Inequalities in young people’s health and wellbeing:
UK and international perspectives
AYPH Conference, March 1st 2011
‘Making a difference: Improving health and wellbeing outcomes for young people’
Professor Candace Currie
Child and Adolescent Health Research Unit (CAHRU)
University of Edinburgh
Examining the evidence
for young people’s health improvement
Where is action needed?
How do we identify health
needs?
Where is action needed? How do we identify
health needs?
• Comparative approaches
• Detection of inequalities and inequities in health
• Social determinants of health – production on
inequalities
Health inequalities
‘Measurable differences in health experience and
health outcomes’ according to characteristics such
as:
• gender
• age
• geography
• socioeconomic status
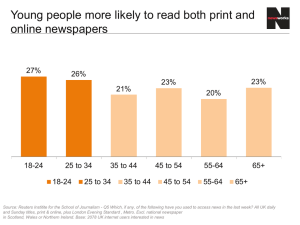
Inequalities in Young
People’s Health
Report from the Health Behaviour
in School-Aged Children (HBSC)
2005/06 Survey in 41 countries
Currie et al, 2008. WHO,
Copenhagen
Health Policy for Children
and Adolescents, No. 5
Gender and Age
• United Nations has stated there is an international
responsibility to achieve equality between the genders
• Yet very little attention is given to gender differences in
most youth health reports
• Adolescent age group often merged with younger
children or with young adults in health statistics
• Importance of different stages of puberty, physical and
emotional development, growing independence and
choice neglected
• Some health risks already established by age 11, others
begin and increase during adolescent years
UNICEF ‘State of the World’s Children’
Report (2011)
‘Where health data on
adolescence are
available, it is often
not disaggregated by
sex, age cohort or
other factors that
could give muchneeded details on the
situation of
adolescents’.
Socioeconomic status
• socioeconomic inequalities are related to social
status and resources such as material
possessions
• there are a number of ways to measure
socioeconomic status of adolescents
• HBSC report uses family material affluence as a
measure of socioeconomic status – HBSC
FAMILY AFFLUENCE SCALE (FAS)
Iceland
Chart showing country variation
in levels of family affluence
Family affluence
low
medium
high
Turkey
Examining the evidence:
for young people’s health improvement
• how do Scotland, England and Wales compare
with each other?
• how does health of young people in UK compare
with Europe and North America?
• what health inequalities do we observe among
young people in UK and internationally?
• what are the implications for action?
Health fair/ poor (age 15)
6th
7th
8th
• UK countries all rank high
on fair/poor health
• In all countries, girls report
poorer health than boys
• In most countries, rates of
poorer health increase
with age especially among
girls
Family affluence
and self–rated health
family affluence
fair/ poor health
Daily fruit (age
15)
3rd
• UK variation
• In UK and all other
countries girls > boys
• Fruit eating declines
with age in almost all
countries
20th
21st
Family affluence and
daily fruit
family affluence
daily fruit
Weekly smoking (age 15)
• England ranks low
compared to Wales and
Scotland – due to girls
16th
19th
• In UK girls > boys;
same is true in about
half of countries;
reverse is true in east
Europe
29th
Family affluence and
weekly smoking
family affluence
weekly smoking
• in north (Europe and N America)
and western Europe
• among girls more commonly
than boys
Drunk at least twice (age 15)
3rd
5th
8th
• All UK countries have high
rates of drunkenness
• In UK girls are as/ more
likely to get drunk than
boys, unlike most other
countries
Picture across UK is similar in terms of prevalence
and gender patterns for self-reported health and
patterns of alcohol use
England relatively positive
cf Scotland & Wales
• Food habits
• Hours spent TV
watching
• Smoking
• Cannabis use
• Condom use
England relatively negative
cf Scotland & Wales
• Medically attended
injury
• Daily 60 minutes of
physical activity
• Bullying
Explanations for similarities and differences
across UK?
• Cultural similarities – eg youth drinking culture
across the UK?
• Differences found in UK health patterns may be
explained by social/demographic factors or
differences in policy and practice?
