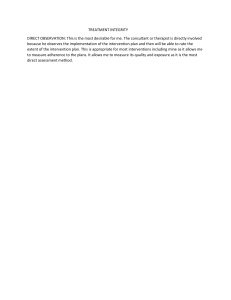
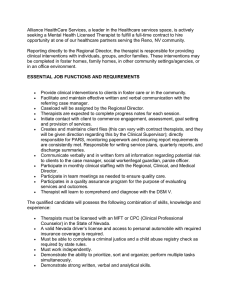
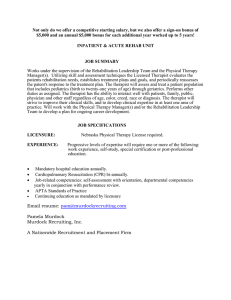
SECTION ONE Clinical Decision Making and Examination Clinical Decision Making Susan B. O’Sullivan, PT, EdD LEARNING OBJECTIVES CHAPTER OUTLINE 1. Define clinical reasoning and identify factors that affect clinical decision making. 2. Describe the key steps in the patient/client management process. 3. Define the major responsibilities of the physical therapist in planning effective treatments. 4. Identify potential problems that could adversely affect the physical therapist’s clinical reasoning. 5. Discuss strategies to ensure patient participation in the plan of care (POC). 6. Identify key elements of physical therapy documentation. 7. Differentiate between the clinical decision making approaches used by the expert versus novice physical therapist. 8. Discuss the importance of evidencebased practice in developing the POC. 9. Analyze and interpret patient/client data, formulate realistic goals and outcomes, and develop a POC when presented with a clinical case study. CLINICAL REASONING/CLINICAL DECISION MAKING 1 INTERNATIONAL CLASSIFICATION OF FUNCTIONING, DISABILITY, AND HEALTH (ICF) 2 PATIENT/CLIENT MANAGEMENT 3 Examination 3 Evaluation 7 Diagnosis 8 Prognosis 9 Plan of Care 9 Discharge Planning 13 Implementation of the Plan of Care 13 Reexamination of the Patient and Evaluation of Expected Outcomes 14 ■ CLINICAL REASONING/ CLINICAL DECISION MAKING Clinical reasoning is a multidimensional process that involves a wide range of cognitive skills physical therapists use to process information, reach decisions, and determine actions. Reasoning can be viewed as an internal Chapter 1 PATIENT PARTICIPATION IN PLANNING 15 DOCUMENTATION 16 Electronic Documentation 16 CLINICAL DECISION MAKING: EXPERT VERSUS NOVICE 16 EVIDENCE-BASED PRACTICE 17 SUMMARY 20 dialogue that therapists continuously employ while meeting the challenges of clinical practice. Clinical decisions are the outcomes of the clinical reasoning process and form the basis of patient/client management. A number of factors influence decision making, including the clinician’s goals, values and beliefs, psychosocial 1 2 SECTION I Clinical Decision Making and Examination skills, knowledge base and expertise, problem-solving strategies, and procedural skills. Many of these factors are the focus of discussion in later chapters in this text. Decision making is also influenced by patient/client characteristics (goals, values and beliefs, and physical, psychosocial, educational, and cultural factors) as well as environmental factors (clinical practice environment, overall resources, time, level of financial support, level of social support). Decision making frameworks, such as algorithms, have been developed by experienced practitioners to guide clinicians in their reasoning processes. For example, Rothstein and Echternach developed the HypothesisOriented Algorithm for Clinicians II (HOAC).1 An algorithm is a graphically represented step-by-step guide designed to assist clinicians in problem solving by considering several possible solutions. It is based on specific clinical problems and identifies the decision steps and possible choices for remediation of a problem. A series of questions are posed, typically in yes/no format, addressing whether the measurements met testing criteria, the hypotheses generated were viable, goals were met, strategies were appropriate, and tactics were implemented correctly. Hypotheses are defined as the underlying reasons for the patient’s problems, representing the therapist’s conjecture as to the cause. Problems are defined in terms of activity limitations. A “no” response to any of the questions posed in an algorithm is an indication for reevaluation of the viability of the hypotheses generated and reconsideration of the decisions made. In using HOAC II as a model for clinical decision making, the therapist also distinguishes between existing problems and anticipated problems, defined as deficits that are likely to occur if an intervention is not used for prevention. The value of an algorithm is that it guides the therapist’s decisions and provides an outline of the decisions made. See Chapter 17, Figures 17.7 and 17.8, for examples of problemcentered algorithms. Physical therapists today practice in complex environments and are called upon to reach increasingly complex decisions under significant practice constraints. For example, a therapist may be required to determine a POC for the complicated patient with multiple co-morbidities within 72 hours of admission to a rehabilitation facility. Reduced levels of treatment authorization with shorter and shorter stays in rehabilitation also complicate the decision making process. Novice practitioners can easily become overwhelmed. This chapter introduces a framework for clinical decision making and patient/client management that can assist in organizing and prioritizing data and in planning effective treatments compatible with the needs and goals of the patient/client and members of the health care team. ■ INTERNATIONAL CLASSIFICATION OF FUNCTIONING, DISABILITY, AND HEALTH (ICF) The World Health Organization’s (WHO’s) International Classification of Functioning, Disability, and Health (ICF) model provides an important framework of terminology for understanding and categorizing health conditions and patient problems by clearly defining health condition, impairment, activity limitation, and participation restriction.2 The American Physical Therapy Association (APT) has joined the WHO, the World Confederation for Physical Therapy (WCPT), the American Therapeutic Recreation Association (ATRA), and other international professional organizations in endorsing the ICF classification. Figure 1.1 presents the ICF model of disability. Impairments are the problems an individual may have in body function (physiological functions of body systems) or structure (anatomical parts of the body). The resulting significant deviation or loss is the direct result of the health condition, a disease, disorder, injury, or trauma, or other circumstance, such as aging, stress, congenital anomaly, or genetic predisposition. For example, a patient with stroke may present with sensory loss, paresis, dyspraxia, and hemianopsia (direct impairments). Impairments may be mild, moderate, severe, or complete and may be permanent or resolving as recovery progresses. Impairments may also be indirect (secondary), the sequelae or complications that Health condition (disorder or disease) Body Functions and Structure Participation Activity Environmental Factors Personal Factors Contextual factors Figure 1.1 ICF Model of Disability. The WHO classification of functioning, disability and health (ICF). World Health Organization. ICF: International Classification of Functioning, Disability, and Health. 2002. Geneva, Switzerland, p 18, with permission. (Form for request for permission available at www.who.int/about/licensing/copyright_ form/en/index.html.) CHAPTER 1 originate from other systems. They can result from preexisting impairments or the expanding multisystem dysfunction that occurs with prolonged bedrest and inactivity, an ineffective POC, or lack of rehabilitation intervention. Examples of indirect impairments include decreased vital capacity and endurance, disuse atrophy and weakness, contractures, decubitus ulcers, deep venous thrombosis, renal calculi, urinary tract infections, pneumonia, and depression. The term composite impairment refers to impairments that are the result of multiple underlying origins, the combined effects of both direct and indirect impairments (e.g., balance deficits, gait deficits). Activity limitations are difficulties an individual may have in executing tasks or actions. Activity limitations can include limitations in the performance of cognitive and learning skills, communication skills, functional mobility skills (FMS) (such as transfers, walking, lifting or carrying objects), and activities of daily living (ADL). Basic activities of daily living (BADL) include self-care activities of toileting, hygiene, bathing, dressing, eating, drinking, and social (interpersonal) interactions. The person with stroke may demonstrate difficulties in all of the above areas and be unable to perform the actions, tasks, and activities that constitute the “usual activities” for this individual. Participation restrictions are problems an individual may experience in involvement in life situations and societal interactions. Categories of life roles include home management, work (job/school/play), and community/ leisure. These include instrumental activities of daily living (IADL) such as housecleaning, preparing meals, shopping, telephoning, and managing finances, as well as work and leisure activities (e.g., sports, recreation, trips). Thus, the individual with stroke is unable to resume societal roles such as working, parenting, attending church, or traveling. Performance qualifiers indicate the extent of participation restriction (difficulty) in performing tasks or actions in an individual’s current real-life environment. All aspects of the physical, social, and attitudinal world constitute the environment. Difficulty can range from mild to moderate to severe or complete. Capacity qualifiers indicate the extent of activity limitation and are used to describe an individual’s highest probable level of functioning (ability to do the task or action). Qualifiers can range from the assistance of a device (e.g., adaptive equipment) or another person (minimal to moderate to maximal assistance) or environmental modification (home, workplace). Thus, the patient with stroke may demonstrate moderate difficulty in locomotion in the home environment (performance qualifiers) and require the use of an ankle-foot orthosis, small-based quad cane, and moderate assistance of one (capacity qualifiers). Environmental factors make up the physical, social, and attitudinal environment in which people live and Clinical Decision Making 3 function. Factors range from products and technology (for personal use in daily living, mobility and transportation, communication) and physical factors (home environment, terrain, climate) to social support and relationships (family, friends, personal care providers), attitudes (individual and societal), and institutions and laws (housing, communication, transportation, legal, financial services, and policies). Qualifiers include factors that serve as barriers (disablement risk factors) or facilitators (assets). Barriers can range from mild to moderate to severe to complete. Facilitators can also range from mild to moderate to substantial to complete. Box 1.1 summarizes ICF disablement terminology. The ICF Checklist (Version 2.1a, Clinician Form for the International Classification of Functioning, Disability, and Health) is a practical tool to elicit and record information on functioning and disability of an individual.3 ■ PATIENT/CLIENT MANAGEMENT Steps in patient/client management include (1) examination of the patient; (2) evaluation of the data and identification of problems; (3) determination of the physical therapy diagnosis; (4) determination of the prognosis and POC; (5) implementation of the POC; and (6) reexamination of the patient and evaluation of treatment outcomes (Fig. 1.2).4 Examination Examination involves identifying and defining the patient’s problem(s) and the resources available to determine appropriate intervention. It consists of three components: the patient history, systems review, and tests and measures. Examination begins with patient referral or initial entry (direct access) and continues as an ongoing process throughout the episode of care. Ongoing reexamination allows the therapist to evaluate progress and modify interventions as appropriate. History Information about the patient’s past history and current health status is obtained from review of the medical record and interviews (patient, family, caregivers). The medical record provides detailed reports from members of the health care team; processing these reports requires an understanding of disease and injury, medical terminology, differential diagnosis, laboratory and other diagnostic tests, and medical management. The use of resource material or professional consultation can assist the novice clinician. The types of data that may be generated from a patient history are presented in Figure 1.3.4 The interview is an important tool used to obtain information and gain understanding directly from the patient. The therapist asks the patient a series of questions regarding general health, past and present medical conditions/complications, and treatment. Specifically 4 SECTION I Box 1.1 Clinical Decision Making and Examination Terminology: Functioning, Disability, and Health Health condition is an umbrella term for disease, disorder, injury, or trauma and may also include other circumstances, such as aging, stress, congenital anomaly, or genetic predisposition. It may also include information about pathogeneses and/or etiology. Body functions are physiological functions of body systems (including psychological functions). Body structures are anatomical parts of the body such as organs, limbs, and