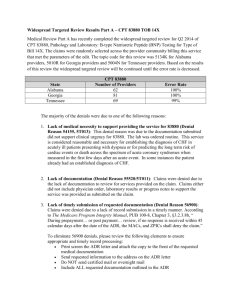
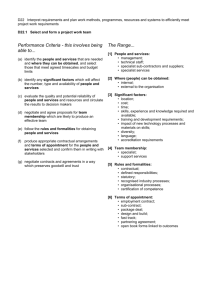
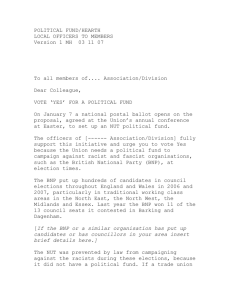
CI140409.qxd 10/28/2003 2:19 PM Page 520 AACN Clinical Issues Volume 14, Number 4, pp. 520-531 © 2003, AACN The Measurement of Brain Natriuretic Peptide in Heart Failure Precision, Accuracy, and Implications for Practice Jill N. Howie, RN, MS, NP; Mary A. Caldwell, RN, PhD, MBA; Kathleen Dracup, RN, DNSc Heart failure (HF) is a major public health problem in the United States. Approximately 4.8 million individuals are diagnosed with this syndrome and an estimated 550,000 new cases are identified each year.1 Advanced HF continues to be one of the most disabling medical conditions and common causes of death in the United States.1 After HF is diagnosed, the 1-year mortality rate increases by almost 20%.1 The magnitude of the HF epidemic will worsen as the population ages and individuals survive the cardiovascular precursors of HF (eg, acute myocardial infarction, valvular disease, hypertension). The cost of caring for patients with HF is staggering, with $3.6 billion paid to Medicare beneficiaries annually.2 Diagnosing and treating those with HF has been a clinical challenge. Patients with HF are asymptomatic in the early phases or may have symptoms such as shortness of breath, fatigue, or ankle swelling that they may not identify as serious. In addition, many patients will present to a clinical setting (physician’s office, emergency department [ED], urgent ■ Although advances have been made in the management of heart failure (HF), hospital readmission rates remain high. Finding a simple blood test to identify HF would dramatically impact the diagnosis and treatment of this syndrome. A better understanding of the pathophysiology of HF may result in improved treatment measures. Current guidelines do not target any clinical or hemodynamic criteria to achieve before discharge. Most efforts to reduce readmissions have been focused on drugs, technology, and the use of specialty HF clinics. Brain natriuretic peptide (BNP) levels have the potential of providing diagnostic, prognostic, and therapeutic information. In addition, BNP levels appear to be associated with future cardiac events such as hospital readmission. The purpose of this article is to review the precision and accuracy of BNP measurement in those with HF, and to describe how measurement of BNP can be used in clinical practice. Ultimately, BNP testing may improve the accuracy of the diagnosis of HF and guide best treatment practices. (KEYWORDS: Brain natriuretic peptide, heart failure, hospitalization, predictors) ▪▪▪▪▪▪▪▪▪▪ From UCSF School of Nursing, San Francisco, Calif. Reprint requests to: Jill Howie, Department of Physiological Nursing, Box 0610, N631G, UCSF School of Nursing, San Francisco, CA 94143 (jill.howie@nursing.ucsf.edu). 520 CI140409.qxd 10/28/2003 2:19 PM Vol. 14, No. 4 November 2003 Page 521 BRAIN NATRIURETIC PEPTIDE IN HEART FAILURE 521 care clinic) with shortness of breath where many other diagnoses need to be excluded. When HF is suspected, the patient must undergo testing that is time consuming, costly, uncomfortable, and not without risks. Those with chronic HF have episodic exacerbations where diagnostic testing is again necessary for identification of acute decompensation. Finding a simple blood test to identify HF would have a dramatic impact on diagnosis and treatment, with earlier diagnosis and a better understanding of the pathophysiology of HF leading to improved treatment. Brain natriuretic peptide (BNP) is a 32amino acid polypeptide involved in the regulation of blood pressure and fluid volume.3 BNP was first identified in porcine brain tissue, hence the confusing term “brain” natriuretic peptide, but is now known to be predominately synthesized and secreted in the cardiac ventricles.3 The terms BNP and Btype natriuretic peptide are now preferred. BNP is one of a “family” of natriuretic peptides, atrial natriuretic peptide (ANP or Atype natriuretic peptide), and C-type natriuretic peptide. The release of BNP occurs in response to increases in ventricular pressure and is directly proportional to ventricular expansion.4 BNP levels abruptly rise when HF worsens. They may also be mildly to moderately elevated in chronic HF and left ventricular (LV) dysfunction because of sustained elevations in LV pressure.3,4 Debate regarding the interpretation of elevated levels of BNP continues, but in general, it is thought that elevated BNP levels in acute HF warrant adjustment in diuretic therapy. For moderately elevated BNP levels associated with chronic HF, treatment is aggressively aimed at diminishing the effects of ventricular remodeling. BNP is becoming more widely utilized underscoring the importance for clinicians to understand the strengths and weaknesses of this test. Therefore, the purpose of this article is to review the precision and accuracy of BNP measurement in those with HF, and to describe how measurement of BNP can be utilized in clinical practice. radiometric assay (IRMA), and immunofluorometric (Triage [Biosite Diagnostics, San Diego, Calif] or IMFA method). Generally, the test is performed using the RIA method, but investigators also report the use of a commercial IRMA method (Shinoria BNP, Shinogi and Co., Ltd., Osaka, Japan). The RIA method is the less desirable method because it has a lower sensitivity and specificity, and is less precise and practical for the technician to use, but is less costly.5 The limitations to the RIA method spurred interest in the development of a more precise and practical method