Integration Networks Pathways - MidCentral District Health Board
advertisement

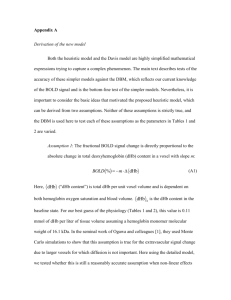
Integration Networks Pathways Addiction & Mental Health District Group Alistair Watson 7 May 2013 The burden of long term conditions • Almost one in three of the population (and half of those over 60) have a long term condition. • This group accounts for two thirds of the health spend. • The number of people with comorbidities is expected to rise by a third in the next ten years. • Common mental health problems affect about one in seven of the adult population, with severe mental health problems affecting one in a hundred. • These conditions fall more heavily on the poorest in society Source: Dept. of Health, England (2012) Local Maori Health Statistics Health Needs Assessment 2005 • • • • Cancer death rate 40% higher Respiratory death rate 80% higher More likely to smoke Make up 15.2% MDHB’s pop – Poorer health yet 14.2% admissions • Three times more likely to not attend outpatients Horowhenua •Higher diabetes discharge rates compared to MidCentral overall •18% more than expected COPD hospital discharges compared to MidCentral overall •19% higher than expected neoplasm (cancer) deaths compared to MidCentral overall (age adjusted). •Children aged 5 showed poorer dental health than children from Manawatu •The highest proportion of smokers among MidCentral territorial authorities (24.6%) •20% higher than expected number of deaths compared to MidCentral overall •Lowest % of households with access to a car Demographics Statistics New Zealand, March 2006 Contracted Providers of Health and Disability Services in MDHB Region General Practice 42 Aged Residential Care facilities 37 Community Pharmacies 33 Dentists 21 Mental Health 8 Personal health 1 Primary Care 99 Secondary care 3 TOTAL 204 OECD Admission rates 2009: COPD The Way Services Are Organised & Utilised Does Matter • Despite standardised approaches to management of common conditions there are major differences in way the care is delivered both nationally & locally • Current way services are utilised is based on the way they are structured & provided • Limited effectiveness due to fragmented planning & organisation and opportunity for improvement exists at every stage of the continuum Changing models of care Moving to care models that shift expenditure / activity away from hospital care, deploying resources more effectively to improve health outcomes and patient experience. Ref: Dr Helen Bevan, NHS Institute Patients with Complex Needs (Integration: A Report from the NHS Future Forum) • Intensive users of services, repeatedly crossing traditional organisational and sector boundaries. • Gaps, duplications or poor reliability of care multiplied as their journeys progress • More difficulty in understanding their or understanding their often tortuous care journeys making it more difficult to exercise choice or control, or manage their own care • Needs may include education, social care, housing & justice Patients with Complex Needs (Integration: A Report from the NHS Future Forum) • Groups most likely to benefit from integrated care include – Children and adults with complex needs – People with enduring mental heath problems – Homeless people – Frail older people and their carers – People at the end of their lives receiving palliative care Expectations for patients with complex or long-term needs (Integration: A Report from the NHS Future Forum) • To receive care as close to home as possible • To be informed about the options available to them • The opportunity to discuss their options with a professional skilled in shared decision making • Easy access to a named care coordinator who knows them and is able to provide a tailored level of support to navigate their care journey and make choices at appropriate junctures • To know what to expect at each step of planned care journeys Expectations for patients with complex or long-term needs (Integration: A Report from the NHS Future Forum) • To have an integrated care plan and where appropriate be offered an integrated budget • Every provider involved in the individual’s care to have access to their care record • Transitions between professionals, teams and organisations to be safe, smooth and efficient • To understand clearly and simply what care and support they are eligible for and how they might pay for it if they are not eligible for state funding • To be confident that appropriate information, training and support are available for carers Definition of Integration “the act of making a whole out of parts, the coordination of different activities to ensure harmonious functioning” Clinical Integration • Many approaches with different terminology: shared care, transmural care, intermediate care, seamless care, disease management, case management, continuous care, integrated care pathways, integrated delivery networks • Patient centric view and needs of complex patients with chronic illness are considered • Scope varies but requires some form of seamless care or multiprofessional approach that values the role of all health professionals • Aim to improve coordination and integration of services Integration • Types of integration (e.g., organisational, professional, clinical, functional) • Breadth of integration (e.g., vertical, horizontal, virtual) • Degree of integration (i.e., across the continuum: linkage, co-ordination to full integration) • Processes of integration (i.e., cultural and social as well as structural and systemic) Clinical Integration • Different models of care: consultative, collaborative, coordinated, multidisciplinary, interdisciplinary, integrative • A continuum from informal to formal arrangements with an increasing intensity of governance in the relationship between the providers • More fully integrated systems coordinate more