- No category
Retinoids in Dermatology: Mechanisms, Effects, and Side Effects
advertisement
Retinoids in Dermatology Series in Dermatological Treatment About the Series Published in association with the Journal of Dermatological Treatment, the Series in Dermatological Treatment keeps readers up to date with the latest clinical therapies to improve problems with the skin, hair, and nails. Each volume in the series is prepared separately and typically focuses on a topical theme. Volumes are published on an occasional basis, depending on the emergence of new developments. Retinoids in Dermatology Ayse Serap Karadag, Berna Aksoy, and Lawrence Charles Parish Facial Skin Disorders Ronald Marks Dermatologic Reactions to Cancer Therapies Gabriella Fabbrocini, Mario E. Lacouture, and Antonella Tosti Acne Scars: Classification and Treatment, Second Edition Antonella Tosti, Maria Pia De Padova, Gabriella Fabbrocini, and Kenneth Beer Phototherapy Treatment Protocols, Third Edition Steven R. Feldman and Michael D. Zanolli Dermatoscopy in Clinical Practice: Beyond Pigmented Lesions, Second Edition Giuseppe Micali and Francesco Lacarrubba Nail Surgery Bertrand Richert, Nilton Di Chiacchio, and Eckart Haneke Abdominal Stomas and Their Skin Disorders, Second Edition Callum C. Lyon and Amanda Smith Textbook of Atopic Dermatitis Sakari Reitamo, Thomas A. Luger, and Martin Steinhoff For more information about this series please visit: https://www.crcpress.com/ Series-in-Dermatological-Treatment/book-series/CRCSERDERTRE Retinoids in Dermatology Edited by Ayse Serap Karadag, MD Department of Dermatology Istanbul Medeniyet University Faculty of Medicine Göztepe Training and Research Hospital Istanbul, Turkey Berna Aksoy, MD Department of Dermatology Bahçeşehir University Faculty of Medicine Istanbul, Turkey Lawrence Charles Parish, MD, MD (Hon) Department of Dermatology and Cutaneous Biology Sidney Kimmel Medical College at Thomas Jefferson University and Jefferson Center for International Dermatology Philadelphia, Pennsylvania, USA CRC Press Taylor & Francis Group 6000 Broken Sound Parkway NW, Suite 300 Boca Raton, FL 33487-2742 © 2020 by Taylor & Francis Group, LLC CRC Press is an imprint of Taylor & Francis Group, an Informa business No claim to original U.S. Government works Printed on acid-free paper International Standard Book Number-13: 978-1-138-31477-1 (Hardback) This book contains information obtained from authentic and highly regarded sources. While all reasonable efforts have been made to publish reliable data and information, neither the author[s] nor the publisher can accept any legal responsibility or liability for any errors or omissions that may be made. The publishers wish to make clear that any views or opinions expressed in this book by individual editors, authors or contributors are personal to them and do not necessarily reflect the views/opinions of the publishers. The information or guidance contained in this book is intended for use by medical, scientific or health-care professionals and is provided strictly as a supplement to the medical or other professional’s own judgement, their knowledge of the patient’s medical history, relevant manufacturer’s instructions and the appropriate best practice guidelines. Because of the rapid advances in medical science, any information or advice on dosages, procedures or diagnoses should be independently verified. The reader is strongly urged to consult the relevant national drug formulary and the drug companies’ and device or material manufacturers’ printed instructions, and their websites, before administering or utilizing any of the drugs, devices or materials mentioned in this book. This book does not indicate whether a particular treatment is appropriate or suitable for a particular individual. Ultimately it is the sole responsibility of the medical professional to make his or her own professional judgements, so as to advise and treat patients appropriately. The authors and publishers have also attempted to trace the copyright holders of all material reproduced in this publication and apologize to copyright holders if permission to publish in this form has not been obtained. If any copyright material has not been acknowledged please write and let us know so we may rectify in any future reprint. Except as permitted under U.S. Copyright Law, no part of this book may be reprinted, reproduced, transmitted, or utilized in any form by any electronic, mechanical, or other means, now known or hereafter invented, including photocopying, microfilming, and recording, or in any information storage or retrieval system, without written permission from the publishers. For permission to photocopy or use material electronically from this work, please access www.copyright.com (http://www.copyright.com/) or contact the Copyright Clearance Center, Inc. (CCC), 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400. CCC is a not-for-profit organization that provides licenses and registration for a variety of users. For organizations that have been granted a photocopy license by the CCC, a separate system of payment has been arranged. Trademark Notice: Product or corporate names may be trademarks or registered trademarks, and are used only for identification and explanation without intent to infringe. Library of Congress Cataloging-in-Publication Data Names: Karadag, Ayse Serap, editor. | Aksoy, Berna, editor. | Parish, Lawrence Charles, editor. Title: Retinoids in dermatology / edited by Ayse Serap Karadag, Berna Aksoy, Lawrence Charles Parish. Other titles: Series in dermatological treatment. Identifiers: LCCN 2019034117 (print) | LCCN 2019034118 (ebook) | ISBN 9781138314771 (hardback ; alk. paper) | ISBN 9780429456732 (ebook) Subjects: MESH: Skin Diseases--drug therapy | Retinoids--therapeutic use | Retinoids--pharmacology Classification: LCC RL120.R48 (print) | LCC RL120.R48 (ebook) | NLM WR 650 | DDC 616.5/061--dc23 LC record available at https://lccn.loc.gov/2019034117 LC ebook record available at https://lccn.loc.gov/2019034118 Visit the Taylor & Francis Web site at http://www.taylorandfrancis.com and the CRC Press Web site at http://www.crcpress.com Contents Contributors vii 1. The Background of Retinoids........................................................................................................................................................1 Ayse Serap Karadag, Berna Aksoy, and Lawrence Charles Parish 2. Mechanism of Action of Vitamin A...............................................................................................................................................3 Sandra Maria Barbalho 3. Mechanism of Action of Topical Retinoids...................................................................................................................................7 Sümeyre Seda Ertekin and Mehmet Salih Gurel 4. Mechanism of Action of Isotretinoin...........................................................................................................................................13 Bodo C. Melnik 5. Mechanism of Action of Acitretin................................................................................................................................................27 Kaitlyn Lam and Ronald Vender 6. Mechanism of Action of Bexarotene............................................................................................................................................33 Catherine M. Ludwig, Claire Wilson, Brandon Roman, and Maria M. Tsoukas 7. Mechanism of Action of Alitretinoin...........................................................................................................................................37 Ömer Faruk Elmas and Necmettin Akdeniz 8. Effects of Retinoids at the Cellular Level (Differentiation, Apoptosis, Autophagy, Cell Cycle Regulation, and Senescence)............................................................................................................................................................................. 41 Jelena Popovic 9. Effects of Retinoids at the Systemic Level.................................................................................................................................. 51 Sandra Maria Barbalho and Letícia Maria Pescinini-Salzedas 10. New Aspects of Isotretinoin Teratogenicity................................................................................................................................55 Bodo C. Melnik 11. Mucocutaneous Side Effects......................................................................................................................................................... 61 Tugba Kevser Uzuncakmak and Ayse Serap Karadag 12. Ophthalmologic Side Effects........................................................................................................................................................67 Remzi Karadag and Fehim Esen 13. Musculoskeletal Side Effects........................................................................................................................................................73 Filiz Cebeci Kahraman, Vefa Aslı Turgut Erdemir, and Melek Aslan Kayıran 14. Neurologic Side Effects.................................................................................................................................................................79 Evren Burakgazi-Dalkilic 15. Psychiatric Side Effects.................................................................................................................................................................83 Joshua Schimmel, Evren Burakgazi-Dalkilic, and Hatice Burakgazi-Yilmaz 16. Gastrointestinal Side Effects........................................................................................................................................................89 Esra Adışen, Burcu Beksaç, and Mehmet Ali Gürer 17. Endocrine and Metabolic Side Effects........................................................................................................................................93 Ayse Serap Karadag, Emin Ozlu, and Bodo C. Melnik v vi Contents 18. Other Systemic Side Effects: Cardiovascular, Pulmonary, Otolaryngorhinologic, Genitourinary, Renal, and Immunologic................................................................................................................................................................................ 105 Emin Ozlu, Akif Bilgen, and Ayse Serap Karadag 19. Retinoids in Acne......................................................................................................................................................................... 111 Ruta Ganceviciene and Christos C. Zouboulis 20. Retinoids in Hidradenitis Suppurativa/Acne Inversa.............................................................................................................. 121 Uwe Wollina, Piotr Brzezinski, and André Koch 21. Retinoids in Rosacea...................................................................................................................................................................125 Marius Rademaker and Harriet Cheng 22. Retinoids in Hair Disorders.......................................................................................................................................................129 Brent J. Doolan and Rodney Sinclair 23. Retinoids in Psoriasis.................................................................................................................................................................. 135 Uwe Wollina, Piotr Brzezinski, and André Koch 24. Retinoids in Keratinization Disorders...................................................................................................................................... 145 Ümit Türsen and Belma Türsen 25. Retinoids in Antiaging Therapy................................................................................................................................................. 157 Zehra Aşiran Serdar and Ezgi Aktaş Karabay 26. Retinoids in Other Skin Diseases............................................................................................................................................... 163 Uwe Wollina, Piotr Brzezinski, and André Koch 27. Retinoids in Lymphoma.............................................................................................................................................................. 171 Robert Duffy and Joya Sahu 28. Retinoids in Cutaneous Chemoprophylaxis............................................................................................................................. 177 Robert Duffy and Joya Sahu 29. Guide to Good Clinical Practice for Vulnerable Populations (Infancy, Childhood, Fertile Period, Elderly)................... 183 Elif Yildirim and Berna Aksoy 30. Retinoids and Concomitant Surgery......................................................................................................................................... 189 H. Mete Aksoy 31. Retinoids and Concomitant Aesthetic Procedures..................................................................................................................197 Zekayi Kutlubay, Ayşegül Sevim Keçici, and Yalçın Tüzün 32. Laboratory and Clinical Follow-Up..........................................................................................................................................201 Nadide Burcu Öztürk and Berna Aksoy 33. Teratogenicity and Registry Programs.....................................................................................................................................207 Reese L. Imhof and Megha M. Tollefson 34. Management of Vitamin A and Retinoid Side Effects............................................................................................................ 213 Asli Tatliparmak and Berna Aksoy 35. Future and Novel Unexplored Indications of Retinoids.......................................................................................................... 