of BNP measurement.6 Briefly, the IRMA method uses monoclonal antibodies and 125I-labeled anti-BNP antibody solution to bind BNP and count its presence with a gamma counter. This laboratory method of testing is precise, but it is also costly, not automated, and requires approximately 36 hours to complete.7 The immunofluorometric assay or Triage method uses two murine antibodies against the biologically active portion of the BNP amino acid. 7 The Triage method utilizes a kit that resembles a blood glucose meter, although the kits require more blood than is provided by a lancet. Therefore, venipuncture is necessary for this point-of care test. Whole blood is added to the sample port, red blood cells are filtered out, and plasma enters the reaction chamber where it reacts with fluorescent antibodies. Finally, the fluorescentbound BNP traverses a detection lane and is counted. The test takes 15 minutes, is fully automated, and costs less than $30. A laboratory test that provides information quickly, noninvasively, and easily is the most desirable type of test.8 For example, troponin level is a test that provides diagnostic information quickly and spurs decision making. The BNP Triage method for diagnosing HF has garnered the most attention from clinicians because it provides the possibility for rapid diagnostic information. In this article, discussion will be limited to the Triage method of testing because it is most practical for clinical settings. Description of the Instruments Precision of the Triage Method BNP levels can be measured using three methods: radioimmunoassay (RIA), immuno- When new instruments are developed for clinical use or research purposes the instru- CI140409.qxd 522 10/28/2003 2:19 PM Page 522 HOWIE ET AL AACN Clinical Issues Figure 1. Accuracy and Precision: When new instruments are developed for clinical use or research purposes the instrument must be fully tested to ensure that the instrument is actually measuring the desired phenomena. Laboratory tests are rigorously tested for their accuracy and precision. However, accuracy and precision may not coincide. In the example of the above target, (A) neither accuracy nor precision is present. In B, the example is precise because it hits the target in the same place each time (reliable), but not accurate because the center is missed. In C, the example is accurate because it hits the target, but not precise because the same part of the target is not hit each time. In D, the example is precise and accurate because the target is struck each time (accurate) and in the same place (precise). ment must be fully tested to ensure that the instrument is actually measuring the desired phenomenon, in this case, volume overload. Thousands of instruments have been developed by nurses, physicians, sociologists, and psychologists to measure phenomena such as quality of life, social support, and perceived control, for example. These instruments undergo rigorous testing for reliability and validity. Clinical laboratory tests must also undergo testing, but the terms most often used to describe them are precision and accuracy. Testing for precision and accuracy is performed often by clinical laboratory physicians. During the past decade, researchers have studied BNP testing methods for precision and accuracy (see Figure 1). Precision de- scribes the consistency or reproducibility between measurements of a physiologic instrument8 (see Table 1). An example of precision relates to a patient having a BNP level drawn and the sample divided in half. The method should provide the same BNP value from each sample from that particular patient. As previously mentioned, the IRMA method for BNP testing has been tested and found to be precise and accurate. Del Ry, Giannessi, and Clerico then compared the precision between the IRMA and Triage methods.7 To examine precision, the authors examined blood samples from 182 healthy adults to use as reference values. Because BNP was a new measurement, the “normal” value is still being debated; therefore, the authors had to establish a “normal” value for CI140409.qxd 10/28/2003 2:19 PM Vol. 14, No. 4 November 2003 Page 523 BRAIN NATRIURETIC PEPTIDE IN HEART FAILURE their samples. They identified this value by noting the range in the samples for both the Triage and the IRMA assay methods; a value above the 95th percentile was the cut-off for a normal range. When between assay imprecision or variability was measured, it was found that more variability exists using the Triage method than the IRMA method. In addition, the Triage method measured some samples with a reported “0” value while the IRMA method measured values up to 10 pg/mL. This finding suggested that Triage method had a lower sensitivity than the IRMA method at the low range and was somewhat less precise. Fortunately, BNP levels at the 0-10 pg/mL level have no clinical significance. The results of this study are consistent with others suggesting that the Triage method is less precise and more variable at low ranges than other methods, but provides useful information for therapy.9,10 Maisel and colleagues compared the Triage and RIA methods with patients in whom abnormal LV function was suspected.11 They hypothesized that BNP might predict abnormal LV function. Echocardiography was used to confirm suspected LV dysfunction and then compared to BNP levels. Interestingly, accuracy (as seen below) was reported in this study whereas precision was not. Accuracy of the Triage Method Del Ry, Giannessi, and Clerico also compared the accuracy between the IRMA and Triage methods.7 Accuracy is most often