their components. Impairments are problems in body function or structure such as a significant deviation or loss. Activity is the execution of a task or action by an individual. Activity limitations are difficulties an individual may have in executing activities. Participation is involvement in a life situation. Participation restrictions are problems an individual may experience in involvement in life situations. Contextual factors represent the entire background of an individual’s life and living situation. • Environmental factors make up the physical, social, and attitudinal environment in which people live and conduct their lives, including social attitudes, architectural characteristics, and legal and social structures. • Personal factors are the particular background of an individual’s life, including gender, age, coping styles, social background, education, profession, past and current experience, overall behavior pattern, character, and other factors that influence how disability is experienced by an individual. Performance qualifier describes what an individual does in his or her current environment. (The current environment includes assistive devices or personal assistance, whenever the individual uses them to perform actions or tasks.) Capacity qualifier describes an individual’s ability to execute a task or an action (highest probable level of functioning in a given domain at a given moment). From World Health Organization (WHO): International Classification of Functioning, Disability and Health (ICF).3 the patient is asked to describe the current problems, primary complaint (reason for seeking physical therapy), and anticipated goals/expected outcomes for the episode of care. The patient will often describe his or her difficulties in terms of activity limitations or participation restrictions (what he or she can or cannot do). The patient is then asked a series of questions designed to explore the nature and history of the current problems/ primary complaint. General questions about functional activities and participation should be directed toward delineating the difference between capacity and performance. For example, “Since your stroke, how much difficulty do you have walking long distances?” “How does this compare to before you had the stroke?” (capacity). Questions directed toward examining performance can include “How much of a problem do you have in walking long distances?” “Is this problem with walking made worse or better with the use of an assistive device?” Questions are also posed regarding the patient’s social and physical environment, vocation, recreational interests, health habits (e.g., smoking history, alcohol use), exercise likes and dislikes, and frequency and intensity of regular activity. Sample interview questions are included in Box 1.2.4, 5 Pertinent information can also be obtained from the patient’s family or caregiver. For example, patients with central nervous system (CNS) involvement and severe cognitive and/or communication impairments and younger pediatric patients will be unable to accurately communicate their existing problems. The family member/caregiver then assumes the primary role of assisting the therapist in identifying problems and providing relevant aspects of the history. The perceived needs of the family member or caregiver can also be determined during the interview. The therapist should be sensitive to differences in culture and ethnicity that may influence how the patient or family member responds during the interview or examination process. Different beliefs and attitudes toward health care may influence how cooperative the patient will be. During the interview, the therapist should listen carefully to what the patient says. The patient should be observed for any physical manifestations that reveal emotional context, such as slumped body posture, grimacing, and poor eye contact. Finally, the interview is used to establish rapport, effective communication, and mutual trust. Ensuring effective communication with the patient and cooperation serves to make the therapist’s observations more valid and becomes crucial to the success of the POC. Systems Review The use of a brief screening examination allows the therapist to quickly scan the patient’s body systems and determine areas of intact function and dysfunction in each of the following systems: cardiovascular/pulmonary, integumentary, musculoskeletal, and neuromuscular. Information is also obtained about cognitive functions, communication, learning style, and emotional status. Areas of deficit together with an accurate knowledge of the main health condition (disorder or disease) (1) confirm the need for further or more detailed examination; (2) rule out or differentiate specific system involvement; (3) determine if referral to another health care professional is warranted (triage); and (4) focus CHAPTER 1 DIAGNOSIS Both the process and the end result of evaluating examination data, which the physical therapist organizes into defined clusters, syndromes, or categories to help determine the prognosis (including the plan of care) and the most appropriate intervention strategies. EVALUATION A dynamic process in which the physical therapist makes clinical judgments based on data gathered during the examination. This process also may identify possible problems that require consultation with or referral to another provider. EXAMINATION The process of obtaining a history, performing a systems review, and selecting and administering tests and measures to gather data about the patient/client. The initial examination is a comprehensive screening and specific testing process that leads to a diagnostic classification. The examination process also may identify possible problems that require consultation with or referral to another provider. OUTCOMES Results of patient/client management, which include the impact of physical therapy interventions in the following domains: pathology/pathophysiology (disease, disorder, or condition); impairments, functional limitations, and disabilities; risk reduction/prevention; health, wellness, and fitness; societal resources; and patient/client satisfaction. Clinical Decision Making 5 PROGNOSIS (Including Plan of Care) Determination of the level of optimal improvement that may be attained through intervention and the amount of time required to reach that level. The plan of care specifies the interventions to be used and their timing and frequency. INTERVENTION Purposeful and skilled interaction of the physical therapist with the patient/client and, if appropriate, with other individuals involved in care of the patient/client, using various physical therapy methods and techniques to produce changes in the condition that are consistent with the diagnosis and prognosis. The physical therapist conducts a reexamination to determine changes in patient/client status and to modify or redirect intervention. The decision to reexamine may be based on new clinical findings or on lack of patient/client progress. The process of reexamination also may identify the need for consultation with or referral to another provider. Figure 1.2 Elements of patient management leading to optimal outcomes. (From APTA Guide to Physical Therapist Practice 4, p. 35 with permission.) the search of the origin of symptoms to a specific location or body part. An important starting point for identification of areas to be screened is consideration of all potential (possible) factors contributing to an observed activity limitation or participation restriction. Consultation is appropriate if the needs of the patient/client are outside the scope of the expertise of the therapist assigned to the case. For example, a patient recovering from stroke is referred to a dysphagia clinic for a detailed examination of swallowing function by a dysphagia specialist (speech-language pathologist). Screening examinations are also used for healthy populations. For example, the physical therapist can screen individuals to identify risk factors for disease such as decreased activity levels, stress, and obesity. Screening is also conducted for specific populations such as pediatric clients (e.g., for scoliosis), geriatric clients (e.g., to identify fall risk factors), athletes (e.g., in pre-performance examinations), and working adults (e.g., to identify the risk of musculoskeletal injuries in the workplace). These screens may involve observation, chart review, oral history, and/or a brief examination. Additional screening examinations may be mandated by institutional settings. For example, in a long-term care facility, the therapist may be asked to review the chart for indications of changes in functional status or need for physical therapy. The therapist then makes a determination of the need for further physical therapy services based on completing a screening examination. Tests and Measures More definitive tests and measures are used to provide objective data to accurately determine the degree of specific function and dysfunction. Examination begins at the level of impairments, for example, diminished muscle strength (manual muscle test [MMT]) and impaired range of motion (ROM) (goniometric measurements), and progresses to functional activities (6-minute Walk Test, Timed Up and Go, Berg Balance Test). Alternatively, 6 SECTION I Clinical Decision Making and Examination General Demographics • Age • Sex • Race/ethnicity • Primary language • Education Social History • Cultural beliefs and behaviors • Family and caregiver resources • Social interactions, social activities, and support system Employment/Work (Job/School/Play) • Current and prior work (job/school/play), community, and leisure actions, tasks, or activities Growth and Development • Developmental history • Hand dominance Living Environment • Devices and equipment (eg., assistive, adaptive, orthotic, protective, supportive, prosthetic) • Living environment and community characteristics • Projected discharge destinations General Health Status (Self-Report, Family Report, Caregiver Report) • General health perception • Physical function (eg., mobility, sleep patterns, restricted bed days) • Psychological function (eg., memory, reasoning ability, depression, anxiety) • Role function (eg., community, leisure, social, work) • Social function (eg., social activity, social interaction, social support) Social/Health Habits (Past and Current) • General health perception • Physical function (eg., mobility, sleep patterns, restricted bed days) • Psychological function (eg., memory, reasoning ability, depression, anxiety) • Role function (eg., community, leisure, social, work) • Social function (eg., social activity, social interaction, social support) Family History • Familial health risks Medical/Surgical History • Cardiovascular • Endocrine/metabolic • Gastrointestinal • Genitourinary • Gynecological • Integumentary • Musculoskeletal • Neuromuscular • Obstetrical • Prior hospitalizations, surgeries, and preexisting medical and other health related conditions • Psychological • Pulmonary Current Condtion(s)/ Chief Complaint(s) • Concerns that led the patient/client to seek the services of a physical therapist • Concerns or needs of patient/client who requires the services of a physical therapist • Current therapeutic interventions • Mechanisms of injury or disease, including date of onset and course of events • Onset and patterns of symptoms • Patient/client, family, significant other, and caregiver expectations and goals for the therapeutic intervention • Previous occurrence of chief complaint(s) • Prior therapeutic interventions Functional Status and Activity Level • Current and prior functional status in self-care and home management, including activities of daily living (ADL) and instrumental activities of daily living (IADL) • Current and prior functional status in work (job/school/play), community, and leisure actions, tasks, or activities Medications • Medications for current condition • Medications previously taken for current condition • Medications for other conditions Other Clinical Tests • Laboratory and diagnostic tests • Review of available records (eg., medical, education, surgical) • Review of other clinical findings (eg., nutrition and hydration) Figure 1.3 Types of data that may be generated from patient history. (From APTA Guide to Physical Therapist Practice 4, p. 36 with permission.) the therapist may begin with an examination of functional performance, during which the therapist analyzes the differences between the patient’s performance and the “typical” or expected performance of a task. For example, the patient with stroke is asked to transfer from bed to wheelchair. The therapist observes the performance and determines that the patient lacks postural support (stability), adequate lower extremity (LE) extensor strength to reach the full upright position, and adequate ROM in ankle dorsiflexors. The therapist then progresses CHAPTER 1 Box 1.2 Clinical Decision Making 7 Sample Interview Questions I. Interview questions designed to identify the nature and history of the current problem(s): What problems bring you to therapy? When did the problem(s) begin? What happened to precipitate the problem(s)? How long has the problem(s) existed? How are you