• Further analysis of HBSC and other data
sources required to answer these questions
UNICEF Innocenti Report Card 9:
‘Children left behind’ (2010)
• Compares the gap in well-being between the
median (average) and worst off children in
richest (OECD) countries
• Considers three aspects of well-being: material,
educational, health
• Asks ‘how far are children being allowed to fall
behind?’ in each country
Measuring bottom end inequality in health
• Three indicators are used:
– self-reported health complaints
– healthy eating
– and frequency of vigorous physical activity
• All three are well-established markers for
children’s current and future health - data are
derived from the 2005-2006 HBSC Survey
Health Inequalities: a breakdown
Physical activity
-3.0
-2.5
-2.0
Fruit and Veg
Health Complaints
-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Netherlands
Norway
Portugal
Germany
Switzerland
Belgium
Ireland
Denmark
Canada
Czech Republic
United Kingdom
Slovakia
Austria
Sweden
France
Finland
Poland
Iceland
Luxembourg
Greece
Spain
United States
Italy
Hungary
Turkey
England
Scotland
Wales
Health Inequality: an overview
-2.0
Netherlands
Norway
Portugal
Germany
Switzerland
Belgium
Ireland
Denmark
Canada
Czech Republic
United Kingdom
Slovakia
Austria
Sweden
France
Finland
Poland
Iceland
Luxembourg
Greece
Spain
United States
Italy
Hungary
Turkey
England
Scotland
Wales
-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
2.0
Social determinants of health
In UK and internationally also observe
marked differences in social
contextual dimensions which may
explain help to explain health
inequalities
Easy to talk to their mother
(15 year olds)
• England ranks 26th
(Wales is 23rd and
Scotland 32nd )
• In most countries boys
find it easier to talk to their
mother than do girls
23rd
26th
32nd
Three or more close
friends (at age 15)
3rd
4th
6th
• England ranks 4th (Wales
is 6th and Scotland 3rd)
• No gender difference in UK
but in some countries boys
> girls
Like school a lot (age 15)
• England ranks highest and
Scotland ranks lowest
13th
20th
• No gender difference in
England and Wales but
girls> boys in around half of
countries
28th
Variation in supportive social contexts in UK
• England is doing well in terms of positive
socioeconomic environment and in terms of
liking school cf other UK countries
• All UK countries score high on friendships with
peers
• Family support appears weaker in UK than many
other countries
2nd
Pressured by schoolwork
(age 15)
3rd
• Wales and England
more pressured than
Scotland
24th
• In most countries girls
more likely to feel
pressured
4+ evenings out with
friends (age 15)
7th
12th
• Scotland ranks highest
and England lowest in
UK
• Boys > girls in most
countries
15th
Variation in ‘risky’ social contexts in UK
• Young people in England &
Wales report high level of
pressure stemming from
schoolwork – can impact on
mental health
• Being out in evening with friends
4+ nights a week is a known
factor in risk taking behaviour –
less prevalent in England than
other UK countries
Inequalities in health of young people across
the UK
• variation in different dimensions of health experience
across UK – need to understand more about underlying
causes
• common sources of inequality are seen to prevail related
to gender, age and family affluence
• overall these are similar to inequalities experienced by
young people throughout Europe and North America but
gender/ socioeconomic patterns do vary
Implications for policy and practice to safeguard
and enhance health of adolescents
• Need to take into account prevailing age, gender
and socioeconomic inequalities
• Evidence vital for priority setting and for
developing approaches to prevention/ intervention
• Identifying areas of need indicates where need to
build assets to support health
Investing in health of young people
‘In the global effort to
save children’s lives,
we hear too little about
adolescence’
‘Surely, we do not want to
save children in their
first decade of life only
to lose them in the
second’
INVESTING IN YOUNG PEOPLE TO SECURE SCOTLAND’S FUTURE
March 22, 2011 from 9AM until 5PM
Speakers include:
►Vivian Barnekow World Health
►Leonardo Menchini Unicef
►David McQueen IUHPE
Organisation
►Clive Needle Euro Health Net
►Dominic Richardson OECD
►David Pattison International Devt. Health Scotland
►Gerry McCartney Public Health Observatory
►Louise Warde-Hunter Action for Children
Conference Fee: FREE, Please register as soon as possible as places are limited.
Venue: John McIntyre Conference Centre, Edinburgh
Full programme and registration:
www.education.ed.ac.uk/cahru
INVESTING IN YOUNG PEOPLE TO SECURE SCOTLAND’S FUTURE
March 22, 2011 from 9AM until 5PM
Topics include:
o Young peoples’ health in international context
o Challenges to Scotland’s health
o Young peoples’ health over the last 20 years
o Sexual health in Scotland
o Mental Health, Transitions and Violence
o Children left behind
o Investment in young people
o Social inequalities & creating a healthy community
Conference Fee: FREE, Please register as soon as possible as places are limited.
Venue: John McIntyre Conference Centre, Edinburgh
Full programme and registration:
www.education.ed.ac.uk/cahru
Thank you
Further information on HBSC
and its publications at www.hbsc.org