established by comparing the measured value to an accepted standard 8 (see Table 1). To establish the accuracy of the two methods, the investigators measured BNP levels in 37 normal adults and 37 adults with varying degrees of HF. They found a close linear relationship with the two methods at concentrations ranging from 0-1300 pg/mL. A Bland-Altman plot revealed that the IRMA method had better sensitivity at the lower range than the Triage method. A Bland-Altman plot is defined in Table 1, but briefly this plot compares the value of two measures to display the variability between the measures.12 In this case, there should be very little or no variability between the IRMA method and the Triage. Furthermore, similar 523 values were obtained in all subjects (patients with or without HF) using both methods. The mean BNP values found in healthy subjects using both methods were similar (10.3⫾11.6 pg/mL and 9.6⫾ 13.1 pg/mL, respectively). The mean BNP values in cardiac subjects were also similar (328.6⫾379.4pg/mL with the IRMA method and 344.2⫾369.1 pg/mL with the Triage method). These data suggest that both methods have similar power to discriminate between normal subjects and patients with HF. Maisel used the Triage method to compare BNP levels in those who were referred with suspected abnormal LV function.11 There were 105 patients with normal cardiac function and 95 patients with abnormal LV function identified by echocardiography. The mean BNP levels were 29.5 ⫾ 62.4 pg/mL and 489 ⫾ 75 pg/mL, respectively. The group difference was significant (p ⬍0.001). A value of 38.5pg/mL was 95% sensitive for the detection of LV dysfunction with a negative predictive value of 93%. A BNP of 75 pg/mL exhibited a 98% specificity, 98% positive predictive value, and 93% accuracy (see Table 1). BNP levels of ⬎100 pg/mL were seen in only 1% of those with normal heart function and 80% of those with abnormal function. These findings indicate that the Triage method is highly sensitive, specific, and selective in identifying those with abnormal LV dysfunction, which is a precursor to and/or indicator of HF. Biologic Variability and Brain Natriuretic Peptide There is strong evidence to suggest that BNP levels vary across certain patient conditions and diseases.5,13,14 Some patient conditions or characteristics such as gender and age are known to cause variations in BNP levels. Female gender is associated with higher BNP levels compared to males and BNP levels increase with age in both genders.13 These differences by age and gender appear to be even more pronounced when LV dysfunction is present or when the patient is on hormone replacement therapy.13,14 Redfield and colleagues13 found that plasma BNP was 21% higher in females on hormone replacement therapy (HRT) than in those not on CI140409.qxd 524 10/28/2003 2:19 PM Page 524 HOWIE ET AL AACN Clinical Issues TABLE 1 Biochemical Measurement Terms Term Definition Accuracy The difference between the measured value and the true value.32 Accuracy is most often established by comparing the measured value to a standard. In studies using nonphysiologic measures accuracy can be termed validity. Accuracy is partially determined by the sensitivity and specificity of the measure in physiologic measurements and using statistical measures.8 Diagnostic studies must be precise, ie, must find the same result upon repeat examination. A Bland-Altman plot will compare the differences between two measures using a plot (observation 1 vs observation 2). The closer the agreement between the two measures, the smaller the variation and the more precise the measure.12 Sources of error in physiologic measures. Error may be preanalytic, analytic and postanalytic.8 Describes the consistency or reproducibility between measurements made by a physiologic instrument.8 In studies using nonphysiologic measures, precision can be termed reliability. Precision is determined by utilizing Levy-Jenning’s charts, duplicate measures, mean absolute difference, imprecision profiles, and other methods. The precision profile is a valuable tool for analyzing assays. It allows researchers to judge assay precision quickly.33 The precision profile monitors precision, sensitivity and working range of an assay. It consists of three different curves on the same plot: 1) Within batch profile of the current assay, based on counting error of the samples, 2) Within batch precision profile of the current assay run, based on the replicate error of the sample, and 3) Between batch profile of all the previous assay runs, based on replicate error of the samples. This provides a graphical representation of amount of error inherent at various analyte concentrations. Two curves are plotted representing the error which allows determination of the working range of the assay. The researcher can also interpolate the estimated error (coefficient of variation) at any concentration value. The primary goal of a precision profile is to gain information about the random errors of measurement which leads to imprecision. Defines how sensitive and specific a measure is, but can only be used with dichotomous variables such as, with disease present vs without disease. It is a graphical way of observing an instrument. Sensitivity and specificity are plotted on a curve with the higher curve representing the more accurate measure.8 The probability that a patient with a given disease will have a positive test result, or the true positive rate.8 The probability that a patient without the disease will have a negative test result, or true negative rate.8 Bland-Altman Plot Error Precision