taking care of the problem(s)? What makes the problem(s) better? What makes the problem(s) worse? What are your goals and expectations for physical therapy? Are you seeing anyone else for the problem(s)? II. Interview questions designed to identify desired outcomes in terms of essential functional activities include the following: What activities do you normally do at home/work/ school? What activities are you unable to do? What activities are done differently and how are they different (i.e., extra time, extra effort, different strategy)? What activities do you need help to perform that you would rather do yourself? What leisure activities are important to you? How can I help you be more independent? III. Interview questions designed to identify environmental conditions in which patient activities typically occur include the following: Describe your home/school/work environment. How do you move around/access areas in the home (i.e., bathroom, bedroom, entering and exiting the home)? How safe do you feel? How do you move around/access areas in the community (i.e., workplace, school, grocery store, shopping center, community center, stairs, curbs, ramps)? How safe do you feel? IV. Interview questions designed to identify available social supports include the following: Who lives with you? Who assists in your care (i.e., basic activities of daily living [BADL], instrumental activities of daily living [IADL])? Who helps you with the activities you want to do (i.e., walking, stairs, transfers)? Are there activities you have difficulty with that would benefit from additional assistance? V. Interview questions designed to identify the patient’s knowledge of potential disablement risk factors include the following: What problems might be anticipated in the future? What can you do to eliminate or reduce the likelihood of that happening? Sources: Section I: from the Documentation Template for Physical Therapist Patient/Client Management in the Guide to Physical Therapist Practice (4, pp. 707–712); Sections II–IV adapted from Randall (5, p. 1,200). to a detailed examination of impairments. The decision as to which approach to use is based on the results of the screening examination and the therapist’s knowledge of the health condition. Key information to obtain during an examination of function is the level of independence or dependence, as well as the need for physical assistance, external devices, or environmental modifications. Adequate training and skill in performing specific tests and measures are crucial in ensuring both validity and reliability of the tests. Failure to correctly perform an examination procedure can lead to the gathering of inaccurate data and the formation of an inappropriate POC. Later chapters focus on specific tests and measures and discuss issues of validity and reliability. The use of disability-specific standardized instruments (e.g., for individuals with stroke, the Fugl-Meyer Assessment of Physical Performance) can facilitate the examination process but may not always be appropriate for each individual patient. The therapist needs to carefully review the unique problems of the patient to determine the appropriateness and sensitivity of an instrument. Box 1.3 presents the categories for tests and measures identified in the Guide to Physical Therapist Practice.4 Novice therapists should resist the tendency to gather excessive and extraneous data in the mistaken belief that more information is better. Unnecessary data will only confuse the picture, rendering clinical decision making more difficult and unnecessarily raising the cost of care. If problems arise that are not initially identified in the history or systems review, or if the data obtained are inconsistent, additional tests or measures may be indicated. Consultation with an experienced therapist can provide an important means of clarifying inconsistencies and determining the appropriateness of specific tests and measures. Evaluation Data gathered from the initial examination must then be organized and analyzed. The therapist identifies and prioritizes the patient’s impairments, activity limitations, and participation restrictions and develops a problem list. It is important to accurately recognize those clinical problems associated with the primary disorder and those associated with co-morbid conditions. Table 1.1 presents a sample prioritized problem list. Impairments, activity limitations, and participation restrictions must be analyzed to identify causal relationships. For example, shoulder pain in the patient with hemiplegia may be due to several factors, including hypotonicity and loss of voluntary movement, which are direct impairments, or soft tissue damage/trauma from improper transfers, which is an indirect impairment, resulting from an activity. Determining the causative 8 SECTION I Box 1.3 Clinical Decision Making and Examination Categories for Tests and Measures Aerobic Capacity/Endurance Anthropometric Characteristics Arousal, Attention, and Cognition Assistive and Adaptive Devices Circulation (Arterial, Venous, Lymphatic) Cranial and Peripheral Nerve Integrity Environmental, Home, and Work (Job/School/Play) Barriers Ergonomics and Body Mechanics Gait, Locomotion, and Balance Integumentary Integrity Joint Integrity and Mobility Motor Function (Motor Control and Motor Learning) Muscle Performance (Including Strength, Power, and Endurance) Neuromotor Development and Sensory Integration Orthotic, Protective, and Supportive Devices Pain Posture Prosthetic Requirements Range of Motion (Including Muscle Length) Reflex Integrity Self-Care and Home Management (Including Activities of Daily Living and Instrumental Activities of Daily Living) Sensory Integrity Ventilation and Respiration/Gas Exchange Work (Job/School/Play), Community, and Leisure Integration or Reintegration (Including Instrumental Activities of Daily Living) Adapted from APTA Guide to Physical Therapist Practice.4 factors is a difficult yet critical step in determining appropriate treatment interventions and resolving the patient’s pain. The skilled clinician is able to identify the role barriers and facilitators in the patient’s environment in order to incorporate measures to minimize or maximize these factors into the POC. A POC that emphasizes and reinforces facilitators enhances function and the patient’s ability to experience success. Improved motivation and engagement are the natural outcomes of reinforcement of facilitators. For example, the patient with stroke may have intact communication skills, cognitive skills, and good function of the uninvolved extremities. Facilitators can also include supportive and knowledgeable family members/caregivers and an appropriate living environment. Diagnosis A medical diagnosis refers to the identification of a disease, disorder, or condition (pathology/pathophysiology) by evaluating the presenting signs, symptoms, history, laboratory test results, and procedures. It is identified primarily at the cellular level. Physical therapists use the term diagnosis to “identify the impact of a condition on function at the level of the system (especially the movement system) and at the level of the whole person.”4 Thus, the term is used to clarify the professional body of knowledge as well as the role of physical therapists in health care. For example: Medical diagnosis: Cerebrovascular accident (CVA) Physical therapy diagnosis: Impaired motor function and sensory integrity associated with nonprogressive disorders of the central nervous system—acquired in adolescence or adulthood4, p. 365 Medical diagnosis: Spinal cord injury (SCI) Physical therapy diagnosis: Impaired motor function, peripheral nerve integrity, and sensory integrity associated with nonprogressive disorders of the spinal cord4, p. 437 The diagnostic process includes integrating and evaluating the data obtained during the examination to describe the patient/client condition in terms that will guide the prognosis and selection of intervention strategies during the development of the POC. The Guide to Physical Therapist Practice organizes diagnostic categories specific to physical therapy by preferred practice patterns.4 There are four main categories of conditions: Musculoskeletal, Neuromuscular, Cardiovascular/Pulmonary, and Integumentary, with preferred practice patterns identified in each (see Appendix 1.A). The patterns are described fully according to the five elements of patient/client management (i.e., examination, evaluation, diagnosis, prognosis, and intervention). Each pattern also includes reexamination to evaluate progress, global outcomes, and criteria for termination of physical therapy services. Inclusion and exclusion criteria for each practice pattern and criteria for multiple-pattern classification are also presented. The patterns represent the collaborative effort of experienced physical therapists who detailed the broad categories of problems commonly seen by physical therapists within the scope of their knowledge, experience, and expertise. Expert consensus was thus used to develop and define the diagnostic categories and preferred practice patterns. Given the central role of physical therapists as movement specialists, the therapist will need to focus the diagnosis on the results of activity analysis and movement problems identified during the examination when formulating the prognosis and POC. The use of diagnostic categories specific to physical therapy, as Sarhman points out, (1) allows for successful communication with colleagues and patients/caregivers about the conditions that require the physical therapist’s expertise, (2) provides an appropriate classification for establishing standards of examination and treatment, and (3) directs examination of treatment effectiveness, thereby enhancing evidence-based practice.6 Physical therapy diagnostic categories also facilitate successful reimbursement when linked to functional outcomes and enhance direct access of physical therapy services. CHAPTER 1 Table 1.1 Clinical Decision Making 9 Sample Prioritized Problem List for a Patient With Stroke Direct Impairments R hemiparesis RUE > RLE Hypotonicity RUE Spasticity RLE: knee ext, plantiflexors Synergy patterns RLE > RUE Mild dysarthria Mild cognitive deficits: dec STM Dec motor planning ability CO-MORBIDITIES: Dec sensation both feet Small ulcer L foot (5th toe) Indirect Impairments Composite Impairments Activity Limitations Participation Restrictions R shoulder subluxation Balance deficits Standing > sitting Dep bed mobility: minA Dec community mobility Dec ROM R shoulder Gait deficits Dep BADL: min/mod A IADL: unable Kyphosis, forward head Dec endurance Dep transfers: modA X 1 Dec ability to perform social roles: husband Dep locomotion: modA X 1 Stairs: unable Inc fall risk Diabetic Peripheral Neuropathy Dec balance Inc fall risk Dec endurance Gait deficits: requires special shoes Dec community mobility Contextual factors: physical, social, attitudinal One-level ranch house; entry with 2 steps, no handrails Highly motivated Personal factors: individual’s life and living situation Spouse is primary caregiver; has osteoporosis and decreased vision (bilateral cataracts). Has 2 involved sons living within 30 mile radius. Key: BADL: basic activities of daily living; Dec: decreased; Dep: dependent; IADL: instrumental activities of daily living; Inc: increased; minA: minimal assistance; modA: moderate assistance; RLE: right lower extremity; RUE: right upper extremity; STM: short term memory. Prognosis The term prognosis refers to “the predicted optimal level of improvement in function and amount of time needed to reach that level.”4, p. 46 An accurate prognosis may be determined at the onset of treatment for some patients. For other patients with more complicated conditions such as severe traumatic brain injury (TBI) accompanied by extensive disability and multisystem involvement, a prognosis or prediction of level of improvement can be determined only at various increments during the course of rehabilitation. Knowledge of recovery patterns (stage of disorder) is sometimes useful to guide decision making. The amount of time needed to reach optimal recovery is an important determination, one that is required by Medicare and many other insurance providers. Predicting optimal levels of recovery and time frames can be a challenging process for the novice therapist. Use of experienced, expert staff as resources and mentors can facilitate this step in the decision making process. For each preferred practice pattern, the Guide to Physical Therapist Practice includes a broad range of expected number of visits per episode of care.4 Plan of Care The plan of care (POC) outlines anticipated patient management. The therapist evaluates and integrates data obtained from the patient/client history, the systems review, and tests and measures within the context of other factors, including the patient’s overall health, availability of social support systems, living environment, and potential discharge destination. Multisystem involvement, severe impairment and functional loss, extended time of involvement (chronicity), multiple co-morbid conditions, and medical stability of the patient are important parameters that increase the complexity of the decision making process. 