information, activities and resources and consolidate organisational structures • Unlikely one model appropriate for all organisations or situations Principles of Clinical Integration (Valentijn PP. Int J Integr Care 2013) • Coordination of person focused care in a single process across time, place and discipline • Requires a person-focused perspective to improve someone’s overall well-being and not focus solely on a particular condition • Patient as a co-creator in the care process; with shared responsibility between the professional and the person to find a common ground on clinical management • Emphasis should be placed on a person’s needs, with people coordinating their own care whenever possible Requirements For Change In Healthcare The essential requirements for success are: • Broad-based clinical leadership • District-wide service planning & organisation • Avoiding the fragmentation induced by existing service structures (Bate P, Mendel P, Robert G: Organizing for Quality. Oxford: Radcliffe Publishing; 2008) MidCentral DHB Journey to date MidCentral DHB Journey to date • • • • Access Community Participation Coordination of Services Infrastructure Development; increasing sector capacity • Integration between primary and secondary care • Quality MidCentral DHB Priority Plans • • • • • • Respiratory Diabetes Cardiovascular Cancer Depression Oral Health Additional Clinical Services • Locally based primary chronic care teams : smoking cessation, physical activity, clinical dieticians • Locally based integrated “disease state” & cancer nurses and respiratory physiotherapists • Psychological support • Community pharmacy • Community specialist cardiology clinics, heart failure service & tests • Community GP sleep apnea, pulmonary rehabilitation & spirometry • Extended palliative care, Liverpool Care of the Dying pathway, psychooncology Other Developments • Multidisciplinary Disease Management advisory groups • Primary Care Health Development Team – Professional development Knowledge and skills frame works, Nurse practitioners – Developing new models of care; “Long term conditions” nursing • Compass Health – Provide managed service operations: community nurses Better Sooner More Convenient Business Case 2010 Vision District wide response to providing the best possible patient experience whilst building a clinically and financially sustainable system. BSMC Programmes of Activity • • • • • • Acute Demand Management Older person’s services Integrated family health centres Whanau Ora Systems levers Other Acute Demand Management • • • • • Self management support Chronic care management Case management Walk in clinics Enhancing intermediary care/Recovery at home • Single point of access to after hours care Older Person’s Services • Inter RAI • Interdisciplinary older person’s teams • Care planning and management tools Systems Levers • • • • • Clinical networks Clinical pathways Organisation design, leadership & governance Workforce development Information management Organisation design, leadership & governance • DHB Clinical Leadership Council • Combined ALT/CPHO Governance and Leadership • DHB Quality Improvement Framework • Contracted Providers Network (proposed) • DHB Clinical Networks • Collaborative Clinical Pathway Programme • Health Care Development Team Workforce development • Transformational leadership programme • Interdisciplinary Knowledge and Skills Framework including LTC and case management • Career path for nursing from novice to expert leading to Nurse Practitioners • GP training scheme Information management • • • • • • • • Traffic Light system “Realtime” GP performance data Shared Care Record (with proposed patient access) Map of Medicine integrated with MedTech (and Houston?) Clinical Portal (“Concerto”) Best Practice Web based Apps Patient access centre Other • • • • Medicines management programme Devolution of radiology Youth one stop shop Urgent community care paramedic pilot (UCC) MidCentral DHB Network Framework Network: an interconnected group or system Clinical Network: is a social-professional structure made up of doctors, nurses and allied health staff tied through interdependencies such as collegiality, friendship, referrals, function or common interest Braithwaite 2010 New Zealand Networks • National – Cardiothoracic – Cardiac - Stroke - Long Term Conditions • Regional – Cancer – Midlands: maternity, elective, cardiac, renal, rural, stroke, mental health/addictions, older people, radiology – Central: cardiac, renal, mental health/addictions, older people, population health, (stroke) – Greater Auckland Integrated Health Network • District – Canterbury: • aged, child & youth, collaborative care, IFHC’s, laboratory, long term conditions,medication, pharmacy, primary care liason, rural urgent • Healthcare pathways – MidCentral: • child/tamariki, mental health/addictions, cancer, elder, urgent, long term conditions, (elective) • Collaborative clinical pathways (Map of Medicine) Network Types • Informational Networks – Education, research and guidelines • Co-ordinated Networks – Care pathways, joint assessments, no binding contract, a ‘managed clinical network’ • Procurement Networks – Budget given to a lead funder or provider, to contract with a range of organisations to deliver integrated care • Managed Networks – Highly managed long-term network of partners, e.g. Kaiser Permanente delivering and co-ordinating care for a whole population (Goodwin et al, 2006) “Need to harness the natural complex sociotechnical properties of the Health System” Braithwaite, Runciman & Merry 2009 Two Types Of Networks • Type A: purpose-designed, funded or imposed by authority, in structured organisational or institutional forms [designed, mandated networks] • Type B: those composed of the relationships amongst clinicians, via professional