Precision Profile Receiver Operating Characteristic Curves Sensitivity Specificity HRT using the Triage assay. However, using the IRMA assay, the difference was present but not significant. This difference in assay values suggests that there may be different normal values between the Triage and the IRMA assay methods. In addition, females and those on HRT may have higher normal values than males. Morrison and colleagues examined BNP levels in 321 patients who presented to an urgent care facility with dyspnea.15 While patients with HF had significantly higher BNP levels than those with pulmonary disease, BNP levels were ⬎200 pg/mL in several cases of pulmonary embolism secondary to in- creased right atrial and ventricular pressures.10,16 Further exploration of BNP levels in pulmonary embolism and other pulmonary diseases is needed. Biologic variability in BNP measurement will need exploration to determine if there are other factors that influence changes in levels such as cultural variations, medications, or genetic variations. Summary of Precision and Accuracy Studies to date suggest that the Triage method is a precise, accurate, and appropri- CI140409.qxd 10/28/2003 2:19 PM Vol. 14, No. 4 November 2003 Page 525 BRAIN NATRIURETIC PEPTIDE IN HEART FAILURE ate measure of BNP. A lower degree of precision and accuracy exists at low BNP levels, but this limitation has little clinical relevance. Accuracy is demonstrated with specificity and sensitivity levels all ⱖ82%. Researchers have reported increased levels of BNP with female gender and increasing age, suggesting that biologic variability exists.13 Future studies will need to address precision in the Triage method more closely. All future studies need to be completed on large samples with diversity in ethnicity, age, body position, fasting, time of day, assay method, genetic factors, and gender factors considered. Clinical Studies Utilizing Brain Natriuretic Peptide in Heart Failure Patients—The Emergency Department The clinical usefulness of BNP is beginning to be studied and appreciated. In the urgent care and emergency room setting, BNP levels have been obtained in patients presenting with dyspnea to identify HF. Dyspnea in the elderly patient with underlying medical problems such as chronic obstructive pulmonary disease (COPD) or other lung disease can suggest exacerbation of an existing medical problem or one of a multitude of possible problems. Echocardiography is the gold standard for verifying the diagnosis of HF but is expensive and not always readily accessible. In addition, echocardiography is technically difficult in severely dyspneic patients as well as in obese patients and those with obstructive lung diseases. In an early study Davis and colleagues17 assessed the diagnostic value of BNP in 52 patients who were admitted acutely to the hospital from the emergency room with dyspnea. They compared the BNP levels with LV ejection fraction, a standard indicator of LV function. Patients were either diagnosed with lung disease, HF, or both. Interestingly, severity of dyspnea was subjectively reported as similar in all patients. A comparison of the patients revealed that BNP had higher sensitivity and specificity in identifying HF than ejection fraction.17 As mentioned previously, Morrison and colleagues15 studied 321 dyspneic patients presenting to an ED to determine if BNP lev- 525 els could accurately differentiate CHF from pulmonary etiologies. A BNP value of 94 pg/mL had a sensitivity of 86% and specificity of 98% for differentiating CHF from pulmonary disease. Dao and colleagues 18 examined BNP levels in 250 patients presenting to an urgent care facility with dyspnea. Using the pointof-care Triage method, the authors sought to determine whether BNP had an impact on the diagnosis of HF. Patient records were reviewed retrospectively and BNP results were not known to reviewers. Patients with HF had significantly higher BNP levels than those with pulmonary or other conditions. Fifteen patients were incorrectly diagnosed at the time of their visit. Patients with HF had a mean BNP value of 1076 pg/mL. Had a cutoff value of 80 pg/mL been utilized, 29 of the 30 misdiagnosed patients would have been diagnosed correctly. In another ED study, researchers investigated utilizing the BNP level with other clinical information to establish or exclude the diagnosis of HF.19 This large multicenter study examined the baseline characteristics of dyspneic patients, including New York Heart Association (NYHA) class and BNP level. Investigators found that the best clinical predictor of HF was increased heart size on chest roentgenogram. Rales were the most accurate finding on physical examination. BNP values, however, were the single most accurate predictor of the presence or absence of HF. Amazingly, a BNP level >100 pg/mL was more accurate (83%) than either the National Health and Nutrition Examination Survey (NHANES) or Framingham criteria, the two most commonly used sets of criteria for diagnosing HF. In a large, multisite, international study examining dyspneic ED patients, knowledge of BNP value improved clinical diagnostic ability.20 In a group of patients where diagnosis was more difficult, BNP correctly identified 74% of patients and only misidentified 7%. BNP measurement discriminated between those with diastolic HF and obstructive lung disease, a distinction that remains challenging. In another study involving dyspneic patients, 26 NYHA class III patients were evaluated for LV systolic and diastolic dysfunction.21 Of those patients, 17 patients were diagnosed with COPD and 9 