Committee on Operating Rules
For Information Exchange
(CORE®)
Understanding the Value of the
ACA Mandated CAQH CORE Operating Rules
Central Ohio HFMA Spring Conference
March 14, 2013
Additional information/resources available at www.caqh.org
Agenda
•
Introduction to CAQH CORE
•
Operating Rules and Affordable Care Act (ACA) Section 1104
•
Overview of ACA Mandated CAQH CORE Operating Rules
– First Set: Eligibility & Claim Status Operating Rules
– Second Set: EFT & ERA Operating Rules
– Third Set: Attachments, Prior Authorization, Enrollment, etc.
•
Reaping the Benefits of Operating Rules
– Engaging Practice Management System (PMS) Vendors
– Measures of Success
– Action Items for Providers
•
2
Q&A
© 2013 CORE. All rights reserved.
Objectives
3
•
Understand what operating rules are and their role in the broader
healthcare context
•
Understand status of the ACA mandates and what they mean for
providers
•
Consider the role of PMS vendors and impact on provide receipt of
compliance transactions
•
Learn about tracking and potential ROI associated with Operating Rules
•
Review a list of immediate action steps for providers to ensure ROI from
operating rules
© 2013 CORE. All rights reserved.
Introduction to CAQH CORE
4
© 2013 CORE. All rights reserved.
CAQH: Current Initiatives
Industry-wide stakeholder collaboration to facilitate development
and adoption of industry-wide operating rules for administrative
transactions. Over 130 participating organizations.
Service that replaces multiple paper processes for collecting
provider data with a single, electronic, uniform data-collection
system (e.g., credentialing).
• 85% of Ohio physicians (MD/DO) are registered in UPD
Service that enables providers to enroll in electronic payments with
multiple payers and manage their electronic payment information
in one location, automatically sharing updates with their selected
payer partners.
Objective industry forum for tracking progress and savings
associated with adopting electronic solutions for administrative
transactions across the industry.
5
© 2013 CORE. All rights reserved.
CAQH CORE Background
•
•
A multi-stakeholder collaboration established in 2005
Mission: To build consensus among
healthcare industry stakeholders on a set of
operating rules that facilitate administrative
interoperability between providers and
health plans
– Enable providers to submit transactions from
the system of their choice (vendor agnostic)
and quickly receive a standardized response
– Facilitate administrative and clinical data
integration
•
Recognized healthcare operating rule
author by NCVHS and HHS
Research and
Develop
Rules (based
on key criteria)
Maintain and
Update
Track
Progress,
ROI and
Report
Build
Awareness
and Educate
Promote
Adoption
6
© 2013 CORE. All rights reserved.
Design
Testing and
Offer
Certification
Provide
Technical
Assistance,
e.g., free tools,
access to Early
Adopters Base
Examples of CORE Participants
The more than 130 CORE Participants represent all key stakeholders
including providers, health plans, vendors, clearinghouses, government
agencies, Medicaids, standard development organizations, banks, etc.
Providers
Health Plans
(Strong presence in Ohio markets)
7
© 2013 CORE. All rights reserved.
Vendors
Overview of ACA Mandated CAQH CORE Operating Rules
8
© 2013 CORE. All rights reserved.
Industry Context: Federally Mandated Operating Rules
•
Today, operating rules support existing standards in many high-volume
industries, e.g. cellular phones, financial services ...Consider the ATM
•
Prior to 2005, national operating rules for medical administrative transactions
did not exist in healthcare outside of individual trading partner relationships
•
In 2005 CAQH CORE began facilitating voluntary development of industrywide healthcare operating rules
•
In 2010, Section 1104 of the Patient Protection and Affordable Care Act
(ACA) required that all HIPAA covered entities be compliant with applicable
HIPAA standards and associated operating rules
The effective date for the first set of ACA mandated operating rules was January
2013; additional deadlines follow through 2016.
9
© 2013 CORE. All rights reserved.