217 Kabir Sardana and Ananta Khurana Index.....................................................................................................................................................................................................227 Contributors Esra Adışen Department of Dermatology Gazi University Faculty of Medicine Ankara, Turkey Evren Burakgazi-Dalkilic Department of Neurology Cooper Medical School of Rowan University Cooper University Hospital Camden, New Jersey Necmettin Akdeniz Department of Dermatology Istanbul Medeniyet University Faculty of Medicine Göztepe Training and Research Hospital Istanbul, Turkey Hatice Burakgazi-Yilmaz Department of Psychiatry Cooper Medical School of Rowan University Cooper University Hospital Camden, New Jersey Berna Aksoy Department of Dermatology Bahçeşehir University Faculty of Medicine Istanbul, Turkey H. Mete Aksoy Department of Plastic, Reconstructive, and Aesthetic Surgery Bahçeşehir University Faculty of Medicine Istanbul, Turkey Sandra Maria Barbalho Department of Biochemistry and Nutrition School of Medicine University of Marília Faculty of Food Technology of Marília São Paulo, Brazil Burcu Beksaç Department of Dermatology Gülhane Research and Training Hospital Ankara, Turkey Akif Bilgen Department of Otolaryngology, Head and Neck Surgery Health Science University Ankara Training and Research Hospital Ankara, Turkey Piotr Brzezinski Department of Dermatology Institute of Biology and Environmental Protection Pomeranian Academy Slupsk, Poland and 6th Military Support Unit Ustka, Poland Harriet Cheng Department of Dermatology Auckland City Hospital Auckland, New Zealand Brent J. Doolan The Royal Children’s Hospital Skin & Cancer Foundation Inc. The Royal Melbourne Hospital Melbourne, Australia Robert Duffy Department of Dermatology and Cutaneous Biology Thomas Jefferson University Philadelphia, Pennsylvania Ömer Faruk Elmas Department of Dermatology Ahi Evran University Faculty of Medicine Kırşehir, Turkey Vefa Aslı Turgut Erdemir Department of Dermatology Istanbul Medeniyet University Faculty of Medicine Göztepe Training and Research Hospital Istanbul, Turkey Sümeyre Seda Ertekin Department of Dermatology Aksaray University Faculty of Medicine Training and Research Hospital Aksaray, Turkey Fehim Esen Department of Ophthalmology Istanbul Medeniyet University Faculty of Medicine Istanbul, Turkey vii viii Ruta Ganceviciene Departments of Dermatology, Venereology, Allergology, and Immunology Dessau Medical Center Brandenburg Medical School Theodor Fontane Dessau, Germany Mehmet Salih Gurel Department of Dermatology Istanbul Medeniyet University Faculty of Medicine Göztepe Training and Research Hospital Istanbul, Turkey Mehmet Ali Gürer Department of Dermatology Gazi University Faculty of Medicine Ankara, Turkey Reese L. Imhof Mayo Clinic School of Medicine Rochester, Minnesota Filiz Cebeci Kahraman Department of Dermatology Istanbul Medeniyet University Faculty of Medicine Göztepe Training and Research Hospital Istanbul, Turkey Ezgi Aktaş Karabay Department of Dermatology Bahçeşehir University Faculty of Medicine Istanbul, Turkey Ayse Serap Karadag Department of Dermatology Istanbul Medeniyet University Faculty of Medicine Göztepe Training and Research Hospital Istanbul, Turkey Remzi Karadag Department of Ophthalmology Istanbul Medeniyet University Faculty of Medicine Göztepe Training and Research Hospital Istanbul, Turkey Melek Aslan Kayıran Department of Dermatology Istanbul Medeniyet University Faculty of Medicine Göztepe Training and Research Hospital Istanbul, Turkey Contributors Ayşegül Sevim Keçici Department of Dermatology University of Medical Sciences Haydarpaşa Numune Training and Research Hospital Istanbul, Turkey Ananta Khurana Department of Dermatology Post Graduate Institute of Medical Education and Research Dr RML Hospital Delhi, India André Koch Department of Dermatology and Allergology Städtisches Klinikum Dresden Academic Teaching Hospital of the Technical University of Dresden Dresden, Germany Zekayi Kutlubay Department of Dermatology Istanbul University Faculty of Medicine Cerrahpaşa Faculty of Medicine Istanbul, Turkey Kaitlyn Lam MD Program University of Toronto Faculty of Medicine Toronto, Ontario, Canada Catherine M. Ludwig University of Illinois College of Medicine Chicago, Illinois Bodo C. Melnik Department of Dermatology, Environmental Medicine and Health Theory University of Osnabrück Osnabrück, Germany Emin Ozlu Department of Dermatology Düzce University Faculty of Medicine Düzce, Turkey Nadide Burcu Öztürk Department of Dermatology Private Practice Kocaeli, Turkey Lawrence Charles Parish Department of Dermatology and Cutaneous Biology Sidney Kimmel Medical College at Thomas Jefferson University and Jefferson Center for International Dermatology Philadelphia, Pennsylvania ix Contributors Letícia Maria Pescinini-Salzedas School of Medicine Department of Pharmacology University of Marília São Paulo, Brazil Jelena Popovic Laboratory for Human Molecular Genetics Institute of Molecular Genetics and Genetic Engineering University of Belgrade Belgrade, Serbia Marius Rademaker Waikato Clinical School School of Medicine University of Auckland Auckland, New Zealand Brandon Roman University of Illinois College of Medicine Chicago, Illinois Joya Sahu Pathology and Hematology Oncology Cutaneous Lymphoma Multidisciplinary Center Sidney Kimmel Medical College at Thomas Jefferson University Philadelphia, Pennsylvania Kabir Sardana Department of Dermatology Post Graduate Institute of Medical Education and Research Dr RML Hospital Delhi, India Megha M. Tollefson Department of Dermatology Mayo Clinic Rochester, Minnesota Maria M. Tsoukas Department of Dermatology University of Illinois College of Medicine Chicago, Illinois Belma Türsen Department of Dermatology Private Practice Mersin, Turkey Ümit Türsen Department of Dermatology Mersin University Faculty of Medicine Mersin, Turkey Yalçın Tüzün Department of Dermatology Medical Park Hospital Istanbul, Turkey Tugba Kevser Uzuncakmak Department of Dermatology Istanbul Medeniyet University Faculty of Medicine Istanbul, Turkey Ronald Vender MD Program University of Toronto Faculty of Medicine Toronto, Ontario, Canada Joshua Schimmel Cooper Medical School of Rowan University Camden, New Jersey Claire Wilson University of Illinois College of Medicine Chicago, Illinois Zehra Aşiran Serdar Department of Dermatology Bahçeşehir University Faculty of Medicine Istanbul, Turkey Uwe Wollina Department of Dermatology and Allergology Städtisches Klinikum Dresden Academic Teaching Hospital of the Technical University of Dresden Dresden, Germany Rodney Sinclair Department of Medicine University of Melbourne Epworth Dermatology Sinclair Dermatology Melbourne, Australia Elif Yildirim Department of Dermatology Sanko University Faculty of Medicine Gaziantep, Turkey Asli Tatliparmak Department of Dermatology Bahçeşehir University Faculty of Medicine Istanbul, Turkey Christos C. Zouboulis Departments of Dermatology, Venereology, Allergology, and Immunology Dessau Medical Center Brandenburg Medical School Theodor Fontane Dessau, Germany 1 The Background of Retinoids Ayse Serap Karadag, Berna Aksoy, and Lawrence Charles Parish Introduction Retinoids are among the most valuable drugs in the dermatologic armamentarium. This up-to-date reference on the use of retinoids in dermatology presents how retinoids function in the skin, how they can be used to treat and prevent various skin diseases, and how they can be effectively monitored. Providing an in-depth update on the pharmacology, clinical use, side effects, and follow-up of retinoid therapy in dermatology, this source also addresses topics related to retinoid use in special circumstances, including vulnerable populations, concomitant surgery, and aesthetic procedures. With chapters by internationally recognized authors, this book will stand as an up-to-date source on the topic. Historical Background General History of Vitamin A and Retinoids The importance of vitamin A has been recognized for over 3500 years, especially as a factor in treating deficiency diseases (1). Night blindness was recognized by the ancient Egyptians (Eber’s Papyrus, 1500 bce and Kahun 1 Papyrus, 1825 bce) who treated the affliction with roasted lamb or ox liver that was squeezed to be applied over the eye and then probably eaten (1–3). Night blindness and goat liver treatment were also later described by the ancient Greeks and by Hippocrates (460–327 bce) (1). By the late nineteenth century, the effects of vitamin A deficiency on growth had been recognized, and milk was discovered to be essential for healthy growth in the laboratory (1,4). Minimal qualitative factors in milk, egg, and butter were found that provided healthy growth and maintenance (1,4,5). By 1915, “fat-soluble factor A” was identified (1,2,6). The unknown factors in milk which support life were termed “accessory food factors,” The term “vitamine” (persisted as “vitamin”) was created to describe these “accessory factors” that are vital to life and probably of an amine (chemically, contains a nitrogen atom with a lone pair of electrons) in 1911 (4,6,7). Fat-soluble factor A was found to be associated with a yellow pigment extracted from plant sources, butter, or eggs (carotene: provitamin), and converted to an active colorless form (vitamin A: retinol) in the animal body in 1920–1930 (1). The chemical structure of vitamin A (β-carotene) was described in 1931, crystallized in 1937, and synthesized in 1947 (1–3,5–7). Between the 1950s and 1980s, the biochemical p­athways, anticarcinogenic activity, and nuclear retinoic acid receptors of vitamin A were established (1,2,8). An international meeting was convened by the World Health Organization (WHO) in 1974 to determine the status of vitamin A acid. It was at this congress in Jakarta, Indonesia that the compound was recognized as having comedolytic activity more than just an irritating effect (2,9). The antikeratotic effects of vitamin A have been recognized since 1932 (9). Three to eight million U of oral retinyl palmitate was used in the treatment of psoriasis, but such high dosage led to the development of hypervitaminosis A; hence, this therapy was abandoned (9). Following the report of 100,000 IU of systemic vitamin A in 1949 (10), this regimen was often used in acne therapy. Vitamin A acid (tretinoin) was discovered in 1946 and became commercially available in 1969 (5). This was followed by the synthesis of isotretinoin (13-cis retinoic acid) in 1971 (3,5) and acitretin in 1980 (11). The historical discovery of vitamin A and retinoids are depicted in Table 1.1. Topical Retinoids Systemic administration of retinyl palmitate was shown to decrease the rate of epidermal proliferation in 1949; however, retinol and retinyl palmitate did not exert any effect when applied topically despite its penetration through the stratum corneum. This discrepancy is probably due to execution of their effects through conversion to metabolites when systemically administered. These disappointing results led researchers to ­testing of other substances, including tretinoin (vitamin A acid, all-transretinoic acid) the major metabolite of retinol topically (9). Tretinoin was later shown to be able to penetrate the epidermis, to induce erythema and sometimes significant irritation of the skin, and to be effective in epidermal keratinization disorders in the early 1960s (9,12). The therapeutic action of tretinoin in acne was initially thwarted due to its irritant qualities. Not until the dose was reduced was its efficacy recognized and finally shown to be due to keratolytic action and an increase of the proliferation of follicular epithelium (9,12). Topical tretinoin demonstrated additional efficacy in various disorders ranging from cutaneous photoaging and carcinogenesis to psoriasis (12,13). With success of tretinoin in acne treatment, the pharmaceutical industry investigated more than 1500 different compounds (10,12). As a result, adapalene was introduced in 1990 for acne treatment (14,15) and tazarotene was found to be effective in treating psoriasis in 1994 (16) and acne in 1997 (17). 1 2 Retinoids in Dermatology TABLE 1.1 Vitamin A and Retinoids in Dermatology • 1900–1910s/Stepp, Hopkins, McCollum, Osborne, Mendel/ Fat-soluble growth factor extracted from eggs, milk, butter, liver • 1911/Funk/Vitamine • 1915/McCollum/Fat-soluble A • 1930/Moore/Carotene and vitamin A • 1931/Karrer/Chemical structure of vitamin A (retinol) • 1946/Arens/Vitamin A acid (tretinoin) • 1947/Isler/Synthesis of vitamin A (retinol) • 1960s/Stüttgen, Kligman/Topical effects of tretinoin • 1971/Bollag/Synthesis of isotretinoin • 1972/Synthesis of etretinate • 1973–1976/First clinical studies with 13-cis retinoic acid • 1980/Palmskog/Synthesis of acitretin • 1997/Miller/Bexarotene in CTCL • 1999/Bollag/Alitretinoin in chronic hand dermatitis Recently, trifarotene has been formulated as a cream for the treatment of facial and truncal acne for which selective retinoic acid receptor-γ (RAR-γ) activity that has recently been developed for moderate facial and truncal acne. The selectivity of trifarotene for RAR-γ distinguishes it from the existing first- and third-generation topical retinoids, which target both RAR-β and RAR-γ. Trifarotene has comedolytic, anti-inflammatory, and anti-pigmenting properties with a comparable safety profile due to its pharmacokinetic stability in keratinocytes and rapid metabolism by hepatic microsomes (18). Systemic Retinoids By 1971, the use of retinoid therapy had been expanded with the introduction of oral tretinoin (9,12) for the treatment of hyperkeratinization disorders, psoriasis, and even skin tumors (9). Significant untoward effects with oral tretinoin even included loss of consciousness, which discouraged its usage. This was attributed to regimens that used excessive dosing (9,10). When isotretinoin (13-cis retinoic acid) was introduced as a new ­isomer of retinoic acid in 1971, it proved to have a better therapeutic index after systemic administration than did oral tretinoin in the treatment of acne (9,10,13). Since 1978, isotretinoin treatment for cystic acne has provided almost miraculous results (13). Etretinate was synthesized in 1972 and subsequently employed for the treatment of psoriasis and keratinization disorders in the 1970s (9,10,19). Acitretin, as the principal metabolite of etretinate, soon replaced it in the 1980s due its improved metabolic profile (10,20). Bexarotene was initially reported for the treatment of cutaneous T-cell lymphoma in 1997 (21) and 9-cis r­ etinoic acid (alitretinoin) for chronic hand dermatitis in 1999 (22). The Future Retinoids, both topically and systemically, continue to be a significant part of the dermatologic armamentarium, in particular for the treatment of acne, psoriasis, cutaneous T-cell lymphoma, and keratinization disorders. They are efficacious for the most part and continue to be first-line, if not second-line agents. Many of the side effects of systemic retinoids are dose-dependent and reversible, except for their teratogenicity, which can be avoided by careful selection of the patients for whom they are prescribed. With new indications being found and additional compounds being synthesized, retinoids remain important and versatile agents in the treatment of skin diseases. REFERENCES 1. Wolf G. A history of vitamin A and retinoids. FASEB J. 1996;10:1102–1107. 2. Sommer A. Vitamin A deficiency and clinical disease: An historical overview. J Nutr. 2008;138:1835–1839. 3. Pawson BA. History of retinoids. J Am Acad Dermatol. 1982;6:577–582. 4. Rosenfeld L. Vitamine—vitamin. The early years of discovery. Clin Chem. 1997;43:680–685. 5. Burg G, Dummer R. Historical perspective on the use of retinoids in cutaneous T-cell lymphoma (CTCL). Clin Lymphoma. 