with dias- CI140409.qxd 526 10/28/2003 2:19 PM Page 526 HOWIE ET AL AACN Clinical Issues TABLE 2 Brain Natriuretic Peptide Levels in Emergency Department Patients With Dyspnea Author BNP Level Sensitivity Specificity Morrison et al: Utility of a rapid B-natriuretic peptide assay in differentiating congestive heart failure from lung disease in patients presenting with dyspnea15 Dao et al: Utility of B-type natriuretic peptide in the diagnosis of congestive heart failure18 Maisel et al: Rapid measurement of B-Type natriuretic peptide in the emergency diagnosis of heart failure19 Average BNP level in patients with CHF was 731 pg/mL BNP level of 94 pg/mL had 91% accuracy 86% (for BNP level of 94) 98% (for BNP level of 94) 1076 + 138 pg/mL in 98% (for BNP level of 80) patients with CHF BNP level of 80 pg/mL had 95% accuracy 675 + 450 pg/mL in 90% (for BNP level patients with CHF of >100) BNP level of 100pg/mL had 83.4% diagnostic accuracy BNP level > 100 pg/mL 94 % (for BNP level of had 81.5% accuracy >100) 92% (for BNP level of 80) McCullough et al: B-type natriuretic peptide and clinical judgment in emergency diagnosis of heart failure20 Cabanes et al: Brain natriuretic peptide blood levels in the differential diagnosis of dyspnea21 Davis et al: Plasma brain natriuretic peptide in assessment of acute dyspnea17 76% (for BNP level of >100) 70% (for BNP level of >100) 224 + 240 pg/mL found in patients with diastolic HF NR NR >22 pmol/L 93% 90% CHF, congestive heart failure; NR, not reported; pmol/L, picomols per liter. Picomols per liter cannot be compared pg/mL or picograms per milliliter. tolic HF. BNP levels were significantly higher in patients with diastolic HF when compared to those with COPD. A summary of these studies is presented in Table 2. Clinical Studies Using Brian Natriuretic Peptide in Patients With Heart Failure The Acute and Critical Care Setting While the studies above provide evidence that BNP levels are useful in diagnosing HF, investigators have also hypothesized that BNP may be valuable in guiding therapy in the acute setting. In a small study in the critical care setting, investigators hypothesized that levels of BNP would decline in association with falling wedge pressures.22 They asserted that the development of a simple and reliable method for assessment of filling pressures would provide a useful gauge for titration of therapy. Twenty patients with acutely decompensated HF and a wedge pressure of ⬎20mmHg were included. Investigators found that there was a significant correlation between percent change in wedge pressure from baseline to treatment and change in BNP level. In addition, dying patients had higher final BNP levels. The researchers suggested that BNP monitoring may be an effective way to improve the inhospital management of patients with acutely decompensated HF. In an effort to assess patient outcomes, 72 patients with acutely decompensated HF were studied.9 The investigators examined BNP levels upon admission and throughout the patients’ hospital stay with physicians blinded to BNP results. Patients who died or were readmitted had either no change or an increase in their BNP level during the course CI140409.qxd 10/28/2003 2:19 PM Vol. 14, No. 4 November 2003 Page 527 BRAIN NATRIURETIC PEPTIDE IN HEART FAILURE of hospitalization. Those patients with a successful outcome had a decline in their overall BNP level. These studies provide evidence that falling BNP values not only exhibit improving clinical condition but provide a useful method for titrating therapy. The Primary Care Setting Diagnosing HF in the primary care setting remains challenging as the symptoms are nonspecific and the clinical signs are not sensitive. 23 The diagnostic challenge is even greater in the early stages of HF. Monitoring BNP levels may help the clinician identify patients who are likely to have HF and require further clinical assessment and/or referral to a cardiologist. A population-based study examined the predictive value of BNP in 122 patients with a suspected new diagnosis of HF.16 Of the 122 patients referred, 35 (29%) were found to have HF based on the definition from the Working Group on HF of the European Society of Cardiology.24 Concentrations of BNP were significantly higher for those with HF. Brain natriuretic peptide values ⬎21.2pmol/L had sensitivity, specificity, and positive predictive values of 97%, 84%, and 70%, respectively. The authors concluded that BNP was a useful tool for determining which patients with suspected HF required further clinical assessment. In addition, another group of investigators evaluated the value of BNP to assess the severity of HF in a cardiology clinic.25 The researchers determined that plasma concentrations of BNP significantly increased in acute HF in relation to its severity. The Prognostic Value While the diagnostic value of BNP now appears undisputed, researchers are beginning to study its prognostic value. Readmission after hospitalization for HF is common, with an estimated 44% of Medicare patients experiencing rehospitalization at 6 months. 26 Having a tool for predicting rehospitalization, morbidity, and mortality events could provide useful information for patients, physicians, and nurses. Table 2 summarizes studies that have utilized BNP levels in patients with HF in an effort to assess prognosis. 