increase - Acute Heart Failure
advertisement

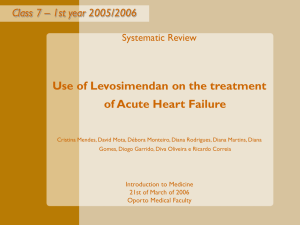
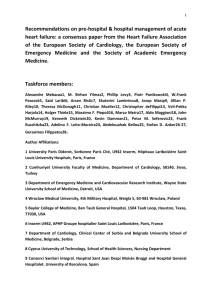
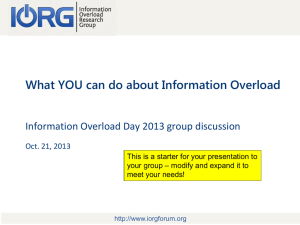
PATHOPHYSIOLOGY HF/AHF Disease Awareness The pathophysiology of heart failure results in an increasingly downward spiral • Acute decompensated HF is associated with frequent hospitalizations1 • With each hospitalization, there is likely myocardial and renal damage that contributes to progressive LV or renal dysfunction, leading to an inevitable downward spiral2 Cardiac function and quality of life Chronic HF Increased risk of decompensations Hospitalizations Time HF=heart failure; LV=left ventricular 1. Alla et al. Heart Fail Rev 2007;12:91–5; 2. Gheorghiade et al. Am J Cardiol 2005;96:11G–17G More rapid decline in chronic HF Acute decompensation Cardiac and renal damage/ incomplete recovery Clinical classification of acute heart failure reflects a spectrum of overlapping presentations • >50% incidence for ↑SBP1 • Mainly pulmonary rather than systemic congestion1 • Many patients have preserved ejection fraction1 • 70% incidence1 Hypertensive AHF Acutely decompensated chronic HF • <3% incidence1 • Clinical characteristics: severe dyspnea, tachypnea, tachycardia and hypoxemia, which may require immediate airway intervention1 Pulmonary edema ACS and HF Cardiogenic shock Right HF • Unknown incidence1 • Many patients have signs and symptoms of ACS that resolve after initial therapy or resolution of ischemia1 • Acute HF frequently precipitated by or associated with an arrhythmia2 • Usually a history of progressive worsening of chronic HF on treatment and evidence of systemic and pulmonary congestion2 • <1% incidence1 • Primarily complicating acute MI, fulminant myocarditis1 • Tissue hypoperfusion after adequate correction of preload and major arrhythmia2 ACS=acute coronary syndrome; AHF=acute HF; HF=heart failure; JVP=jugular venous pressure; LV=left ventricular; MI=myocardial infarction; SBP=systolic blood pressure 1. Gheorghiade et al. Circulation 2005;112:3958–68; 2. Dickstein et al. Eur Heart J 2008;29:2388–442 • Unknown incidence1 • Low output syndrome in the absence of pulmonary congestion, increased JVP and low LV filling pressures2 The Short-term and long-term Pathophysiogical consequences of AHF‡ Processes mediating short-term effects Initiation phase Vasoconstriction Decreased cardiac function Processes mediating long-term effects Amplification phase O2 supply-demand mismatch Fluid overload Hemodynamic abnormalities INCREASE Myocardial overload and renal dysfunction Myocardial damage as shown by ↑hs-cTnT Neurohormonal activation Oxidative stress INCREASE Inflammation INCREASE Myocardial fibrosis and remodelling as shown by ↑fibroblast proliferation and activation Renal damage as shown by ↑uric acid INCREASE Renal dysfunction as shown by ↑Cystatin C, ↑Creatinine, ↑BUN INCREASE INCREASE NTNT-p r proBNP Preload Afterload Congestion Organ damage and dysfunction ‡Proposed schematic of acute heart failure pathophysiology Biolo et al. Circ Heart Fail 2010;3:44–50; Bott-Flügel et al. Eur J Heart Fail 2008;10:129–32; Cotter et al. Am Heart J 2008;155:9–18; Cotter et al. Eur J Heart Fail 2008;10:165–69; Feng & Wang. J Geriatr Cardiol 2008;5:1–6; Hunt et al. J Am Coll Cardiol 2009;53:e1–e90; Oikonomou et al. Hellenic J Cardiol 2011;52:30–40; Tsutsui et al. Am J Physiol Heart Circ Physiol 2011;301:H2181–90 Patterns of ventricular remodelling are different for HFrEF and HFpEF HFrEF – a condition of volume overload • characterized by eccentric hypertrophy • results in globular heart with thinning of the LV walls, decreased systolic function and enlarged