FAMILY ASSESSMENT
TOOLS
DEPARTMENT OF PUBLIC HEALTH & PREVENTIVE MEDICINE
FACULTY OF MEDICINE, UNIVERSITAS PADJADJARAN
2013
LEARNING OBJECTIVES
• Describe the advantages for assessing
family (C2)
• Define the family genogram, family map,
family APGAR and its function (C2)
Why do we Need tools to Assess the family?
• assess family functioning
• assess family dynamic
• assess coping mechanisms
of the family
• assess resources
• assess family structure
Why do we Need tools to Assess the family?
• to have a picture of the multigenerational
patterns of behavior or illnesses.
• to assess the normal crisis or common
illness to be encountered in each stage of
development.
• to provide anticipatory care and guidance.
An understanding of the family in terms of the
struggles to be functional will enable FP to make
correct diagnosis and intervention
FAMILY DYNAMICS
• An interactions and
relationships among
the individual
members of a family
• Reflects and
influence the
physical, mental and
spiritual health of the
individuals in a
family.
FAMILY DYNAMICS
• An understanding of the dynamics helps the
attending family physician to diagnose the
disease and dis-ease in the patient sitting in
his consultation room and to recognize the
factors that may help or retard the recovery of
this patient.
FAMILY ASSESSMENT TOOLS
Anatomy
• Genogram
Development
• Family
life cycle
Function
• APGAR
• Family
Map
• Lifeline
• SCREEM
Impact
• BATHE
GENOGRAM
Is a biopsychosocial family tree.
It records the family in its life cycle,
family illnesses and relationship
A genogram is a versatile clinical tool
that can help FP integrate a patient’s
family information into the medical
problem-solving process for better
patient care
• A genogram supplements the problem list giving
FP an overview of the main problems affecting the
family over 3 or more generations
• A genogram can be drawn in skeletal form during
one of the first few visits, ideally the first visit and
then it can elaborated during subsequent visits as
more is known about the family
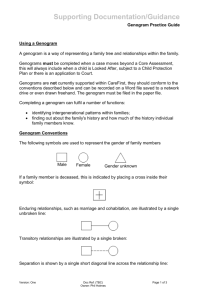
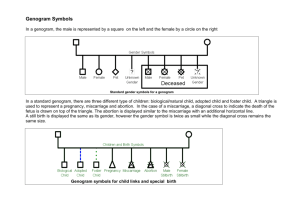
GENOGRAM COMPONENTS
Symbols
Standardized Symbols used in Family Genograms
male
female
d
date of divorce
D
Date of death
abortion or miscarriage
Sex not specified
Deceased/death
A
Adopted female
b
date of birth
m
date of marriage
Induced abortion
Pregnancy-child in utero
Dizygotic twins
Monozygotic Twins
STANDARDIZED SYMBOLS USED IN FAMILY GENOGRAMS
Symbols of diseases or situation
Obesity
♥
♥
Allergy
xxx
xxx
Alcoholism
Heart disease
Stroke
Depression
Asthma
War Casualty
Hypertension
COMMONLY USED ABBREVIATIONS
ALC
Alcoholic
GI
GI tract disease
ALL
Allergy
HT
Hypertension
MI
Myocard Infarction
ARTH Arthritis
CAD
Coronary Artery
Disease
CVA
Cerebrovascular
Accident
CA
Cancer
DEP
Depression
DM
Diabetes mellitus
MVP Mitral Valve Prolapse
PUD Peptic Ulcer Disease
SLE Systemic Lupus
Erythematosis
TB
Tuberculosis
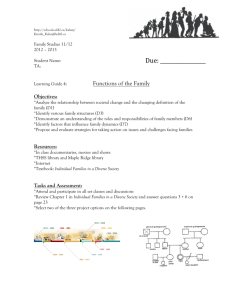
STANDARDIZED SYMBOLS USED IN FAMILY GENOGRAMS
Close relationship
1989
married and year
Family living together
1990
1992
Separation and
year
Divorce and year
1989
Unmarried
relationship
Conflictual relationship
Distance relationship
1989
1992
Bakri, as of 8 April 2010
1. Symbols
2. Three or more generations
3. The name of family
4. A listing of the first born of
each family to the left, with
siblings listed sequentially to
the right
5. The names of all family
member
1969
I
II
III
Ardi,68
1970
Nia,64
6. Age or year of birth of all family members
7. Any deaths, incl. age of death and cause
8. Dates of marriages and divorces
9. Significant diseases or problems of family members
10. Indication of members living together in the same
household
11. A key depicting all symbols used
12. Symbols selected for simplicity and maximum visibility
FAMILY INFORMATION IS USED IN 3 TYPE
SITUATIONS:
1. Evaluating somatic complaint by testing
biopsychosocial hypotheses
2. Assessing a patient’s risk for biomedical and
mental disorders
3. Planning management by considering how
family factors may facilitate or complicate it
USES OF THE GENOGRAM
(CROUCH AND DAVIS, 1987)
• Allowing the family physician and other health professional to
review quickly the family situation
• Building rapport by using the first names of family members,
knowing who is living in the home
• Identifying at a glance significant risk factors : Hypertension,
DM, Ca, Obesity etc
• Recognizing the need for screening in patients who at high risk
• Promoting lifestyle changes and health education (healthy
living)
• Demonstrating that family relationship are a concern of the
family physician and important to the health of each family
member
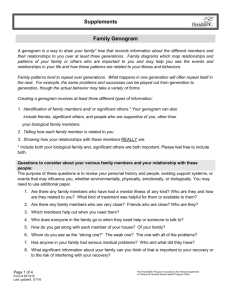
Relationship of the members
This is a self-drawing by an 8 year
old girl who participated in a
support group for children
affected by domestic violence
sponsored by Cedar Valley
Friends of the Family.
