Pulmonary Hypertension
RYAN O’GOWAN, MBA, PA-C
FAPACVS
FCCM
Disclosures
I have no financial relationships with any drug
or device manufacturers to disclose.
Objectives
At the conclusion of this lecture the participant
should be able to:
Define Pulmonary Arterial Hypertension (PAH) and discuss
its clinical relevance, including various modes of evaluation
and diagnosis.
Discuss and define the various subgroups of PAH according
to the World Health Organization (WHO) classification.
Discuss available treatment strategies and their
mechanisms for selected WHO subgroups.
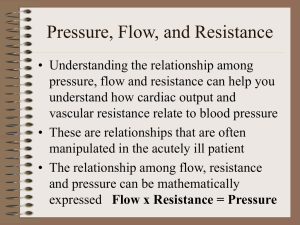
Definition
Pulmonary Arterial Hypertension:
“is a syndrome resulting from restricted flow through the
pulmonary arterial circulation resulting in increased
pulmonary vascular resistance and ultimately in right heart
failure. ”
ACCF/AHA 2009 Expert Consensus Document on Pulmonary Hypertension
Clinical Diagnosis
Clinical Definition of pulmonary
hypertension:
Mean PA pressure>25 mm Hg
PCWP <15mm Hg
Cardiac output may be normal or reduced
Galie N, et al. Eur Heart J. 2009;30(20):2493-2537.
Normal Pulmonary Physiology
Pathophysiology
Pathophysiology
Causes of Pulmonary Hypertension
ACCF/AHA 2009 Expert Consensus Document on Pulmonary Hypertension
Diseases Associated with Pulmonary Hypertension
ACCF/AHA 2009 Expert Consensus Document on Pulmonary Hypertension
Presentation
Shortness of breath with exertion
Dry cough
Lower extremity edema
Weakness & malaise
No Physical Exam findings other than those
associated with Right Heart failure can reliably
diagnose pulmonary hypertension
American Thoracic Society source document on Pulmonary Hypertension
Epidemiology of Pulmonary Hypertension
Average age at presentation- 36 years
Prevalence women>men by 2:1
Three year survival after diagnosis ~50%
Incidence: 10-15 people per million of population
Number of U.S. patients: 10,000-20,000.
Patients who survive go on to be candidates for total
lung transplant.
American Thoracic Society source document on Pulmonary Hypertension
Evaluation and Diagnosis
•S W A N - G A N Z C A T H E T E R I Z A T I O N
•S E L E C T I V E R I G H T H E A R T
CATHETERIZATION
•E C H O C A R D I O G R A P H Y
•C T S C A N N I N G F O R P U L M O N A R Y E M B O L I
Swan Ganz Catheterization
Clinical Procedures in Anesthesia and Intensive Care, p 416. JB Lippincott, 1994
Selective Right Heart Catheterization
Uses the Swan to gather:
right atrial pressure (RAP)
right ventricular pressure (RVP)
pulmonary arterial pressure (PAP)
pulmonary capillary wedge pressure
(PCWP)
systemic arterial pressure (BP) and
heart rate
cardiac output (CO)
pulmonary arterial vasoreactivity
pulmonary arterial (PA) ("mixed
venous") saturation
superior vena cava (SVC) saturation
inferior vena cava (IVC) saturation
right atrial (RA) saturation
right ventricular (RV) saturation
Echocardiography
Rev Esp Cardiol. 2010;63:583-96 - Vol. 63 Num.05
CT Chest- PE Protocol
WHO Classification
•C L A S S I
IDIOPATHIC
PAH (IPAH)
•C L A S S I I
PAH WITH LEFT HEART DISEASE
•C L A S S I I I
PAH SECONDARY TO HYPOXIA
•C L A S S I V
CHRONIC THROMBOEMBOLIC
PULMONARY HYPERTENSION
(CTEPH)
•C L A S S V
MISCELLANEOUS
Class I Pulmonary Hypertension
Idiopathic (IPAH)
Heritable (HPAH)
Bone morphogenetic protein receptor type 2 (BMPR2)
Activin receptor-like kinase 1 gene (ALK1), endoglin
Drug- and toxin-induced
Cocaine,Amphetamines
Fenfluramine (Taken off the market)
Associated with (APAH):
Connective tissue diseases (SLE)
Human immunodeficiency virus (HIV) infection
Portal hypertension
Congenital heart disease (CHD)
Schistosomiasis
Chronic hemolytic anemia
Persistent pulmonary hypertension of the newborn (PPHN)
J Am Coll Cardiol. 2009;54:S43–54.
Class II Pulmonary Hypertension
PAH with Left Heart Disease:
Mitral Valve Disease (Stenosis/Regurgitation)
Aortic Valve Disease (Stenosis/Regurgitation)
Systolic Dysfunction
Diastolic Dysfunction
J Am Coll Cardiol. 2009;54:S43–54.
Class III Pulmonary Hypertension
PAH secondary to hypoxia:
COPD
Interstitial Lung Disease (ILD)
Pulmonary Diseases with Mixed Restrictive and Obstructive
Patterns
Obstructive Sleep Apnea (OSA)
Alveolar Hypoventilation Disorders
Chronic Exposure to High Altitudes
J Am Coll Cardiol. 2009;54:S43–54.
Class IV Pulmonary Hypertension
Chronic thromboembolic pulmonary hypertension
(CTEPH)
Patients may have presentations consistent with
hypercoagulable states.
Common heritable sources of thrombosis include:
Factor V Leiden
Prothrombin G 20101A Mutation
Proteins C & S Deficiency
Lupus Procoagulant
J Am Coll Cardiol. 2009;54:S43–54.
Class V Pulmonary Hypertension
Miscellaneous
Hematological disorders: myeloproliferative disorders,
splenectomy
Systemic disorders: sarcoidosis, pulmonary Langerhans
cell histiocytosis, lymphangioleiomyomatosis,
neurofibromatosis, vasculitis
Metabolic disorders: glycogen storage disease, Gaucher
disease, thyroid disorders
Others: tumor obstruction, fibrosing mediastinitis,
chronic renal failure on dialysis
J Am Coll Cardiol. 2009;54:S43–54.
Treatment Strategies
GROUPS 1-5
PHARMACOLOGIC THERAPIES
PULMONARY ENDARTERECTOMY FOR GROUP
4
Updated Evidence-Based Treatment Algorithm in Pulmonary Arterial Hypertension
J Am Coll Cardiol. 2009;54(1s1):S78-S84.
.
Copyright © The American College of Cardiology.
All rights reserved. Used with permission.
Initial Pharmacologic Treatment
Mainstay of treatment: Group 1-4
Calcium Channel Blockers with Vasoreactivity Treatment
(Class B- for responders)
Amlodipine
Diltiazem
Nifedipine
Pharmacologic Treatment
Group 2 Pulmonary Hypertension
Ambrisentan
Bosentan
Sildenafil
Pharmacologic Treatment
Group 3 Pulmonary Hypertension
Ambrisentan
Bosentan
Epoprostenol IV
Iloprost Inhaled
Sildenafil
Group 4 Pulmonary Hypertension
Epoprostenol IV (Class A)
Iloprost Inhaled (Class B)
Pulmonary Thromboendarterectomy (Performed in selected
referral centers-UC-San Diego*)
TPA for active clot from “fresh” PE
Endovascular Treatment CTE
Pulmonary Endarterectomy
Endovascular Treatment CTE
Thank you for your time.