2000;1:S41–S44. 6. Semba RD. The discovery of the vitamins. Int J Vitam Nutr Res. 2012;82:310–315. 7. Hammerling U. The centennial of vitamin A: A century of research in retinoids and carotenoids. FASEB J. 2013;27:3887–3890. 8. Saffiotti U, Montesano R, Sellakuma AR, Bork SA. Experimental cancer of the lung. Cancer 1967;20:857–864. 9. Stüttgen G. Historical perspectives of tretinoin. J Am Acad Dermatol. 1986;15:735–740. 10. Boyd AS. An overview of the retinoids. Am J Med. 1989;86:568–574. 11. Palmskog G. Determination of plasma levels of two aromatic retinoic acid analogues with antipsoriatic activity by high-performance liquid chromatography. J Chromatogr. 1980;221:345–351. 12. Leyden JJ. Tretinoin therapy in photoageing: Historical perspective. Br J Dermatol. 1990;122:S83–S86. 13. Stüttgen G. Historical observations. Dermatology. Clin Dermatol. 1996;14:135–142. 14. Hensby C, Cavey D, Bouclier M et al. The in vivo and in vitro anti-inflammatory activity of CD271: A new retinoid-like modulator of cell differentiation. Agents Actions. 1990;29:56–58. 15. Verschoore M, Langner A, Wolska H et al. Efficacy and safety of CD 271 alcoholic gels in the topical treatment of acne ­vulgaris. Br J Dermatol. 1991;124:368–371. 16. Esgleyes-Ribot T, Chandraratna RA, Lew-Kaya DA et al. Response of psoriasis to a new topical retinoid, AGN 190168. J Am Acad Dermatol. 1994;30:581–590. 17. Topical retinoid introduced for plaque psoriasis, acne vulgaris. Am J Health Syst Pharm. 1997;4:2037. 18. Tan J, Thiboutot D, Popp G et al. Randomized phase 3 evaluation of trifarotene 50 µG/G cream treatment of moderate facial and truncal ACNE. J Am Acad Dermatol. 2019;80(6):1691−1699. 19. Pettit JH. Oral retinoid for psoriasis. A report of a double blind study. Acta Derm Venereol Suppl (Stockh). 1979;59:133–136. 20. Kingston TP, Matt LH, Lowe NJ. Etretin therapy for severe psoriasis. Evaluation of initial clinical responses. Arch Dermatol. 1987;123:55–58. 21. Miller VA, Benedetti FM, Rigas JR et al. Initial clinical trial of a selective retinoid X receptor ligand, LGD1069. J Clin Oncol. 1997;15:790–795. 22. Bollag W, Ott F. Successful treatment of chronic hand eczema with oral 9-cis-retinoic acid. Dermatology 1999;199:308–312. 2 Mechanism of Action of Vitamin A Sandra Maria Barbalho Introduction Vitamin A (VA) is a fat-soluble agent that includes a cyclic ring, a polyene side chain, and a polar end group (1). It is involved in a plethora of biologic pathways that may include: 1. Regulation of adaptive or innate immunity (differentiation, growth, and migration of immune cells) 2. Vision cycle activity 3. Protection against oxidative stress 4. Prevention of malignant cell formation 5. Developmental morphogenesis 6. Stem cell differentiation 7. Neuronal signaling 8. Skin maintenance VA deficiency is common in developing countries and predisposes to the development of secondary infections, night blindness, and such immunologic disorders as shown in Figure 2.1 (2,3). The hepatic stellate cells in the space between hepatocytes and liver sinusoidal endothelial cells of the hepatic lobule can store 50%–80% of all VA as a retinyl ester (the main reservoir of VA in the body). Significant amounts are also found in the pancreas, lungs, intestines, adipose tissue, and the eyes. When the intake of VA is insufficient, retinol is released from the stellate cells to maintain the required circulating levels (2 µmol/L) (4). The term VA typically includes retinol, retinaldehyde, retinoic acid (RA) isomers, and retinyl esters, such as retinyl palmitate, that are the primary forms of VA obtained from animal products (2). FIGURE 2.1 Some consequences of the deprivation of vitamin A. Retinol and retinyl esters require enzymatic modifications to produce RA, which is the most biologically active form of VA (5). Mammals depend on diet to obtain enough VA once they are not able to synthesize this vitamin. Foods like carrots, sweet potato, squash, and apricots are sources of carotenoids; and eggs, milk, fish, and liver are sources of retinyl esters. The maintenance of VA levels is essential to growth, vision, reproduction, immunologic status, and metabolism (5,6). Metabolism of Vitamin A Retinoids may be acquired as retinyl esters (from animals) or β-carotene (from plants) and are absorbed in the small intestine, where they are carried to the liver by chylomicrons as retinylesters. In the liver, retinyl esters may be stored or are hydrolyzed to produce retinol that circulates bound to retinol-binding protein 4 (RBP4). It may enter the target cell using the stimulated by retinoic acid gene 6 (STRA6) homologs transporter or may cross the cell membrane by passive diffusion. In the cell, it binds to the cellular retinol-binding protein (CRBPI, CRBPII, and CRBPIII) and is modified to produce retinaldehyde by alcohol dehydrogenases (ALDH), such as retinol dehydrogenase (7,8). Retinaldehyde dehydrogenase catalyzes the conversion of retinaldehyde to different forms of RA: all-transRA (ATRA), 9-cis RA, 11-cis RA, 13-cis RA, and 9,13-di-cis RA (Figure 2.2). These compounds are further metabolized to 4-OH-RA, 4-oxo-RA, 18-OH-RA, 16-OH-RA, and 18-OH-RA by CYP26A1 and CYP26B1 (cytochrome P450 enzymes) to be subsequently excreted (Figure 2.2). The oxidation of ATRA produces 4-OH-RA and is possibly the most important route of elimination of ATRA. Other relevant enzymes include retinyl ester hydrolase (REH) that is related to the hydrolysis and release of the stored retinol and lecithin retinol acyltransferase (LRAT) and diacylglycerol O-acyltransferase (DGAT1) that are associated with its esterification (2,9,10). Cleavage of β-carotene by β, β-carotene-9,10-dioxygenase 2 or by mammalian β, β-carotene-15,150–monooxygenase-1 may also produce retinaldehyde (10,11). Of the five chemical isomers of RA, ATRA is the central biologic active form and is the main enzymatic compound involved in retinaldehyde oxidation (the action of the other isomers is incompletely understood). ATRA is associated with RA-binding proteins (CRABPI and CRABPII) and promotes regulation of the transcription of retinoid-responsive genes due to its effects on nuclear receptors. Both 9-cis RA and ATRA play roles using 3 4 Retinoids in Dermatology FIGURE 2.2 Metabolism of vitamin A. Retinol is metabolized to retinal by alcohol dehydrogenase (ALDH) or retinol dehydrogenase (RDH). Retinaldehyde dehydrogenases catalyze the conversion of retinal to RA that is further metabolized to 4-OH-RA, 4-oxo-RA, 16-OH-RA, and 18-OH-RA. (Modified from Stevison F et al. Adv Pharmacol. 2015;74:373–412.) different receptors and act in the nucleus, inducing gene expression by binding to nuclear transcription factors. There are different types of RA receptors (RARs) and retinoid X receptors (RXRs) that are capable of recognizing consensus sequences, named RA-response elements (RAREs). They may control the RA-responsive genes resulting in many different responses that include the uptake of retinol from the blood, the conversion of retinol to RA, and the presence and activity of the receptor RARs and RXRs. RARs can bind ATRA and 9-cis RA; RXR can bind only to 9-cis RA (9–12). RAR-RXR receptors, in the absence of ligands, bind to co-repressors leading to condensation of the chromatin and inaccessible DNA. The presence of RA results in the dissociation of co-repressors. This regulation activates or reduces gene expression and is responsible for cell growth, differentiation, and apoptosis (7,13). Figure 2.3 summarizes the uptake of vitamin A, transport, and gene regulation. Role of Retinoic Acid ATRA has been related to many biologic processes and may play a relevant role in the treatment of several pathologic conditions. It is critical to the health of the epithelium, growth, bone health, reproduction, tissue regeneration and repair, carbohydrate and lipid metabolism, and immune system. It seems to be crucial in modulating different inflammatory processes and in preventing different types of cancers. The cellular responses resulting from the action of ATRA are promoted by its union to RAR and PPAR-β/δ (peroxisome proliferator-activated receptors) (2,14). With the activation of these receptors, there is transcription of target genes, resulting in regulatory mechanisms that are related to the homeostasis (15). VA plays an essential role in immunity, and its deficiency increases morbidity and mortality from some pathogens (16). Retinol increases the gut mucosal immunity, and ATRA itself is vital to immune homeostasis due to the regulation of B-cell, T-cell, and dendritic cell action and balance in the release of anti-inflammatory cytokines (17). The deficiency of VA leads to enhanced differentiation of naive CD4+ T cells into T-helper 1 cells (TH1), and synthesis of interferon-γ. The presence of ATRA in high concentrations results in downregulation of TH2 and TH17 responses and starts the T regulatory cell differentiation. VA, together with TGF-β, enhance the Foxp3 expression that is important in development of Treg cells and reducing inflammation. These processes modulate the inflammatory processes and prevent the induction of autoimmune T cells (18). In the skin, RA interferes with dendritic cells and T cells. Dendritic cells express ALDH to produce RA and also activate Treg cell differentiation and Foxp3 expression, leading to immunomodulatory and anti-inflammatory activities. Retinoid levels in the skin are tightly controlled and are stored as retinyl esters. RA, when locally synthesized in the epidermis, may increase 5 Mechanism of Action of Vitamin A FIGURE 2.3 The uptake of carotenoids and retinol occurs in the enterocytes. Retinyl esters and carotenoids are transported to the liver by the chylomicrons. Circulating retinyl esters may come from the liver stores, and in target cells produce RA isomers (ALDH, XO, AO, and P450 enzymes). ATRA and 9-cis RA may stimulate the transcription of genes due to the activation of RAR and RXR. The clearance of ATRA to oxidized products is performed mainly by CYP26 (cytochrome P450 enzymes). REH, retinyl ester hydrolase; RoDH, retinol dehydrogenase; RBP, retinol-binding protein; CM, chylomicron; LRAT, lecithin retinol acyl-transferase; ALDH, alcohol dehydrogenase; XO, xanthine oxidase; AO, aldehyde oxidase; ATRA, all-trans-retinoic acid; 9-cis RA, 9-cis retinoic acid; CRBP, cellular retinol-binding protein; CRABP, cellular retinoic acid-binding protein; RAR, retinoic acid receptor; RXR, retinoid X receptors. (Modified from Saeed A et al. Nutrients. 2018;29;10(1):20. pii: E29; Stevison F et al. Adv Pharmacol. 2015;74:373–412.) dermal collagen synthesis, inhibit collagenase activity, augment the expression of CRABPII, CRBP mRNA, and protein, inhibit UV-induction of matrix metalloproteinases, and induce collagen synthesis in photoaged skin. It also contributes to reducing scaling and cutaneous inflammation (18,19). Conclusions VA plays many different roles in the human body. It is necessary for reproduction, growth, immunity, tissue repair, and epithelium health. For these reasons, it is indispensable for the maintenance of the homeostasis. REFERENCES 1. Janesick A, Wu SC, Blumberg B. Retinoic acid signaling and neuronal differentiation. Cell Mol Life Sci. 2015;72(8): 1559–1576. 2. Saeed A, Dullaart RPF, Schreuder TCMA, Blokzijl H, Faber KN. Disturbed vitamin A metabolism in non-alcoholic fatty liver disease (NAFLD). Nutrients. 2018;10(1):29. pii: E29. 6 Retinoids in Dermatology 3. Chawla B, Swain W, Williams AL, Bohnsack BL. Retinoic acid maintains function of neural crest-derived ocular and craniofacial structures in adult zebrafish. Invest Ophthalmol Vis Sci. 2018;59(5):1924–1935. 4. Senoo H, Mezaki Y, Fujiwara M. The stellate cell system (vitamin A-storing cell system). Anat Sci Int. 2017;92(4): ­ 387–455. 5. Saeed A, Hoekstra M, Hoeke MO, Heegsma J, Faber KN. The interrelationship between bile acid and vitamin A homeostasis. Biochim Biophys Acta. 2017;1862:496–512. 6. Tanumihardjo SA, Russell RM, Stephensen CB. Biomarkers of nutrition for development (BOND)-vitamin A review. J Nutr. 2016;146:1816S–1848S. 7. Khalil S, Bardawil T, Stephan C. Retinoids: A journey from the molecular structures and mechanisms of action to clinical uses in dermatology and adverse effects. J Dermatolog Treat. 2017;28(8):684–696. 8. Kawaguchi R, Zhong M, Kassai M, Ter-Stepanian M, Sun H. Vitamin A transport mechanism of the multitransmembrane cell-surface receptor STRA6. Membranes (Basel). 2015;5(3):425–453. 9. Stevison F, Jing J, Tripathy S, Isoherranen N. Role of retinoic acid-metabolizing cytochrome P450 s, CYP26, in inflammation and cancer. Adv Pharmacol. 2015;74:373–412. 10. Maden M. Retinoid signalling in the development of the central nervous system. Nat Rev Neurosci. 2002;3(11):843–853. 11. Chen J, Cao X, An Q, Zhang Y, Li K, Yao W, Shi F et al. Inhibition of cancer stem cell like cells by a synthetic retinoid. Nat Commun. 2018;11,9(1):1406. 12. He XY, Zhao J, Chen ZQ, Jin R, Liu CY. High expression of retinoic acid induced 14 (RAI14) in gastric cancer and its prognostic value. Med Sci Monit. 2018;24:2244–2251. 13. Bastien J, Rochette-Egly C. Nuclear retinoid receptors and the transcription of retinoid target genes. Gene. 2004;328: 1–16. 14. Gudas LJ, Wagner JA. Retinoids regulate stem cell differentiation. J Cellular Physiol. 2011;226:322–330. 15. Larange A, Cheroutre H. Retinoic acid and retinoic acid receptors as pleiotropic modulators of the immune system. Annu Rev Immunol. 2016;34:369–394. 16. Ross AC. Vitamin A and retinoic acid in T cell-related immunity. Am J Clin Nutr. 2012;96:1166S–1172S. 17. Raverdeau M, Mills KHG. Modulation of T cell and innate immune responses by retinoic acid. J Immunol. 2014;192: 2953–2958. 18. Wen J, Lopes F, Soares G, Farrell SA, Nelson C, Qiao Y et al. Phenotypic and functional consequences of haploinsufficiency of genes from exocyst and retinoic acid pathway due to a recurrent microdeletion of 2p13.2. Orphanet J Rare Diseases. 2013;8:100. 19. Kong R, Cui Y, Fisher GJ, Wang X, Chen Y, Schneider LM, Majmudar GA. Comparative study of the effects of retinol and retinoic acid on histological, molecular, and clinical properties of human skin. J Cosmet Dermatol. 2016;(1): ­ 49–57. 