Health Improvement Plan of Bangladesh
advertisement

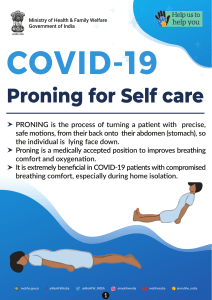
Health Financing in Bangladesh Dr. Mohammad Khairul Hasan Deputy Chief , Planning Wing MOHFW Date: 18.02.2014 Introduction • Government of Bangladesh (GOB) has constitutional obligation to ensure public health to all citizens. • GOB is committed to achieve health related MDGs, vision 2021 goals, etc. • Health, population and nutrition are among the most urgent development agenda of the Government of Bangladesh (GOB). 2 SALARY GOB OTHER RECURRENT NON -DEV 32 OPS HPNSDP 22 PROJECT DEVELOPMENT Source EXPENDITURE DP MOF ALLOCATION TO MOHFW MTBF ADP PC Health Expenditure & Financing Features • Per capita health expenditure US$16 (2007), $27 (2011). • Total health expenditure (THE) as % of GDP 3.4% Health Expenditure & Financing Features 10% 26% Public Health Expenditure Out of Pocket Expenditure 64% Direct External Funding , Private, NGOs & Others Trend of MOHFW Budget (5 years) Budget Year NonDevelopment (Taka in Crore) Development Total 2009-10 3925.36 3075.00 7000.36 2010-11 4676.00 3472.92 8148.92 2011-12 5327.00 3561.75 8888.75 2012-13 5529.62 3825.39 9355.01 2013-14 58,93.00 3602.00 9495.00 10000 8888.75 9000 8148.92 8000 7000.36 7000 4000 5529.62 5327.00 6000 5000 9495.00 9355.01 5893.00 4676.00 3925.36 3075.00 3472.92 3561.75 3825.39 3602.00 3000 2000 1000 0 2009-10 2010-11 Non Development 2011-12 2012-13 2013-14 Development Total MOHFW Budget Compared to National Budget (Five years) Year National Budget (Taka in Corer) MOHFW Budget (Taka in Crore) (%) 2009-10 1,13,819 7000.36 6.17% 2010-11 1,32,170 8148.92 6.17% 2011-12 1,63,589 8888.75 5.43% 2012-13 1,91,738 9355.01 4.88% 2013-14 2,22,491 9495.00 4.27% Trend of GOB Health Budget Allocation • Share of MOHFW budget as percentage of GDP decreased gradually from 1.01% in FY 2009-10 to 0.91% in FY 2012-13. Whereas it was 0.7% in Pakistan, 1.2% in India and 2.1% in Nepal as per 2011. • In absolute term MOHFW budget increased to 9495.00 crore in 2013-14 from 7000.00 crore in 200910, an increase of about 36% over 4 years. • Over the last 4 years national budget increased from 1,13,819 crore to 2,22,491 core about 95% • Compared to national budget , share of MOHFW budget decreased to 4.27% from 6.17% for the same period. • WHO suggests that health budget should be at least 15% of the national budget for developing countries. Comparison National and MOHFW Budget (%) 250000 222491 7.00% 191738 200000 6.00% 163589 150000 5.00% 132170 113819 3.00% 2.00% 50000 8148.92 8888.75 9355.01 9495 0 1.00% 0.00% 2009-10 5.43% 4.88% 4.27% 4.00% 100000 7000.36 6.17% 6.17% 2010-11 National Budget 2011-12 2012-13 2013-14 MOHFW Budget (%) Current Health Budget Expenditure Pattern • MTBF is the budget projection instrument for financing both non-development and development budget. • Almost 90% MOHFW’s non-development budget is spent for the salary of personnel (60%), MSR and recurrent expenditure. Current Health Budget Expenditure Pattern • Development budget is use to fund MOHFW’s development related activities for accelerated achievement in health related MDGs by 2015, 6th Five Year Plan and vision 2021 targets. • MOHFW is implementing 3rd SWAp called Health, Population and Nutrition Sector Development Program (HPNSDP) for 2011-16 along with some parallel projects (now 22) included in the ADP. Source of Health Budget – Major portion of the health budget (Non-development and Development together) being provided by GOB . – Total estimated cost of HPNSDP (2011-16) is Tk. 56,993.00 crore (about US$ 7.7 billion). Of this GOB contribution is Tk. 43,420.00 crore (76%) and DP contribution is Tk. 13,573.00 crore (24%). – Development budget requirement of HPNSDP estimated through 32 OPs is Tk. 22,177.00 crore ( 39% of total cost of HPNSDP) 24% 76% GOB DP Development Budget gap of HPNSDP (Taka in crore) Financial Year Estimated PIP budget of HPNSDP Allocation given by the MTBF budget for HPNSDP Funding gap/Difference 2011-12 2012-13 2013-14 2014-15 3786.00 5007.00 5140.00 4000.00 3040.55 2832.28 2877.61 3378.00 -745.45 -2174.72 -2262.39 -622.00 2015-16 4243.00 -527.20 Total 22176.00 3715.80 (provisional) 15844.24 -6331.76 (29%) 25000 20000 15000 10000 5000 0 2011-12 2012-13 2013-14 2014-15 2015-16 Total -5000 -6331.76 -10000 Estimated PIP budget of HPNSDP Allocation given by the MTBF budget for HPNSDP Funding gap/Difference RFW of HPNSDP & Current Status BASELINE UPDATE 2013 TARGET 2016 Infant mortality rate (IMR) 52 BDHS 2007 43 BDHS 2011 31 Challenges Under 5 mortality rate 65 BDHS 2007 53 BDHS 2011 48 On track Neonatal mortality rate 37 BDHS 2007 32 BDHS 2011 21 Challenges Maternal mortality ratio 194 BMMS 2010 194 BMMS 2010 ≤143 Challenges Total fertility rate (TFR) 2.7 BDHS 2007 2.3 BDHS 2011 2.00 Challenges Prevalence of stunting among children under 5 years of age 43.2% BDHS 2007 38.7% UESD 2013 38% On track Prevalence of underweight among children under 5 years of age 41.0% BDHS 2007 35.1% UESD 2013 33% On track <1% SS 2007 <1% SS 2011 <1% On track INDICATOR Prevalence of HIV in MARP Challenges of Health Sector Funding • Per capita health spending ($27 ) is very low compared to most South Asian countries (India$59, Sri Lanka-$97, Nepal-$33) while WHO recommends for $54 per capita spending for a fully functioning health system-Inadequacy /Accessibility concern. • Out of pocket expenditure is very high (64%), against the global status of 32%.-Equity concern. • HPNSDP has already faced a financing gap of Tk. 5’182.56 crore in the last 3 years of implementation. Trend shows there will remain about Tk. 6,332.00 crore at the end of the program in 2016. • Budget deficit will make it difficult to achieve some RFW Indicators of HPNSDP- Low level of public spending. Additional Resources Mobilization Prospect • GOB Mid Term Budgetary Framework (MTBF) based on revenue income (tax, non-tax and other sources) of GOBmoderate prospect - Increase user fees and its retention by MOHFW - Increase sin tax, e.g., tax on cigarettes and narcotics and allocate MOHFW - Competition with other Ministries for increased allocation in the context of differential priorities of GOB (e.g., for infrastructure, electricity, education, etc) - Efficiency in budget utilization by MOHFW and it’s Directorates. Additional Resources mobilization • Donor financing- low prospect of substantial increase : - Integrating DP parallel funded program into MOHFW planning and budgeting process. -`Potential window of Global Fund (GAVI, GFATM, etc.). • Public Private Partnership (PPP)-low prospect - Since introduction of PPP Policy MOHFW has been able to process only one project (Kidney dialysis). - Encourage multi and national companies to support health sector as part of Corporate Social Responsibilities Additional Resources mobilization Prospect (cont.) • Social health insurance-moderate prospect - Premium based pre-paid health insurance scheme can be introduced gradually beginning with formal sector. Then go for informal sector and others. • Local Govt. institutions/Municipalities/Upazila Parishad etc. - Can provide health budget through LLP & other mechanism. Issues of concern before introducing health insurance for UHC Before introducing social insurance widely following are the essential elements to make the health system ready: • Regulate volatile private health sector in terms of quality and pricing of services. • Develop service standardization model and introduce fixed fee schedule of services across the health facilities ( both public & private). • Both public and private health facilities should have same quality of services and fixed pricing schedule of services with accreditation and monitoring mechanism. • Adjustment of MTBF budget allocation between non-development and development parts to make some room for the copayment of health insurance premium for the poor and to make efficient use of resources. Way forward • For achieving universal health coverage in the long run both accelerated HPN service delivery through SWAp (mainly for primary HPN care) and financing through social health insurance scheme (for curative and specialized care except EOC) may work together. • SWAp/HPNSDP is the instrument to provide primary HPN services and continue uninterrupted services at all public health and FP facilities (esp. outpatient services regarded as pro-poor) in order to achieve MDG and other national goals. • Continuation of health Safety net programs like Demand side financing (DSF) Maternal health voucher scheme, Community Clinic approach, Nutrition services etc. Thank You