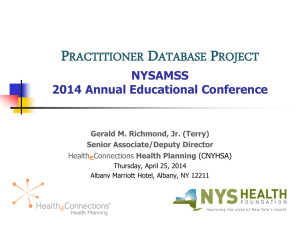
Industry Context: A Spectrum of Change For Providers
•
Goal: Generate a responsive, and adaptive, system-wide approach to administrative IT
adoption that aligns with other U.S. healthcare strategic initiatives
•
Each major transaction in the revenue cycle was addressed by HIPAA in 1996; standards
alone did not go far enough to reach Administrative Simplification – therefore, ACA
amended HIPAA
•
Due to ACA and other pressures, during the next several years the entire revenue cycle
process will experience significant transformation as the industry adopts operating rules
–
The exchange of data critical to a provider’s revenue cycle, e.g. patient financials
–
The infrastructure requirements that drive interoperability and ROI
Health Plan
820 Premium Payment
Provider
270 Eligibility Inquiry
Membership
271 Eligibility Response
Charge Capture
Clinical O/E,
Utilization Review
278 Referral Response
Billing
837 Claim/Encounter
277 Request for Info
278 Referral Request
275 Claim Attachment
A/R
and Treasury
277 Status Response
835 Remittance (EOB)
Bank
© 2013 CORE. All rights reserved.
Claim
Adjudication
276 Status Inquiry
CCD+ (EFT)
10
Pre-Adjudication
A/P
Enrollment
834 Enrollment
Sponsor
Purpose of Operating Rules
•
•
The Patient Protection and Affordable Care Act (ACA) defines operating
rules as “the necessary business rules and guidelines for the electronic
exchange of information that are not defined by a standard or its
implementation specifications”
They address gaps in standards, help refine the infrastructure that supports
electronic data exchange and recognize interdependencies among
transactions; they do not duplicate standards
Rights and
responsibilities of all
parties
Security
Exception processing
11
© 2013 CORE. All rights reserved.
Operating Rules:
Key
Components
Transmission
standards and formats
Response timing
standards
Liabilities
Error resolution
ACA Mandated Operating Rules Compliance Dates:
Required for all HIPAA Covered Entities
Operating rules encourage an interoperable network and, thereby, are vendor agnostic
Compliance in Effect
as of January 1, 2013
HIPAA covered entities conduct these transactions
using the CAQH CORE Operating Rules
Implement by
January 1, 2014
• Electronic funds transfer (EFT) transactions
• Health care payment and remittance advice (ERA)
transactions
Implement by
January 1, 2016
•
•
•
•
•
Rule requirements available.
12
• Eligibility for health plan
• Claims status transactions
© 2013 CORE. All rights reserved.
Health claims or equivalent encounter information
Enrollment and disenrollment in a health plan
Health plan premium payments
Referral certification and authorization
Health claims attachments
ACA Mandated Healthcare Operating Rules:
First Set - Eligibility & Claim Status
13
© 2013 CORE. All rights reserved.
Mandated Eligibility & Claim Status Operating Rules:
Scope –Effective as of January 1, 2013
Enforcement Action Begins
March 31, 2013
Mandated Eligibility & Claim
Status Operating Rules
Compliance date January 1, 2013
Type of Rule
Addresses
Data Content:
Eligibility
Need to drive further
industry value in
transaction
processing
Infrastructure:
Eligibility and
Claim Status
Voluntary Eligibility &
Claim Status
Operating Rule
CAQH CORE Eligibility & Claim Status Operating Rules
More Robust
Eligibility
Verification Plus
Financials
Enhanced Error
Reporting and
Patient
Identification
Industry needs for
common/
accessible
documentation
Companion
Guides
System
Availability
Industry-wide goals
for architecture/
performance/
connectivity
Response
Times
Connectivity
and Security
“We are addressing the
important role
acknowledgements play in EDI
by strongly encouraging the
industry to implement the
acknowledgement requirements
in the CAQH CORE rules we are
adopting herein.”
HHS Interim Final Rule
Acknowledgements*
*Please Note: In the Final Rule for Administrative Simplification: Adoption of Operating Rules for Eligibility for a Health Plan
and Health Care Claim Status Transaction, CORE 150 and CORE 151 are not included for adoption. HHS is not requiring
compliance with any operating rules related to acknowledgement, the Interim Final Rule.
14
© 2013 CORE. All rights reserved.
