Guidelines for gynecology examination
advertisement

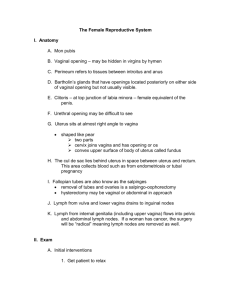
Guidelines for the Gynecological Examination General Considerations: Always have another person in the room with you as a chaperone (especially if you are the opposite gender). Introduce yourself to the patient. Address the patient using her last name unless she states otherwise. You may want to ask her what she would prefer to be called. Wash your hands or use sanitizer and explain to the patient that you will be doing a breast and pelvic examination today. Explain each part of the exam before you perform it. Throughout the breast and vaginal exam explain what you are going to do, ensuring that the woman is involved in her care. Always “talk before touch.” Encourage her to ask questions, and help her feel as comfortable as possible during this exam. Respect the modesty of the patient. Adequately drape her during the exam; cover what isn’t being examined. Do not leave the woman in the stirrups unattended. After the exam, make sure the patient is not dizzy when she gets out of the lithotomy position. After the exam, offer a tissue for the patient to remove the excessive lubricant. Breast Examination: Ask the patient if she does self-breast examinations. Let her know that you can go over the self-breast examination as you are inspecting and examining her breasts. With patient sitting upright ask her to lower the sheet so that you can inspect her breasts. Do not lower the sheet yourself but ask patient to do it. Inspect breasts for: Size Symmetry Contour Color, thickening, venous patterns Skin rashes or lesions Inspect nipple for: Size, shape, direction Lesions Hair distribution Discharge Inversion With hands against hips, then with arms above head, inspect breasts for: Dimpling (puckering of skin) Contour Retraction of nipple Skin rashes or lesions If breasts are pendulous ask patient to lift her breasts to allow inspection of skin under the breasts. With patient in a sitting position: Palpate supraclavicular nodes Palpate axillary nodes, next to the rib cage and deep into the armpit. Keep arm at about 45 degree angle and have patient relax arm so that the axillary nodes can be palpated. The examiner may use the drape sheet to protect hand from deodorant in the axilla Palpation Exam of the Breasts Ask patient to recline on examining table, providing leg with the table shelf. 1 Ask her to place one hand behind her head and to move the drape to allow thorough palpation of that breast. Palpate each breast in a systematic manner, compressing tissue with light, moderate, and deep pressure between the pads of two to three fingers and chest wall. Utilize a circular or kneading motion. The entire breast tissue can be covered by circular motion or vertical strip method, but for this course for consistency, we will be teaching vertical strip method. Take care to palpate into the axilla and lateral to the midaxillary line. For larger breasts the opposite hand can be used to stabilize the breast while palpating the tissue. Gloves need not be worn to examine intact skin. If the examiner or the patient has a rash or lesions, then gloves should be worn. Palpate for: Density, symmetry and character of tissue Differences within each breast and between the two breasts Irregular masses or densities Masses may be mobile or fixed Size of any masses Palpate behind the areola. Explain breast self-examination to the patient, if desired. THE VAGINAL EXAM Instruction and Preparation: Prepare your equipment. o Choose a speculum of appropriate size. A Small (white handle plastic) or Regular Pedersen (metal) speculum can be used for a woman who has had penile intercourse or is able to use tampons, but has not had a vaginal birth. If the woman has had a vaginal birth or is obese, a larger Graves speculum (metal) or large plastic (green handle) will be helpful. Do not think that smaller is always better. The correct size for the woman is the most comfortable. o Open the plastic cover but keep the speculum in the plastic cover and attach the light to bottom of the speculum. Do not touch the blades of the speculum with your hands. o Place Pap materials (not applicable for practicum as Pap will not be done on the patient instructors), lubricant, and swabs on the white paper on the counter/tray. o Place 4 pairs of gloves on the white paper on the counter/tray. The white paper is your clean area. The patient should have the process explained to her prior to the actual exam. During the exam, each step should be related to the patient prior to performing the portion of the exam. Wash hand or use sanitizer before putting on gloves. Always examine the patient with gloved hands. The pelvic examination is a “clean” procedure not a “sterile” procedure. The goal is to not contaminate the patient with a hand that has touched anything in the room and to not contaminate the room with a hand that has touched the patient. If possible designate one hand to be the “examining” hand and to only touch the patient and the other hand to be the “room/speculum” hand and only touch the speculum and swabs. However, if hands need to be switched for the bimanual examination OR if you ever are concerned that your hand that will be touching the patient may have touched something in the room, change your gloves. Text is written for right-handed examiners - reverse hands for left-handed examiners. Position for exam: Ask patient to lie back on the table with the heels in the foot stirrups. Ask her to move her hips down to the very bottom of the table and then a little more. If she feels like her hips (buttocks) are slightly off the end of the table, then she is in the correct position for the exam. Ask her to allow her knees to relax out to the sides. If you need to position the legs farther out, you may put your arms on the outside of her knees and ask her to move her knees out until they reach your hands. Never put your hands between her knees to move them on your own. Make your patient feel that she is in charge of positioning. Wash hands or use sanitizer before putting on gloves. Glove both hands. Inspection of the Vulva 2 Always tell the patient “You will feel my touch” before touching any part of the body, but especially the sensitive parts. Before touching the labia, touch the