527 Researchers have examined the utility of BNP as a method of risk stratifying HF patients for future cardiac events such as rehospitalization and mortality (see Table 2). As previously mentioned, 72 patients with acutely decompensated HF were studied prospectively to assess outcomes.9 The authors examined patient medical records at 30 days after discharge for readmission, or death, and measured BNP levels daily. BNP levels tended to increase during hospitalization in patients who were rehospitalized or died. In addition, univariate analysis revealed that the predischarge BNP level was strongly associated with outcomes. Also, discharge BNP levels of ⬍430 pg/mL had a strong negative predictive value for hospital readmission. Interestingly, although NYHA class improved in those who were readmitted to the hospital, there were only minimal decreases in BNP levels during hospitalization. Investigators have also examined survival in HF patients over the age of 65, comparing discharge BNP levels with future cardiac events.27 Their findings revealed that discharge BNP levels of ⬍132 pg/mL were associated with significantly fewer cardiac events than those with higher BNP levels. In a study examining HF patients over time, investigators assessed the prognostic power of BNP by following 78 stable HF clinic patients for a mean time of 398 days.28 A HF survival score (HFSS) was created based on a multivariable prognostic model. Results indicated that higher levels of BNP correlated with a high-risk HFSS and low BNP values correlated with a low HFSS score. BNP provided the ability to discriminate patients with chronic clinical events from patients without clinical events, with a cut-off value of 107.5 pg/mL, given a specificity of 75% and sensitivity of 88%. Berger et al29 evaluated the predictive value of BNP for determining sudden cardiac death in HF patients. During a 3-year period, 452 patients were followed. A total of 44 patients experienced cardiac death and in a multivariate model, BNP was the only independent predictor of sudden death. Selvais and colleagues25 also determined that BNP concentration was an independent predictor of prognosis in patients with HF. Patients with BNP values ⬎106 pg/mL had an increased risk of mortality. These studies provide evi- Description Findings Cheng et al: A Rapid Bedside Test for B-Type Peptide Predicts Treatment Outcomes in Patients Admitted for Decompensated HF: A Pilot Study9 2001 72 males NYHA class III patients admitted for decompensated HF; BNP levels measured daily; determined association between initial and pre-discharge BNP levels and subsequent adverse outcomes. BNP levels tended to increase during hospitalization in those who were rehospitalized or died; univariate analysis revealed that the predischarge BNP level was strongly associated with rehospitalization or mortality; in surviving patients, BNP levels were strong predictors of subsequent readmission; although NYHA class decreased in those who were readmitted to the hospital, there were only minimal decreases in BNP levels during hospitalization. Koglin et al: Role of BNP in Risk Stratification of Patients with Congestive HF28 2001 78 (69 males) BNP levels were obtained from HF clinic patients; clinical course followed for mean of 398 days. A risk stratification model provided a survival score (HRSS) and stratified patients into low-risk, medium-risk, and high-risk groups; BNP levels and HFSS showed a significant inverse correlation; a high HFSS indicating a low risk for adverse outcome was related to low BNP levels; changes in BNP levels were significantly related to changes in limitations in physical activity; a cut-off BNP value of 107.5 pg/mL was able to discriminate patients with, from those without, clinical events. Tamura et al: Prognostic Impact of Plasma BNP for Cardiac Events in Elderly Patients with Congestive HF27 2001 48 elderly Patients admitted for first episode HF; clinical characteristics, BNP, ejection fraction, left ventricular mass index were compared to patients without recurrent cardiac events. 12 cardiac events were observed; NYHA class was higher in patients with cardiac events than those without. BNP levels in those patients with cardiac events were significantly higher; cardiac event rate was significantly higher in those with BNP levels ⬎132pg/mL using Kaplan-Meier analysis. Berger et al: B-Type Natriuretic Peptide Predicts Sudden Death in Patients With Chronic HF29 2001 452 (57 females) BNP levels, clinical and hemodynamic variables in those with ejection fraction <35%; Patients without heart transplant or mechanical assist devices were followed for sudden cardiac death. Selvais et al: Cardiac Natriuretic Peptides for Diagnosis and Risk Stratification in HF: Influences of Left Ventricular Dysfunction and Coronary Artery Disease on Cardiac Hormonal Activation 25 1998 27 controls, 32 CAD 101 HF BNP, ANF, N-pro ANF, and LVEF were compared in all patients to evaluate the diagnostic ability, severity of HF and predict 2 year mortality. Sudden cardiac failure occurred in 44 patients (49%) and pump failure in 31 patients; 293 survived without transplant or device up to 3 years, 89 died, 65 had transplant, 14 died from other causes; in a multivariate model only log BNP level was an independent predictor of sudden death; using a cut-off point of log BNP <130 pg/mL, death-free survival rates were significantly higher (99%) in patients below compared with patients above (81%). Concentrations of ANF, N-proANF, and BNP increased in relation to HF severity; only N-proANF was able to distinguish between controls, CAD, and HF patients; BNP was able to distinguish HF severity; N-proANF and BNP were the best independent predictors of outcome and mortality. ANF, atrial natriuretic factor; N-proANF, atrial natriuretic factor prohormone; LVEF, left ventricular ejection