ACA Federal Compliance Requirement Highlights:
Eligibility and Claim Status
Three dates are critical for implementation of the first set of ACA mandated Operating Rules
There are two types of penalties related to compliance1
Key Area
HIPAA Mandated
Implementation
Dates
First Date
January 1, 2013
Compliance Date
Enforcement Date Extension
March 31, 20134
Applicable
Penalties
Second Date
December 31, 2013
Health Plan Certification Date
Third Date
No Later than April 1, 2014
Health Plan Penalty Date
Who: Health plans
Who: Health plans
Action: Implement CAQH CORE
Eligibility & Claim Status Operating
Rules
Action: File statement with HHS
certifying that data and information
systems are in compliance with the
standards and operating rules2
Action: HHS will assess penalties against
health plans that have failed to meet the
ACA compliance requirements for
certification and documentation2
Amount: Due to HITECH, penalties
for HIPAA non-compliance have
increased, now up to $1.5 million
per entity per year
Amount: Fee amount equals $1 per covered life3 until certification is complete;
penalties for failure to comply cannot exceed on an annual basis an amount equal
to $20 per covered life or $40 per covered life for deliberate misrepresentation
Who: All HIPAA covered entities
Description
ACA-required Health Plan Certification
1 CMS
OESS is the authority on the HIPAA and ACA Administrative Simplification provisions and requirements for compliance and enforcement. The CMS
website provides information on the ACA compliance, certification, and penalties and enforcement process.
2 According to CMS, regulation detailing the health plan certification process is under development, and they will release details surrounding this process later
this year; CAQH CORE will continue to offer its voluntary CORE Certification program and will share lessons learned with CMS as the Federal process is
developed.
3 Covered life for which the plan’s data systems are not in compliance; shall be imposed for each day the plan is not in compliance
4 Per the Jan 2, 2013 CMS OESS announcement of the 90-day Period of enforcement extension Discretion for Compliance with Eligibility and Claim Status
Operating Rules
15
© 2013 CORE. All rights reserved.
Compliance with Eligibility & Claim Status Operating Rules:
90-Day Period of Enforcement Discretion
•
•
•
On January 2, 2013, CMS OESS* announced a 90-Day Period of
Enforcement Discretion to reduce the potential of significant disruption to
the healthcare industry
Enforcement action will begin March 31, 2013 with respect to HIPAA
covered entities (including health plans, health care providers, and
clearinghouses, as applicable) that are not in compliance with the ACA
mandated Eligibility and Claim Status Operating Rules
OESS began accepting complaints associated with compliance with the
operating rules on January 1, 2013
– If requested by OESS, covered entities that are the subject of complaints (known
as “filed-against entities”) must produce evidence of either compliance or a good
faith effort to become compliant with the operating rules during the 90-day period
• For more information review CMS’s Administrative Simplification Enforcement Tool
(ASET), which is a web-based application where entities may file a complaint against a
covered entity for potential non-compliance related to Transactions and Code Sets and
Unique Identifiers
* CMS Office of E-Health Standards and Services (OESS) is the U.S. Department of Health and Human Services’ (HHS) component
that enforces compliance with HIPAA transaction and code set standards, including operating rules, identifiers and other standards
required under HIPAA by the Affordable Care Act.
16
© 2013 CORE. All rights reserved.
Checkpoint #1: What do the Eligibility & Claim Status
Operating Rules Mean for Providers?
The ACA mandated Eligibility & Claim Status Operating Rules ensure realtime access to robust eligibility and claim status data for providers
–
How do providers benefit from the Eligibility and Claim Status Operating Rules?
•
More accurate patient eligibility verification: Real-time information on health plan eligibility and
benefit coverage before or at the time of service
–
•
•
Improved point of service collections: Real-time provider access to key patient financials including
YTD deductibles, co-pays, coinsurance, in/out of network variances via the ASC X12 v5010
270/271 transactions
Decrease in claim denials: Real-time claim status data ensures provider is aware of status in
billing process
–
–
Providers experienced a 24% increase in electronic eligibility verifications*
Providers experienced a 10-12% reduction in denials related to eligibility*
How can my provider organization ensure we benefit from the Eligibility and Claim
Status Operating Rules?
•
•
Identify all systems and vendors that touch the ASC X12 v5010 270/271 and ASC X12 v5010
276/277 transactions
Conduct internal gap analyses using the CAQH CORE Eligibility & Claim Status Operating Rules
Analysis & Planning Guide and/or reach out to your vendors to ensure compliance
* Based on the CAQH CORE Phase I Measures of Success Study when working with Phase I CORE Certified health plans.
