, no cx neck- may be flat
against wall
• Decreased vaginal rugae, pale,
thin, bleeds easily from E
• Vaginal pH is high >5.0 from lactobacilli from E
• Polyps common
Pap Smear in Older Women
• WHY?
• Stenotic Os is common-to find os use OsFinder,
cytobrush, lacrimal probes (ENT)
• Hypoestrogenic smears may look abnormal-prep
with E for 3 wks before Pap
• SCJ is high within the canal-use cytobrush is
necessary
Order of Specimen Collections
• 1. pH-from side walls
• 2. Vaginal specimens- wet prep-take from side walls
• 3. Pap Smear
• 4. Gc, Ct tests or urine tests
• Avoid contaminating with blood if possible
Hysterectomy
• Surgical & path report? Bilateral oophorectomy?
• Taking exogenous hormones(estrogen &
testosterone)?
• If hysterectomy for cancer-continue PAP smears
from cervical/vaginal cuff & close inspection of
vulva-vagina
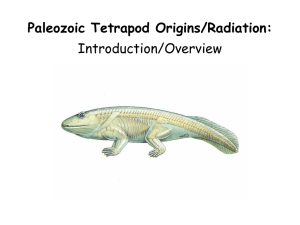
USIN G YOUR MANO & FINGER
M E A S U R EM EN TS T O S 'Z E
U T E R IN E L E N G T H & W ID T H
& S iZ E O VA R lE S
l
C m d istance o f
b o t h f in aers
VAGrNAL FIN GERS
D E T ERMIN fNG S
IZ E
O F O VA R IES
D ETER MIN IN G WIDTH
O F UT E R U S
DETERMINING LENG,TH
OF UTERUS
AB DOMINAL HAND
C·m distance middle
digit to notch
...._....cm distance from index
dig it to notch
' - . . - Cm distance fro m 1 t j o int
to notch
not
DETERMINI;NG L ENGTH
OF C;E RVIX
Cm d·s t,anc,e to
151 j1o int
Cm distance to
1 st joi nt
Palpation of Uterus
•
Assess cervix & uterus for nodularity
(myomas, tumors)
• Fibroids feel rock-hard & irregular
• Fibroids-associated with enlarged, irregular,
tender uteri and abnormal bleeding
Palpation of Uterus
• Assess position
• Assess flexion & mobility
• Assess for cervical motion tenderness (CMT)
• Assess length & width
••
I
cervical motion
tenderness
Palpating Uterine Position
• Anterior
• Anteflexed >45 anterior curvature
• Mid Position
• Posterior
• Retroflexed >45 posterior curvature
Palpating Uterus-Position
• If Rt fingers in vagina: Rt foot on step
• Locate cervix (Cx); if cannot feel it, use abd. hand to pull
uterus down until you can feel Cx internally
• Slide internal fingers along posterior & anterior neck of
Cx
• Can you feel the neck going upward? Anterior position?
Palpating Uterus-Position
• If you feel the cervical neck going downward could
be posterior or retroflexed position?
• If anterior position-lift uterus up with internal
fingers & palpate with your abd hand
• Width? Regularity? Mobility?
Palpating Uterine Contour
• If the uterus is posterior, it could also be
retroflexed
• You must do a recto-vaginal exam to determine
the position & feel the fundus more accurately
Performing a Rectal-Vaginal Exam
• With index finger in the vagina & middle finger
in the rectum, find the cervix-your land-mark by
touching her cervix with both fingers
Palpating Uterine
Contour …
• With posterior or retroflexed uteri, the ovaries fall
back or are posterior & are easier to palpate rectally
Determining Uterine Size
• Width: when palpating cervix, feel the widening
neck & estimate width with your measured
fingers; this estimates the width of the lower
uterine segment
• Lift up uterus, estimate length with abd hand
measurements
Pelvic Examination Techniques in
challenging Clinical Situations
Physical Exam of the Obese Woman
• Will table support? Is table wide enough?
