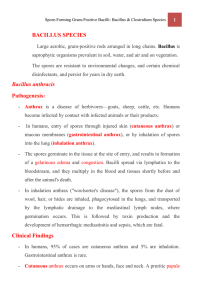
Chapter 11: Bacillus and Clostridium Species I. Bacillus Species A. General Characteristics • Gram-positive, spore-forming bacilli. • Found ubiquitously in nature (soil, water, air, and vegetation). • They survive extreme conditions due to spore formation. • Bacillus species include both non-pathogenic saprophytic organisms and highly virulent species. • Major pathogenic species: 1. Bacillus anthracis (anthrax) 2. Bacillus cereus (food poisoning and infections) B. Bacillus anthracis (Anthrax) 1. 2. 3. 4. Morphology and Identification o Size: Large bacilli, 1 × 3–4 µm. o Shape: Square ends, arranged in chains, with centrally located spores. o Capsule: Virulent strains produce a poly-γ-dglutamic acid capsule (antiphagocytic). Culture Characteristics o Colonies: Round, gray-white colonies with a “cut glass” appearance. o Hemolysis: Non-hemolytic on blood agar. o Motility: Non-motile (distinguishing feature from B. cereus). Pathogenesis and Virulence Factors o Anthrax Toxins: ▪ Protective Antigen (PA): Binds to receptors and forms a channel for toxin entry. ▪ Edema Factor (EF): Adenylate cyclase that increases cyclic AMP, causing edema. ▪ Lethal Factor (LF): Protease that disrupts immune response, leading to cell death. o Pathogenesis: Anthrax spores enter through the skin, mucosa, or lungs. Germination occurs, leading to local edema, followed by systemic spread and sepsis. Clinical Manifestations o Cutaneous Anthrax (95%): Begins as a papule, then forms a necrotic ulcer with a black eschar. Can cause sepsis if untreated. o Inhalational Anthrax: Flu-like symptoms, hemorrhagic mediastinitis, and septic shock. o Gastrointestinal Anthrax: Caused by ingestion of spores; severe abdominal pain, vomiting, bloody diarrhea. Injection Anthrax: Related to heroin users; characterized by extensive edema and septicemia. Laboratory Diagnosis o Microscopy: Large Gram-positive rods in chains. o Culture: Growth on blood agar with characteristic colonies. o Confirmation: PCR for toxin genes, immunofluorescence, or specific bacteriophage lysis. Treatment o First-line antibiotics: Ciprofloxacin, doxycycline, or penicillin. o For bioterrorism exposure: Ciprofloxacin or doxycycline for 60 days plus anthrax vaccine. o Antitoxins: Raxibacumab or Anthrax Immune Globulin (AIGIV) to neutralize toxins. Prevention o Vaccination: AVA BioThrax® for military personnel or high-risk individuals. o Control: Proper disposal of infected animal carcasses, use of protective clothing. o 5. 6. 7. C. Bacillus cereus 1. 2. 3. 4. 5. Overview o A common soil bacterium causing food poisoning and occasional infections in immunocompromised individuals. Food Poisoning o Emetic Form: ▪ Associated with improperly stored rice. ▪ Toxin causes nausea and vomiting 1–5 hours after ingestion. o Diarrheal Form: ▪ Associated with contaminated meat or vegetables. ▪ Toxin causes watery diarrhea and abdominal pain 8–16 hours after ingestion. Infections o Causes severe ocular infections, including endophthalmitis and keratitis. o Can cause systemic infections (meningitis, endocarditis, and bacteremia), particularly in immunocompromised patients. Diagnosis o Culture: Grows on blood agar with βhemolysis. o Microscopy: Gram-positive, motile rods. o Food poisoning diagnosis: Based on history of food consumption and toxin assays in food or stool. Treatment o o For food poisoning, treatment is supportive. Serious infections: Vancomycin, clindamycin, or ciprofloxacin. 2. II. Clostridium Species A. General Characteristics • Gram-positive, spore-forming bacilli. • Obligate anaerobes. • Commonly found in soil, marine sediments, sewage, and intestines of animals. • Highly virulent due to toxin production, causing diseases like tetanus, botulism, gas gangrene, and pseudomembranous colitis. B. Clostridium tetani (Tetanus) 1. 2. 3. 4. 5. 6. 