3 Mechanism of Action of Topical Retinoids Sümeyre Seda Ertekin and Mehmet Salih Gurel Introduction mediated endocytosis (7). The pathways of intracellular molecular mechanism of action have been well investigated for ATRA but may not be valid for all topical retinoid compounds. Once in the cytoplasm, ATRA is transported to the nucleus by cellular retinoic acid-binding proteins (CRABPs). The dominant CRABP in the skin is CRABP II, and it is considered to play an important role in retinoid bioavailability, as it is upregulated by ATRA (8). The term “retinoids” encompasses compounds derived from vitamin A as well as compounds that demonstrate structural and/or functional similarity to vitamin A and are able to interact with retinoid receptors. Retinoids exert a wide variety of effects on cellular differentiation and proliferation, embryogenesis, and the immune system. The first topical retinoid, all-trans-retinoic acid (ATRA), was approved by the Food and Drug Administration (FDA) in 1971 for the treatment of acne. With the discovery and characterization of retinoid receptors, knowledge of the retinoid mechanism of action has significantly advanced. Since then, retinoids have continued to evolve, and an increasing number of synthetic retinoids have been synthesized. Currently, topical retinoids are used for a variety of dermatologic conditions, ranging from acne, photoaging, psoriasis, and Kaposi sarcoma to cutaneous T-cell lymphoma (1–3). Nuclear Retinoid Receptors and Their Distribution in Human Skin Mechanism of Action Retinoic Acid−Mediated Gene Transcription Intracellular Transport to Nucleus Given that retinoid receptors are transcription factors, they should accomplish their biologic effects on the skin through regulating the activation or inhibition of gene expression. In the absence of ligand, retinoid receptors are bound as dimers to specific The physiologic and pharmacologic effects of retinoids are mainly mediated by two distinct families of nuclear retinoid receptors: retinoic acid receptors (RAR) and retinoid X receptors (RXR) (Table 3.1). These receptor families are referred to as liganddependent transcription factors, and they belong to a superfamily of nuclear hormone receptors which include the steroid, thyroid hormone, vitamin D, and peroxisome proliferator-activated receptors (PPARs). Both RAR and RXR families exhibit three receptor isotypes (α, β, γ) and a number of isoforms for each isotype. Classification of Retinoids RAR and RXR have different ligand binding affinities; ATRA Three generations of synthetic retinoids have been developed for only binds to RARs, while 9-cis RA binds both to RARs and topical and systemic treatment of several skin diseases (Table 3.1). RXRs. Each nuclear retinoid receptor exhibits a modular strucFirst-generation retinoids are naturally occurring non-­ ture composed of six regions. Out of them, three regions are of aromatic retinoids. They include vitamin A (all-trans retinol), importance: the A/B region maintains a ligand independent trantretinoin (ATRA), isotretinoin (13-cis retinoic acid), and alitretiscriptional activation function, the C region harbors DNA recognoin (9-cis retinoic acid). This group retains the cyclic structure nizing and binding domain, and the E region corresponds to the of vitamin A with chemically modified polyene side chain and ligand-binding domain (9). The human epidermis expresses all the polar end group. RAR and RXR isotypes, but RAR-γ and RXR-α represent the Second-generation monoaromatic retinoids are formed by majority of the cutaneous retinoid receptors (10–12). RXR levels replacement of the cyclic end group of vitamin A with various are found to be five times greater than RARs in the skin (12). ring systems. This group includes acitretin and etretinate. Retinoid receptors bind to retinoids in the form of dimers. Third-generation polyaromatic retinoids are synthesized by RARs only function when they form heterodimers with RXRs cyclization of the polyene side chain, and they are called aroti(RAR/RXR), whereas RXRs may also act as homodimers noids. These include adapalene, tazarotene, and bexarotene (3,4). (RXR/RXR). RXR can also form heterodimers with a variety Recently, a novel first-in-class fourth-generation topical retiof other nuclear receptors like vitamin D, PPARs, and thyroid noid, trifarotene, has been described and is under investigation for hormone, and this fact provides a mechanism for the ability of clinical safety and efficacy in acne and lamellar ichthyosis (5,6). retinoids to activate various cellular pathways (10–12). When retinoids are applied to the skin, the molecules pass through the cellular membrane of keratinocytes via non-receptor 7 8 Retinoids in Dermatology TABLE 3.1 Chemical Structure of Topical Retinoids Tretionin (all-trans-retinoic acid) Isotretinoin (13-cis retinoic acid) Adapalene Tazarotene Bexarotene Alitretionin (9-cis retinoic acid) Trifarotene Source: Adapted from https://pubchem.ncbi.nlm.nih.gov/ [accessed on May 1, 2019]. DNA sequences which are called retinoic acid response elements (RAREs). Various RAREs have been identified in the promoters of several retinoid-target genes. Unliganded and DNA-bound retinoid receptors repress transcription through recruitment of co-repressor molecules such as nuclear receptor co-repressor (N-CoR) and silencing mediator for retinoid and thyroid receptor (SMRT). Binding of retinoic acid to its receptor leads to dissociation of co-repressors and subsequent binding of co-activators. These co-activators cause conformational changes in the receptors and decompact condensed chromatin by showing histone acetylase activity. This conformational change facilitates the positioning of the transcriptional machinery at the promoter side of DNA and results in transactivation. Retinoid receptors regulate transcription of a large number of genes which mainly play a role in differentiation (13,14). Apart from this RARE-dependent direct upregulating of gene transcription, retinoids can indirectly downregulate some genes by antagonizing the effect of the transcription factor activator protein-1 (AP1). AP1 controls a wide range of cellular processes, including cell growth, proliferation, and apoptosis. Indirect AP1 inhibition appears to be a major mechanism of pharmacologic antiproliferative, anti-oncogenic, and anti-inflammatory effects of retinoids (15). In addition to its genomic effects, some retinoid functions are proved to be mediated through non-genomic effects (e.g., phosphorylation), but their biologic relevance is still under investigation (16). Intracellular Metabolism of Natural Retinoids Externally-applied retinoids are metabolized in human epidermis. Excess all-trans retinol in keratinocytes is either esterified to 9 Mechanism of Action of Topical Retinoids retinyl esters, catalyzed by lecithin:retinol acyltransferase (LRAT) or sequentially oxidized to ATRA, with all-trans retinaldehyde as the intermediate metabolite. Excess ATRA within cell is catabolized by cytochrome-P450 enzyme systems, such as CYP26, to its metabolites 4-hyroxy-all-trans-retinoic acid and 4-oxo-retinoic acid. This process can be induced by retinoic acid itself and may show important inter-individual variation. It may be the reason for differences between individuals in response to topically applied retinoids (17). Additionally, ATRA-induced catabolism of ATRA by CYP26 is a key mechanism of resistance to retinoids. To overcome this resistance, a new strategy has been developed, which aims to increase the levels of intracellular endogenous ATRA by inhibiting CYP26. These inhibitors are referred to as retinoic acid metabolism−blocking agents (RAMBAs) (18). Among these, liarozole, an imidazole derivative, is the most investigated one and has been approved to use for the treatment of congenital ichthyosis (19). Synthetic Topical Retinoids Tretinoin (All-trans-Retinoic Acid) All-trans-retinoic acid is a naturally occurring first-generation retinoid which is normally present in the skin. The synthetic form of topical ATRA (tretinoin) has been approved by the FDA for the treatment of acne and photoaging (1). It has also been used off-label for several dermatologic conditions like pigmentary disorders, wound healing, Darier disease, verrucae plana, and actinic keratosis (20). It binds to all RAR isotypes, but not to RXRs. It normalizes follicular epithelial differentiation and keratinization. It increases mitotic activity of follicular epithelia and turnover rate of thin, loosely-adherent corneocytes. Shedding of those corneocytes from the follicle is the principal mechanism of its comedolytic activity. In addition, it has been shown to induce the expression of heparin-binding EGF-like growth factor (HB-EGF), which results in epidermal hyperplasia in atrophic photodamaged epidermis (21,22). Isotretinoin 13-cis retinoic acid (isotretinoin) is a stereoisomer of tretinoin and occurs naturally from the metabolism of tretinoin in the epidermis (23). Its synthetic derivatives act in a comparable way to tretinoin and alter epithelization of the follicles and aid desquamation; however, isotretinoin seems to have a slightly more antiinflammatory effect compared to its stereoisomer. Inhibition of leukotriene-B4-induced transdermal migration of polymorphonuclear leukocytes is more pronounced with topically applied isotretinoin than tretinoin (24). This might explain the relatively low level of irritation or inflammation seen with the topical isotretinoin, making its use more tolerable for patients. Adapalene Adapalene is a chemically stable, photostable, and highly lipophilic synthetic retinoid which has a selective affinity for retinoid receptors RAR-β and RAR-γ. Although it does not bind to CRABPs, it has been shown to induce expression of CRABP-II. Its FDA-approved indication is acne. Due to its lipophilic properties, it is selectively uptaken by the follicular unit, and that may contribute to its success in anti-acne activity. It normalizes the differentiation and keratinization of follicular epithelial cells, thus leading to a comedolytic effect. In addition, in contrast to other classical retinoids, adapalene is a naphthoic acid derivate which has an NSAID-like structure and increased anti-­inflammatory effect. It decreases leukotriene and prostaglandin production through inhibition of lipoxygenase activity and arachidonic acid metabolism (25). Adapalene can modulate the epidermal immune system by increasing CD1d expression and decreasing IL-10 expression by keratinocytes. Decreasing expression of toll-like receptor-2 (TLR-2) by keratinocytes can help to explain the antiinflammatory activity of adapalene observed in clinical practice (26). These mechanisms may explain the reason for decreased risk of irritation with adapalene. Systemic absorption of adapalene is negligible. Only trace amounts have been found in the plasma of acne patients following chronic topical application of adapalene. Tazarotene Tazarotene is a prodrug that undergoes esterase hydrolysis in cutaneous tissue to form its active metabolite, tazarotenic acid. It has a higher affinity to RAR-γ/β than RAR-α, but it does not bind to RXR (3). Its FDA-approved indications for topical use are psoriasis and acne vulgaris. It modulates the pathogenesis of psoriasis by regulating gene expression of retinoid-induced genes, including those that regulate cell proliferation, differentiation, and inflammation. Tazarotene appears to downregulate the expression of keratinocyte transglutaminase, hyperproliferative keratins K6 and K16, IL-6, skin-derived antileukoproteinase (SKALP), involucrin, and migration inhibitory factor-related protein (27); however, it may induce filaggrin, which is underexpressed in psoriatic skin. Three tazarotene-inducible genes (TIG-1, TIG-2, TIG-3) are described. Although their exact role in psoriasis pathogenesis is not clear, their expression is very low in psoriatic skin compared with the adjacent normal skin. TIG-2/TIG-3 are also underexpressed in cutaneous squamous cell carcinoma and basal cell carcinoma (28,29). The induced expression of those genes by tazarotene leads to a reduction in keratinocyte proliferation in psoriatic skin. Systemic absorption of the prodrug is very low due to its rapid skin metabolism (3). Bexarotene Bexarotene binds selectively to RXR receptors, and therefore it is a “rexinoid.” Its FDA-approved indication for topical use is cutaneous T-cell lymphoma (CTCL). Bexarotene inhibits cell cycle and induces apoptosis of malignant T cells by activating RXR receptors. It causes apoptosis by decreasing anti-apoptotic protein (survivin) and activating caspase-3 (30). RXRs can also form heterodimers with non-retinoid nuclear receptors including vitamin D, thyroid hormone, and PPARs. It may show some of its anti-inflammatory and antitumor effects through inducing PPAR-γ pathway. Plasma concentrations after topical application are usually low but are dependent on the treated body surface area. Alitretionin (9-cis Retinoic Acid) Alitretionin is a naturally occurring retinoid routinely found in the skin. It binds effectively to all RARs and RXRs, therefore 10 Retinoids in Dermatology TABLE 3.2 Binding of Topical Retinoids to Nuclear Receptors Nuclear Receptor Binding Ability Topical Retinoids Generation RAR-α RAR-β RAR-γ RXR-α RXR-β RXR-γ All-trans-retinoic acid (tretinoin) First generation + + + − − − 13-cis retinoic acid (isotretinoin) First generation + + + − − − 9-cis retinoic acid (alitretinoin) “Panretin” First generation + + + + + + Adapalene Third generation ± + + − − − Tazarotene Third generation ± + + − − − Bexarotene “Rexinoid” Third generation − − − + + + Trifarotene Fourth generation − − + − − − Sources: Chandraratna RA. J Am Acad Dermatol. 1998;39:S124–S128, Riahi; RR et al. Am J Clin Dermatol. 2016;17:265–276; Nagpal S et al. Cell Growth Differ. 1996;7:1783–1791. it is referred to as “pan-agonist.” A synthetic form of topical alitretinoin has been approved by the FDA for the treatment of AIDS-related Kaposi sarcoma (KS). The pro-apoptotic effect of alitretinoin is related to RXRs, whereas RARs mediate the antiproliferative activity. Alitretionin has been shown to downregulate expression of IL-6 and alter the expression of viral encoded oncogenes that are present in the lesions of KS (31,32). Trifarotene Trifarotene is a novel first-in-class fourth-generation topical retinoid with a potent and selective RAR-γ activity which distinguishes it from the already existing first- and third-generation topical retinoids (5). It was developed for topical use in acne and lamellar ichthyosis treatment. In multiple murine models, trifarotene showed better comedolytic, anti-inflammatory, and anti-­pigmenting properties compared with other topical retinoids (5). It is pharmacokinetically stable in keratinocytes, but it is degraded rapidly in hepatic microsomes; therefore it is believed to have a favorable safety profile (5). Two recently conducted phase III studies of topical trifarotene demonstrated that it is a safe and efficacious treatment for both facial and truncal acne (6). Conclusions Topical retinoids play a significant role in the management of various skin conditions. RARs and RXRs are the keystones in the mechanism of action of all topical retinoids. In the presence of retinoid, the RARs and RXRs can bind specific DNA regulatory sequences and can thereby alter expression of many regulatory proteins. By changing the expression of keratins, growth factors, and transglutaminases, topical retinoids exert a wide variety of effects on epithelial differentiation and proliferation and the skin immune system. Due to their structural differences, each commercially available retinoid must be accepted as a unique drug because they show different receptor binding ability, clinical efficacy, pharmacodynamics, and side effects (33,34) (Table 3.2). REFERENCES 1. Stüttgen G. Historical perspectives of tretinoin. J Am Acad Dermatol. 