17
© 2013 CORE. All rights reserved.
Mandated Healthcare Operating Rules:
Second Set - EFT & ERA
18
© 2013 CORE. All rights reserved.
Mandated EFT & ERA Operating Rules:
Required for All HIPAA Covered Entities
•
Healthcare EFT Standard: July 2012 CMS announces CMS-0024-IFC is in
effect adopting the NACHA ACH CCD plus Addenda Record (CCD+) and
the X12 835 TR3 TRN Segment as the HIPAA mandated healthcare EFT
standard
•
EFT & ERA Operating Rules: August 2012: CMS published an Interim
Final Rule with Comment, CMS-0028-IFC; adopts Phase III CAQH CORE
Operating Rules for the Electronic Funds Transfer (EFT) and Health Care
Payment and Remittance Advice (ERA) transactions except for rule
requirements pertaining to Acknowledgements*
Compliance date for both the Healthcare EFT Standard
and EFT & ERA Operating Rules is January 1, 2014
* CMS-0028-IFC excludes requirements pertaining to acknowledgements.
19
© 2013 CORE. All rights reserved.
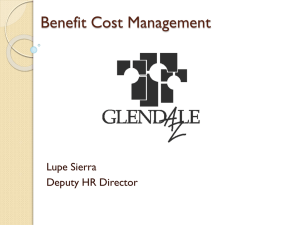
CAQH CORE EFT & ERA Operating Rules in Action
Indicates where
a CAQH CORE
EFT/ERA Rule
comes into play
Pre- Payment: Provider
Enrollment
EFT Enrollment
Data Rule
ERA Enrollment
Data Rule
Provider first enrolls in EFT and
ERA with Health Plan(s) and
works with bank to ensure
receipt of the CORE-required
Minimum ACH CCD+ Data
Elements for reassociation
Claims Payment Process
Health Plan
Health Care
Claim
Payment/Advice
(835)
Infrastructure
Rule
Claims
Processing
Payment/Advice (835)
© 2013 CORE. All rights reserved.
Provider
Billing &
Collections
Electronic Funds Transfer (CCD+/TRN)
Treasury
Bank
Stage 1:
Initiate EFT
20
Uniform Use of
CARCs &
RARCs Rule
Bank
EFT & ERA
Reassociation
(CCD+/835)
Rule
Treasury
Checkpoint #2: What do the EFT & ERA Operating
Rules Mean for Providers?
The ACA mandated EFT & ERA Operating Rules ensure more streamlined
provider enrollment and processing of the EFT & ERA transactions
–
How will providers benefit from the EFT & ERA Operating Rules?
•
•
•
–
Standardized electronic enrollment for EFT/ERA: Providers will be able to enroll in both EFT and
ERA electronically with all health plans using a consistent set of data elements
Potential reduction in manual claim rework: With health plans more consistently using denial and
adjustments codes per the CORE-defined Business Scenarios, providers will have less rework
Reduction in A/R days: Automated and timely re-association of EFT and ERA leading to
efficiencies and reduced errors for payment posting
How can my provider organization ensure we benefit from the EFT & ERA Operating
Rules?
•
•
Identify all systems and vendors that touch the ASC X12 v5010 835 and the Healthcare EFT
Standard transactions
Conduct internal gap analyses using the CAQH CORE EFT & ERA Operating Rules Analysis &
Planning Guide and/or reach out to your vendors to ensure compliance
* Based on the CAQH CORE Phase I Measures of Success Study when working with Phase I CORE Certified health plans.
21
© 2013 CORE. All rights reserved.
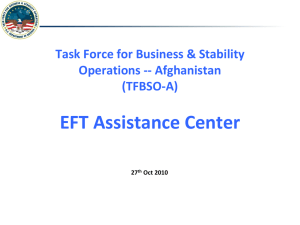
Example: CAQH CORE Uniform Use of CARCs and
RARCs Rule - Four Business Scenarios
Pre CORE
Rule 360
300+
RARCs
800+
CARCs
4
CAGCs
Inconsistent Use of
Tens of Thousands
of Potential Code
Combinations
Four Common Business Scenarios
Post CORE
Rule 360
CORE Business
Scenario #1:
Additional
Information
Required –
Missing/Invalid/
Incomplete
Documentation
(≈470 code combos)
CORE Business
Scenario #2:
Additional
Information
Required –
Missing/Invalid/
Incomplete Data
from Submitted
Claim
CORE Business
Scenario #3:
Billed Service Not
Covered by Health
Plan
CORE Business
Scenario #4:
Benefit for Billed
Service Not
Separately Payable
(≈330 code combos)
(≈30 code combos)
(≈300 code combos)
Code Combinations not included in the CORE-defined Business
Scenarios may be used with other non-CORE Business Scenarios
22
© 2013 CORE. All rights reserved.