7. Morphology and Identification o Gram-positive, motile rods with terminal spores (drumstick appearance). o Anaerobic growth. Toxin o Tetanospasmin: Neurotoxin that blocks release of inhibitory neurotransmitters (GABA, glycine), causing spastic paralysis. Pathogenesis o Spores enter through a wound and germinate in anaerobic conditions. o Toxin travels to the CNS, blocking inhibitory signals, leading to muscle spasms. Clinical Manifestations o Lockjaw (trismus), followed by muscle stiffness and spasms. o Generalized tetanus leads to severe muscle spasms and respiratory failure. Diagnosis o Based on clinical presentation and history of injury. o Isolation of C. tetani is not required for diagnosis. Treatment o Tetanus immune globulin (TIG) to neutralize unbound toxin. o Antibiotics: Penicillin or metronidazole. o Supportive care: Muscle relaxants, mechanical ventilation if necessary. Prevention o Vaccination with tetanus toxoid (part of DPT vaccine). o Booster doses every 10 years. 3. 4. 5. 6. 7. D. Clostridium perfringens 1. 2. 3. 4. C. Clostridium botulinum (Botulism) 1. Morphology and Identification Gram-positive rods, anaerobic, sporeforming. o Toxin-producing strains differentiated by toxin types (A-G). Botulinum Toxin o One of the most potent neurotoxins, blocks acetylcholine release at neuromuscular junctions, causing flaccid paralysis. Types of Botulism o Foodborne botulism: Ingestion of preformed toxin in improperly preserved food (canned, smoked, vacuum-packed). o Infant botulism: Ingestion of spores, often from honey, leading to toxin production in the gut. o Wound botulism: Contamination of wounds with spores, often seen in injection drug users. Clinical Manifestations o Symptoms begin 18–24 hours after toxin ingestion: double vision, difficulty swallowing, descending flaccid paralysis. o In infant botulism, signs include poor feeding and floppy baby syndrome. Diagnosis o Detection of toxin in serum, stool, or food via mouse bioassay or ELISA. o Culture of C. botulinum from clinical samples. Treatment o Antitoxin administration as soon as possible to neutralize circulating toxin. o Supportive care, including respiratory support (mechanical ventilation). Prevention o Proper food handling: Boil food for 20 minutes before consumption. o Avoid honey in infants under 1 year. o Gas Gangrene (Clostridial Myonecrosis) o C. perfringens is the most common cause of gas gangrene, characterized by rapid tissue destruction and gas formation. Pathogenesis o Spores enter through traumatic wounds. o Alpha toxin (lecithinase) destroys cell membranes, causing tissue necrosis. o Gas formation due to carbohydrate fermentation. Clinical Presentation o Severe pain, swelling, and crepitus in tissues. o Rapid progression to sepsis and shock. Diagnosis o Microscopy: Large Gram-positive rods. o Culture: Anaerobic growth with double zone hemolysis. 5. 6. Treatment o Surgical debridement is essential. o High-dose penicillin. o Hyperbaric oxygen therapy may be used to inhibit bacterial growth. Food Poisoning o Caused by enterotoxin-producing strains. o Symptoms: Diarrhea and abdominal cramps within 6–24 hours of ingestion. o Self-limiting, no specific treatment required. E. Clostridium difficile 1. 2. 3. 4. Pseudomembranous Colitis o Caused by overgrowth of C. difficile after antibiotic use. o Produces Toxin A (enterotoxin) and Toxin B (cytotoxin), leading to colonic inflammation and diarrhea. Clinical Manifestations o Watery diarrhea, fever, abdominal pain, and pseudomembranes in the colon. Diagnosis o Toxin detection in stool via ELISA or PCR. o Endoscopic findings: Pseudomembranes in the colon. Treatment o Discontinuation of the causative antibiotic. o First-line treatment: Metronidazole or vancomycin. o For recurrent infections: Fecal microbiota transplantation. Clinical Cases in Spore-Forming Gram-Positive Bacilli Case 1: Botulism A 35-year-old housewife living on a farm presents to the emergency department with the following symptoms: • Chief Complaints: Double vision and difficulty talking. • History: Symptoms began 2 hours ago, and she noticed a dry mouth and generalized weakness. The night before, she served home-canned green beans, which she tasted before boiling. None of the other family members are ill. Key Clinical Signs: • Neurological: Symmetrical descending paralysis affecting cranial nerves, upper extremities, and trunk. Diagnosis: • Botulism caused by ingestion of botulinum toxin in improperly canned food. Management: • Treatment: Immediate administration of botulinum antitoxin and supportive care, including mechanical ventilation if necessary. Learning