Evidence based rehabilitation
advertisement

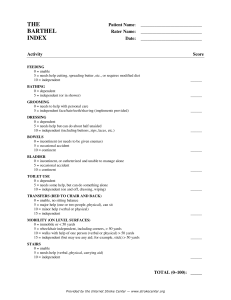
“Evidence based rehabilitation” Professor Cath Sackley PhD, MSc, MCSP, FCOT Rehabilitation Sciences, University of East Anglia A cluster randomised controlled trial of an occupational therapy intervention for residents with stroke living in UK carehomes. Cath Sackley, Marion Walker, Andrea Roalfe, Caroline Watkins, Chris Burton, Jonathan Mant, Karen Lett, Keith Wheatley, Bart Sheehan, Lesley Sharp, Katie Stant, Sheriden Bevan, Farzana Rashid, Joanna Fletcher Smith, Kerry Steel, Guy Peryer, Gina Sands, Joanna Briggs, Kate Wilde, Peter Sharp, Lisa Irvine, Garry Barton, Kath Mortimer, Max Feltham National Institute for Health Research. NIHR HTA Research Programme through clinical interest ~ 25% of all stroke survivors are unable to go home after their stroke • Significant rise in the number of people living with stroke related disabilities between 1990 – 2010 • Stroke survivors residing in care homes are more physically and cognitively impaired with high support needs compared to those living in the community UK MRC Framework for Evaluating Complex Interventions Phase IV Phase III Phase II Phase I Pre-clinical Theory Modelling Continuum of increasing evidence Exploratory trial Definitive RCT Long term implementation Phase 1 A survey of immobility related complications Residents with stroke Contractures- 59 (48%) Pressure sores- 24 (20%) Shoulder pain-59 (48%) Falls- 80 (66%) Other pain- 59 (48%) How do residents spend their days? walking with assistance 1.7% standing 1.0% walking without assistance 0.3% Sitting (eyes open or closed) 97.0% Sackley C. et al. 2006. International Journal of Therapy and Rehabilitation, 13(8): 370-373. Phase 1 Staff Attitudes Staff feel they are employed to care Care viewed as ‘doing for’ rather than maintaining independence Would like to know more about basic rehab Care Home AHP provision Regional Survey AHP provision in care homes: • At best, patchy • Rarely used qualified staff • Inequality in access (particularly Occupational Therapy) Staff attitudes : • Staff feel they are employed to care • Care viewed as ‘doing for’ rather than maintaining independence • Staff showed an interest in learning about rehabilitation practices Sackley C.M. et al. 2001. Age and Ageing, 30(6): 532-3. OTCH Phase II exploratory trial Cluster RCT (n=118). Primary outcome: Barthel @ 3 months. Poor Outcome 20/63 (32%) were worse/dead in the intervention group compared with 31/55 (56%) in the control group. Group difference –25% (95% CI –51% to 1%), similar at 6 months. Self Care ADL BI score had increased by 0.6 (SD 3.9) in the intervention group and decreased by 0.9 (2.2) in the control group. Group difference 1.5 (95% CI –0.5 to 3.5). Mobility RMI score increased by 0.4 (3.0) in the intervention group decreased by –0.4 (1.9) in control. Group difference: 0.8 (95% CI –0.6 to 2.2). Sackley C. et al. 2006. Stroke, 37(9):2336-41. Meta-analysis: OT on personal activities of daily living Standard mean difference (random) (95% Cl) 0.27 (-0.16 to 0.70) 0.17 (-0.18 to 0.53) 0.33 (-0.21 to 0.88) 0.10 (-0.66 to 0.86) 0.14 (-0.30 to 0.57) 0.38 (0.07 to 0.69) 0.40 (0.00 to 0.80) -0.08 (-0.31 to 0.15) Study Corr 1995 Gilbertson 2000 Chiu 2004 Walker 1996 Logan 1997 Walker 1999 Sackley 2006 Parker 2001 Total (95% Cl) 0.18 (0.04 to 0.32) -1 -0.5 Favours control 0 1 0.5 Favours treatment Test for heterogeneity: x2=8.08, df=7, P=0.33, /2=13.3% Test for overall effect: z=2.45, P=0.01 Legg L.et al. 2007. BMJ, 335(7626):922. OTCH Phase III Cluster RCT Care-home setting: Birmingham, Bangor, Portsmouth, Nottingham, Central Lancashire, Peninsula, West Midlands (n=228) Participants: 1042 care home residents with a history of stroke or TIA Exclusion: Care home residents receiving end of life care. Inclusive: Includes those with communication and cognitive impairments. Primary outcome and timepoint: Independent assessment of Barthel @ 3 months. Secondary outcomes : Barthel @ 6 & 12 months. Rivermead Mobility, Depression (GDS-15), Quality of Life (EQ-5D). Analysis: Intention to treat Economic evaluation: Social perspective Randomised (228 homes, 1042 participants) Allocated to Occupational therapy Allocated to Control 114 homes, average size= 5, 568 participants 114 homes, average size= 4·2, 474 participants Received allocation= 545 Did not receive allocation = 23 Reasons: 16 died, 7 withdrawals Received allocation= 458 Did not receive allocation = 16 Reasons: 15 died, 1 withdrawal 3 month assessment= 491 (96% retention) 3 month assessment= 416 ( 93% retention) Primary outcome completed = 479 (113 care homes) 3 incomplete, 9 missing, 48 died, 1 withdrawal, 3 ineligible, 2 lost to follow-up Primary outcome completed= 391 (111 care homes) 12 incomplete, 13 missing, 37 died, 1 ineligible, 4 lost to follow-up 6 month assessment= 446 6 month assessment= 380 (90% retention) (90% retention) Primary outcome completed = 424 (111 care homes) 7 incomplete, 15 missing, 41 died, 4 withdrawals 4 lost to follow-up Primary outcome completed= 369 (109 care homes) 2 incomplete, 9 missing, 33 died, 3 withdrawals, 4 lost to follow-up 12 month assessment= 386 (84% retention) 12 month assessment= 306 (83% retention) Primary outcome completed= 355 (104 care homes) 14 