10 SECTION I Clinical Decision Making and Examination A major focus of the POC is producing meaningful changes at the personal/social level by reducing activity limitations and participation restrictions. Achieving independence in locomotion or activities of daily living (ADL), return to work, or participation in recreational activities is important to the patient/client in terms of improving quality of life (QOL).7 QOL is defined as the sense of total well-being that encompasses both physical and psychosocial aspects of the patient/client’s life. Finally, not all impairments can be remediated by physical therapy. Some impairments are permanent or progressive, the direct result of unrelenting pathology such as amyotrophic lateral sclerosis (ALS). In this example, a primary emphasis on reducing the number and severity of indirect impairments and activity limitations is appropriate. Essential components of the POC include (1) anticipated goals and expected outcomes; (2) the predicted level of optimal improvement; (3) the specific interventions to be used, including type, duration, and frequency; and (4) criteria for discharge. Goals and Expected Outcomes An important first step in the development of the POC is the determination of anticipated goals and expected outcomes, the intended results of patient/client management. Goal and outcome statements address patient-identified priorities and predicted changes in impairments, activity limitations, and participation restrictions. They also address predicted changes in overall health, risk reduction and prevention, wellness and fitness, and optimization of patient/client satisfaction. The difference is in terms of time frame. Outcomes define the patient’s expected level at the conclusion of the episode of care or rehabilitation stay, whereas goals define the interim steps that are necessary to achieve expected outcomes.4 Goal and outcome statements should be realistic, objective, measurable, and time limited. There are four essential elements: • Individual: Who will perform the specific behavior or activity required or aspect of care? Goals and outcomes are focused on the patient/client. This includes individuals who receive direct care physical therapy services and/or individuals who benefit from consultation and advice, or services focused on promoting, health, wellness, and fitness. Goals can also be focused on family members or caregivers, for example, the parent of a child with a developmental disability. • Behavior/Activity: What is the specific behavior or activity the patient/client will demonstrate? Goals and outcomes include changes in impairments (e.g., ROM, strength, balance) and changes in activity limitations (e.g., transfers, ambulation, ADL) or participation restrictions (e.g., community mobility, return to school or work). • Condition: What are the conditions under which the patient/client’s behavior is measured? The goal or outcome statement specifies the specific conditions or measures required for successful achievement, for example, distance achieved, required time to perform the activity, the specific number of successful attempts out of a specific number of trials. Statements focused on functional changes should include a description of the conditions required for acceptable performance. For example, the functional levels of performance in the Functional Independence Measure (FIM) are used in the majority of rehabilitation centers in the United States. This instrument grades levels from No Helper/Independence (grade 7) to No Helper/Modified Independence (grade 6; device), to Helper/Modified Dependence (grades 5, 4, and 3; supervision, minimal, moderate, assistance), to Helper/Complete Dependence (grades 2 and 1; maximal, total assistance) (see Chapter 8 and Figure 8.5 for a complete description of this instrument).8 The type of environment required for a successful outcome of the behavior should also be specified: clinic environment (e.g., quiet room, level floor surface, physical therapy gym), home (e.g., one flight of eight stairs, carpeted surfaces), and community (e.g., uneven grassy surfaces, curbs, ramps). • Time: How long will it take to achieve the stated goal or outcome? Goals can be expressed as shortterm (generally considered to be 2 to 3 weeks) and long-term (longer than 3 weeks). Outcomes describe the expected level of functional performance attained at the end of the episode of care or rehabilitation stay. In instances of severe disability and incomplete recovery, for example, the patient with traumatic brain injury, the therapist, and team members may have difficulty determining the expected outcomes at the beginning of rehabilitation. Long-term goals can be used that focus on the expectations for a specific stage of recovery (e.g., minimally conscious states, confusional states). Goals and outcomes can also be modified following a significant change in patient status. Each POC has multiple goals and outcomes. Goals may be linked to the successful attainment of more than one outcome. For example, attaining ROM in dorsiflexion is critical to the functional outcomes of independence in transfers and locomotion. The successful attainment of an outcome is also dependent on achieving a number of different goals. For example, independent locomotion (the outcome) is dependent on increasing strength, ROM, and balance skills. In formulating a POC, the therapist accurately identifies the relationship between and among goals and sequences them appropriately. Box 1.4 presents examples of outcome and goal statements. In rehabilitation settings, the POC also includes a statement regarding the patient’s overall rehabilitation CHAPTER 1 Box 1.4 Clinical Decision Making 11 Examples of Outcome and Goal Statements The following are examples of expected outcomes, all to be achieved within the anticipated rehab stay: The patient will be independent and safe in ambulation using an ankle-foot orthosis and a quad cane on level surfaces for unlimited community distances and for all daily activities within 8 weeks. The patient will demonstrate modified dependence with close supervision in wheelchair propulsion for limited household distances (up to 50 feet) within 8 weeks. The patient will demonstrate modified dependence with minimum assistance of one person for all transfer activities in the home environment within 6 weeks. The patient will demonstrate independence in basic activities of daily living (BADL) with minimal setup and equipment (use of a reacher) within 6 weeks. The patient and family will demonstrate enhanced decision making skills regarding the health of the patient and use of health care resources within 6 weeks. The following are examples of anticipated goals with variable time frames: Short-Term Goals The patient will increase strength in shoulder depressor muscles and elbow extensor muscles in both upper extremities from good to normal within 3 weeks. The patient will increase ROM 10 degrees in knee extension bilaterally to within normal limits within 3 weeks. The patient will be independent in the application of lower extremity orthoses within 1 week. The patient and family will recognize personal and environmental factors associated with falls during ambulation within 2 weeks. The patient will attend to task for 5 min out of a 30-min treatment session within 3 weeks. Long-Term Goals The patient will independently perform transfers from wheelchair to car within 4 weeks. The patient will ambulate with bilateral knee-ankle-foot orthoses (KAFOs) and crutches using a swing-through gait and close supervision for 50 feet within 5 weeks. The patient will maintain static balance in sitting with centered, symmetrical weight-bearing and no upper extremity support or loss of balance for up to 5 minutes within 4 weeks. The patient will sequence a three- to five-step routine task with minimum assistance within 5 weeks. potential. This is typically a one-word statement: excellent, good, fair, or poor. The therapist considers multiple factors when determining rehabilitation potential, such as the patient’s condition and onset date, co-morbidity, mechanism of injury, and baseline data. The next step is to determine the intervention, defined as the purposeful interaction of the physical therapist with the patient/client and, when appropriate, other individuals involved in the care of the patient/client, using various physical therapy procedures and techniques to produce changes in the condition. Components of physical therapy intervention include coordination, communication, and documentation; patient/client-related instruction; and procedural interventions (Fig. 1.4).4 Effective communication enhances collaboration and understanding. Therapists are also responsible for coordinating care at many different levels. The therapist delegates appropriate aspects of treatment to physical therapy assistants and oversees the responsibilities of physical therapy aides. The therapist coordinates care with other professionals, family, or caregivers regarding a specific treatment approach or intervention. For example, for early transfer training to be effective, consistency in how everyone transfers the patient is important. The therapist also coordinates discharge planning with the patient and family and other interested persons. Therapists may be involved in providing POC recommendations to other facilities such as restorative nursing facilities. Coordination and Communication Patient/Client-Related Instruction Case management requires therapists to be able to communicate effectively with all members of the rehabilitation team, directly or indirectly. For example, the therapist communicates directly with other professionals at case conferences, team meetings, or rounds or indirectly through documentation in the medical record. In an era of managed care and shorter time allocations for an episode of care, effective patient/client-related instruction is critical to ensuring optimal care and successful rehabilitation. Communication strategies are developed within the context of the patient/client’s age, cultural backgrounds, language skills, and educational level, and Interventions 12 SECTION I Clinical Decision Making and Examination The Three Components of Physical Therapy Intervention Coordination, Communication, Documentation Patient/ Client-Related Instruction Procedural Interventions Therapeutic exercise Functional training in self-care and home management, including activities of daily living (ADL) and instrumental activities of daily living (IADL) Functional training in work (job/school/play), community, and leisure integration or reintegration, including IADL, work hardening, and work conditioning Manual therapy techniques, including mobilization/manipulation Prescription, application, and, as appropriate, fabrication of devices and equipment (assistive, adaptive, orthotic, protective, supportive, or prosthetic) Airway clearance techniques Integumentary repair and protective techniques Electrotherapeutic modalities Physical agents and mechanical modalities Figure 1.4 The three components of physical therapy intervention. (From APTA Guide to Physical Therapist Practice 4, p. 98 with permission.) the presence of specific communication or cognition impairments. Therapists may provide direct one-on-one instruction to a variety of individuals, including patients, clients, families, caregivers, and other interested persons. Additional strategies can include group discussions or classes, or instruction through printed or audiovisual materials. Educational interventions are directed toward ensuring an understanding of the patient’s condition, training in specific activities and exercises, determining the relevance of interventions to improve function, and achieving an expected course. In addition, educational interventions are directed toward ensuring a successful transition to the home environment (instruction in home exercise programs [HEP]), returning to work (ergonomic instruction), or resuming social activities in the community (environmental access). It is important to document what was taught, who participated, when the instruction occurred, and overall effectiveness. The need for repetition and reinforcement of educational content should also be documented in the medical record. Procedural Interventions Skilled physical therapy includes a wide variety of procedural interventions, which can be broadly classified into three main groups. Restorative interventions are directed toward remediating or improving the patient’s status in terms of impairments, activity limitations, participation restrictions, and recovery of function. The involved segments are targeted for intervention. This approach assumes an existing potential for change (e.g., neuroplasticity of brain and spinal cord function; potential for muscle strengthening or improving aerobic endurance). For example, the patient with incomplete spinal cord injury (SCI) undergoes locomotor training using body weight support and a treadmill (BWSTT). Patients with chronic progressive pathology (e.g., the patient with Parkinson’s disease) may not respond to restorative interventions aimed at resolving direct impairments; interventions aimed at restoring or optimizing