Points: • Botulism presents as descending flaccid paralysis due to inhibition of acetylcholine release by the botulinum toxin. • Foodborne botulism is associated with improperly canned or preserved foods that allow spores of C. botulinum to germinate and produce toxins. Case 2: Gas Gangrene (Clostridium perfringens) III. Key Concepts Summary • • • • Bacillus species are aerobic, spore-forming bacteria, with Bacillus anthracis causing anthrax and Bacillus cereus causing food poisoning. Clostridium species are anaerobic, spore-forming bacteria that cause diseases through potent exotoxins, including C. tetani (tetanus), C. botulinum (botulism), C. perfringens (gas gangrene), and C. difficile (pseudomembranous colitis). Diagnosis often involves identifying the organism in clinical specimens or detecting toxins. Prevention includes vaccination (e.g., tetanus), proper food handling (botulism), and careful antibiotic use (C. difficile). A young man sustains major soft tissue injury and open fractures of his right leg in a motorcycle accident. One day later, he develops the following symptoms: • Chief Complaints: Fever (38°C), increased heart rate, sweating, and restlessness. • Physical Examination: The leg is swollen and tense, with dark serous fluid draining from the wounds. The skin is cool, pale, and shiny. Crepitus is present (indicating gas formation in tissues). Key Clinical Signs: • Hematocrit is 20% (50% of normal), and circulating hemoglobin is normal. Serum shows free hemoglobin. Diagnosis: • Gas gangrene caused by Clostridium perfringens, based on clinical presentation and crepitus (gas formation) in the tissues. Hemolysis: • Hemolysis in this patient is likely due to the action of lecithinase (alpha toxin) produced by C. perfringens, which lyses cell membranes and causes tissue necrosis. Management: • Emergency surgical debridement to remove necrotic tissue. • High-dose penicillin and possibly hyperbaric oxygen therapy to inhibit bacterial growth. Learning Points: • Gas gangrene is a rapidly progressing, life-threatening infection characterized by myonecrosis and gas production. Early surgical intervention is essential to prevent further tissue destruction and systemic sepsis. Management: • Treatment: Supportive care for symptoms, which typically resolve within 24 hours. Learning Points: • B. cereus food poisoning has two distinct forms: emetic (associated with fried rice) and diarrheal (associated with contaminated meat dishes). The emetic form is caused by a heat-stable toxin that induces rapid-onset vomiting. Case 5: Tetanus (Clostridium tetani) Case 3: Anthrax A bioterrorism event results in 22 cases of anthrax, 11 of which are inhalational and 11 are cutaneous. Among the inhalational cases, five patients die. Symptoms in these patients included: • Chief Complaints: Flu-like symptoms initially, followed by substernal chest pain, cough, and difficulty breathing. • Physical Examination: Hemorrhagic pleural effusions, pronounced mediastinal widening (visible on chest X-rays), and rapidly progressing sepsis. Diagnosis: • Inhalational anthrax, caused by inhalation of Bacillus anthracis spores, based on clinical presentation and history of bioterrorism exposure. Pathogenesis: • Lethal toxin (LF) and edema toxin (EF), combined with protective antigen (PA), cause extensive hemorrhagic mediastinitis and sepsis, which are often fatal. Management: • Early antibiotic treatment with ciprofloxacin or doxycycline. • Post-exposure prophylaxis for those at risk, including 60 days of antibiotic therapy and three doses of anthrax vaccine. Learning Points: • Inhalational anthrax is rare but highly fatal, especially if diagnosis and treatment are delayed. Rapid progression to sepsis and hemorrhagic mediastinitis are hallmark features. A 45-year-old man who immigrated to the U.S. 5 years ago presents with muscle spasms, particularly in his right leg, following a puncture wound from a lawn mower injury. Symptoms progressed over several days, and by day 8, he was unable to open his jaw (lockjaw). Key Clinical Signs: • Generalized muscle spasms triggered by stimuli (e.g., loud noises). Diagnosis: • Tetanus, caused by C. tetani, based on clinical presentation and recent puncture