1986;15:735–740. 2. Giguere V, Ong ES, Segui P et al. Identification of a receptor for the morphogen retinoic acid. Nature. 1987;330:624–629. 3. Chandraratna RA. Rational design of receptor-selective retinoids. J Am Acad Dermatol. 1998;39:S124–128. 4. Rigopoulos D, Ioannides D, Kalogeromitros D et al. Comparison of topical retinoids in the treatment of acne. Clin Dermatol. 2004;22:408–411. 5. Aubert J, Piwnica D, Bertino B et al. Nonclinical and human pharmacology of the potent and selective topical retinoic acid receptor-gamma agonist trifarotene. Br J Dermatol. 2018;179:442–456. 6. Tan J, Thiboutot D, Popp G et al. Randomized phase 3 evaluation of trifarotene 50 muG/G cream treatment of moderate facial and truncal acne. J Am Acad Dermatol. 2019;80(6):1691−1699. 7. Vieira AV, Schneider WJ, Vieira PM. Retinoids: Transport, metabolism, and mechanisms of action. J Endocrinol. 1995;146:201–207. 8. Reichrath J, Lehmann B, Carlberg C et al. Vitamins as hormones. Horm Metab Res. 2007;39:71–84. 9. Bastien J, Rochette-Egly C. Nuclear retinoid receptors and the transcription of retinoid-target genes. Gene. 2004;328:1–16. 10. Reichrath J, Mittmann M, Kamradt J et al. Expression of retinoid-X receptors (-alpha, -beta, -gamma) and retinoic acid receptors (-alpha, -beta, -gamma) in normal human skin: An immunohistological evaluation. Histochem J. 1997;29:127–133. 11. Fisher GJ, Voorhees JJ. Molecular mechanisms of retinoid actions in skin. FASEB J. 1996;10:1002–1013. 12. Fisher GJ, Talwar HS, Xiao JH et al. Immunological identification and functional quantitation of retinoic acid and retinoid X receptor proteins in human skin. J Biol Chem. 1994;269:20629–20635. 13. Chen JD, Evans RM. A transcriptional co-repressor that interacts with nuclear hormone receptors. Nature. 1995;377:454–457. 14. Glass CK, Rosenfeld MG. The coregulator exchange in transcriptional functions of nuclear receptors. Genes Dev. 2000;14:121–141. 15. Lefebvre P. Molecular basis for designing selective modulators of retinoic acid receptor transcriptional activities. Curr Drug Targets Immune Endocr Metab Disord. 2001;1:153–164. 16. Blomhoff R, Blomhoff HK. Overview of retinoid metabolism and function. J Neurobiol. 2006;66:606–630. 17. Smith G, Wolf CR, Deeni YY et al. Cutaneous expression of cytochrome P450 CYP2S1: Individuality in regulation Mechanism of Action of Topical Retinoids 18. 19. 20. 21. 22. 23. 24. 25. 26. by therapeutic agents for psoriasis and other skin diseases. Lancet. 2003;361:1336–1343. Njar VC, Gediya L, Purushottamachar P et al. Retinoic acid metabolism blocking agents (RAMBAs) for treatment of cancer and dermatological diseases. Bioorg Med Chem. 2006;14:4323–4340. Vahlquist A, Blockhuys S, Steijlen P et al. Oral liarozole in the treatment of patients with moderate/severe lamellar ichthyosis: Results of a randomized, double-blind, multinational, placebo-controlled phase II/III trial. Br J Dermatol. 2014;170:173–181. Riahi RR, Bush AE, Cohen PR. Topical retinoids: Therapeutic mechanisms in the treatment of photodamaged skin. Am J Clin Dermatol. 2016;17:265–276. Stoll SW, Elder JT. Retinoid regulation of heparin-binding EGF-like growth factor gene expression in human keratinocytes and skin. Exp Dermatol. 1998;7:391–397. Darlenski R, Surber C, Fluhr JW. Topical retinoids in the management of photodamaged skin: From theory to evidencebased practical approach. Br J Dermatol. 2010;163:1157–1165. Lehman PA, Malany AM. Evidence for percutaneous absorption of isotretinoin from the photo-isomerization of topical tretinoin. J Invest Dermatol. 1989;93:595–599. Wozel G, Chang A, Zultak M et al. The effect of topical retinoids on the leukotriene-B4-induced migration of polymorphonuclear leukocytes into human skin. Arch Dermatol Res. 1991;283:158–161. Jones DA. The potential immunomodulatory effects of topical retinoids. Dermatol Online J. 2005;11:3. Tenaud I, Khammari A, Dreno B. In vitro modulation of TLR-2, CD1d and IL-10 by adapalene on normal human skin and acne inflammatory lesions. Exp Dermatol. 2007;16:500–506. 11 27. Duvic M, Asano AT, Hager C et al. The pathogenesis of psoriasis and the mechanism of action of tazarotene. J Am Acad Dermatol. 1998;39:S129–133. 28. Peris K, Fargnoli MC, Chimenti S. Preliminary observations on the use of topical tazarotene to treat basal-cell carcinoma. N Engl J Med. 1999;341:1767–1768. 29. Zheng Y, Luo S, Wang G et al. Downregulation of tazarotene induced gene-2 (TIG2) in skin squamous cell carcinoma. Eur J Dermatol. 2008;18:638–641. 30. Zhang C, Hazarika P, Ni X et al. Induction of apoptosis by bexarotene in cutaneous T-cell lymphoma cells: Relevance to mechanism of therapeutic action. Clin Cancer Res. 2002;8:1234–1240. 31. Duvic M, Friedman-Kien AE, Looney DJ et al. Topical treatment of cutaneous lesions of acquired immunodeficiency ­syndrome-related Kaposi sarcoma using alitretinoin gel: Results of phase 1 and 2 trials. Arch Dermatol. 2000;136:1461–1469. 32. Bodsworth NJ, Bloch M, Bower M et al. Phase III vehicle-­ controlled, multi-centered study of topical alitretinoin gel 0.1% in cutaneous AIDS-related Kaposi’s sarcoma. Am J Clin Dermatol. 2001;2:77–87. 33. Cunliffe WJ. A new topical retinoid—why a new topical acne therapy? Br J Dermatol. 1998;139(Suppl 52):1–2. 34. Khalil S, Bardawil T, Stephan C et al. Retinoids: A journey from the molecular structures and mechanisms of action to clinical uses in dermatology and adverse effects. J Dermatolog Treat. 2017;28:684–696. 35. Nagpal S, Thacher SM, Patel S et al. Negative regulation of two hyperproliferative keratinocyte differentiation markers by a retinoic acid receptor-specific retinoid: Insight into the mechanism of retinoid action in psoriasis. Cell Growth Differ. 1996;7:1783–1791. 4 Mechanism of Action of Isotretinoin Bodo C. Melnik Introduction Systemic isotretinoin (13-cis retinoic acid) (Figure 4.1) is the most efficient treatment option for the management of severe forms of acne vulgaris, especially nodulocystic acne (1). Of all known antiacne drugs, isotretinoin exerts the strongest sebum-­suppressive effect (2,3), which primarily results from sebocyte apoptosis (4–6). Isotretinoin’s apoptosis-inducing effect is the basis for its use in chemoprevention of basal cell carcinoma s­yndrome, as well as the treatment of childhood neuroblastoma and promyelocytic leukemia (7–13). In addition, isotretinoin induces apoptosis in Dalton lymphoma ascites cells, adult T-cell leukemia (ATL) cells, B16F-10 melanoma cells, and p­ rimary human keratinocytes (14–17). Apoptosis not only explains isotretinoin’s mode of action in the treatment of acne and ­isotretinoin-responsive malignancies, but it is also related to isotretinoin’s adverse drug effects including teratogenicity (18,19). Sebocyte and Meibomian Cell Apoptosis Involution of sebaceous glands in acne patients treated with oral isotretinoin has been shown to be the major cause of sebum suppression (20,21). The temporal changes in gene expression in acne skin during isotretinoin treatment suggested a model wherein isotretinoin induces apoptosis reducing sebaceous gland size, decreasing expression of lipid-metabolizing enzymes, and increasing matrix remodeling during acne resolution (22,23). Surprisingly, isotretinoin’s principal apoptosis-inducing mode of action was not characterized until three decades after its introduction for the treatment of severe acne (3–6). To understand isotretinoin’s pro-apoptotic signaling in acne, the major signaling pathways in acne pathogenesis are briefly characterized (24). The key hormone of puberty, insulin-like growth factor 1 (IGF-1), promotes AKT-mTORC1-mediated sebaceous lipogenesis as well as the production of sebocytederived proinflammatory cytokines including interleukin 1β (IL-1β) (25–30). IGF-1 augments the synthesis of adrenal and gonadal androgens (31), which in synergy with IGF-1 stimulate sebaceous gland hypertrophy and sebum production (31,32). IGF-1 induces the expression of the anti-apoptotic protein survivin, a member of the inhibitor of apoptosis protein family, which is upregulated in the serum of acne patients in an IGF-1dependent manner (33). IGF-1, via activating the kinase AKT, promotes nuclear-cytoplasmic extrusion of the pro-apoptotic transcription factors FoxO1 and FoxO3a (34–37), a further prosurvival mechanism of sebaceous glands which is overstimulated in sebaceous glands of acne patients (38). Epidermal FoxO1 immunostaining was lower in acne lesion compared with normal skin (17). In 2010, our group (39,40) hypothesized that oral isotretinoin may increase nuclear levels of FoxO1 at the expense of cytoplasmic FoxO1 (Figure 4.1). Our hypothesis has recently been confirmed (41). In primary human keratinocytes, isotretinoin enhances the expression of p53, FoxO1, and p21 but it inhibits phosphorylated FoxO1 (17). In addition, there is an increased nucleo-cytoplasmic ratio of non-phosphorylated FoxO1 and FoxO3a after 6 weeks of oral isotretinoin treatment of acne patients (41) (Figure 4.2). As a result, isotretinoin treatment enhances pro-apoptotic nuclear FoxO signaling, which is deficient in acne skin due to increased pro-survival IGF-1-AKT-mTORC1 signaling (42). Long-term systemic treatment of female New Zealand rabbits with isotretinoin induces degenerative changes in the Meibomian gland acini, leading to a decrease in basaloid cells lining the acini walls (43). Isotretinoin’s effect on the Meibomian glands mimics its apoptotic effects on the sebaceous glands of the skin of isotretinoin-treated acne patients, resulting in both reduced quality and quantity of meibum due to fewer Meibomian cells (44). Endocrine Effects Isotretinoin-mediated activation of hepatic FoxO1 downregulates the expression of growth hormone receptor (GHR) in the liver (45), the central organ secreting IGF-1 into the circulation. FoxO1 not only suppresses GHR expression but also the activation of peroxisome proliferator-activated receptor γ (PPAR-γ) (46), which mediates hepatic secretion of IGF-1 (47). This explains the observed decrease of IGF-1 during isotretinoin treatment (48). Isotretinoin also causes mild suppression of pituitary hormone levels observed in acne patients (49). Free triiodothyronine, free thyroxine, luteinizing hormone, prolactin, and total testosterone, as well as morning cortisol and adrenocorticotropic hormone (ACTH), are decreased during isotretinoin treatment (49–51). FoxO1 directly interacts with STAT3 and prevents STAT3 from binding to the specificity protein 1 (SP1)-proopiomelanocortin (POMC) promoter complex, and thereby inhibits STAT3-mediated POMC expression. 13 14 Retinoids in Dermatology FIGURE 4.1 Sebocyte apoptosis explains the sebum-suppressive effect of systemic isotretinoin. In the sebocyte, isotretinoin is isomerized to all-transretinoic acid (ATRA), which is transported to the nucleus via cellular retinoic acid-binding protein 2 (CRABP-2). In the nucleus, ATRA binds to retinoic acid receptor (RAR) that activates the RAR-responsive target genes TP53 promoting the expression of p53 and of ARF, promoting the expression of p14. p14 is a negative regulator of mouse double minute 2 (MDM2), the key inhibitor of p53. Increased IGF-1 signaling is attenuated by p53 via suppression of IGF-1 receptor (IGF1R) and upregulation of phosphatase and tensin homolog (PTEN) suppressing the activity of the kinase AKT. p53 induces the expression of BLIMP1, FoxO1, and FoxO3, known suppressors of c-Myc. p53, FoxO1, and FoxO3 activate the expression of tumor necrosis factor-related apoptosisinducing ligand (TRAIL), which activates caspase 3 leading to sebocyte apoptosis. Abbreviations: BLIMP1, B lymphocyte-induced maturation protein 1; FoxO, forkhead box class O; mTORC1, mechanistic target of rapamycin complex 1; PI3K, phosphoinositide-3 kinase; S6K1, ribosomal protein S6 kinase; SREBP1, sterol regulatory-element binding protein 1. FoxO1 also binds directly to the POMC promoter and negatively regulates its transcription. In addition, FoxO3a interacts with STAT3 and inhibits POMC promoter activity (52,53). Isotretinoin-induced upregulation of FoxO1 and FoxO3a may thus explain isotretinoin-mediated suppression of POMC-dependent pituitary gene expression, the precursor of ACTH. Isotretinoinmediated upregulation of p53 attenuates androgen receptor (AR) gene expression (54). p53 and FoxO1 suppress AR expression and transactivation, respectively (55,56). This has been demonstrated in the skin of isotretinoin-treated acne patients, where isotretinoin has reduced AR expression as well as 5α-reductase activity in the skin, which has lost 80% of their ability to form 5α-dihydrotestosterone (57,58). In contrast, p53 deletion has activated AR signaling and restored c-MYC-induced differentiation in sebaceous glands (59). p53 is a negative regulator of thyroid hormone receptor-signaling pathways (60). Isotretinoin, Expression of p53 and p53 Target Genes Isotretinoin (13-cis retinoic acid) exerts its sebocyte-specific activity through selective intracellular isomerization to alltrans-retinoic acid (ATRA) (61). In human sebocytes in vitro, isotretinoin and ATRA decrease sebocyte proliferation in a dose- and time-dependent manner (62). In sebocytes, isotretinoin increases the expression of cellular retinoid acid-binding protein-2 (CRABP-2) (63), which transports ATRA to the nucleus for gene regulation (64,65) (Figure 4.1). The CRABPII gene promoter contains a TATA-box that is rapidly activated by ATRA through a retinoic acid response element (RARE) (65). CRABP-2 is strongly expressed in suprabasal sebocytes compared to the e­ pidermis in isotretinoin-treated patients, promoting a preferential transport of ATRA to retinoic acid receptors (RARs) in sebocytes (63). ATRA induces cell differentiation primarily by binding to RARs, the transcription factors that associate with RXRs and bind to RAREs in the nucleus (64). ATRA/RAR-signaling induces secondary responses in gene expression, encoding transcription factors and signaling proteins that further augment a whole cascade of gene expression including apoptosis-inducing proteins such as p53, FoxO1, FoxO3a, and tumor necrosis factorrelated apoptosis-inducing ligand (TRAIL) (66–68). Isotretinoin treatment only increased TRAIL expression in sebocytes but not in keratinocytes. TRAIL expression localized within basal and suprabasal layers of sebaceous glands increased after 1 week of isotretinoin therapy (6). Importantly, ATRA upregulates the expression of p53, a key transcription factor regarded as the guardian of the genome (66,69,70). The addition of isotretinoin to primary human keratinocytes increases the expression of p53 and FoxO1 (17). The expression of FoxO1, the 15 Mechanism of Action of Isotretinoin (a) (b) (c) (d) FIGURE 4.2 Characteristic immunohistochemical staining pattern of (a) non-phosphorylated FoxO1 before isotretinoin treatment with predominant cytoplasmic FoxO1 distribution and (b) after 6 weeks of initiation of isotretinoin therapy with accentuated nuclear FoxO1 expression. Representative staining pattern of non-phosphorylated FoxO3 before isotretinoin treatment with predominant cytoplasmic FoxO3 distribution (c) and (d) after 6 weeks of initiation of isotretinoin therapy with accentuated nuclear FoxO3 expression. Original magnification ×400. (With kind permission of Agamia et al. Exp Dermatol. 