fraction; CAD, coronary artery disease. Page 528 N 2:19 PM Year 10/28/2003 Author/Title CI140409.qxd TABLE 3 Studies of Brain Natriuretic Peptide (BNP) and Prognosis in Heart Failure (HF) CI140409.qxd 10/28/2003 2:19 PM Vol. 14, No. 4 November 2003 Page 529 BRAIN NATRIURETIC PEPTIDE IN HEART FAILURE dence that BNP levels can present predictive information about the course of HF. BNP for Everyone? Given the success of BNP measurements in primary and acute care, a reasonable question to ask is, “Should mass screenings for HF utilizing BNP be undertaken?” The results from the Framingham Heart Study indicate that BNP screening may not be helpful in this setting.30 In a large prospective cohort study, 3177 participants (1707 female) underwent testing to determine if BNP was a useful screening test for LV hypertrophy and systolic dysfunction. Each subject underwent echocardiography and venipuncture for BNP. Receiver operating characteristic curves (ROC) were obtained with echocardiography results plotted as the dependent variable and log BNP levels plotted as the independent variable. Briefly, ROC curves (see Table 1) plot sensitivity and specificity on a graph that defines the area under the curve (AUC). AUC is used to determine global test performance, with an AUC ⬍.5 indicating no discriminative ability. Overall, the ROC curves for elevated LV mass or systolic dysfunction were ⱕ.75, far below the desired high specificity level of .95. Of note, men and women were compared separately with men having higher discrimination than women. Thus, it appears that BNP is not appropriate as a mass screening test. Future Recommendations This review provides strong evidence that BNP measurements are a useful part of the diagnostic work-up for individual patients in a variety of settings. BNP levels are sensitive and specific for the diagnosis of abnormal heart function and HF. In addition, declining BNP levels appear to correlate with falling wedge pressures in acutely decompensated patients, with declining BNP levels better predictive outcomes. In the primary care setting, BNP levels might provide a useful indicator of which patients are likely to have HF and require further assessment. Future cardiac events may also be predicted by knowledge of BNP levels. Indeed, BNP levels may provide more useful information for the future 529 care of patients with HF than any other rapid diagnostic test. In 2001 the European Society of Cardiology convened a taskforce for the diagnosis and treatment of congestive HF.31 The group published guidelines stating that BNP levels can be helpful in the diagnostic process, especially in untreated patients. Patients suspected of having HF, especially in primary care, can be selected for further investigation if BNP levels are elevated. Epidemiological studies have demonstrated that BNP levels have a high predictive value (low rate of false positives), thereby improving the diagnostic work-up process. In addition, the guidelines also suggest that high levels of BNP identify those at risk for future cardiovascular events including death. Future studies are necessary to provide more information regarding cut-off points for normal, abnormal, and HF values in specific assays such as IRMA and Triage. Gender-specific studies are needed to further explore the normal values for women and those on HRT. Additional research should include larger sample sizes and be conducted in more diverse populations. Lastly, researchers need to focus on the predictive power of BNP and the possibility of developing admission and discharge criteria utilizing both clinical symptoms and BNP. As technology advances, BNP levels may reach the point of a very rapid assay, as in the measurement of blood glucose levels. Will BNP measures be feasible and helpful for patients in their own homes? If such a rapid assay is developed, will prehospital use be added to Advanced Cardiac Life Support? Will medical and nursing care of patients who are managed in skilled nursing homes be improved by BNP testing? Often, these patients are the most challenging to diagnose as they may not be able to describe symptoms because of dementia and they often have comorbidities that put them at risk for acute HF. A rapid assay may be able to provide information for diuretic therapy and fend off a hospitalization event. Conclusion The Triage method is desirable because it is rapid, convenient, and now shown to detect CI140409.qxd 530 10/28/2003 2:19 PM Page 530 HOWIE ET AL HF and abnormal LV dysfunction. Finding a blood test for HF that is precise and accurate would change the future for diagnosing and treating patients with HF. In a variety of settings such as the ED, cardiology clinic, primary care clinic, and the intensive care unit, BNP levels provide information regarding the presence of HF, severity, and resolution of acute exacerbation. Furthermore, several studies present beginning evidence that BNP levels at time of hospital discharge and over time provide predictive information regarding hospital readmission rates and mortality. References 1. American Heart Association (AHA). 2002 Heart and Stroke Statistical Update. Dallas, Tex: AHA; 2001. 2. Health Care Financing Review. Statistical Supplement. 2000. Rockville, Md: HCFA. 3. Maeda K, Tsutamoto T, Wada A, et al. Plasma brain natriuretic peptide as a biochemical marker of high left ventricular end-diastolic pressure in patients with symptomatic left ventricular dysfunction. Am Heart J. 1998;135: 825832. 4. Mizuno Y, Yoshimura M, Harada E, et al. Plasma levels of A- and B-type natriuretic peptides in patients with hypertrophic cardiomyopathy or idiopathic dilated cardiomyopathy. Am J Cardiol. 