function and modifying indirect impairments can, however, have a positive outcome. Compensatory interventions are directed toward promoting optimal function using residual abilities. The activity (task) is adapted (changed) in order to achieve function. The uninvolved or less involved segments are targeted for intervention. For example, the patient with left hemiplegia learns to dress using the right upper extremity (UE); the patient with complete T1 paraplegia learns to roll using upper extremities (UEs) and momentum. Environmental adaptations are also used to facilitate relearning of functional skills and optimal performance. For example, the patient with TBI is able to dress by selecting clothing from color-coded drawers. Compensatory interventions can be used in conjunction with restorative interventions to maximize function or when restorative interventions are unrealistic or unsuccessful. Preventative interventions are directed toward minimizing potential problems (e.g., anticipated indirect impairments, activity limitations, and participation restrictions) and maintaining health. For example, early resumption of upright standing using a tilt table minimizes the risk of pneumonia, bone loss, and renal calculi in the patient with SCI. A successful educational program for frequent skin inspection can prevent the development of pressure ulcers in that same patient with SCI. Interventions are chosen based on the medical diagnosis, the evaluation of examination, the physical therapy diagnosis, the prognosis, and the anticipated goals and expected outcomes. The therapist relies on knowledge of foundational science and interventions (e.g., principles of motor learning, motor control, muscle performance, task-specific training, and cardiovascular conditioning) in order to determine those interventions that are likely to achieve successful outcomes. It is important to identify all possible interventions early in the process, to carefully weigh those alternatives, and then to decide on the interventions that have the best probability of success. Narrowly adhering to one treatment approach reduces the available options and may limit or preclude successful outcomes. Use of a protocol (e.g., predetermined CHAPTER 1 exercises for the patient with hip fracture) standardizes some aspects of care but may not meet the individual needs of the patient. Protocols can foster a separation of examination/evaluation findings from the selection of treatments. Watts suggests that clinical judgment is clearly an elegant mixture of art and science.9 Professional consultation with expert clinicians and mentors is an effective means of helping the novice sort through the complex issues involved in decision making, especially when complicating factors intervene. For example, a consultation would be beneficial for the inexperienced therapist who is treating a patient that is chronically ill, has multiple co-morbidities or complications, impaired cognition, inadequate social supports, and severe activity limitations. A general outline of the POC is constructed. Schema can be used to present a framework for approaching a specific aspect of treatment and assist the therapist in organizing essential intervention elements of the plan. One such commonly used schema for exercise intervention is the FITT equation (frequency-intensity-time-type), presented in Box 1.5. The therapist should ideally choose interventions that accomplish more than one goal and are linked to the expected outcomes. The interventions should be effectively sequenced to address key impairments first and to achieve optimum motivational effect, interspacing the more difficult or uncomfortable procedures with easier Box 1.5 Clinical Decision Making 13 ones. The therapist should include tasks that ensure success during the treatment session and, whenever possible, should end each session on a positive note. This helps the patient retain a positive feeling of success and look forward to the next treatment. Discharge Planning Discharge planning is initiated early in the rehabilitation process during the data collection phase and intensifies as goals and expected outcomes are close to being reached. Discharge planning may also be initiated if the patient refuses further treatment or becomes medically or psychologically unstable. If the patient is discharged before outcomes are reached, the reasons for discontinuation of services must be carefully documented. Elements of an effective discharge plan are included in Box 1.6. The therapist should also include the discharge prognosis, typically a one-word response such as excellent, good, fair, or poor. It reflects the therapist’s judgment of the patient’s ability to maintain the level of function achieved at the end of rehabilitation without continued skilled intervention. Implementation of the Plan of Care The therapist must take into account a number of factors in structuring an effective treatment session. The patient’s comfort and optimal performance should be a priority. The environment should be structured appropriately to The FITT Equation for Exercise Intervention Frequency: How often will the patient receive skilled care? This is typically defined in terms of the number of times per week treatment will be given (e.g., daily or three times per week), or the number of visits before a specific date. Intensity: What is the prescribed intensity of exercises or activity training? For example, the POC includes sit-to-stand repetitions, 3 sets of 5 reps each, progressing from high seat to low. Time (duration): How long will the patient receive skilled care? This is typically defined in terms of days or weeks (e.g., three times per week for 6 weeks). The duration of an anticipated individual treatment session should also be defined (e.g., 30- or 60-minute sessions). Type of intervention: What are the specific exercise strategies or procedural interventions used? Necessary components that should be identified include the following: • Posture and activity: a description of the specific posture and activity the patient must perform (e.g., sitting, weight shifting or standing, modified plantigrade, reaching). • Techniques used: mode of therapist action or intervention used (e.g., guided, active-assisted, or resisted movement), or specific technique (e.g., rhythmic stabilization, dynamic reversals). • Motor learning strategies used: strategies specific to type of feedback (e.g., knowledge of results, knowledge of performance) and scheduling of feedback (e.g., constant or variable), practice schedule (e.g., blocked, serial, or random order), and environment (e.g., closed/structured or open/variable). • Additional required elements: those elements necessary to assist the patient in the exercise or activity (e.g., verbal cues, manual contacts) or equipment (e.g., elastic band resistance, therapy ball, body weight support system with motorized treadmill). 14 SECTION I Box 1.6 Clinical Decision Making and Examination Elements of the Discharge Plan Patient, family, or caregiver education: instruction includes information regarding the following: • Current condition (pathology), impairments, activity limitations, and participation restrictions • Ways to reduce risk factors for recurrence of condition and developing complications, indirect impairments, activity limitations, and participation restrictions • Ways to maintain/enhance performance and functional independence • Ways to foster healthy habits, wellness, and prevention • Ways to assist in transition to a new setting (e.g., home, skilled nursing facility) • Ways to assist in transition to new roles Plans for follow-up care or referral to another agency: patient/caregiver is provided with the following: • Information regarding follow-up visit to rehabilitation center or referral to another agency (e.g., home care agency, outpatient facility) as needed • Information regarding community support group and community fitness center as appropriate Instruction in a home exercise plan (HEP): patient/ caregiver instruction regarding the following: • Home exercises, activity training, ADL training • Use of adaptive equipment (e.g., assistive devices, orthoses, wheelchairs) Evaluation/modification of the home environment: • Planning regarding the home environment and modifications needed to assist the patient in the home (e.g., installation of ramps and rails, bathroom equipment such as tub seats, raised toilet seats, bathroom rails, furniture rearrangement or removal to ease functional mobility) • All essential equipment and renovations should be in place before discharge reduce distractions and focus the patient’s attention on the task. Patient privacy should be respected, with adequate draping and positioning. The therapist should consider good body mechanics, effective use of gravity and position, and correct application of techniques and modalities. Any equipment should be gathered prior to treatment and be in good working order. All safety precautions must be observed. The patient’s pretreatment level of function or initial state should be carefully examined. General state organization of the CNS and homeostatic balance of the somatic and autonomic nervous systems are important determinants of how a patient may respond to intervention. A wide range of influences, from emotional to cognitive to organic, may affect how a patient reacts to a particular treatment. Patients who are overly stressed may demonstrate altered homeostatic responses. For example, the patient with TBI who presents with high arousal and agitated behaviors can be expected to react to treatment in unpredictable ways, characterized by “fight or flight” responses. Similarly, patients with TBI who are lethargic may be difficult to arouse and demonstrate limited ability to participate in therapy sessions. Responses to treatment should be carefully monitored throughout the episode of care, and treatment modifications should be implemented as soon as needed to ensure successful performance. Therapists develop the “art of clinical practice” by learning to adjust their input (e.g., verbal commands and manual contacts) in response to the patient. Treatment thus becomes a dynamic and interactive process between patient and therapist. Shaping of behavior can be further enhanced by careful orientation to the purpose of the tasks and how they meet the patient’s needs, thereby ensuring optimal cooperation and motivation.10 Reexamination of the Patient and Evaluation of Expected Outcomes This last step is ongoing and involves continuous reexamination of the patient and a determination of the efficacy of treatment. Reexamination data are evaluated within the context of the patient’s progress toward anticipated goals and expected outcomes set forth in the POC. A determination is made whether the goals and outcomes are reasonable given the patient’s diagnosis and progress. If the patient attains the desired level of competence for the stated goals, revisions in the POC are indicated. If the patient attains the desired level of competence for the expected outcomes, discharge is considered. If the patient fails to achieve the stated goals or outcomes, the therapist must determine why. Were the goals and outcomes realistic given the clinical problems and database? Were the interventions selected at an appropriate level to challenge the patient, or were they too easy or too difficult? Were facilitators appropriately identified and the patient sufficiently motivated? Were intervening and constraining factors (barriers) identified? If the interventions were not appropriate, additional information is sought, goals modified, and different treatment interventions selected. Revision in the POC is also indicated if the patient progresses more rapidly or slowly than expected. Each modification must be evaluated in terms of its overall impact on the POC. Thus, the plan becomes a fluid statement of how the patient is progressing and what goals and outcomes are achievable. Its overall success depends on the therapist’s ongoing clinical decision making skills and on engaging the patient’s cooperation and motivation. Patient involvement in the development and monitoring of the POC should be documented. CHAPTER 1 ■ PATIENT PARTICIPATION IN PLANNING A patient-centered approach that involves the patient in collaborative planning and evaluation of outcomes is important in a successful POC. The patient is viewed as an active participant and partner who can make informed choices and assume responsibility for his or her own health care. Therapists who place strong emphasis on communicating effectively; educating their patients, families, and caregivers; and teaching self-management skills are able to successfully empower patients. The natural outcomes of this approach are improved therapy outcomes and overall satisfaction with care.11 Some rehabilitation plans have failed miserably simply because the therapist did not fully involve the patient in the planning process, producing goals or outcomes that were not meaningful to the patient (e.g., for the patient with incomplete SCI, independent wheelchair mobility). That same patient may have established a very different set of personal goals and expectations (e.g., return to walking). For many patients for