One cannot escape sensing this
child's unhappiness; the frown she
drew on her little face clearly sets
the mood. However, the up-sidedown rainbow is perhaps the most
significant message... Generally,
we think of rainbows as a happy
reminder of hope for the future. In
this simple drawing, the little girl
innocently, but quite vividly
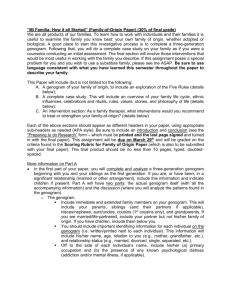
FAMILY MAP
Genogram : 24 January 2008
Ani
Sugeng
myoma
84
AMI
43
60
Utomo Sri
58
DM
CA
Colon/Renal
54
FAM
Arti
Putro
Lung Ca
1959
48 44
Tyio
Tuti
84
44
Nina
Sam 46
20
16
Aria
Imam
APGAR
• This is a five-item questionnaire
designed to elicit the patient’s
perception of the current state of his
family relationships, and serves as a
rapid screening instrument for family
dysfunction.
APGAR
• Adaptation is the capability of the family to utilize and
share inherent resources
• Partnership is sharing of decision making. This measures
the satisfaction attained in solving problems by
communicating.
• Growth refers to both and emotional growth. This
measures the satisfaction of the availability freedom of
change
APGAR
• Affection is how emotions like love, anger and hatred are shared
between members. This measures the members’ satisfaction
with intimacy and emotional interaction that exist in the family.
• Resolve refers to how time, space and money are shared. This
measures the members’ satisfaction with the commitment made
by other members of the family.
• 8-10 point (Highly functional family)
• 4-7 point (Moderately dysfunctional family)
• 0-3 point (Severely dysfunctional family)
BATHE TECHNIQUES
(Stuart and Lieberman’s)
• 15 minutes method of
primary care counseling
• It helps draw out the quiet
patient and provides a
structure of when to move on
in a talkative patient
B = Background
A = Affect
T = Troubling
H = Handling
E = Empathy
• B = Background : assessing what’s the
background situation (areas of psychological
problems)
• “How are things at home?” At work?
• What’s different in your life between now and before?
• A = Affect = the patient’s affect (about common
areas generating strong feelings)
• “How do you feel about your home life?”
• “How do you feel about your work/school?”
• T = Troubling: the problem that is most troubling for
the patient
• “What most worries you about your life?”
• “How stressed are you by this problem?”
• “What do you think this problem means to
you?”
• H = Handling: the manner in which the patient has
been handling the problem, problems are often
mishandled life difficulties
• “How are you handling the problems in your
life?”
• “What have you tried to solve the difficulty?”
• “How much support are you getting at
home/work?”
• “Who gives you support for dealing with
problems?”
• E = Empathy : respons that conveys
empathy,express understanding of the patient’s
distress
• “I can understand that you would feel angry”
• “That must have been difficult”
• “This is a tough situation to be in”
Thank you…
1. Rakel RE. The Family Genogram. In Rakel RE.
Textbook of Family Practice. Sixth Edition. WB Saunders
Co. Philadelphia. 2002. pp 19 – 30.
2. Lee Gan, Azwar.A, Wonodirekso. Family Medicine
Practice. Singapore, 2004. section 3 chapter 3 pp 58-62