Have assistant stand to side of table to
stabilize & reassure her
• The vulva may be hidden by the panniculus &
a longer speculum is often necessary
Providing Pelvic Examinations with
Obese Women
• The vulva may be larger-insure the labia are
examined carefully, completely
• Obese women may have difficulty reaching
their vulva; discuss use of flexible shower
heads to reach her perineum & rectal area or
squatting positions in bath for cleansing
Special Issues Providing Pelvic
Examinations with Obese Women
• The extra adipose tissue of the vulva makes visualization
of the cervix difficult and may require a longer specula to
reach the cervix
Examinations with Obese Women
Speculum Exam
• Use an instrument: ring forceps (closed) or
tongue blade to gently push walls to the side
to improve visibility
• Use larger speculum as comfort dictates
Special Issues Providing Pelvic
Examinations with Obese Women
• The cervix may be difficult to visualize or
palpate…have her pull her knees up …curled
up in this position may give better speculum
visualization of the cervix
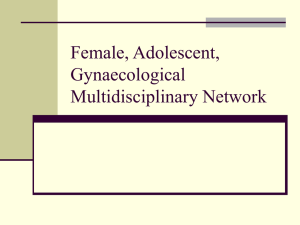
Difficult Palpation of the Uterus
• Obese women
• Virginal women
• A digital rectal exam with the woman in
lithotomy position (or any position that works)
• With anterior pelvic compression this technique
can be very helpful
,
'
0 8/ UTHSCSA © 1998
Visualizing or Palpating the Cervix
in Very Obese Women
• Place woman on covered floor in knee-chest
position; kneeling behind her, insert two fingers
into the vagina, the cervix will be easier to locate
• For Pap: place a Pap brush between 2 fingers,
insert into vagina, feel for cervix and obtain pap
Special Issues Providing Pelvic
Examinations with Obese Women
• The bimanual exam is more challenging & may be very
difficult to palpate uterus or ovaries
• Place the abdominal hand UNDER the panniculus to
decrease amount of adipose tissue between the
examiner’s hand & the uterus
• A pelvic US may be indicated
Pelvic Tenderness
•
Tender uterus: ectopic cervical
motion tenderness (CMT), myoma,
cancer, endometritis- salpingitis,
adhesions
• Ballot to assess mobility
• Fixed uterus suggests adhesions
Consider Non-Gynecologic Causes of
"pelvic pain”
• Spine-palpate sacrum & coccyx via rectum
• Radiculopathy-back exam: ROM, vertebral
compression (osteoporosis), disc diseasestraight leg lift, osteoarthritis
Pelvic Pain
• Bladder-interstitial cystitis
• Cystitis-less symptoms in older women
• Palpate bladder with vaginal fingers under bladder
& abd fingers pressing down on bladder
• Bowel-cancer, impaction
• ALWAYS do rectal exam
Adenomyosis
• Endometrial tissue within the myometrium of
the uterus
• Heavy, painful menses & large, boggy uterusHalban’s sign
• 20% of uteri removed for abnormal bleeding
show adenomyosis
Ovary Norms
• Normal ovaries can range from 2-4 cm depending
on time in cycle
• During ovulation the ovary may be as large as 4 cm;
bring pt back in 2 weeks to recheck if concerned or
pelvic US
Older Ovaries
• By 2 years post menopause most ovaries not
palpable
• If palpable consider ovarian cancer
• Consider ultrasound if unsure
Follicular Ovarian Cysts
• 95% Follicular cysts are < 5 cm
• Found during follicular-proliferative phase
• Most common; can rupture, hemorrhage (rare)
• Usually ~3 cm; can range to 8-10 cm
Corpus Luteum Cyst
• Occur during luteal or post-ovulatory phase
• Rarely exceed 4 cm, but can get up to 11 cm
• Can rupture & bleed & mimic ectopic
• All cysts can tort, very painful
The Recto-Vaginal Exam
• Apply lubricant or lidocaine
• Explain exam will cause pressure, but should NOT
be painful; feeling an urge to defecate is normal
• With index finger in vagina, place lubricated middle
finger at the anus
Recto-Vaginal Exam
• Ask her to bear down gently against your finger,
insert only to 1st joint, stop, ask her to relax
muscles & don’t move finger
• Once muscles relax; ask her to bear down &
gently insert finger; stop & don’t move until she
relaxes
Recto-Vaginal Exam
• Then palpate slowly & tell her when you rotate
finger-feel septum between rectum & vagina
with both fingers (1 in rectum, 1 in vagina)
• Palpate rectal ampulla note polyps or masses
• Assess uterus & ovaries with bimanual as
indicated
Rectal Exam
• Use single digit
• Palpate high for masses
• Ampulla tight, stenotic, stiff ?
• Look at finger for bleeding
• Stool for occult blood, colonoscopy
The First Pelvic Exam
• What has she heard?
• Previous experiences with providers?
• What does she expect?
• ACOG recommends first appointment with GYN
provider between ages 13 and 15
First Pelvic
• Does it need to be done?
• Risk? contraception? Does it all have to be done
the 1st visit?
• Cultural issues, translators, chaperones?
• Mom, boyfriends and 4 girlfriends want to be in
room for exam…oh my!
Reasons for pelvic exam in a younger
woman
• Pelvic pain
• Unusual bleeding/discharge
• Assault
• Request