2018;27:1344–1351 and Experimental Dermatology.) metabolic transcription factor of starvation (71), is increased in primary human sebocytes during serum starvation associated with increased expression of p53 (72). p53 is the key transcription factor promoting the expression of various pro-apoptotic proteins including FoxO1, FoxO3, and TRAIL (73–76). FoxO3a has been identified as a further promoter of TRAIL expression (77). Isotretinoin treatment of SEB-1 sebocytes induced p21 (cyclindependent kinase inhibitor 1A [CDKN1A]) resulting in p21-­ dependent cell cycle arrest (4). p21 is the prototype of p53 target genes (78). In isotretinoin-treated SEB-1 sebocytes, upregulation of p21 led to cell cycle arrest (4). p21 prevents phosphorylation of the retinoblastoma (Rb) protein maintaining E2F-regulated genes in a repressed state, which leads to downregulation of SREBP1c and its downstream target stearoyl-CoA desaturase 1 (SCD), resulting in a decrease in mono-unsaturation of membrane phospholipids, decreased phosphatidylinositol-(4,5)-diphosphate (PIP2) and (phosphatidylinositol-(3,4,5)-triphosphate (PIP3) levels, and ultimately decreased phosphorylation and activation of AKT (79). Chronic activation of p53 in mice results in a loss of sebaceous glands (80). B-lymphocyte-induced nuclear maturation protein 1 (BLIMP1), a recently identified marker of differentiated sebocytes (81), binds to the TP53 promoter and represses p53 transcription (82), whereas epidermal-specific deletion of BLIMP1 resulted in sebaceous gland enlargement (81). Taken together, there is a close interaction between ­isotretinoin-mediated upregulation of p53 and p53-dependent expression of pro-apoptotic genes including FoxO1, FoxO3a, and TRAIL that orchestrate sebocyte apoptosis. p53-p21 signaling induces cell cycle arrest and suppresses lipogenesis via downregulation of SREBP-1. Sebocyte apoptosis and suppression of sebaceous lipogenesis both reduce sebum production (83). The cell’s capacity to isomerize isotretinoin to ATRA and to express abundant intracellular CRABP-2 appear to be the pivotal requirements for isotretinoin’s p53-mediated pro-apoptotic and sebumsuppressive effects (61,64,84). Neuroblastoma Treatment and Teratogenicity Isotretinoin/ATRA-mediated upregulation of p53 and proapoptotic p53-induced targets including FoxO1, FoxO3a, and TRAIL also explains its tumor-suppressive effect (7–16,85). Isotretinoin is effective in the treatment of neuroblastoma (9–12). Intracellular isomerization of isotretinoin to ATRA plays a key role for its activity in neuroblastoma cells (11); however, when neuroblastoma cells becomes ATRA-resistant (86), isotretinoin promotes proliferation and reduces p53 signaling (87). Neuroblastoma is a tumor of the neural crest (88). Animal studies have confirmed that administration of isotretinoin increases apoptosis of neural crest cells (89–91). Accumulating translational evidence supports the view that isotretinoininduced upregulation of p53 promotes neural crest cell apoptosis, explaining isotretinoin-mediated teratogenicity (for further details see Chapter 10) (19). Alterations of Skin Barrier Function Isotretinoin treatment consistently induces mucocutaneous side effects by exhibiting dry skin with increased transepidermal water loss, often leading to retinoid dermatitis (93,94). Aquaporin 3 (AQP3) is an aquaglyceroporin which transports 16 water, glycerol, and small solutes across the plasma membrane (95). Elevated expression level of AQP3 results in impaired barrier integrity and increased pro-inflammatory cytokine production, mimicking the pathologic conditions in Notch-deficient mice and in atopic dermatitis (96). ATRA, and especially isotretinoin, enhanced the expression of AQP3 in human keratinocytes and human skin (97,98). At the promoter level, the expression of AQP3 is induced by p53 (99,100). As a result, isotretinoin-induced upregulation of AQP3 explains isoretinoin’s adverse effect on epidermal barrier homeostasis. Aquaporin 1 (AQP1) is widely distributed in the human brain and is associated with water secretion into the subarachnoid space. Notably, AQP1 is an ATRA-inducible gene (101) that has been linked to retinoid-induced intracranial hypertension (102), which is a known potential adverse effect of systemic isotretinoin treatment (103). Stratum corneum ceramides play key functions in epidermal barrier homeostasis. There is recent evidence for the involvement of p53 in the regulation of ceramide metabolism (104). Telogen Effluvium Long-term use of isotretinoin in higher doses affects hair growth and is associated with increased hair loss and telogen effluvium (105,106). Hair follicles undergo repetitive stages of cell proliferation and programmed cell death. The catagen stage of physiologic apoptosis is connected with dynamic changes in morphology and alterations in gene expression (107,108). ATRA induces premature hair follicle regression, leading to a catagenlike stage in human hair follicles (109). It has been demonstrated in murine hair follicles that p53 is strongly expressed and colocalized with apoptotic markers in the regressing hair follicle compartments during catagen. This suggests that p53 is involved in the control of apoptosis in the hair follicle during physiologic regression (110). Upregulation of p53 may thus explain the molecular basis of isotretinoin-induced hair loss. Risk of Depression Isotretinoin-associated depression is a matter of concern and appears to develop in a small subgroup of vulnerable predisposed individuals, particularly those with a personal or family history of mental disorders (111,112). Recent theories for the pathogenesis of depression suggest decreased hippocampal and prefrontal cortex neurogenesis (113–115). Isotretinoin treatment of mice decreased hippocampal neurogenesis and reduced hippocampal volume (116,117). Treatment of hypothalamic cells with 10 µM isotretinoin for 48 h decreased cell growth to 45.6 ± 13% of control (118). Intracerebroventricularly applied ATRA to adult rats increased RAR-α protein expression in the hippocampus and impaired hippocampal neurogenesis correlated with depressionlike symptoms (119). Isotretinoin and ATRAs at high concentrations negatively affect the dendritic morphology of cultured hippocampal neurons mediated through RARs (120). RARA polymorphisms may define individuals with increased risk for isotretinoin-induced adverse drug effects including depression (121). Enhanced Retinoids in Dermatology isotretinoin-ATRA-RARA-p53 signaling may thus explain increased hippocampal apoptosis that results in isotretinoinmediated depression. Intriguingly, the common antidepressant lithium, which induces acneiform drug reactions (122), reduces apoptosis and p53 expression in the hippocampus (123). Hypertriglyceridemia Isotretinoin treatment can induce moderate to severe hypertriglyceridemia in about 25% of patients (124,125). Isotretinoininduced hypertriglyceridemia in rats is mediated by RARs (126). Isotretinoin treatment increases plasma very low-density lipoprotein (VLDL) levels and VLDL apolipoprotein B-100 (apoB-100) (127). Hepatic VLDL synthesis is controlled by FoxO1. Augmented FoxO1 activity promotes hepatic VLDL overproduction and predisposes to the development of hypertriglyceridemia (128). Triglyceride loading to apoB-100 is facilitated by microsomal triglyceride transfer protein (MTP), which is activated by FoxO1 (129,130). Each VLDL molecule contains one apoB-100, which is required for triglyceride loading onto the VLDL particle. ApoB-100 and apoB-48 are created by a premature stop codon by apoB mRNA-editing enzyme complex 1 (apobec1). A p53 response element (p53RE) has been identified in the genes encoding for apoB and apobec1 and confirmed that these genes are transcriptionally regulated by p53 (131). Isotretinoinmediated upregulation of p53 in the liver may explain p53- and FoxO1-induced VLDL hypertriglyceridemia. Cross-Talk between Isotretinoin, Vitamin D, and p53 Increasing attention has been paid to the contribution of ­vitamin D deficiency in the pathogenesis of acne (132–134). The level of 25-hydroxyvitamin D is inversely associated with the severity of acne (135,136). Isotretinoin treatment of acne patients increases serum levels of 25-hydroxy- and 1,25-dihydroxyvitamin D (136,137). Remarkably, a cross-talk between vitamin D and p53-signaling occurs at different levels. p53 promotes the expression of vitamin D receptor (VDR) (138), which in synergy with p53 stimulates the expression of p21 (139), a critical cell cycle inhibitor which is upregulated in isotretinoin-treated SEB-1 sebocytes (4). Increased IGF-1-PI3K-AKT signaling in acne activates mouse double minute 2 (MDM2) (140,141), the key negative regulator of p53 promoting proteasomal degradation of p53 (142). ATRA activates p14 expression resulting in ubiquitin-dependent degradation of MDM2 and subsequent stabilization of p53 (143). MDM2 binds to FoxO1 and FoxO3a and promotes their ubiquitination and degradation (144). p53, FoxO1, FoxO3a, and VDR are all bound and inhibited by MDM2 (145,146). Both 1,25-dihydroxyvitamin D and ATRA increase the transcription of VDR in blood cells (147,148). VDR promotes the transcription of DNA-damage inducible transcript 4 (DDIT4), which is a negative regulator of mTORC1 (149). mTORC1 is suppressed by p53 at various checkpoints (150). p53 inhibits the expression of IGF-1 receptor (IGF1R) (151) and AR (54,55), but increases the expression of phosphatase and tensin homolog 17 Mechanism of Action of Isotretinoin (PTEN), FoxO1, FoxO3a, and VDR (70,138), and thereby inhibits IGF-1-PI3K-AKT-mTORC1 signaling, which is upregulated in sebaceous glands of acne patients (26–28). Isotretinoin via upregulation of p53 and vitamin D/VDR signaling in a synergistic fashion decreases mTORC1 activity and promotes cell cycle arrest and apoptosis. Notably, activated mTORC1 augments the expression of IL-17 (152). In contrast, ATRA and 1,25-dihydroxyvitamin D3 inhibited Propionibacterium acnesinduced Th17 differentiation and IL-17 synthesis (153), underlining the biologic cross-talk between isotretinoin, p53, and vitamin D in acne. Paradoxic Effects in Immortalized Sebocytes In analogy with findings in sebaceous glands of acne patients (24,28,42), IGF-1-stimulated PI3K/AKT signaling reduces nuclear levels of FoxO1 proteins in immortalized SZ95 sebocytes (154); however, when studying the pharmacologic effect of isotretinoin in immortalized SZ95 sebocytes, investigators observed a paradoxic activation of PI3K/AKT. This results in decreased nuclear FoxO1 levels and leads to the erroneous conclusion that isotretinoin may not attenuate PI3K/AKT signaling (155) as predicted earlier (40). In SEB-1 immortalized sebocytes, the addition of isotretinoin unexpectedly increases the expression of sterol regulatory element-binding protein 1 (SREBP1) and enhanced sebocyte lipogenesis (156); notably, the expression of SREBP1 is negatively controlled by p53 (79,157,158). To understand this paradox, it is of critical importance to remember that immortalized SZ95- and SEB1 sebocytes are derived from human sebocytes transfected with Simian virus (SV40) (159,160). The key mechanism of immortalization is SV40 large T antigen-mediated complex formation with p53 resulting in p53 inactivation (161,162). SV40 large T antigenmediated inactivation prevents adequate p53-mediated apoptosis resulting in immortalization. The addition of isotretinoin (10−8–10−5 mol/L) to SZ95 sebocytes did not affect externalized phosphatidylserine levels, DNA fragmentation, and lactate dehydrogenase cell release, despite increased caspase 3 levels (163). Importantly, SV40 large T antigen-p53 complexes bind and activate the IGF1 promoter stimulating IGF-1/PI3K/AKT-mediated cell growth and survival (164). By using the PI3K inhibitor LY294002, isotretinoin-mediated upregulation of AKT-signaling in SZ95 sebocytes could be located to be upstream of PI3K (155). Thus, SV40 large T antigenp53 complex formation increased IGF-1 expression and reduced the inhibitory effects of p53 in both IGF-1 receptor expression and p53-mediated expression of PTEN. This results in enhanced IGF-1/PI3K/AKT signaling of isotretinoin-treated SZ95 sebocytes. In addition, SV40 large T antigen-mediated inactivation of p53 enhances SREBP-1 expression. Unfortunately, immortalized p53-inactivated SZ95- and SEB-1 sebocytes are not suitable cell models to study the pharmacologic effects of isotretinoin (165). Normalization of Disturbed Keratinization Disturbed follicular keratinization and comedogenesis are hallmarks of acne pathogenesis (24,166). Isotretinoin normalizes the pattern of keratinization within the sebaceous follicle (167). It inhibits the expression of cytokeratin 1/10, 14, filaggrin, and matrix metalloproteinase-3 (MMP3), but it enhances cytokeratin 7, 13, 19, and laminin B1, as well as IL-1 in normal human ­epidermal keratinocytes. Isotretinoin and ATRA show similar effects on cell growth in primary human keratinocytes and HaCaT cultures tested with increasing proliferation at low cell densities. They are rather inactive at high ones in normal keratinocytes and exhibit an antiproliferative effect in HaCaT keratinocytes (168). Isotretinoin added to human pilosebaceous ducts in culture causes an additional significant reduction in the rate of [3H] thymidine uptake, pointing to reduced epithelial duct proliferation during isotretinoin treatment (169). Isotretinoin reduced proliferation of primary human keratinocytes (HPKs) is associated with enhanced expression of p53, FoxO1, and p21, but there are also reduced phosphorylated FoxO1 and involucrin expressions (17). FoxO1 promotes differentiation and apoptosis in HPKs, whereas IGF-1 reduces keratinocyte differentiation through PI3K/AKT/FoxO1 pathway (17). Notably, the p53 target TRAIL, which plays a role in keratinocyte differentiation (170) and sebocyte apoptosis (6), is not increased in human epidermal keratinocytes in response to isotretinoin (6). This may explain the higher susceptibility of sebocytes for isotretinoin-induced apoptosis compared to keratinocytes. The primary change found in cellular material expressed from open comedones of isotretinoin-treated patients is disintegration of