Mandated Healthcare Operating Rules:
Third Set – Attachments, Prior Authorization, Enrollment, etc.
23
© 2013 CORE. All rights reserved.
Mandated Attachments, Prior Auths, Enrollment, etc.:
Third Set
•
•
24
Remaining operating rule mandate, effective January 1, 2016, will address the following
transactions:
–
Health claims or equivalent encounter information
–
Enrollment and disenrollment in a health plan
–
Health plan premium payments
–
Referral certification and authorization
–
Claims attachments
Secretary of HHS recommended CAQH CORE as author for the remaining ACA mandated
operating rules
–
Q1 2013: Key opportunities/out of scope areas being identified via research, survey findings, and call
discussions
–
Q2 2013: Potential rule options will be developed, reviewed, and agreed upon by CORE Subgroups
and Work Groups
–
Q3 2013: CORE Subgroup and Work Group discussion and straw polling will be conducted
–
Q4 2013: Detailed documentation of draft rule requirements by CORE Participants
© 2013 CORE. All rights reserved.
How to Contribute to Development of Third Set
•
Entities are encouraged to join CAQH CORE to directly contribute:
– The most effective way for individual organizations to assure they have direct input
on the mandated and voluntary operating rules is by becoming a CORE Participating
Organization; any entity may join. Cost is extremely low or free. Benefits include:
• Participation on Subgroup/Work Group rules-writing calls, surveys, straw polls, and ballots;
eligibility to Co-Chair
• Entity vote on CAQH CORE Operating Rules at Work Group and Full CORE Membership
voting levels
• Access to CAQH CORE Education Sessions specific to CORE Participating Organizations
•
Entities unable to join CAQH CORE can contribute via:
– CAQH CORE Town Hall Calls
• CAQH CORE holds bi-monthly Town Hall calls which provide attendees an update on recent
activities including status of rule development; email core@caqh.org to be added to the
distribution list
– CAQH CORE Industry Surveys
• CAQH CORE periodically conducts industry-wide surveys for directional feedback on
operating rule opportunities; email core@caqh.org to be added to the distribution list
25
© 2013 CORE. All rights reserved.
Engaging Vendors
26
© 2013 CORE. All rights reserved.
The Importance of Industry Collaboration
STREAMLINED ADMINISTRATIVE DATA EXCHANGE
Health
Plans
CORERequired
Data &
Infrastructure
Vendors/Clearinghouses
(Vendors may not be HIPAA covered entities)
V e n d o r - A g n o s t i c
27
CORERequired
Data &
Infrastructure
Providers
R u l e s
•
HIPAA-covered entities work together to exchange transaction data in a variety of ways
•
Vendors, often acting as business associates that provide services or process transactions
on a provider’s behalf, play a crucial role in enabling provider clients to realize the benefits
of industry adoption of CAQH CORE Operating Rules
•
Key steps to ensuring streamlined administrative data exchange:
–
Assess impacted systems/vendors: Understand which systems/vendors touch the
administrative transactions
–
Engage with your vendors: Confirm with vendors compliance/ability to support ACA mandated
operating rules as certain vendors, including PMSs, third-party billing companies, etc. are not
considered HIPAA-covered entities rather they act as the provider’s business associate
–
Encourage voluntary CORE Certification: Work with your vendors to publicly confirm systems
are conformant with applicable operating rules
© 2013 CORE. All rights reserved.