whom complete recovery is not expected, the overall “goal of any rehabilitation program must be to increase the ability of individuals to manage their lives in the context of ongoing disability, to the greatest extent possible.”11, p. 7 This cannot be effectively done if the therapist assumes the role of expert and sole planner, establishing the rules, regulations, and instructions for rehabilitation. Rather, it is critical to engage the patient in collaborative problem solving and promote lifelong skills in health management. The patient’s ability and motivation to participate in planning do vary. The more ill the patient, the more anxiety, and the less likely that he or she will want to be actively involved in planning. As the illness resolves and the patient begins to improve, the more likely he or she will be to want to be engaged in planning the treatment. Also the more difficult the problems encountered, the more likely patients are to put their trust in “the experts” and the less likely they are to trust their own abilities to reach effective decisions. The therapist needs to guard against promoting dependence on the expert (the “my therapist syndrome”) to the exclusion of the patient’s listening to his or her own thoughts and feelings. The patient’s feelings of perceived helplessness are increased while the patient’s ability to utilize his or her own decision making abilities is delayed or restricted. Ozer et al11 address these issues in an excellent reference titled Treatment Planning for Rehabilitation—A Patient-Centered Approach. The authors suggest asking the patient a series of probing questions to engage patients in the treatment planning process (Box 1.7). The level of participation in this process may start out limited but can be expected to expand as the collaborative process is continued. A Levels of Participation Scale can be used to evaluate and document patient participation in the planning process (Box 1.8). In determining the patient’s level Box 1.7 Clinical Decision Making 15 Questions Designed to Engage the Patient in the Treatment Planning Process 1. What are your concerns? 2. What is your greatest concern? 3. What would you like to see happen? What would make you feel that you are making progress in dealing with your chief concern? What are your goals? 4. What is your specific goal? 5. What results have you achieved? 6. What problems do you have? What questions do you have? 7. What would you like to see accomplished that would make you feel that you are making some progress in dealing with your greatest concern? From Ozer, M, Payton, O, and Nelson, C: Treatment Planning for Rehabilitation—A Patient-Centered Approach. McGraw-Hill, New York, 2000, pp. 37 and 60, with permission. Box 1.8 Levels of Participation Scale A = FREE CHOICE: The therapist asks an open-ended question. The patient explores and selects the answer (what) and further specifies where? and to what degree? B = MULTIPLE CHOICE: The therapist asks questions, provides suggestions (three options). The patient selects one choice from the alternatives presented. C = CONFIRMED CHOICE: The therapist asks questions, provides a recommendation (one choice), and asks for agreement. The patient puts into own words what has been selected. D = FORCED CHOICE: The therapist asks questions, provides a recommendation (one option); the patient agrees (or disagrees) with what has been selected. E = NO CHOICE: The therapist prescribes, does not ask; the patient is compliant (or noncompliant). From Ozer, M, Payton, O, and Nelson, C: Treatment Planning for Rehabilitation—A Patient-Centered Approach. McGraw-Hill, New York, 2000, p. 44, with permission. of functioning, the therapist starts at the upper end of the scale (free choice) and moves down the scale as necessary. The lowest level of participation is recorded. For most patients, the lowest level of participation is optimally Level B Multiple Choice. Patients with significant cognitive or communication deficits (e.g., the patient with TBI) typically will require lower levels of participation. The goal as the patient recovers and progresses in rehabilitation is to increasingly involve the patient in the planning process, to whatever extent possible. In these situations, the therapist can document improving 16 SECTION I Clinical Decision Making and Examination levels of participation as evidence of meeting a goal of improving self-efficacy and self-management. ■ DOCUMENTATION Documentation is an essential requirement for timely reimbursement of services and communication among the rehabilitation team members. Written documentation is formally done at the time of admission and discharge, and at periodic intervals during the course of rehabilitation (interim or progress notes). Many facilities require documentation for every treatment session. The format and timing of notes will vary according to the regulatory requirements specified by institutional policy and thirdparty payers. Data included in the medical record should be meaningful (important, not just nice to have), complete and accurate (valid and reliable), timely (recorded promptly), and systematic (regularly recorded). All handwritten entries should be in ink, legible, and signed with a legal signature. Written charting errors should be corrected by a single line through the error and initialing and dating directly above the error. See Appendix 1.B: Defensible Documentation—General Documentation Guidelines from APTA (American Physical Therapy Association), practice-dept@apta.org. In the United States, all health care facilities must adhere to the ICD-9-CM Official Guidelines for Coding and Reporting.12 These codes are developed by the Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics (NCHS) and based on the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Adherence to these guidelines is required under the Health Insurance Portability and Accountability Act (HIPAA). Typical billing codes related to the preferred practice patterns are listed in the Guide to Physical Therapist Practice.4 Electronic Documentation There is increasing emphasis on using electronic documentation in physical therapy, which can provide a fully integrated and completely paperless workflow for managing patient care. This includes managing referrals, initial intake data, progress and discharge notes, scheduling, and billing. Advantages of electronic documentation include standardization of data entry, increased speed of access to data, and integration of data that can be used for a wide variety of applications (e.g., clinical management of patients, quality control, clinical research). Therapists no longer have to track down medical records to review or input data, because information is readily available from any computer or electronic device with Internet access. Therapists also can receive notification of when the patient arrives or checks in, what notes are due, and scheduled evaluations and POC updates. Software programs typically do not allow notes be filed unless all the required elements are completed. Overall efficiency of practice management is increased with decreased errors in documentation and improved accuracy of reimbursements. Many different companies provide software programs for physical therapy that focus on specific practice settings (e.g., outpatient rehabilitation therapy, home care, private practice). Therapists using documentation software for electronic entry of patient data should ensure that programs comply with appropriate provisions for security and confidentiality. ■ CLINICAL DECISION MAKING: EXPERT VERSUS NOVICE There is an accumulating body of evidence on expertise in physical therapy practice, spearheaded by the pivotal work of Jenson and colleagues.13-15 These researchers have shown that the knowledge, skills, and decision making abilities used by expert clinicians can be identified, nurtured, and taught. Embrey et al16 suggest that the novice therapist may benefit from a period of active mentoring by expert clinicians early in clinical practice (e.g., clinical residency). This information has important implications for novice therapists and for educators involved in teaching clinical decision making. Experienced clinicians utilize a forward reasoning process (reasoning from data to hypothesis) in which the clinician is able to recognize patient cues and patterns as being similar to previously identified cases. Decisions are formulated based on higher-order (metacognitive) skills and reflective processes. Hypothesis testing is not typically verbalized. Thus, actions are based on a rich experience-based clinical knowledge and pattern recognition. In contrast, a backward reasoning process (also termed hypothetico-deductive process) involves identifying cues from the patient, proposing a hypothesis (reasoning from hypothesis to data), gathering supporting data for cue interpretation and evaluating the hypothesis, and determining appropriate actions. Experts may use hypothesis-testing methods when routine problem recognition fails (e.g., for an unfamiliar problem) or when they are practicing out of their area of expertise.15, 17 Decision making is influenced by knowledge and experience. Experts have more knowledge and experience and are able to organize, integrate, and shape information into a usable format. Their knowledge base is multidimensional; their clinical reasoning is reflective and focused; and they demonstrate increased confidence in evaluating patients and problem solving.15 Organization of knowledge is specific and highly dependent on the mastery of a particular practice area. Content domains in physical therapy take the form of the specialty areas (orthopedic, neurological, pediatric, and so forth). As expertise increases, master clinicians increase their abilities to categorize information, improving in both mastery of depth and complexity of content. They are able to use collegial knowledge effectively, seeking out mentors and readily consulting their peers on practice issues. Novice therapists, on the other hand, collect data, but do not always recognize important data. Simple review of data and use of book-learned, declarative knowledge CHAPTER 1 do not allow the novice to recognize meaningful relationships and generate accurate hypotheses within a realistic time frame. New therapists also tend to be rigidly governed by rules for decision making. For example, they adhere to standardized frameworks (protocols), whereas experts easily adapt and refocus their approach if a different direction is indicated. Experts also demonstrate improved intervention skills that are well integrated with their mastery of knowledge and clinical reasoning. Improved skills and expertise are developed through intense, focused, and deliberate practice. Jensen et al point out that experts are highly motivated and are constantly striving to improve their skills, demonstrating a strong inner drive for lifelong learning.18 The APTA recognizes expertise in a board-certification process for clinical specialists. The therapist who utilizes a receptive/systematic datagathering style generally suspends judgment until all possible data are gathered. The data are analyzed individually and collectively before a final determination is made of how to organize and use them. A contrasting style is perceptive and intuitive. The individual who utilizes a perceptive data-gathering style will seek and respond to ongoing cues and patterns, defining and organizing clinical problems early. Information processing is largely intuitive. Thus, these clinicians are able to respond to a large number of stimuli as they occur and consider initiation of early treatment options.15 Research suggests that styles may differ by expert group. May and Dennis19 and Jensen et al18 found that clinicians with expertise in orthopedics tended to utilize a receptive/systematic style, generating hypotheses only after a methodical and ordered search of data. Embrey et al16, 20 found that expert clinicians working in pediatric settings tended to utilize a perceptive data-gathering style and process information intuitively. Thus, they responded rapidly to cues and patterns (movement scripts) and changes that occurred within the treatment session. May and Dennis19 reported that practitioners experienced in cardiopulmonary and neurological physical therapy also tended to respond more favorably to the perceptive/intuitive style. Thus, the differences noted in terms of the types of cognitive strategies reported appear to be evoked by specific problem structure and domain. Important differences exist between expert and novice clinicians in the area of self-monitoring. Expert clinicians are able to frequently and effectively utilize self-assessment to modify and redefine their clinical decisions. This reflective aspect of practice results in improved improvisational performance, the actions that occur when therapists are actually treating patients. They are better able to control the treatment situation (i.e., constant interruptions, the demands of many scheduled patients, and multiple tasks) and the time allotted. Conversely, novice therapists demonstrate self-monitoring, but are less able to utilize the information effectively to control the situation. They react