2000;86:1036-1040,A11. 5. Clerico A, Iervasi G, Del Chicca M, et al. Circulating levels of cardiac natriuretic peptides (ANP and BNP) measured by highly sensitive and specific immunoradiometric assays in normal subjects and in patients with different degrees of heart failure. J Endocrinol Invest. 1998;21:170-179. 6. Clerico A, Del Ry S, Giannessi D. Measurement of cardiac natriuretic hormones (atrial natriuretic peptide, brain natriuretic peptide, and related peptides) in clinical practice: the need for a new generation of immunoassay methods. Clin Chem. 2000;46:1529-1534. 7. Del Ry S, Giannessi D, Clerico A. Plasma brain natriuretic peptide measured by fullyautomated immunoassay and by immunoradiometric assay compared. Clin Chem Lab Med. 2001; 39:446-450. 8. DeKeyser F, Pugh L. (1991). Approaches to physiologic measurement. In Waltz C, Strickland O, Lenz E, eds. Measurement in Nursing Research (pp 387-412.). Philadelphia: FA Davis. 9. Cheng V, Kazanagra R, Garcia A, et al. A rapid bedside test for B-type peptide predicts AACN Clinical Issues treatment outcomes in patients admitted for decompensated heart failure: A pilot study. J Am Coll Cardiol. 2001;37:386-391. 10. Maisel A. B-type natriuretic peptide in the diagnosis and management of congestive heart failure. Cardiol Clin. 2001;19:557-571. 11. Maisel A, Koon J, Krishnaswamy P, et al. Utility of B-natriuretic peptide as a rapid, point of care test for screening patients undergoing echocardiography to determine left ventricular dysfunction. Am Heart J. 2001;141:367374. 12. Alasbimnjournal.9.2 Reviewing Literature: Basic advice for nuclear medicine technologists. 2002;18:1-5. Available: http://www2.alasbimnjournal.cl/alasbimn/CDA. Retrieved July 21, 2003. 13. Redfield M, Rodeheffer R, Jacobsen S, et al. Plasma brain natriuretic peptide concentration: Impact of age and gender. J Am Coll Cardiol. 2002;40:976-982. 14. Maffei S, Del Ry S, Prontera C, et al. Increase in circulating levels of cardiac natriuretic peptides after hormone replacement therapy in postmenopausal women. Clin Sci (Lond). 2001;101:447-453. 15. Morrison K, Harrison A, Krishnaswamy P, et al. Utility of a rapid B-natriuretic peptide assay in differentiating congestive heart failure from lung disease in patients presenting with dyspnea. J Am Coll Cardiol. 2002;39:202-209. 16. Cowie MR, Struthers AD, Wood DA, et al. Value of natriuretic peptides in assessment of patients with possible new heart failure in primary care. Lancet. 1997;350:1349-1353. 17. Davis M, Espiner E, Richards G, et al. Plasma brain natriuretic peptide in assessment of acute dyspnoea. Lancet. 1994;343:440-444. 18. Dao Q, Krishnaswamy P, Kazanegra R, et al. Utility of B-type natriuretic peptide in the diagnosis of congestive heart failure in an urgent-care setting. J Am Coll Cardiol. 2001;37: 379-385. 19. Maisel A, Krishnaswamy P, Nowak R, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. NEJM. 2002;347:161-167. 20. McCullough PA, Nowak RM, McCord J, et al. B-type natriuretic peptide and clinical judgment in emergency diagnosis of heart failure: Analysis From Breathing Not Properly (BNP) Multinational Study. Circulation. 2002;106: 416-422. 21. Cabanes L, Richaud-Thiriez B, Fulla Y, et al. Brain natriuretic peptide blood levels in the differential diagnosis of dyspnea. Chest. 2001; 120:2047-2050. 22. Kazanegra R, Cheng V, Garcia A, et al. A rapid test for B-type natriuretic peptide corre- CI140409.qxd 10/28/2003 2:19 PM Vol. 14, No. 4 November 2003 Page 531 BRAIN NATRIURETIC PEPTIDE IN HEART FAILURE lates with falling wedge pressures in patients treated for decompensated heart failure: A pilot study. J Card Fail. 2001;7:21-29. 23. Remes J, Miettinene H, Reunanen A, et al. Validity of clinical diagnosis of heart failure in primary health care. Eur Heart J. 1991;12:315-321. 24. The Task Force on Heart Failure of the European Society of Cardiology. Guidelines for the diagnosis of heart failure. Eur Heart J. 1995;16:741-751. 25. Selvais L, Donckier J, Robert A, et al. Cardiac natriuretic peptides for diagnosis and risk stratification in heart failure: influences of left ventricular dysfunction and coronary artery disease on cardiac hormonal activation. Eur J Clin Invest. 1998;28:636-642. 26. Krumholtz HM, Parent EM, Tu N, et al. Readmission after hospitalization for congestive heart failure among Medicare beneficiaries. Arch Intern Med. 1997;157:99-104. 27. Tamura K, Takahashi N, Nakatani Y, et al. Prognostic impact of plasma brain natriuretic peptide for cardiac events in elderly patients 531 with congestive heart failure. Gerontology. 2001;47:46-51. 28. Koglin J, Pehlivanli S, Schwaiblmair M, et al. Role of brain natriuretic peptide in risk stratification of patients with congestive heart failure. J Am Coll Cardiol. 2001;38:1934-1941. 29. Berger R, Huelsman M, Strecker K, et al. Btype natriuretic peptide predicts sudden death in patients with chronic heart failure. Circulation. 2002;105:2392-2397. 30. Vasan RS, Benjamin EJ, Larson MG, et al. Plasma natriuretic peptides for community screening for left ventricular hypertrophy and systolic dysfunction: The Framingham Heart Study. JAMA. 2002;288:1252-1259. 31. Remme WJ, Swedberg K. Guidelines for the diagnosis and treatment of chronic heart failure. Eur Heart J. 2001;22:1527-1560. 32. Wiess, M. (1973). Biomedical instrumentation. Philadelphia, Pa: Chilton Book Company. 33. Packard Instrument Company. Experpect QC: Precision Profile. Available: http://www. packardbioscience.com/pdf.appnotes/GN004 .pdf. Retrieved May 31, 2002.