Analysis & Planning Guides Assist in Understanding
Applicability of Rules to Various Trading Partners
•
•
CAQH CORE offers two Analysis & Planning Guides (for Eligibility & Claim Status and EFT
& ERA) which provide guidance for Project Managers, Business Analysts, System
Analysts, Architects, and other project staff to complete systems analysis and planning for
implementation of the CAQH CORE Operating Rules
Guide should be used by project staff to:
– Understand applicability of the CAQH CORE Operating Rule
requirements to organization’s systems and processes that
conduct the transactions
– Identify all impacted external and internal systems and
outsourced vendors that process the transactions
– Conduct detailed rule requirements gap analysis to identify
system(s) that may require remediation and business
processes which may be impacted
•
The guides include three tools to assist entities in completing analysis and planning:
–
–
–
28
Stakeholder & Business Type Evaluation
Systems Inventory & Impact Assessment Worksheet
Gap Analysis Worksheet
© 2013 CORE. All rights reserved.
Voluntary CORE Certification
29
© 2013 CORE. All rights reserved.
Voluntary CORE Certification
•
Since its inception, CAQH CORE has offered a voluntary CORE
Certification to health plans, vendors, clearinghouses, and providers
–
–
Learn more about voluntary CORE Certification here
Voluntary CORE Certification provides verification that your IT systems or product operates
in accordance with the federally mandated operating rules
• Certification and testing are separate activities
–
–
Testing is completed by CORE-authorized testing entities and occurs on-line based on
stakeholder-specific test scripts; test scripts developed by CORE participants
Cost of testing and certification is extremely low or free
• CORE Certification is a 4-step process:
1.
Pre-certification Planning and Systems Evaluation:
–
–
2.
Sign and Submit the CORE Pledge:
–
3.
Comprised of three phases: Pre-testing, Testing and Post-testing
Testing is by stakeholder-specific test scripts by rule
Apply for the CORE Certification Seal:
–
30
Formally communicate your intent to pursue CORE Certification
CORE Certification Testing:
–
–
4.
Understand requirements of the CORE Operating Rules and scope your internal efforts to adopt rules
CORE has free gap analysis tool; email CORE@CAQH.org
Entities successfully achieving CORE Certification will receive a CORE “Seal”
from CAQH that corresponds with the CORE Phase and stakeholder-type
© 2013 CORE. All rights reserved.
Measures of Success
31
© 2013 CORE. All rights reserved.
CORE Measures of Success: Tracking ROI
•
CORE made an early commitment to track Measures of Success
•
Health Plans, vendors and providers that are pursuing voluntary CORE
Certification are invited to participate in the ROI study
– Also need participation from providers that are not CORE-certified, but trading data
with CORE-certified entities
•
CAQH CORE contracted with IBM to conduct tracking and analysis
– Analyze two 3-month measurement periods; volunteers asked to record expenses
and then impact one year later
•
Outcomes available from health plans covering 33 million lives and their
vendor and provider partners
– Provider groups working with CORE-certified health plans saw 10-12% fewer claim
denials and a 20% increase of patients verified prior to a visit
– The time needed by vendors and clearinghouses to connect to trading partners
significantly reduces with a common approach to connectivity
32
© 2013 CORE. All rights reserved.
The Business Case: All Stakeholders
•
More robust and accessible data has and will continue to enhance the
flow of information between providers and health plans
•
CAQH CORE Operating Rules help stakeholders leverage
investments
– Common infrastructure supports multiple methods and future transaction
types
– Solutions reusable with new partners
•
Streamlined implementation with CAQH CORE partners
– Better technical skill and resources
– Less customization, reduced testing
– Lower cost connectivity using the public internet
•
Costs to implement CAQH CORE Operating Rules vary widely,
depending on how much technology change is required
* IBM assessed results achieved by Phase I CAQH CORE Operating Rules early adopters (represents 33
million covered lives and 1.2 million providers)
33
© 2013 CORE. All rights reserved.
Checkpoint #3: Key Action Items for Providers
Determine if your organization is conducting the applicable electronic
transactions:
– The ACA mandated operating rules only apply to providers if they are conducting
the associated electronic transactions
If you conduct the transactions, assess your organization’s
readiness/compliance:
Use the CAQH CORE Analysis & Planning Guides (for Eligibility & Claim Status
and EFT & ERA) to help you assess impacted systems/vendors
Speak with your PMS vendor* about their compliance/ability to support your
practice
Ask your clearinghouse(s) if the product(s) your practice uses is compliant
(clearinghouses are HIPAA covered, and thus should already be compliant)
If not already, encourage your vendors/clearinghouses to become voluntarily
CORE-Certified to test conformance
* REMINDER: PMSs are not HIPAA-covered entities, and thus are not mandated to be compliant - so provider requests are critical!