incomplete, 17 missing, 54 died, 3 withdrawals, 3 lost to follow-up Primary outcome completed= 285 (100 care homes) 7 incomplete, 14 missing, 64 died, 5 withdrawals, 5 lost to follow-up Interventions 1 Interventions: Short term (3 month) targeted OT to improve mobility & self-care independence • Information, advice & caregiver training • Activity & mobility training Interventions 2 Interventions: Short term (3 month) targeted OT to improve mobility & self-care independence • Assistive devices & adaptations • Wheelchairs & seating reviewed Control: Standard care (not a lot) Summary of OTCH Intervention Framework • Employed a patient-centred goal-setting approach • Treatment regime developed using consensus professional opinion • 3-month intervention to improve mobility & self-care independence • Staff training was a key component. • Six Categories: - Assessment, Reassessment and Goal Planning - Communication - ADL training - Transfers and mobility (including wheelchairs) - Adaptive equipment (including seating) - Other (such as treating impairments) Barthel Index at Baseline Randomisation arm Barthel Index [0-20] Occupational therapy Control Very Severe [0-4] 268 (47.7%) 234 (50.1%) Severe [5-9] 129 (23.0%) 104 (22.3%) Moderate [10-14] 91 (16.2%) 76 (16.3%) Mild [15-19] 64 (11.4%) 46 (9.9%) Independent [20] 10 (1.8%) 7 (1.5%) 562 467 Total Additional Participant Characteristics at Baseline Intervention mean (sd) n Control mean (sd) n Sheffield [0 – 20] impaired [<15] 10.9 (7.1) 424 (58%) 11.9 (6.9) 374 (57%) MMSE [0-30 ] cognitive impairment [0-20] 13.6 (9.5) 398 (70%) 13.2 (9.0) 362 (73%) Barthel [0-20] 6.5 (5.8) 562 6.3 (5.7) 467 Rivermead [0-15] 3.1 (3.8) 557 2.8 (3.7) 456 GDS [0-15] 6.8 (3.9) 498 6.4 (3.5) 415 EQ-5D (3L) 0.20 (0.38) 506 0.24 (0.36) 423 Therapy Time Distribution • Visits = 2538 to N= 498 residents • Mean = 5.1 (SD 3.04) visits/resident • Median Duration = 30mins (IQR 15-60) • Six Categories: - Assessment and Goal Planning: - Communication: - ADL training: - Transfers and mobility : - Adaptive equipment : - Other : 23% 49% 7% 8% 7% 6% Primary & Secondary Outcomes @ 3 months Randomisation arm Occupational Control Therapy Adj n Adj n mean* mean* (se) (se) Barthel Rivermead GDS-15 EQ-5D 5.47 (0.20) 539 2.74 (0.11) 465 6.09 (0.21) 383 0.24 (0.02) 409 5.29 (0.21) 436 2.73 (0.12) 382 6.30 (0.22) 324 0.23 (0.02) 338 ICC Difference in adjusted means (95% CI) P value 0.09 0.19 0.48 (-0.33 to 0.70) 0.04 0.02 0.90 0.07 (-0.28 to 0.31) -0.21 0.44 0.06 (-0.76 to 0.33) 0.01 0.65 (-0.04 to 0.06) Process Evaluation Summary • Embedded process evaluation to develop an explanatory account of how the intervention was implemented within the trial. • Interviews with trial therapists and critical incidents. • Four overarching mechanisms which characterised implementation: (1) Balancing research and professional requirements, (2) Building rapport with care home staff, (3) Re-engineering the personal environments of care home patients, (4) Therapists’ learning about the intervention and its impacts over time. • How these mechanisms operated was contingent on multiple factors such as the prior experience of therapists, and the contexts characterising the care homes included in the trial. • Masterson-Algar , et al. Journal of Evaluation and Clinical Practice, submitted. Health Economics Summary • The intervention costs more than the NICE cost-effectiveness threshold of £20,000/QALY across all analyses. • Significant difference in cost /QALY between participants in nursing homes (£63k/QALY) compared with residential care (£28k/QALY). • Based on current cost-effectiveness thresholds, we would not endorse the OTCH programme. Summary • Neutral findings are deemed as robust . • Participant baseline characteristics were representative of the UK care home population, in regards to age, gender balance, levels of frailty and support needed. • The OT treatment offered to participants was similar to an NHS intervention, indicated by the OTCH process evaluation. • The evidence does not support the use of an OT package to increase or maintain abilities in personal activities of daily living, for an older care home population with stroke-related disabilities. Conclusions • These neutral findings are similar to those reported in other recently reported RCTs conducted in a care-home population (Underwood et al, 2013; Kerse et al, 2008). • These studies assessed the influence of exercise on depression ratings using the GDS, and the influence of functional activity on quality of life / frequency of falls. • Both trials reported either a neutral or a minimal effect, mediated by levels of cognitive impairment. • What are the next steps for research in this clinically complex population with high incidence of depression, cognitive and physical impairment? OT Intervention with John Some of the ‘perks’ of being involved in stroke research… John was interviewed by local TV news and enjoyed his 15 minutes of fame! OT Intervention with John Some of the ‘perks’ of being involved in stroke research… John met HRH Princess Anne when she visited the research unit OT Intervention with John Some of the ‘perks’ of being involved in stroke research… Notts County FC acknowledged his support with a lifetime season ticket and merchandise Acknowledgements