wound. Pathogenesis: • The tetanospasmin toxin produced by C. tetani blocks release of inhibitory neurotransmitters (GABA and glycine), leading to spastic paralysis. Management: • Tetanus immune globulin (TIG) to neutralize unbound toxin. • Antibiotics (penicillin or metronidazole) to clear the infection. • Supportive care: Sedation and muscle relaxants, and possible mechanical ventilation. Learning Points: • Tetanus presents with muscle stiffness, lockjaw, and generalized spasms. Tetanospasmin blocks inhibitory neurotransmitter release, resulting in uncontrolled muscle contractions. Review Questions from Clinical Cases 5. Case 4: Food Poisoning (Bacillus cereus) A food commonly associated with Bacillus cereus food poisoning is fried rice. The patient, a 30-year-old woman, presents with the following symptoms after consuming fried rice at a restaurant: • Chief Complaints: Nausea, vomiting, and abdominal cramps that began 2 hours after eating. Diagnosis: • Bacillus cereus food poisoning, emetic form, based on the short incubation period (1–5 hours) and ingestion of improperly stored fried rice. 6. 7. Botulism Case: What is the most likely cause of the symmetrical descending paralysis? o Answer: Botulism (caused by ingestion of botulinum toxin). Gas Gangrene Case: Which microorganism is responsible for the hemolysis and gas production in the wound? o Answer: Clostridium perfringens, producing alpha toxin (lecithinase). Anthrax Case: What is the recommended postexposure prophylaxis for inhalational anthrax in a bioterrorism event? Answer: Ciprofloxacin or doxycycline for 60 days, plus vaccination. Bacillus cereus Case: What food is most commonly associated with the emetic form of Bacillus cereus food poisoning? o Answer: Fried rice. Tetanus Case: What neurotransmitters are blocked by tetanus toxin, leading to spastic paralysis? o Answer: Glycine and γ-aminobutyric acid (GABA). o 8. 9. Flashcards Bacillus Species: General Characteristics Flashcard 1 Q: What are the general characteristics of Bacillus species? A: Bacillus species are large, Gram-positive, spore-forming rods that are aerobic or facultatively anaerobic, commonly found in soil, water, and vegetation. Flashcard 2 Q: Name the two most clinically significant Bacillus species. A: Bacillus anthracis (causes anthrax) and Bacillus cereus (causes food poisoning and infections). Bacillus anthracis: Morphology and Identification Flashcard 3 Q: Describe the morphology of Bacillus anthracis. A: Bacillus anthracis is a large, Gram-positive bacillus with square ends, arranged in chains, and forms central spores. Virulent strains are encapsulated with a poly-γ-d-glutamic acid capsule. Flashcard 4 Q: What is the appearance of Bacillus anthracis colonies on blood agar? A: Non-hemolytic, gray-white colonies with a “ground-glass” appearance. Flashcard 5 Q: Is Bacillus anthracis motile? A: No, Bacillus anthracis is non-motile, which helps differentiate it from Bacillus cereus. Bacillus anthracis: Pathogenesis and Virulence Factors Flashcard 6 Q: What are the three main components of the anthrax toxin? A: Protective Antigen (PA), Edema Factor (EF), and Lethal Factor (LF). Flashcard 7 Q: How does Protective Antigen (PA) function in anthrax pathogenesis? A: PA binds to host cell receptors and forms a channel through which Edema Factor (EF) and Lethal Factor (LF) enter the cell. Flashcard 8 Q: What does Edema Factor (EF) do in anthrax infections? A: EF is an adenylate cyclase that increases cyclic AMP, causing cell edema and fluid accumulation. Flashcard 9 Q: What role does Lethal Factor (LF) play in anthrax? A: LF is a protease that disrupts immune cell signaling, leading to cell death and contributing to systemic shock and death. Bacillus anthracis: Clinical Manifestations Flashcard 10 Q: What are the four types of anthrax in humans? A: Cutaneous anthrax, inhalational anthrax, gastrointestinal anthrax, and injection anthrax. Flashcard 11 Q: What is the most common form of anthrax, and what are its symptoms? A: Cutaneous anthrax (95% of cases) begins as a pruritic papule, progresses to a vesicle, and forms a black eschar surrounded by edema. Without treatment, it can lead to sepsis. Flashcard 12 Q: Describe the progression of inhalational