inner thigh, then not lifting your hand, continue to palpation of the labia. Inspect pubic hair for pattern Inspect mons pubis and pubic hair area for lesions With right hand (speculum hand) hand palpate inguinal lymph nodes for tenderness or enlargement since this area is intact skin. Use left (examining hand) to separate labia and inspect all skin folds including clitoris, urethera, labia minora, introitus (vaginal opening), perineal body, perianal skin. Inspect urethra, periurethral gland openings, hymen, Bartholin gland openings. Palpate Bartholin glands if enlarged. Ask patient to bear down to check for cystocele, rectocele, uterine prolapse. Use backs of hands to separate buttocks if needed to inspect perivaginal and perianal skin. Remember skin lesions in the perineum are common, miserable, potentially dangerous and often treatable. It takes only a few seconds to do a thorough inspection. Speculum insertion Prior to inserting the speculum, inform the patient that she will feel pressure but there should not be any pain. Ask her to tell you if there is anything more than discomfort. Insert Left (examining) Hand index finger or two fingers into vagina to: Assess for pain or tenderness that might inhibit exam. Assess the vaginal anatomy for direction of the speculum Locate the cervix in the posterior vagina Separate labia minor to clearly visualize vaginal introitus for speculum insertion As one gets more experienced in the pelvic examinations, it may not be necessary to locate the cervix prior to speculum insertion. Speculum insertion Metal speculums must be warmed to body temperature Use warm water if needed on speculum blades Separate labia minora with left (examining) hand fingers Hold handle of speculum with right (speculum) hand Insert speculum blades into vagina with blades parallel to table or at a slight oblique angle Remember how the vaginal anatomy was assessed and the cervix was located with the digital exam. Insert the speculum fully into the vagina, using good posterior pressure Open the speculum after it is fully inserted Deepen the posterior pressure with the opening of the speculum Inspect the vagina and cervix Character and amount of vaginal discharge. (some may be normal) Bleeding Pink squamous cervical tissue Dark pink or red columnar or transitional cervical tissue around the os Size and shape of cervix and cervical os Lesions on cervix or vagina Take STI tests, Pap test, wet smear as indicated Pap smear will not be done but method on how to do one will be assessed. Obtaining the PAP smear Visualize the cervix Collect a sample from the ectocervix with the broom type collection device. o Rotate the broom (360 °) while keeping it flush with the tissue of the cervix. 3 o Place into the vial of fixative if using the broom and ThinPrep Method. Removing the speculum Release the upper blade to allow speculum to close completely as it is withdrawn For plastic speculum, use left (examining) hand finger or thumb to hold toothed tab completely up For metal, make sure screw is completely released. Increase posterior pressure to allow cervix to escape blades. Allow vaginal muscles to close speculum. Never force it closed. Increase posterior pressure and make sure blades can close completely before withdrawal. Bimanual Exam If you are more comfortable palpating the cervix with your right hand, at this point, after the speculum is removed, change your gloves. The text below is written for those who have not changed gloves. So if you changed gloves, reverse hands. First perform abdominal exam using right (speculum) hand. Start at the umbilicus and palpate firmly down to the symphysis pubis. Check for masses or tenderness. The edge of the enlarging uterus or pelvic mass will be felt above the pubic symphyis after about 14 weeks pregnancy size. Keep right hand on low abdomen while inserting vaginal fingers. Use lubricant on left (examining) hand index and middle fingers. Insert two fingers (if possible) into vagina. Locate cervix. Move cervix to check for cervical motion tenderness Place index finger above and middle finger below cervix (anterior and posterior fornix) Use right (speculum) hand to press uterus down to fingers in the vagina. Press vaginal fingers toward uterus. Anteverted uterus (fundus) is best felt through anterior fornix. Retroverted uterus (fundus) is best felt through posterior fundus. Adnexa (ovaries and tubes) are palpated directly to the right and left of the cervix All pelvic structures are best palpated through the vaginal wall. The hand on the abdomen presses the structures down to the examining vaginal fingers. Palpate uterus for: Size Mobility Tenderness (including tenderness to motion of the cervix) Position (anteverted, retroverted, midline, etc) Shape Masses The uterus can be felt as a firm, almost rubbery mass against the background of the pelvis. Palpate ovaries (adnexa) for: Masses Tenderness Normal ovaries may rarely be palpated, but often are lost in the background of the pelvis. Any palpable mass in the adnexa needs further evaluation. Rectal or rectovaginal exam will not be done during our practicum but instructions on how to do one will be assessed. Perform recto-vaginal exam if indicated to assess: Recto-vaginal wall Recto-vaginal pouch 4 Retroverted uterus Rectal masses Anal Sphincter tone Perform rectal exam if indicated only to assess: Anal sphincter tone Rectal masses Pelvic structures when vaginal exam is not possible Rectal exam Explain to patient that exam is indicated. Get verbal consent to exam. Recognize that exam is uncomfortable, but should not be painful. Change gloves. Use a clean glove for each new orifice examined. Use adequate jelly lubrication. Visualize the anus before inserting finger. Rectal finger should be at a slight angle up, toward the umbilicus. For recto vaginal exam, insert anal finger first (third finger), then vaginal finger (index finger). Assess anal sphincter tone. Assess rectovaginal wall and rectovaginal pounch for masses or fistulas Identify cervix with vaginal finger and rectal finger. Use speculum hand to stabilize the abdomen to palpate the uterus and adnexa Remove the vaginal finger (rectovaginal exam) Rotate rectal finger to assess for masses Remove finger and offer tissues. A good thorough exam will take less than 30 seconds. 5