desmosomes associated with a lack of cohesion between cornified cells (171). In mice models, isotretinoin-disturbed barrier function results in increased transepidermal water loss and stratum corneum loosening (172). Isotretinoin also modifies the composition of intercorneocyte lipids, the mortar-like domain which is responsible for the barrier function of the stratum corneum. In comedones of patients systemically treated with isotretinoin, the relative amounts of total ceramides increase in relation to non-ceramide lipids (173). As a result, isotretinoin exerts various modes of actions in hyperproliferative disorders of keratinization, including anti-comedogenic effects in acne. Inflammatory and Anti-Inflammatory Action Inflammatory flares during the initiation of isotretinoin treatment may result from increased expression of 5-lipoxygenase (ALOX5) (156), which is a direct p53-target gene (174). Longterm anti-inflammatory effects of isotretinoin in acne are either indirectly mediated by isotretinoin-p53-induced sebocyte ­apoptosis with consecutive reduction of pro-inflammatory acne sebum or directly induced by isotretinoin-p53-mediated suppression of nuclear factor κB (NF-κB) dependent expression of pro-inflammatory mediators (175). IGF-1-stimulated sebocytes produce IL-1β and other pro-inflammatory cytokines (30). In addition, sebum-derived lipids augment the secretion of IL-1β, even in the absence of P. acnes (176). Sebum lipids influence macrophage polarization and activation (173). Sebum supports the growth of P. acnes, which triggers tolllike receptor 2 (TLR2)-induced pro-inflammatory cytokine production (177). TLR-2 recognizes P. acnes CAMP f­actor 1 from highly inflammatory strains (178). Oral isotretinoin reduces 18 Retinoids in Dermatology clinical acne grades, the abundance of P. acnes, decreased blood monocyte TLR-2 expression, and subsequent inflammatory cytokine response to P. acnes (179,180). Several weeks after isotretinoin treatment of acne patients, blood serum levels of IL-1α, IL-1β, IL-4, IL-17, tumor necrosis factor-α (TNF-α), and IFN-γ levels are decreased (181,182). Isotretinoin treatment reduces sebum levels of matrix metalloproteinase (MMP) 9 and MMP-13 (183). Recently, increased Th17/IL-17 signaling has been regarded as the crucial ­pro-inflammatory pathway in acne pathogenesis (184). ATRA acts as a key regulator of TGF-β-dependent immune responses, capable of inhibiting the IL-6-driven induction of pro-inflammatory Th17 cells and promoting anti-inflammatory regulatory T cell (Treg) differentiation (185). Agents such as isotretinoin and vitamin D3, which target the Th17 pathway, appear to attenuate Th17-driven inflammatory skin diseases including acne and hidradenitis suppurativa (acne inversa) (186,187). Notably, binding of p53 to STAT3 suppresses Th17 cell differentiation, whereas deficiency of p53 enhances Th-17 cell differentiation (188). In the skin of acne patients, IL-1β and TLR-2 mRNA expression are markedly reduced by isotretinoin treatment, whereas there is higher mRNA expression of TRAIL and lipocalin 2 (LCN2) in acne lesions during isotretinoin treatment (189). In the serum of these patients, isotretinoin lowers the levels of TNF-α, IL-17A, and IFN-γ. Isotretinoin treatment reduces acne lesions but not directly lesional acne inflammation, and enhances the numbers of infiltrating macrophages (189). Remarkably, in primary human monocytes and macrophages, p53 and NF-κB co-regulate the expression of pro-inflammatory genes (190). Neutrophils and macrophages lacking p53 (p53−/−) have elevated responses to LPS stimulation compared with p53+/+ cells, producing greater amounts of pro-inflammatory cytokines, including TNF-α, IL-6, and MIP-2, and demonstrating enhanced NF-κB DNA-binding activity (191). Skin expression levels of cathelicidin, human β-defensin 2, lactoferrin, psoriasin (S100A7), and koebnerisin (S100A15) decrease during isotretinoin treatment (192). This constellation is in synergy with epidermal barrier disruption and explains the increased risk for cutaneous Staphylococcus aureus infections during isotretinoin treatment (193). Delayed Wound Healing Clinical observations suggest that wound healing may be altered in patients treated with systemic isotretinoin (194). Mechanical dermabrasion and fully ablative laser surgery are not recommended in the setting of systemic isotretinoin treatment (195). p53, which is upregulated by isotretinoin, impairs wound healing, whereas inhibition of p53 enhances wound healing (196,197). p53 is an inducer of S100A2 (198), which forms a complex with p53 that potentiates p53-mediated transcription and increases p53 expression (199). It has recently been demonstrated in epithelialspecific S100A2 transgenic mice that the p53-S100A2 positive TABLE 4.1 p53-Regulated Target Genes Involved in Isotretinoin’s Mode of Action p53 Target Genes Tumor necrosis factor-related apoptosis-inducing ligand, TRAIL (TNFSF10) upregulation Insulin-like growth factor-1 receptor (IGF1R) suppression Androgen receptor (AR) suppression IGF binding protein-3 (IGFBP3) upregulation Cyclin-dependent kinase inhibitor 1A, p21 (CDKN1A) upregulation B lymphocyte-induced maturation protein 1 (BLIMP1) (PRDM1) upregulation Sestrin 1 (SESN1) and sestrin 2 (SESN2) upregulation Forkhead box O1 (FOXO1) upregulation Forkhead box O3a (FOXO3A) upregulation AMP-activated protein kinase (PRKAA1) Aquaporin 3 (AQP3) upregulation Aquaporin 1 (AQP1) upregulation Apolipoprotein B100 (APOB) and apoB mRNA editing enzyme complex 1 (APOBEC1) Vitamin D receptor (VDR) Sterol response element-binding protein 1 c (SREBF1) Desired and Adverse Drug Effects Sebocyte apoptosis: sebum suppression Meibomian cell apoptosis: dry eyes Neural crest cell apoptosis: teratogenicity Hypothalamic cell apoptosis: depression Attenuated pro-survival and mitogenic signaling of IGF-1 Reduced AR expression Enhanced pro-apoptotic signaling and suppressed PPAR-γ signaling: attenuated lipogenesis G1/S cell cycle arrest: suppression of comedogenesis and keratinocyte proliferation, suppression of sebocyte proliferation Increased BLIMP1-mediated c-MYC suppression reducing sebocyte differentiation Activation of AMPK inhibiting mTORC1, sebum suppression Suppression of AR, SREBP1c and PPAR-γ; suppression of lipogenesis; suppression of POMC, suppression of ACTH Enhanced upregulation of TRAIL: enhancement of apoptosis; suppression of POMC Increased expression of AMPK and AMPK-mediated inhibition of mTORC1 Increased aquaporin 3 expression: increased transepidermal water loss, dry skin, xerosis Increased aquaporin 1 expression increasing cerebrospinal fluid, increased risk of pseudotumor cerebri Increased hepatic synthesis of apoB100, hypertriglyceridemia with increased hepatic secretion of triglyceride-rich VLDL Increased vitamin D signaling, suppression of cell proliferation, suppression of mTORC1 Decreased expression of SREBP-1 with suppression of lipogenesis, sebum suppression Mechanism of Action of Isotretinoin feedback loop negatively regulates epithelialization in cutaneous wound healing (175). Pyogenic Granuloma Increased risk of granuloma pyogenicum formation has been reported during systemic isotretinoin treatment (200). These vascular lesions spontaneously resolve once isotretinoin is discontinued (201). Pyogenic granuloma has been related to increased expression of vascular endothelial growth factor (VEGF) (202). Notably, the p53 target gene FOXO1 directly regulates VEGF expression and is needed for normal angiogenesis during wound healing (92,203). Isotretinoin-p53-mediated overexpression of FoxO1 may promote VEGF-induced pyogenic granuloma. Conclusions After four decades of following isotretinoin’s clinical introduction as the most effective drug in the treatment of severe acne, we are able to understand its molecular mode of action. Accumulating evidence underscores isotretinoin’s sebumsuppressive mode of action in acne, its beneficial effects in disorders of keratinization, its endocrine effects, its apoptosisinducing activity, and its anti-inflammatory actions, as well as its adverse effects, all of which are related to enhanced expression of p53 and modified expression of p53 target genes (Table 4.1). Isotretinoin-mediated upregulation of p53 explains its desired pharmacologic efficacy in acne, in disorders of keratinization, and in childhood neuroblastoma as well as its adverse effects, including teratogenicity. Immortalized sebocytes with SV40 large T antigen-­mediated inactivation of p53 are not suitable in vitro models to study isotretinoin’s mode of action under physiologic or clinical conditions. Experimental data derived from immortalized p53-inactivated sebocytes should be considered with caution, as p53, the guardian of the genome, is involved in multiple signaling cascades regulating cell homeostasis, metabolism, cell-cycle ­ control, and apoptosis. REFERENCES 1. Peck GL, Olsen TG, Yoder FW, Strauss JS, Downing DT et al. Prolonged remissions of cystic and conglobate acne with 13-cis-retinoic acid. N Engl J Med. 1979;300:329–333. 2. Landthaler M, Kummermehr J, Wagner A, Plewig G. Inhibitory effects of 13-cis-retinoic acid on human sebaceous glands. Arch Dermatol Res. 1980;269:297–309. 3. Strauss JS, Stranieri AM. Changes in long-term sebum production from isotretinoin therapy. J Am Acad Dermatol. 1982;6:751–756. 4. Nelson AM, Gilliland KL, Cong Z, Thiboutot DM. 13-cis Retinoic acid induces apoptosis and cell cycle arrest in human SEB-1 sebocytes. J Invest Dermatol. 2006;126:2178–2189. 5. Nelson AM, Zhao W, Gilliland KL, Zaenglein AL, Liu W, Thiboutot DM. Neutrophil gelatinase-associated lipocalin mediates 13-cis retinoic acid-induced apoptosis of human sebaceous gland cells. J Clin Invest. 2008;118:1468–1478. 19 6. Nelson AM, Cong Z, Gilliland KL, Thiboutot DM. TRAIL contributes to the apoptotic effect of 13-cis retinoic acid in human sebaceous gland cells. Br J Dermatol. 2011;165:526–533. 7. Bettoli V, Zauli S, Virgili A. Retinoids in the chemoprevention of non-melanoma skin cancers: Why, when and how. J Dermatolog Treat. 2013;24:235–237. 8. Graf N, Riesinger P, Reinhard H. Retinoids in the treatment of acute promyelocytic leukemia. Review of the literature. Klin Padiatr. 1995;207:43–47. 9. Masetti R, Biagi C, Zama D, Vendemini F, Martoni A, Morello W et al. Retinoids in pediatric onco-hematology: The model of acute promyelocytic leukemia and neuroblastoma. Adv Ther. 2012;29:747–762. 10. Ponthan F, Borgström P, Hassan M, Wassberg E, Redfern CP, Kogner P. The vitamin A analogues: 13-cis retinoic acid, 9-cis retinoic acid, and Ro 13–6307 inhibit neuroblastoma tumour growth in vivo. Med Pediatr Oncol. 2001;36:127–131. 11. Veal G, Rowbotham S, Boddy A. Pharmacokinetics and pharmacogenetics of 13-cis-retinoic acid in the treatment of neuroblastoma. Therapie. 2007;62:91–93. 12. Cash T, Alazraki A, Qayed M, Katzenstein HM. Prolonged isotretinoin in ultra high-risk neuroblastoma. J Pediatr Hematol Oncol. 2017;39:e33–e35. 13. Li M, Sun Y, Guan X, Shu X, Li C. Advanced progress on the relationship between RA and its receptors and malignant tumors. Crit Rev Oncol Hematol. 2014;91:271–282. 14. Guruvayoorappan C, Pradeep CR, Kuttan G. 13-cis-retinoic acid mediates apoptosis in Dalton’s lymphoma ascites cells by regulating gene expression. J Basic Clin Physiol Pharmacol. 2007;18:267–276. 15. Maeda Y, Miyatake J, Sono H, Matsuda M, Tatsumi Y, Horiuchi F et al. 13-cis retinoic acid inhibits growth of adult T cell leukemia cells and causes apoptosis; possible new indication for retinoid therapy. Intern Med. 1996;35:180–184. 16. Guruvayoorappan C, Pradeep CR, Kuttan G. 13-cis-retinoic acid induces apoptosis by modulating caspase–3, bcl–2, and p53 gene expression and regulates the activation of transcription factors in B16F–10 melanoma cells. J Environ Pathol Toxicol Oncol. 2008;27:197–207. 17. Shi G, Liao PY, Cai XL, Pi XX, Zhang MF, Li SJ et al. FoxO1 enhances differentiation and apoptosis in human primary keratinocytes. Exp Dermatol. 2018;27:1254–1260. 18. Melnik BC. Apoptosis may explain the pharmacological mode of action and adverse effects of isotretinoin, including teratogenicity. Acta Derm Venereol. 2017;97:173–181. 19. Melnik BC. Overexpression of p53 explains isotretinoin’s ­teratogenicity. Exp Dermatol. 2018;27:91–93. 20. Goldstein JA, Comite H, Mescon H, Pochi PE. Isotretinoin in the treatment of acne: Histologic changes, sebum production, and clinical observations. Arch Dermatol. 1982;118:555–558. 21. Zelickson AS, Strauss JS, Mottaz J. Ultrastructural changes in sebaceous glands following treatment of cystic acne with isotretinoin. Am J Dermatopathol. 1986;8:139–143. 22. Nelson AM, Zhao W, Gilliland KL, Zaenglein AL, Liu W, Thiboutot DM. Early gene changes induced by isotretinoin in the skin provide clues to its mechanism of action. Dermatoendocrinol. 2009;1:100–101. 23. Nelson AM, Zhao W, Gilliland KL, Zaenglein AL, Liu W, Thiboutot DM. Temporal changes in gene expression in the skin of patients treated with isotretinoin provide insight into its mechanism of action. Dermatoendocrinol. 2009;1:177–187. 20 24. Melnik BC. Acne vulgaris: The metabolic syndrome of the pilosebaceous follicle. Clin Dermatol. 2018;36:29–40. 25. Smith TM, Gilliland K, Clawson GA, Thiboutot D. IGF–1 induces SREBP–1 expression and lipogenesis in SEB–1 sebocytes via activation of the phosphoinositide 3-kinase/Akt pathway. J Invest Dermatol. 2008;128:1286–1293. 26. Melnik BC, Zouboulis CC. Potential role of FoxO1 and mTORC1 in the pathogenesis of Western diet-induced acne. Exp Dermatol. 2013;22:311–315. 27. Monfrecola G, Lembo S, Caiazzo G, De Vita V, Di Caprio R, Balato A et al. Mechanistic target of rapamycin (mTOR) expression is increased in acne patients’ skin. Exp Dermatol. 2016;25:153–155. 28. Agamia NF, Abdallah DM, Sorour O, Mourad B, Younan DN. Skin expression of mammalian target of rapamycin and forkhead box transcription factor O1, and serum insulin-like growth factor-1 in patients with acne vulgaris and their relationship with diet. Br J Dermatol. 2016;174:1299–1307. 29. Melnik BC. Acne vulgaris: An inflammasomopathy of the sebaceous follicle induced by deviated FoxO1/mTORC1 ­signalling. Br J Dermatol. 2016;174:1186–1188. 30. Kim H, Moon SY, Sohn MY, Lee WJ. Insulin-like growth factor-1 increases the expression of inflammatory biomarkers and sebum production in cultured sebocytes. Ann Dermatol. 2017;29:20–25. 31. Melnik BC, Schmitz G. Role of insulin, insulin-like growth ­factor-1, hyperglycaemic food and milk consumption in the pathogenesis of acne vulgaris. Exp Dermatol. 2009;18:833–841. 32. Ju Q, Tao T, Hu T, Karadağ AS, Al-Khuzaei S, Chen W. Sex hormones and acne. Clin Dermatol. 2017;35:130–137. 33. Assaf HA, Abdel-Maged WM, Elsadek BE, Hassan MH, Adly MA, Ali SA. Survivin as a novel biomarker in the pathogenesis of acne vulgaris and its correlation to insulin-like growth factor-I. Dis Markers. 2016;2016:7040312. 