left ventricular volume Left ventricle volume overload HFrEF Left ventricle normal HFpEF Volume overload Pressure overload Increased diastolic pressure Increased systolic pressure Increased systolic wall stress Increased systolic wall stress Series addition of new sarcomeres Parallel addition of new myofibrils Chamber enlargement Wall thickening Eccentric hypertrophy Concentric hypertrophy HFpEF=heart failure with preserved ejection fraction; HFrEF=heart failure with reduced ejection fraction Adapted from Colucci (Ed.). Atlas of Heart Failure, 5th ed. Springer 2008; Grossman et al. In: Perspectives in Cardiovascular Research; Myocardial Hypertrophy and Failure. Vol 7. Edited by Alpert NR. New York: Raven Press;1993:1–15 HFpEF – a condition of pressure overload • characterized by concentric hypertrophic growth • results in normal sized LV cavity with thickened walls and preserved systolic function Left ventricle pressure overload Long-term Consequences of AHF: Higher NTproBNP levels are associated with increased risk of mortality in patients with AHF Higher levels of NT-proBNP are associated with increased risk of mortality by 90 days in patients hospitalized for AHF‡2 NT-proBNP levels increase During episodes of AHF1 Quartile of NT-proBNP Hazard Ratio 95% CI p value 1st 1.0 2nd 1.7 0.7–4.4 0.247 3rd 2.5 1.0–6.0 0.043 4th 4.3 1.9–9.9 <0.001 0.1 1 Hazard ratio AHF=acute heart failure; CI=confidence interval; NT-proBNP=N-terminal-pro-B-type natriuretic peptide ‡Analysis of data from 568 patients hospitalized for AHF in the Biomarkers in Acute Heart Failure (BACH) study †The NT-proBNP cutoffs were 2,248, 5,017, and 10,455 pg/mL for the 25th, 50th and 75th percentiles, respectively 1. Biolo et al. Circ Heart Fail 2010;3:44–50; 2. Maisel et al. J Am Coll Cardiol 2010;55:2062–76 10 Reference Long-term Consequences of AHF: Cardiac troponin, a marker of myocyte injury/death, is commonly elevated in AHF and is associated with increased mortality Troponin is often released in patients with AHF1 Higher levels of troponin T predict greater mortality in patients with AHF‡2 All-cause mortality at 6 months (%) P=0.002 P=0.007 31.5 27.8 Elevated troponin 14.1 is associated with poor outcomes in AHF1 <0.03 0.03–0.07 >0.07 Cardiac troponin T (g/L) AHF=acute heart failure ‡Analysis of data from 364 patients hospitalized for AHF from the Finnish Acute Heart Failure (FINN-AKVA) study 1. Kociol et al. J Am Coll Cardiol 2010;56:1071–8; 2. Ilva et al. Eur J Heart Fail 2008;10:772–9 Long-term Consequences of AHF: Worsening renal function in patients hospitalized for AHF predicts poor outcomes Further worsening of renal function occurs in ~25% of patients hospitalized for AHF#3,4 1. 2. 3. 4. 5. Maggioni et al. Eur J Heart Fail 2010;12:1076–84; Rudiger et al. Eur J Heart Fail 2005;7:662–70; Forman et al. J Am Coll Cardiol 2004;43:61–7; Akhter et al. Am J Cardiol 2004;94:957–60; Lassus et al. Eur Heart J 2010;31:2791–98 0.5 >0.5 mg/L increase in cystatin C 0.4 Cumulative mortality ~30–40% of patients hospitalized for AHF have renal impairment†1,2 An increase in cystatin C in the first 48 hours following hospitalization for AHF is associated with poor prognosis‡5 0.3 ≤0.5 mg/L increase in cystatin C 0.2 0.1 0 0 100 200 300 400 Days AHF=acute heart failure †Renal impairment defined as an estimated glomerular filtration rate <50 mL/min/1.73 m2 or creatinine clearance <50 mL/min; #Worsening of renal function defined as an increase in serum creatinine of >0.3 mg/dL or >0.5 mg/dL; ‡Analysis of data from 292 patients hospitalized for AHF from the Finnish Acute Heart Failure (FINN-AKVA) study Item Code: 153049 Copyright © Novartis Pharma AG.