THE PERIPHERAL NERVOUS SYSTEM
advertisement

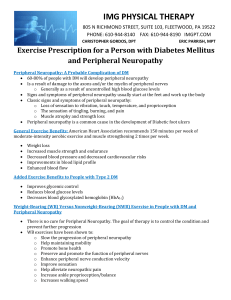
مرحبا بالحضور الكرام بسم هللا الرحمن الرحيم وما أوتيتم من ألعلم إال ق ليال• صدق اهلل العظيم • Peripheral Neuropathy In Dyslipidemia with special Emphasis on diabetes mellitus (Biochemical & Electrophysiological study) Peripheral neuropathy • Def: PNP is a generic term for peripheral nerve disorders of any cause. • Mononeuropathy refers to involvement of a single nerve whereas polyneuropathy refers to involvement of multiple nerves. PNP in Dyslipidemia 1. dyslipidemia could be associated with subclinical peripheral neuropathy, which may occur more frequently in patients with very high mean serum level of T.G, T.C and LDL. 2. The type of peripheral neuropathy that occurs in Dyslipidemia is mainly a sensory type, although motor neuropathy can not be excluded. 3. The underlying mechanism is mixed axonal degeneration and segmental demyelination; however, the demyelination is thought to be secondary to the axonal degeneration. The peripheral neuropathy associated with dyslipidemia is symmetrical type. Pathogenesis of Peripheral Neuropathy in Dyslipidemia I. II. Involvement of structural lipids The action of lipoproteins as enzyme co-factor and as a bound intermediate in the biosynthesis of polysaccharides and proteins. III. Nerve infarction which is mediated via fat embolism or lipid induced platelet aggregation. Types of peripheral neuropathy in DM • PNP affect 30% of diabetic patients. • Diabetic neuropathy divided into: A. somatic: include: 1. polyneuropathy symmetrical (mainly sensory and distal) Asymmetrical (mainly motor and proximal) 2. Mononeuropathy (including mononeuritis multiplex) B. Visceral (autonomic) Pathogenesis of peripheral neuropathy in DM The pathogenesis of sensorimotor neuropathy in D.M is multifactorial and related metabolic disturbances, such as hyperglycemia, dyslipidemia, oxidative stress and growth factor deficiency all contribute to the development of this complication. Several metabolic products, such as: 1. Advanced glycated end products. 2. Activation of protein kinase C enzyme. 3. Sorbitol aldose reductase (polyol) pathway flux, are claimed to have a role in pathogenesis of neuropathy Dyslipidemia as a contributory factor in etiopathogenesis of diabetic neuropathy Dyslipidemia leads to high levels of oxLDLs that may injure DRG neurons via LOX-1 receptor and contribute to the development of diabetic neuropathy. Also these oxLDLs that carry lipids to the periphery could be one factor that acts in concert with glucose to increase sensory nerve injury. These same mechanisms also occur in the blood microvessels, leading to multiple neurovascular targets for oxidative stress mediated injury. Role of Electrophysiology in Dyslipidemia Neurological complications of dyslipidemia were firstly noticed in hereditary lipid disorders like Tangier disease, abetalipoprotienemia, later on many studies was carried out to disclose the relation between peripheral neuropathy and dyslipidemia, but in spite of all these studies the proportion of dyslipidemic patients with peripheral neuropathy is still unknown and based on literature review. ELECTROPHYSIOLOGICAL ASSESSMENT OF THE PERIPHERAL NERVOUS SYSTEM:Electrophysiological methods have made an important contribution in elucidating the pathophysiology of peripheral nerve disorders by ELECTRONEUROGRAPHY which include:A. SENSORY NERVE CONDUCTION. B. MOTOR NERVE CONDUCTION. C. F -WAVE CONDUCTION STUDY. PARAMETER DSL (msec) Subject N O. Rt. Median N. Mean ±S.D Rt. Ulnar N. Mean ± S.D Rt.Com.Per. N. Mean ± S.D Rt. Post.Tib. N. Mean ± S.D Patients 68 2.65 ± 0.58 2.44 ± 0.50 3.52± 0.88 3.60± 0.96 Control 42 2.44 ± 0.17 2.29 ± 0.16 3.05 ± 0.22 3.12 ± 0.27 P.value Amplitude (µv) (S) (H.S) (H.S) Patients 68 22.63 ±5.56 20.75±3.69 9.65± 2.97 9.92± 3.75 Control 42 25.25 ±2.24 22.04 ±1.71 11.07 ±1.37 11.66 ±1.81 P.value C.V (m/sec) (N.S) (H.S) (S) (H.S) (H.S) Patients 68 57.34 ±7.12 57.55 ±6.77 47.70±8.19 47.88±8.01 Control 42 59.67 ±3.07 59.41 ±3.44 51.48 ±4.55 51.61 ±3.97 (H.S) (H.S) P.value (S) (N.S) Patients with Abnormal Electrophysiologic Results PARAM ETER DSL (msec) SUBJECT N O. Rt.Median Rt.Ulnar Rt.Com. N. N. Per. N Mean ± S.D Mean ± S.D Mean ±S.D Rt.Post. Tib. N. Mean ± S.D Control 42 2.44 ± 0.17 2.29 ± 0.16 3.05± 0.22 3.12 ± 0.27 Affected 21 3.11 ± 0.84 2.79 ± 0.75 4.39 ± 1.06 4.73 ± 0.96 P.value AMPLIT Control UDE Affected (µv) P.value C.V (m/sec) (H.S) (H.S) (H.S) (H.S) 42 25.25 ±2.24 22.04±1.71 11.07 ±1.37 11.66 ±1.81 21 18.25 ±5.87 17.76±4.92 6.62 ± 3.23 5.96 ± 3.46 (H.S) (H.S) (H.S) (H.S) Control 42 59.67 ±3.07 59.4 ±3.44 51.48 ±4.55 51.61 ±3.97 Affected 21 51.45 ±9.58 54.0 ±8.56 39.19 ±7.25 38.85 ±6.91 P.value (H.S) (H.S) (H.S) (H.S) Recommendations Dyslipidemia is a causative factor for peripheral neuropathy, which stresses the importance of screening patients with peripheral neuropathy of unknown origin for dyslipidemia, as it is a potentially treatable condition. Electrophysiologically, we recommend to examine the patients, at first, for nerves of lower limbs, as they are usually the first to be affected. Starting with sensory fibers assessment and further tests are done according to these findings. Unilateral sensory nerve conduction study will be reasonably informative since the disease process found to affect both sides of the body equally. Examination of upper limbs mainly median nerve sensory conduction study will be supportive and helpful to see the degree of extension of the disease process. Motor nerve conduction study could be helpful and informative if the patients have abnormal sensory nerve conduction study. So further evaluation of patients by MNCS and F-wave conduction study is recommended. Thank you