anthrax. A: Inhalational anthrax starts with flu-like symptoms, then progresses to hemorrhagic mediastinitis, pleural effusion, and sepsis, leading to rapid death. Flashcard 13 Q: What is gastrointestinal anthrax? A: Gastrointestinal anthrax occurs after ingestion of spores, leading to severe abdominal pain, vomiting, bloody diarrhea, and possible sepsis. Flashcard 14 Q: What is injection anthrax, and who is at risk? A: Injection anthrax occurs in drug users who inject contaminated heroin. It causes painless, extensive subcutaneous edema, progressing to septicemia. Bacillus anthracis: Diagnosis and Treatment Flashcard 15 Q: How is anthrax diagnosed in the lab? A: Diagnosis is based on Gram-stained smears (showing large Gram-positive rods in chains), culture on blood agar (nonhemolytic, ground-glass colonies), and PCR for toxin genes. Flashcard 16 Q: What are the first-line antibiotics for treating anthrax? A: Ciprofloxacin or doxycycline, usually combined with additional antibiotics for severe cases. Flashcard 17 Q: What antitoxins are used in the treatment of anthrax? A: Raxibacumab (a monoclonal antibody) and Anthrax Immune Globulin (AIGIV), which neutralize anthrax toxins. Flashcard 18 Q: What is the anthrax vaccine, and who should receive it? A: The anthrax vaccine (AVA BioThrax®) is given to military personnel, lab workers, and others at high risk of exposure to Bacillus anthracis. Flashcard 27 Q: What are the four major diseases caused by Clostridium species? A: Tetanus, botulism, gas gangrene, and pseudomembranous colitis. Bacillus cereus: Pathogenesis and Clinical Manifestations Flashcard 19 Q: What are the two types of food poisoning caused by Bacillus cereus? A: Emetic type (vomiting) and diarrheal type. Clostridium tetani: Pathogenesis and Clinical Manifestations Flashcard 28 Q: What is the primary toxin produced by Clostridium tetani, and what is its effect? A: Tetanospasmin, a neurotoxin that blocks the release of inhibitory neurotransmitters (GABA and glycine), causing spastic paralysis. Flashcard 20 Q: What foods are commonly associated with the emetic form of Bacillus cereus food poisoning? A: Fried rice that has been improperly stored. Flashcard 29 Q: How do Clostridium tetani spores enter the body? A: Through a puncture wound or trauma, especially in areas with low oxygen tension. Flashcard 21 Q: What are the symptoms of the emetic form of Bacillus cereus food poisoning? A: Nausea and vomiting within 1–5 hours after consuming the contaminated food. Flashcard 30 Q: What are the key symptoms of tetanus? A: Muscle stiffness, lockjaw (trismus), generalized muscle spasms, and respiratory failure. Flashcard 22 Q: What foods are commonly associated with the diarrheal form of Bacillus cereus food poisoning? A: Meat dishes, sauces, and vegetables. Flashcard 23 Q: What are the symptoms of the diarrheal form of Bacillus cereus food poisoning? A: Profuse diarrhea, abdominal pain, and cramps occurring 8– 16 hours after ingestion. Bacillus cereus: Infections and Treatment Flashcard 24 Q: Apart from food poisoning, what other infections can Bacillus cereus cause? A: Severe eye infections (keratitis, endophthalmitis), wound infections, meningitis, and catheter-associated bacteremia. Flashcard 25 Q: What is the treatment for serious Bacillus cereus infections? A: Vancomycin, clindamycin, or ciprofloxacin for systemic infections. For food poisoning, supportive care is typically sufficient. Clostridium Species: General Characteristics Flashcard 26 Q: What are the general characteristics of Clostridium species? A: Clostridium species are large, Gram-positive, spore-forming bacilli that are obligate anaerobes and produce a variety of toxins. They are found in soil, marine sediments, sewage, and the intestines of animals and humans. Clostridium tetani: Diagnosis and Treatment Flashcard 31 Q: How is tetanus diagnosed? A: Tetanus is diagnosed based on clinical presentation and history of a wound. Laboratory confirmation is not necessary. Flashcard 32 Q: What is the treatment for tetanus? A: Tetanus immune globulin (TIG) to neutralize toxin, antibiotics (penicillin or metronidazole), wound debridement, and supportive care such as muscle relaxants and mechanical ventilation if necessary.