interests, referrals, supports, friendships, communications & advice [natural networks] Braithwaite, Runciman & Merry 2009 Socialising Network in Emergency Department. Creswick N,Westbrooke JI & Braithwaite J. Understanding communication networks in the emergency department, BMC Health Services Research, 2009 9 247. Natural Networks • For every health care problem there are hubs and clusters made up of clinicians & others with a special interest & expertise in that area • Form a self selected group with a natural interest to identify and solve ‘coal face’ clinical problems in voluntary collaboration with others • Clinicians with common concerns & complementary expertise voluntarily grouped Child Health/Tamariki: To improve the provision of health services to children and their families/whānau through optimised service development and delivery processes Child Health/Tamariki Ora District Group: Functions/Objectives • Promotes sector wide inclusive approach, that incorporates Whānau Ora • Develops an open & supportive environment for those working in the child health/tamariki ora community • Improves quality, safety & effectiveness of care • Develops & sustains collaboration & communication with stakeholders and between related network groups • Develops an annual plan including about 6 time limited projects Child Health/Tamariki Ora District Group: Membership • DHB funding manager • Consumer representative • Intersectoral representative • Child health advocate • Maternal • Clinicians: • Nursing • Allied • Medical • • • • Managers Community Maori NGO Network Forum • To engage with clinicians & consumers to: – – – • • Exchange information on current network activities Identify & prioritise current issues, & Seek advice on strategies to address current issues Open to all interested consumers, clinicians & managers Held once per year, or more frequently according to need District Group Work Plans • Choose about 6 time limited coal face projects • May include – Developing patient-centred integrated model of service delivery – Clinical pathways – Developing common performance indicators – Developing evidence-based clinical standards, guidelines & protocols • Requires formation of about 6 person work group & collaboration with wider clinical community Mental Health And Addictions Work Plans • Development of a robust crisis respite journey • Alcohol and drug services targeted for young people • Create models for change / treatment journey PHO / GP / Psychiatrist support (to improve connectedness) • Increase access to the shared care scheme to support primary delivery • Link to Whānau Ora • Suicide minimisation across the district • Building psychosocial models of care, brief interventions Child Health/Tamariki Work Plans • ‘Health Home’: Establish a single, principal data repository to link families & whānau with service providers & facilitate access • Disability-ASD children: Increase capacity of and improve access to secondary care child health services for children with autism spectrum disorder • Behavioral and Learning Referral: Consolidated entry into services for those with behavior & learning issues • Parental child health education: Teaching parents how to assess & manage their child’s health care needs & issues • Map of Medicine Child/Tamariki Ora: Further integrate 1 & 2 care services for child health To assist MidCentral DHB create and maintain a Clinical Network structure and in doing so ensures that clinicians and consumers (and their family/whānau) are the core of health service development and improvement Transitional Steering Group: Membership • Chief medical officer • Director of nursing • Chair Central PHO Clinical Board • PHO clinical director • PHO management representative • Funding division representative • Operations directors • Community representative • Manawhenua Hauora Board representative • PHO director Maori Health • Maori health representative • Business case representative • Chairs DMGs/Reference Groups • Director integrated care (Chair) To provide leadership, direction and influence to ensure clinical quality, effectiveness and sustainability of health services for the people/populations of the district Central PHO Alliance Leadership Team (ALT) •Ultimate programme governance •Programme Sponsor CEOs - MDHB and Central PHO Sign-off from organisational perspective MDHB Clinical Leadership Council Receives all information Monitors the programme from a clinical perspective Reviews and advises if significant impacts to delivery of care, funding allocations or resources No changes/ No impacts identified in pathway Operations Director(s), MidCentral Health, GM and Clinical Director CPHO MidCentral Health & CPHO Clinical Boards Sign off the paper from a managerial perspective Review and sign-off paper If changes to resourcing required If changes to clinical practice Transitional Steering Group Approves the final report / outcome District Groups Considers report/outcome and feedbacks to working group Approves the final report / outcome Working Groups Managerial/ Organisational Clinical Programme Undertake to complete working plan of the District Group District Groups/ Clinical Networks Nominate pathways for development Develop workplans Communication • • • • • • • • Network brand Website Network newsletter 3 monthly DHB & PHO newsletters Press releases Presentations at clinical & other meetings Fora Surveys of constituent groups • SharePoint for district & collaborative groups Resourcing • Work undertaken as part of usual role (DHB and other employees) • Meetings expected to be during work hours • Parking & travel expenses for meetings • Use of normal DHB support functions • 0.5 FTE administration officer • 2.8 FTE network manager • 0.5 FTE clinical lead NSW Agency for Clinical Innovation - Clinical Networks Project Logic Framework Haines et al. Implementation Science 2012, 7:16