more to external stimuli and the confusion of Clinical Decision Making 17 competing demands and are less able to offer alternate intervention strategies. Self-monitoring is viewed as a positive experience by the experts twice as often as by novice therapists, an indication that the inexperienced therapists are sensitive to their limitations. The experts are also more willing to take risks and to admit when they did not know something.15, 21 Expert clinicians provide patient-centered care. They spend more time with their patients, gathering and evaluating information and involving their patients in collaborative problem solving. Experts maintain as a central goal of care the empowerment of their patients to make autonomous decisions. They affirm the importance of patient education in assisting patients to resolve problems and assume control over their own health care. Teaching strategies therefore focus on maintaining health and preventing the development of indirect impairments, activity limitations, and restrictions to participation. The therapist assumes active roles as coach and teacher.10 In an era of cost containment and limited services, this is an important value and one that is essential for ensuring successful long-term outcomes. Novice therapists, on the other hand, demonstrate greater interest in mastering hands-on skills and in ensuring the success of their treatments.17 Expert clinicians are able to maintain focus on the patient during treatment, as evidenced in their verbal and nonverbal communications. They are able to consistently demonstrate a sense of commitment and caring toward their patients. The experts demonstrate a smooth interplay of hands-on treatment with effective communication that is responsive to the needs of each individual patient.10, 15 Conversely, novice therapists are influenced by the demands of full-time clinical practice and experience increased challenges in finding adequate time to listen and talk with their patients. They report increased difficulties communicating with “difficult” and “unmotivated” patients.22 Psychosocial sensitivity is a key factor in directing experienced clinicians during the physical therapy sessions. Novice therapists maintain their focus more on the problems and the mechanics of treatment rather than on the psychosocial needs of the patient.22 ■ EVIDENCE-BASED PRACTICE The analysis of research evidence paired with the physical therapist’s experience and expertise provides a powerful tool to guide clinical decision making. There are areas of practice in physical therapy that lack rigorous examination and evidence. Therapists may employ some interventions simply because they are in widespread use. Therapists may also elect to use interventions because they are new and different or because they are the focus of “anecdotal testimonials” in continuing education courses. Harris points out, “The responsibility to deliver evidence-based treatment techniques rests with all physical therapists.”23, p. 176 To that end, the APTA developed a Clinical Research 18 SECTION I Clinical Decision Making and Examination Agenda designed to support, explain, and enhance physical therapy clinical practice.24 The Research Agenda was revised in 2011 to be reflective of the rapid changes in health care and in rehabilitation.25 It identifies broad categories of research and is consistent with the ICF. The APTA’s Hooked on Evidence project provides links to Evidence in Practice (www.ptjournal.org) and provides training programs to assist individuals in this process. Evidence-based medicine (EBM) is defined as “the integration of best research evidence with our clinical expertise and our patient’s unique values and circumstances.”26, p. 1 The term evidence-based practice (EBP) encompasses a broader range of health professions. The essential steps of EBP26 are as follows: Step 1: A clinical problem is identified and an answerable question is formulated. Step 2: A systematic literature review is conducted and evidence collected. Step 3: The research evidence is critically analyzed for its validity (closeness to the truth), impact (size of the effect), and applicability (usefulness in clinical practice). Step 4: The critical appraisal is synthesized and integrated with the clinician’s expertise and the patient’s unique biology, values, and circumstances. Step 5: The effectiveness and efficiency of the steps in the evidence-based process are evaluated. A well-built research question contains three elements: (1) a specific patient/client group or population, (2) the specific interventions or exposures to be Box 1.9 studied, and (3) the outcomes achieved. For example, one study examined interventions commonly applied for low back pain (therapeutic exercise, transcutaneous electrical nerve stimulation [TENS], thermotherapy, ultrasound, massage, E-stim system, traction) using outcomes identified as being important to the patient (pain, function, patient global assessment, QOL, and return to work).27 Systematic review (SR) is a comprehensive examination of the literature. The researcher determines key resources to provide the evidence. These include (1) peer-reviewed and evidence-based journals, (2) online services (e.g., Cochrane Reviews, APTA Open Door, PEDro), and (3) search engines (e.g., PubMed). Box 1.9 provides a brief list of electronic medical databases. Specific criteria are developed for the inclusion and exclusion of the research studies selected for review. Studies employing different designs may be analyzed individually or compared qualitatively; studies of similar design may be combined quantitatively (e.g., meta-analysis). Critical analysis of research findings involves detailed examination of methodology, results, and conclusions. The clinician should be able to answer the following questions: (1) What is the level of evidence? (2) Is the evidence valid? and (3) Are the results important and clinically relevant? Thus, interpretation and synthesis of the evidence must be considered within the context of the specific patient/client problem. Examination begins with the purpose of the study, which should be clearly stated, and the review of literature, which should be relevant in terms of the specific question asked. The Evidence-Based Practice: Electronic Medical Databases www.ncbi.nlm.nih.gov/ PubMed PubMEd—U.S. National Library of Medicine (NLM): search service to Medline and Pre-Medline (database of medical and biomedical research), free public access www.hookedonevidence.com APTA Open Door—Hooked on Evidence: database of evidence-based physical therapy practice, members only www.pedro.org.au/ Physiotherapy Evidence Database (PEDro) of physical therapy: RCTs, systematic reviews, and evidence-based clinical practice www.cochrane.org/reviews Cochrane Database of Systematic Reviews (Cochrane Reviews); primary source for clinical effectiveness information http://hiru.mcmaster.ca/ cochrane/centers/Canadian Canadian Cochrane Center www.cinahl.com CINAHL: database of nursing and allied health research www.york.ac.uk/inst/crd/ crddatabases.htm DARE: database of abstracts of evidence reviews from medical journals www.naric.com/research RehabDATA: database of disability and rehabilitation research www.cirrie.buffalo.edu? Center for International Rehabilitation Research Information and Exchange: database of rehabilitation research www.ovid.com Ovid: database of health and life science research CHAPTER 1 methods/design should be closely examined. Research design varies and can be evaluated in terms of levels of evidence, with grades of recommendation in order of most to least rigorous (Table 1.2). Although a randomized clinical trial (RCT) provides the most rigorous design, there are times when other designs are indicated. For example, there may be ethical issues involving control groups that receive no treatment when treatment is clearly beneficial. In addition, when outcomes are not clearly understood or defined (e.g., quality-of-life issues), designs such as single-case studies may be indicated. The reader is referred to Appendix 1-C: Overview of Evidence-Based Practice Concepts for additional discussion. Critical Appraisal Tools (CATs) are available to assist the inexperienced clinician in the evaluation of research (see Law, Appendix A: Critical Review Form, Quantitative Studies28, p. 331; and Jewell, Appendix B: Evidence Appraisal Worksheets).29, p. 427 Clinicians also need to utilize effective strategies to organize and store the data and to update data on a regular basis. Reference management systems such as Endnote and Reference Manager (ISI ResearchSoft, 800 Jones Street, Berkeley, CA 94710) are available to assist the therapist. Evidence-based clinical practice guidelines (EBCPGs) are defined by the Institute of Medicine as systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances.30 They are developed through a combination of (1) expert consensus (e.g., the Guide to Physical Clinical Decision Making 19 Therapist Practice5); (2) systematic reviews and metaanalysis; and (3) analysis of patient preferences combined with outcome-based guidelines. For example, the Philadelphia Panel is a multidisciplinary, international panel of rehabilitation experts comprising a group of Clinical Specialty Experts from the United States and the Ottawa Methods Group from Canada. This panel developed a structured and rigorous methodology to formulate evidence-based practice guidelines.31 For example, the panel analyzed the evidence following a structured and rigorous review of selected interventions for low back pain.27 The evidence was then translated into EBCPGs by reviewing key outcomes and deciding whether the intervention had clinical benefit. Categories of absolute and relative benefit were used. The panel established a clinical improvement of 15% or more relative to the control as an acceptable level of evidence. Recommendations were graded based on levels (methodological quality) of the studies. Grade A or B recommendations were required to demonstrate clinically important changes and statistical significance. The panel’s positive recommendations were then sent to 324 clinical practitioners for their feedback. The panel reviewed practitioners’ feedback and revised their recommendations accordingly. In the low back pain study, the panel recommended the following EBCPGs: (1) the use of therapeutic exercises for chronic, subacute, and post-surgery low back pain and (2) continuation of normal activities for acute low back pain. The panel found lack of evidence regarding efficacy for the use of other interventions (e.g., thermotherapy, therapeutic ultrasound, massage, electrical stimulation). EBCPGs have Table 1.2 Levels of Evidence for Treatment Effectiveness Level 1 SRa of a number of RCTsb of studies (meta-analysis) that substantially agree (do not have significant statistical variation) Level 2 Individual RCT with narrow confidence window (size of treatment effect precisely defined) Observational study with dramatic effectc Level 3 Level 4 Level 5 Nonrandomized controlled cohort studyd Case-control,e case-series,f or historically controlled studies Mechanism-based reasoning (expert opinion) a. SR, systematic review: a review in which the primary studies are summarized, critically appraised, and statistically combined; usually quantitative in nature with specific inclusion/exclusion criteria. b. RCT, randomized controlled trial: an experimental study in which participants are randomly assigned to either an experimental or control group to receive different interventions or a placebo; the most rigorous study design. c. All-or-none study: a study in which treatment produces a dramatic change in outcomes; all patients die before treatment; none die after treatment. d. Cohort study: a prospective (forward-in-time) study; a group of participants (cohort) with a similar condition receives an intervention and is followed over time and outcome evaluated; comparison is made to a matched group who do receive the intervention (quasi-experimental with no randomization). e. Case-control study: a retrospective study in which a group of subjects with a condition of interest are identified for research after outcomes are achieved; e.g., studying the impact of an intervention on level of participation; a comparison group is used. f. Case series: clinical outcomes are evaluated of a single group of patients with a similar condition. Adapted from OCEBM Levels of Evidence Working Group—Jeremy Howick, Iain Chalmers (James Lind Library), Paul Glasziou, Trish Greenhalgh, Carl Heneghan, Alessandro Liberati, Ivan Moschetti, Bob Phillips, Hazel Thornton, Olive Goddard, and Mary Hodgkinson: The Oxford 2011 Levels of Evidence. Oxford Centre for Evidence-Based Medicine. Retrieved from www.cebm.net/index.aspx?o=5653. 