34
© 2013 CORE. All rights reserved.
Additional CAQH CORE Resources
•
•
Become a CORE Participant
Join us for these free CAQH CORE Education Events held jointly with:
–
CMS OESS: “The Basics of Mandated Operating Rules for Providers”
•
–
ASC X12: “Eligibility and Claims Status Transactions: A Deep Dive”
•
–
Tuesday, March 26, 2013 from 2:00 pm to 3:30 pm ET
NACHA: “Save the Date” for an in-depth look at the EFT Standard and EFT &
ERA Operating Rules
•
35
Wednesday, March 20, 2013 from 2:00pm-3:00pm ET
Tuesday, April 10, 2013 from 2:00 - 3:00 pm ET
•
Review the CAQH CORE Operating Rules for free
•
Access general FAQs regarding the ACA operating rules mandate
•
Submit your questions to the CAQH CORE Request Process by emailing
core@caqh.org
© 2013 CORE. All rights reserved.
Appendix
36
© 2013 CORE. All rights reserved.
ACA Mandated Eligibility & Claim Status Operating Rules
Infrastructure
Data Content
Rules
Eligibility
& Benefits
Eligibility,
Benefits &
Claims
Status
High-Level CAQH CORE Requirements
Respond to generic and explicit inquiries for a defined set of 50+ high volume
services with:
• Health plan name and coverage dates
• Static financials (co-pay, co-insurance, base deductibles)
• Benefit-specific and base deductible for individual and family
• In/Out of network variances
• Remaining deductible amounts
• Enhanced Patient Identification and Error Reporting requirements
•
•
•
•
•
Companion Guide – common flow/format
System Availability service levels – minimum 86% availability per calendar week
Real-time and batch turnaround times (e.g., 20 seconds or less for real time and
next day for batch)
Connectivity via Internet and aligned with NHIN direction, e.g., supports plug and
play method (SOAP and digital certificates and clinical/administrative alignment).
Acknowledgements (transactional)*
*NOTE: In the Final Rule for Administrative Simplification: Adoption of Operating Rules for Eligibility for a Health Plan and Health Care Claim Status
Transaction, requirements pertaining to use of Acknowledgements are NOT included for adoption. Although HHS is not requiring compliance with any
operating rule requirements related to Acknowledgements, the Final Rule does note “we are addressing the important role acknowledgements play in
EDI by strongly encouraging the industry to implement the acknowledgement requirements in the CAQH CORE rules we are adopting herein.”
37
© 2013 CORE. All rights reserved.
ACA Mandated EFT & ERA Operating Rules
Data
Content
Rule
Uniform Use of CARCs
and RARCs (835) Rule
•
Identifies a minimum set of four CAQH CORE-defined Business Scenarios with
a maximum set of CAQH CORE-required code combinations that can be
applied to convey details of the claim denial or payment to the provider
•
•
•
Identifies a maximum set of standard data elements for EFT enrollment
Outlines a flow and format for paper and electronic collection of the data
elements
Requires health plan to offer electronic EFT enrollment
•
Similar to EFT Enrollment Data Rule
•
Addresses provider receipt of the CAQH CORE-required Minimum ACH CCD+
Data Elements required for re-association
Addresses elapsed time between the sending of the v5010 835 and the CCD+
transactions
Requirements for resolving late/missing EFT and ERA transactions
Recognition of the role of NACHA Operating Rules for financial institutions
Claim Adjustment Reason Code (CARC)
Remittance Advice Remark Code (RARC)
Rule 360
EFT Enrollment Data Rule
Rule 380
ERA Enrollment Data Rule
Rule 382
Infrastructure
High-Level Requirements
EFT & ERA Reassociation
(CCD+/835) Rule
Rule 370
•
•
•
•
Health Care Claim
Payment/Advice (835)
Infrastructure Rule
Rule 350
•
•
•
Specifies use of the CAQH CORE Master Companion Guide Template for the
flow and format of such guides
Requires entities to support the Phase II CAQH CORE Connectivity Rule.
Includes batch Acknowledgement requirements*
Defines a dual-delivery (paper/electronic) to facilitate provider transition to
electronic remits
* CMS-0028-IFC excludes requirements pertaining to acknowledgements.
38
© 2013 CORE. All rights reserved.