Development of diabetic retinopathy
management guidelines for implementation
in low-resource settings.
Dr Rahul Chakrabarti
IAPB 9th General assembly,
19th September, 2012
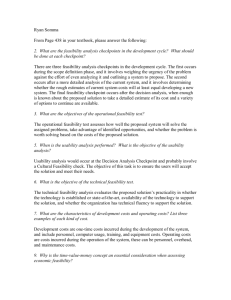
Methods
• Published guidelines (n=32)
Multi-database • Satisfying inclusion criteria (n=11)
search
Inclusion
criteria
• Epidemiology
• Stages of DR
• Detection
• Management
• Evidence-based recommendations
• Developed by panel of experts
• English-language
Update
evidence
Face-Validity
Feasibility
Issues
• Lack of agreement in recommendations
• Health systems and resource limitations
• Age of evidence
Implement
• Literature review
• Draft guidelines
• Review of guidelines by expert panel of
retinal specialists
• Feasibility for implementation in lowresource countries
• Case study methodology
• Implementing guidelines in a low-resource
setting
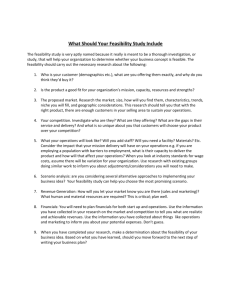
Screening for DR
Guideline
Screening method
NICE (2005)
45 degree mydriatic photography
12-18 months
NHMRC (2008)
Dilated ophthalmoscopy
Non-mydriatic photography if not
available
24 months
WHO (2005)
Dilated two field photography
12 months
AAO (2008)
Slit-lamp biomicroscopy
12 months
Evidence
Single field 45°, non-mydriatic
image is adequate to detect
‘referable’ retinopathy
24 months
Further details on Poster #73
Examination interval: Patients
with Diabetes, without baseline
DR
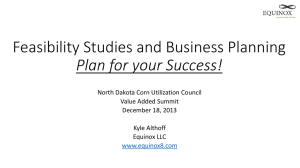
Framework to assess
Feasibility of Guidelines
Feasibility
Health services
Governance
Health workforce
Technology and
equipment
Financing
Linkages
Adopting
Guidelines
Cadre
Affordability
Government
Education
Local
responsibility
Distribution
Access
NGO
Capacity
Quality assurance
Task-shift
Training
Local govt
Other
Acknowledgement
• PhD supervisors:
Professor Jill Keeffe, Dr Alex Harper
•
This research is being supported by the University of Melbourne Australian Postgraduate Award,
Riady Scholarship, and M.A. Bartlett Research Fund.
•
CERA receives Operational Infrastructure Support from the State Government of Victoria.
 0
0