20 SECTION I Clinical Decision Making and Examination been published for rehabilitation of patients with the following conditions: • Shoulder pain37 • Fibromyalgia38, 39 • Low back pain27 • Knee pain32 • Knee pain and mobility impairments: meniscal and articular cartilage lesions33 • Hip pain and mobility impairments: osteoarthritis34 • Heel pain: plantar fasciitis35 • Neck pain36 According to Rothstein, these studies are clinically important in that they “are not telling us what is known and what is not known, but what is supported by evidence and what is not supported by evidence.”40, p. 1,620 The guidelines provide a summation of best possible evidence for use in clinical practice. SUMMARY An organized process of clinical decision making allows the therapist to systematically plan effective treatments. The steps identified in the patient/client management process are (1) examine the patient, and collect data through history, systems review, and tests and measures; (2) evaluate the data and identify problems; (3) determine the diagnosis; (4) determine the prognosis and POC; (5) implement the POC; and (6) reexamine the patient and evaluate treatment outcomes. Patient participation in planning is essential in ensuring successful outcomes. Evidence-based practice allows the therapist to select interventions that have been shown to provide meaningful change in patient’s lives. Inherent to the therapist’s success in this process are an appropriate knowledge base and experience, cognitive processing strategies, self-monitoring strategies, and communication and teaching skills. Documentation is an essential requirement for effective communication among the rehabilitation team members and for timely reimbursement of services. Questions for Review 1. What are the key steps in patient/client management? 2. Differentiate between impairments, activity limitations, and participation restrictions. Define and give an example of each. 3. What are the essential elements of goal and outcome statements? Write two examples of each. 4. Differentiate between restorative and compensatory interventions. Give an example of each. 5. What is the FITT equation? Give an example of how is it used in formulating interventions for a POC. 6. What are the advantages of electronic documentation systems? Disadvantages? 7. What are the elements of a well-built research question? Give an example. What is the highest level of evidence available for evidence-based clinical practice guidelines? CASE STUDY PRESENT HISTORY The patient is a 78-year-old woman who tripped and fell at home ascending the stairs outside the front door. She was admitted to the hospital after sustaining a transcervical, intracapsular fracture of the right femur. The patient had an open reduction and internal fixation (ORIF) procedure of the right lower extremity (RLE) to reduce and pin the fracture. After 2 weeks of acute hospital admission, the patient is at home and referred for home care physical therapy. PAST MEDICAL HISTORY Patient is a very thin woman (98 pounds) with long-standing problems with osteoporosis (on medication for 5 years). She has a history of falls, three in the last year alone. Approximately 3 years ago she had a myocardial infarction and presented with third-degree heart block, requiring implantation of a permanent pacemaker. She underwent cataract surgery with lens implantation in the right eye 2 years ago; the left eye is scheduled for similar surgery within the next few months. CHAPTER 1 Clinical Decision Making MEDICAL DIAGNOSES Coronary artery disease (CAD), hypertension (HTN), mitral valve prolapse, s/p permanent heart pacer, s/p right cataract with implant, osteoporosis (moderate to severe in the spine, hips, and pelvis), osteoarthritis with mild pain in right knee, s/p left elbow fracture (1 year ago), left ankle fracture (2 years ago), urinary stress incontinence. MEDICATIONS Fosamax 70 mg weekly Atenolol 24 mg PO qd MVI (multivitamin concentrate) with Fe tab PO qd Metamucil 1 tbs prn PO qd, Colace 100 mg PO bid Tylenol No. 3 tab prn/mild pain SOCIAL SUPPORT/ENVIRONMENT The patient is a retired schoolteacher who was recently widowed after 48 years of marriage. She has two sons, one daughter, and four grandchildren; all live within an hour’s driving distance. One of her children visits every weekend. She has a rambunctious black Labrador puppy that is 8 months old and was given to her “for company” at the time her husband died. She was walking the dog at the time of the accident. She is an active participant in a garden club, which meets twice a month, and in weekly events at the local senior center. Previously she was driving her car for all community activities. She lives alone in a large old New England farmhouse. Her home has an entry with four stairs and no rail. Inside there are 14 rooms on two floors. The downstairs living area has a step down into the family room with no rail. There are 14 stairs to the second floor, with rails on either side. The upstairs sleeping area is cluttered with large, heavy furniture. The second floor bathroom is small, with a high old tub with pedestal feet and a lip. There is no added equipment. PHYSICAL THERAPY EXAMINATION 1. Mental status Alert and oriented × 3 Pleasant, cooperative, articulate No apparent memory deficits Good problem solving and safety awareness about hip precautions 2. Cardiopulmonary status Pulse 74; BP 110/75 Endurance: good; min SOB with 20 min of activity 3. Sensation Vision: wears glasses; cloudy vision L eye; impaired depth perception Hearing: WFL Sensation: BLEs intact 4. Skin Incision is healed and well approximated Wears bilateral TEDs q a.m. × 6 wks 5. ROM LLE, BUEs: WFL Affected RLE: Flex 0° to 85° Ext NT Abd 0° to 20° Add NT IR, ER NT Right knee and ankle WFL 21 22 SECTION I Clinical Decision Making and Examination 6. Strength LLE, BUEs: WFL Affected RLE: Hip flex NT (not tested) Hip ext NT Hip abd NT Knee ext 4/5 Ankle DF 4/5, PF 4/5 7. Posture Flexed, stooped posture: moderate kyphosis, flexed hips and knees 1/ -inch leg length shortening on RLE; uses wedge when sitting 2 Mild resting head tremor 8. Balance Sitting balance: WFL Standing balance: Eyes open: good; leans slightly to left side Eyes closed: unsteady, begins to fall Arises from chair without help, some initial unsteadiness; sitting down: safe, smooth motion Uses 2-inch foam cushions to elevate seat of kitchen chair and living room chair 9. Functional status Patient was completely independent (I) before her fall. Results of functional examination: I bed mobility I transfers; unable to do tub transfers at present I ambulation with standard walker × 200 feet on level surfaces, partial weight-bearing RLE Increased flexion of knees and dorsal spine I one flight of stairs with rail and SBQC I dressing; requires minimal assist (MinA) of home health aide for sponge baths Requires moderate assistance (ModA) of home health aide for homemaker activities 10. Patient is highly motivated “I want to get my life back together, get my dog home again so I can take care of him.” PRIMARY INSURANCE Medicare Guiding Questions 1. Develop a prioritized problem list for this patient’s POC. Identify and categorize the patient’s impairments (direct, indirect, composite). Identify her activity limitations and participation restrictions. 2. What information is available about her functional status within the home in terms of performance versus capacity qualifiers? 3. What is her rehabilitation prognosis? 4. Write two expected outcome and two goal statements to direct her POC. 5. Identify two treatment interventions for her POC. 6. What precautions should be observed? 7. What tests and measures can be used to determine successful attainment of outcomes? CHAPTER 1 Clinical Decision Making 23 For additional resources, including answers to the questions for review and case study guiding questions, please visit http://davisplus.fadavis.com References 1. Rothstein, JM, Echternach, JL, and Riddle, DL: The hypothesisoriented algorithm for clinicians II (HOAC II): A guide for patient management. Phys Ther 83:455, 2003. 2. World Health Organization (WHO): ICF: Towards a Common Language for Functioning, Disability, and Health. Geneva, Switzerland, 2002. Retrieved March 4, 2011, from www.who. int/classifications/en. 3. World Health Organization (WHO): ICF CHECKLIST, Version 2.1a, Clinician Form for International Classification of Functioning, Disability and Health. Geneva, Switzerland, 2003. Retrieved March 4, 2011, from www.who.int/classifications/icf/ training/icfchecklist.pdf. 4. American Physical Therapy Association: Guide to physical therapist practice. Phys Ther 81:1, 2001. 5. Randall, KE, and McEwen, IR: Writing patient-centered functional goals. Phys Ther 80:1197, 2000. 6. Sarhman, SA: Diagnosis by the physical therapist—a special communication. Phys Ther 68:1703, 1988. 7. Rothstein, J: Disability and our identity. Phys Ther 74:375, 1994. 8. Guide for the Uniform Data Set for Medical Rehabilitation (including the FIM instrument), Version 5.0. State University of New York, Buffalo, 1996. 9. Watts, N: Decision analysis: A tool for improving physical therapy education. In Wolf, S (ed): Clinical Decision Making in Physical Therapy. FA Davis, Philadelphia, 1985, p 8. 10. Resnik, L, and Jensen, G: Using clinical outcomes to explore the theory of expert practice in physical therapy. Phys Ther 83:1090, 2003. 11. Ozer, M, Payton, O, and Nelson, C: Treatment Planning for Rehabilitation—A Patient-Centered Approach. McGraw-Hill, New York, 2000. 12. World Health Organization: International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) (Volumes 1, 2, 3, and Guidelines). Distributed by the National Center for Health Statistics (NCHS) and the Centers for Medicare and Medicaid Services (CMS). Retrieved March 4, 2011, from www.cdc.gov/nchs/icd/icd9cm.htm. 13. Jensen, GM, Shepard, KF, and Hack, LM: The novice versus the experienced clinician: Insights into the work of the physical therapist. Phys Ther 70:314, 1990. 14. Jensen, GM, Gwyer J, Shepard KF, et al: Expert practice in physical therapy. Phys Ther 80:28–51, 2000. 15. Jensen, GM, Gwyer, JM, Hack, LM, et al: Expertise in Physical Therapy Practice, ed 2. Saunders Elsevier, St. Louis, 2006. 16. Embrey, DG, Guthrie, MR, White, OR, et al: Clinical decision making by experienced and inexperienced pediatric physical therapists for children with diplegic cerebral palsy. Phys Ther 76:20, 1996. 17. Edwards, I, Jones, M, Carr, J, et al: Clinical reasoning strategies in physical therapy. Phys Ther 84:312, 2004. 18. Jensen, GM, et al: Attribute dimensions that distinguish master and novice physical therapy clinicians in orthopedic settings. Phys Ther 72:711, 1992. 19. May, BJ, and Dennis, JK: Expert decision making in physical therapy: A survey of practitioners. Phys Ther 71:190, 1991. 20. Embrey, DG: Clinical applications of decision making in pediatric physical therapy: Overview. Pediatr Phys Ther 8:2, 1996. 21. Embrey, DG, and Yates, L: Clinical applications of self-monitoring by experienced and novice pediatric physical therapists. Pediatr Phys Ther 8:3, 1996. 22. Greenfield, BH, Anderson, A, Cox, B, et al: Meaning of caring to 7 novice physical therapists during their first year of clinical practice. Phys Ther 88:1154, 2008. 23. Harris, S: How should treatments be critiqued for scientific merit? Phys Ther 76:175–181, 1996. 24. Guccione, A, Goldstein, M, and Elliott, S: Clinical research agenda for physical therapy. Phys Ther 80:499–513, 2000. 25. Goldstein, M, Scalzitti, D, Craik, R, et al: The revised research agenda for physical therapy. Phys Ther 91:165–174, 2011. 26. Staus, S, Glasziou, P, Richardson, W, et al: Evidence-Based Medicine: How to Practice and Teach EBM, ed 4. ChurchillLivingstone-Elsevier, New York, 2011. 27. Philadelphia Panel: Evidence-based clinical practice guidelines on selected rehabilitation interventions for low back pain. Phys Ther 81:1641, 2001. 28. Law, M, and MacDermid, J (eds): Evidence-Based Rehabilitation, ed 2. Slack Inc., Thorofare, NJ, 2008. 29. Jewell D: Guide to Evidence-Based Physical Therapy Practice. Jones & Bartlett, Boston, 2008. 30. Scalzitti, D: Evidence-based guidelines: Application to clinical practice. Phys Ther 81:1622, 2001. 31. Philadelphia Panel: Evidence-based clinical practice guidelines on selected rehabilitation interventions: Overview and methodology. Phys Ther 81:1629, 2001. 32. Philadelphia Panel: Evidence-based clinical practice guidelines on selected rehabilitation interventions for knee pain. Phys Ther 81:1675, 2001. 33. Orthopedic section, APTA: Knee pain and mobility impairments: Meniscal and articular cartilage lesions clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health. JOSPT 40(6):A30, 2010. 34. Orthopedic section, APTA: Hip pain and mobility impairments— hip osteoarthritis: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health. JOSPT 39(4):A18, 2009. 35. Orthopedic section, APTA: Heel pain—plantar fasciitis: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health. JOSPT 40(6):A30, 2010. 36. Orthopedic section, APTA: Neck pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health. JOSPT 40(6):A30, 2010. 37. Philadelphia Panel: Evidence-based clinical practice guidelines on selected rehabilitation interventions for shoulder pain. Phys Ther 81:1719, 2001. 38. Ottawa Panel: Ottawa Panel evidence-based clinical practice guidelines for aerobic fitness exercises in the management of fibromyalgia: Part 1. Phys Ther 88:857, 2008. 39. Ottawa Panel: Ottawa Panel evidence-based clinical practice guidelines for strengthening exercises in the management of fibromyalgia: Part 2. Phys Ther 88:873, 2008. 40. Rothstein, J: Autonomous practice or autonomous ignorance? Phys Ther 81:1620, 2001.