34. Melnik BC. FoxO1—The key for the pathogenesis and therapy of acne? J Dtsch Dermatol Ges. 2010;8:105–114. 35. Zhang X, Tang N, Hadden TJ, Rishi AK. Akt, FoxO and regulation of apoptosis. Biochim Biophys Acta. 2011;1813:1978–1986. 36. Eijkelenboom A, Burgering BM. FOXOs: Signalling integrators for homeostasis maintenance. Nat Rev Mol Cell Biol. 2013;14:83–97. 37. Tsitsipatis D, Klotz LO, Steinbrenner H. Multifaceted functions of the forkhead box transcription factors FoxO1 and FoxO3 in skin. Biochim Biophys Acta Gen Subj. 2017;1861:1057–1064. 38. Melnik BC. The TRAIL to acne pathogenesis: Let’s focus on death pathways. Exp Dermatol. 2017;26:270–272. 39. Melnik BC. Is nuclear deficiency of FoxO1 due to increased growth factor/PI3K/Akt- signalling in acne vulgaris reversed by isotretinoin treatment? Br J Dermatol. 2010;162:1398–1400. 40. Melnik BC. Isotretinoin and FoxO1: A scientific hypothesis. Dermatoendocrinol. 2011;3:141–165. 41. Agamia NF, Hussein OM, Abdelmaksoud RE, Abdalla DM, Talaat IM, Zaki EI et al. Effect of oral isotretinoin on the nucleo-cytoplasmic distribution of FoxO1 and FoxO3 proteins in sebaceous glands of patients with acne vulgaris. Exp Dermatol. 2018;27:1344–1351. 42. Seleit I, Bakry OA, Abdou AG, Hashim A. Body mass index, selected dietary factors, and acne severity: Are they related to in situ expression of insulin-like growth factor-1? Anal Quant Cytopathol Histpathol. 2014;36:267–278. Retinoids in Dermatology 43. Kremer I, Gaton DD, David M, Gaton E, Shapiro A. Toxic effects of systemic retinoids on meibomian glands. Ophthalmic Res. 1994;26:124–128. 44. Moy A, McNamara NA, Lin MC. Effects of isotretinoin on Meibomian glands. Optom Vis Sci. 2015;92:925–930. 45. Dong XC, Copps KD, Guo S, Li Y, Kollipara R, DePinho RA et al. Inactivation of hepatic Foxo1 by insulin signaling is required for adaptive nutrient homeostasis and endocrine growth regulation. Cell Metab. 2008;8:65–76. 46. Fan W, Imamura T, Sonoda N, Sears DD, Patsouris D, Kim JJ et al. FOXO1 transrepresses peroxisome proliferator-activated receptor gamma transactivation, coordinating an insulininduced feed-forward response in adipocytes. J Biol Chem. 2009;284:12188–12197. 47. Wan X, Wang S, Xu J, Zhuang L, Xing K, Zhang M et al. Dietary protein-induced hepatic IGF–1 secretion mediated by PPARγ activation. PLOS ONE. 2017;12:e0173174. 48. Karadağ AS, Ertugrul DT, Tutal E, Akin KO. Short-term isotretinoin treatment decreases insulin-like growth ­factor-1 and insulin-like growth factor binding protein-3 levels: Does isotretinoin affect growth hormone physiology? Br J Dermatol. 2010;162:798–802. 49. Karadağ AS, Ertugrul DT, Tutal E, Akin KO. Isotretinoin influences pituitary hormone levels in acne patients. Acta Derm Venereol. 2011;91:31–34. 50. Uyar B, Solak A, Saklamaz A, Akyildiz M, Genc B, Gökduman A. Effects of isotretinoin on the thyroid gland and thyroid function tests in acne patients: A preliminary study. Indian J Dermatol Venereol Leprol. 2016;82:587–588. 51. Yıldırım N, Doğan S, Atakan N. Evaluation of thyroid function tests of acne vulgaris patients treated with systemic isotretinoin. J Dermatolog Treat. 2017;28:141–144. 52. Yang G, Lim CY, Li C, Xiao X, Radda GK, Li C et al. FoxO1 inhibits leptin regulation of pro-opiomelanocortin promoter activity by blocking STAT3 interaction with specificity protein 1. J Biol Chem. 2009;284:3719–3727. 53. Ma W, Fuentes G, Shi X, Verma C, Radda GK, Han W. FoxO1 negatively regulates leptin-induced POMC transcription through its direct interaction with STAT3. Biochem J. 2015;466:291–298. 54. Alimirah F, Panchanathan R, Chen J, Zhang X, Ho SM, Choubey D. Expression of androgen receptor is negatively regulated by p53. Neoplasia. 2007;9:1152–1159. 55. Shenk JL, Fisher CJ, Chen SY, Zhou XF, Tillman K, Shemshedini L. p53 represses androgen-induced transactivation of prostate-specific antigen by disrupting hAR aminoto carboxyl-terminal interaction. J Biol Chem. 2001;276: 38472–38479. 56. Fan W, Yanase T, Morinaga H, Okabe T, Nomura M, Daitoku H et al. Insulin-like growth factor 1/insulin signaling activates androgen signaling through direct interactions of Foxo1 with androgen receptor. J Biol Chem. 2007;282:7329–7338. 57. Boudou P, Soliman H, Chivot M, Villette JM, Vexiau P, Belanger A et al. Effect of oral isotretinoin treatment on skin androgen receptor levels in male acneic patients. J Clin Endocrinol Metab. 1995;80:1158–1161. 58. Boudou P, Chivot M, Vexiau P, Soliman H, Villette JM, Julien R et al. Evidence for decreased androgen 5 alpha-reduction in skin and liver of men with severe acne after 13-cis-retinoic acid treatment. J Clin Endocrinol Metab. 1994;78:1064–1069. Mechanism of Action of Isotretinoin 59. Cottle DL, Kretzschmar K, Schweiger PJ, Quist SR, Gollnick HP, Natsuga K et al. c-MYC-induced sebaceous gland differentiation is controlled by an androgen receptor/p53 axis. Cell Rep. 2013;3:427–441. 60. Bhat MK, Yu C, Yap N, Zhan Q, Hayashi Y, Seth P et al. Tumor suppressor p53 is a negative regulator in thyroid hormone receptor signaling pathways. J Biol Chem. 1997;272:28989–289893. 61. Tsukada M, Schröder M, Roos TC, Chandraratna RA, Reichert U, Merk HF et al. 13-cis retinoic acid exerts its specific activity on human sebocytes through selective intracellular isomerization to all-trans retinoic acid and binding to retinoid acid receptors. J Invest Dermatol. 2000;115:321–327. 62. Zouboulis CC, Korge B, Akamatsu H, Xia LQ, Schiller S, Gollnick H et al. Effects of 13-cis-retinoic acid, all-transretinoic acid, and acitretin on the proliferation, lipid synthesis and keratin expression of cultured human sebocytes in vitro. J Invest Dermatol. 1991;96:792–797. 63. Sitzmann JH, Bauer FW, Cunliffe WJ, Holland DB, Lemotte PK. In situ hybridization analysis of CRABP II expression in sebaceous follicles from 13-cis retinoic acid-treated acne patients. Br J Dermatol. 1995;133:241–248. 64. Napoli JL. Cellular retinoid binding-proteins, CRBP, CRABP, FABP5: Effects on retinoid metabolism, function and related diseases. Pharmacol Ther. 2017;173:19–33. 65. Wei LN. Cellular retinoic acid binding proteins: Genomic and non-genomic functions and their regulation. Subcell Biochem. 2016;81:163–178. 66. Gudas LJ, Wagner JA. Retinoids regulate stem cell differentiation. J Cell Physiol. 2011;226:322–330. 67. Kim MJ, Ahn K, Park SH, Kang HJ, Jang BG, Oh SJ et al. SIRT1 regulates tyrosine hydroxylase expression and differentiation of neuroblastoma cells via FOXO3a. FEBS Lett. 2009;583:1183–1188. 68. Sakoe Y, Sakoe K, Kirito K, Ozawa K, Komatsu N. FOXO3A as a key molecule for all-trans retinoic acid-induced granulocytic differentiation and apoptosis in acute promyelocytic leukemia. Blood. 2010;115:3787–3795. 69. Lee DD, Stojadinovic O, Krzyzanowska A, Vouthounis C, Blumenberg M, Tomic-Canic M. Retinoid-responsive transcriptional changes in epidermal keratinocytes. J Cell Physiol. 2009;220:427–439. 70. Mrass P, Rendl M, Mildner M, Gruber F, Lengauer B, Ballaun C et al. Retinoic acid increases the expression of p53 and proapoptotic caspases and sensitizes keratinocytes to apoptosis: A possible explanation for tumor preventive action of retinoids. Cancer Res. 2004;64:6542–6548. 71. Gross DN, van den Heuvel AP, Birnbaum MJ. The role of FoxO in the regulation of metabolism. Oncogene. 2008;27:2320–2336. 72. Zhang MF, Cai XL, Jing KP, Pi XX, Liao PY, Li SJ et al. Differentiation model establishment and differentiationrelated protein screening in primary cultured human sebocytes. Biomed Res Int. 2018;2018:7174561. 73. Pappas K, Xu J, Zairis S, Resnick-Silverman L, Abate F, Steinbach N et al. p53 maintains baseline expression of multiple tumor suppressor genes. Mol Cancer Res. 2017;15:1051–1062. 74. Kurinna S, Stratton SA, Tsai WW, Akdemir KC, Gu W, Singh P et al. Direct activation of forkhead box O3 by tumor suppressors p53 and p73 is disrupted during liver regeneration in mice. Hepatology. 2010;52:1023–1032. 21 75. Renault VM, Thekkat PU, Hoang KL, White JL, Brady CA, Kenzelmann Broz D et al. The pro-longevity gene FoxO3 is a direct target of the p53 tumor suppressor. Oncogene. 2011;30:3207–3221. 76. Kuribayashi K, Krigsfeld G, Wang W, Xu J, Mayes PA, Dicker DT et al. TNFSF10 (TRAIL), a p53 target gene that mediates p53-dependent cell death. Cancer Biol Ther. 2008; 7:2034–2038. 77. Modur V, Nagarajan R, Evers BM, Milbrandt J. FOXO proteins regulate tumor necrosis factor-related apoptosis inducing ligand expression. Implications for PTEN mutation in prostate cancer. J Biol Chem. 2002;277:47928–479237. 78. Fischer M. Census and evaluation of p53 target genes. Oncogene. 2017;36:3943–3956. 79. Rueda-Rincon N, Bloch K, Derua R, Vyas R, Harms A, Hankemeier T et al. p53 attenuates AKT signaling by modulating membrane phospholipid composition. Oncotarget. 2015;6:21240–21254. 80. Kim J, Nakasaki M, Todorova D, Lake B, Yuan CY, Jamora C et al. p53 induces skin aging by depleting Blimp1+ sebaceous gland cells. Cell Death Dis. 2014;5:e1141. 81. Kretzschmar K, Cottle DL, Donati G, Chiang MF, Quist SR, Gollnick HP et al. BLIMP1 is required for postnatal epidermal homeostasis but does not define a sebaceous gland progenitor under steady-state conditions. Stem Cell Reports. 2014;3:620–633. 82. Yan J, Jiang J, Lim CA, Wu Q, Ng HH, Chin KC. BLIMP1 regulates cell growth through repression of p53 transcription. Proc Natl Acad Sci USA 2007;104:1841–1846. 83. Melnik BC. p53: Key conductor of all anti-acne therapies. J Transl Med. 2017;15:195. 84. Veal GJ, Errington J, Redfern CP, Pearson AD, Boddy AV. Influence of isomerisation on the growth inhibitory effects and cellular activity of 13-cis and all-trans retinoic acid in neuroblastoma cells. Biochem Pharmacol. 2002;63:207–215. 85. Celay J, Blanco I, Lázcoz P, Rotinen M, Castresana JS, Encío I. Changes in gene expression profiling of apoptotic genes in neuroblastoma cell lines upon retinoic acid treatment. PLOS ONE. 2013;8:e62771. 86. Ronca F, Yee KS, Yu VC. Retinoic acid confers resistance to p53-dependent apoptosis in SH-SY5Y neuroblastoma cells by modulating nuclear import of p53. J Biol Chem. 1999;274:18128–18134. 87. Waetzig V, Haeusgen W, Andres C, Frehse S, Reinecke K, Bruckmueller H et al. Retinoic acid-induced survival effects in SH-SY5Y neuroblastoma cells. J Cell Biochem. 2019;120(4):5974−5986. 88. Louis CU, Shohet JM. Neuroblastoma: Molecular pathogenesis and therapy. Annu Rev Med. 2015;66:49–63. 89. Johnston MC, Bronsky PT. Animal models for human craniofacial malformations. J Craniofac Genet Dev Biol. 1991; 11:277–291. 90. Watanabe T, Goulding EH, Pratt RM. Alterations in craniofacial growth induced by isotretinoin (13-cis-retinoic acid) in mouse whole embryo and primary mesenchymal cell culture. J Craniofac Genet Dev Biol. 1988;8:21–33. 91. Lammer EJ, Armstrong DL. Malformations in hindbrain structures among humans exposed to isotretinoin (13-cis retinoic acid) during early embryogenesis. In: Morriss-Kay G, editor. Retinoids in Normal Development and Teratogenesis. New York: Oxford University Press, 1991; pp. 281–295. 22 92. Ren B. FoxO1 transcriptional activities in VEGF expression and beyond: A key regulator in functional angiogenesis? J Pathol. 2018;245:255–257. 93. Çölgeçen E, Özyurt K, Ferahbaş Kesikoğlu A. The effect of systemic isotretinoin treatment on skin biophysical parameters among patients with acne vulgaris. Turk J Med Sci. 2016;46:1641–1644. 94. Lee JE, Chang JY, Lee SE, Kim MY, Lee JS, Lee MG et al. Epidermal hyperplasia and elevated HB-EGF are more prominent in retinoid dermatitis compared with irritant contact dermatitis induced by benzalkonium chloride. Ann Dermatol. 2010;22:290–299. 95. Boury-Jamot M, Daraspe J, Bonté F, Perrier E, Schnebert S, Dumas M et al. Skin aquaporins: Function in hydration, wound healing, and skin epidermis homeostasis. Handb Exp Pharmacol. 2009;(190):205–217. 96. Guo L, Chen H, Li Y, Zhou Q, Sui Y. An aquaporin 3-notch1 axis in keratinocyte differentiation and inflammation. PLOS ONE. 2013;8:e80179. 97. Bellemère G, Von Stetten O, Oddos T. Retinoic acid increases aquaporin 3 expression in normal human skin. J Invest Dermatol. 2008;128:542–548. 98. Xing F, Liao W, Jiang P, Xu W, Jin X. Effect of retinoic acid on aquaporin 3 expression in keratinocytes. Genet Mol Res. 2016;15:15016951. 99. Zheng X, Chen X. Aquaporin 3, a glycerol and water transporter, is regulated by p73 of the p53 family. FEBS Lett. 2001;489:4–7. 100. Choudhary V, Olala LO, Kagha K, Pan ZQ, Chen X, Yang R et al. Regulation of the glycerol transporter, aquaporin-3, by histone deacetylase-3 and p53 in keratinocytes. J Invest Dermatol. 2017;137:1935–1944. 101. Umenishi F, Schrier RW. Induction of human aquaporin-1 gene by retinoic acid in human erythroleukemia HEL cells. Biochem Biophys Res Commun. 2002;293:913–917. 102. Stiebel-Kalish H, Eyal S, Steiner I. The role of aquaporin-1 in idiopathic and drug-induced intracranial hypertension. Med Hypotheses. 2013;81:1059–1062. 103. Lee AG. Pseudotumor cerebri after treatment with tetracycline and isotretinoin for acne. Cutis. 1995;55:165–168. 104. Jeffries KA, Krupenko NI. Ceramide signaling and p53 pathways. Adv Cancer Res. 2018;140:191–215. 105. Heilgemeir GP, Braun-Falco O, Plewig G, Sund M. Effect of 13-cis-retinoic acid on hair growth. Hautarzt. 1982;33:533–536. 106. Kmieć ML, Pajor A, Broniarczyk-Dyła G. Evaluation of biophysical skin parameters and assessment of hair growth in patients with acne treated with isotretinoin. Postepy Dermatol Alergol. 2013;30:343–349. 107. Botchkareva NV, Ahluwalia G, Shander D. Apoptosis in the hair follicle. J Invest Dermatol. 2006;126:258–264. 108. Veselá B, Matalová E. Expression of apoptosis-related genes in the mouse skin during the first postnatal catagen stage, focused on localization of Bnip3L and caspase-12. Connect Tissue Res. 2015;56:326–335. 109. Foitzik K, Spexard T, Nakamura M, Halsner U, Paus R. Towards dissecting the pathogenesis of retinoid-induced hair loss: All-trans retinoic acid induces premature hair follicle regression (catagen) by upregulation of transforming growth factor-beta2 in the dermal papilla. J Invest Dermatol. 2005;124:1119–1126. Retinoids in Dermatology 110. Botchkarev VA, Komarova EA, Siebenhaar F, Botchkareva NV, Sharov AA, Komarov PG et al. p53 involvement in the control of murine hair follicle regression. Am J Pathol. 2001;158:1913–1919. 111. Bremner JD, Shearer KD, McCaffery PJ. Retinoic acid and affective disorders: The evidence for an association. J Clin Psychiatry. 2012;73:37–50. 112. Oliveira JM, Sobreira G, Velosa J, Telles Correia D, Filipe P. Association of isotretinoin with depression and suicide: A review of current literature. J Cutan Med Surg. 2018;22:58–64. 113. Sapolsky RM. Depression, antidepressants and the shrinking hippocampus. Proc Natl Acad Sci USA. 2001;98:12320–12322. 114. Vaidya VA, Fernandes K, Jha S. Regulation of adult hippocampal neurogenesis: Relevance to depression. Expert Rev Neurother. 2007;7:853–864. 115. Apple DM, Fonseca RS, Kokovay E. The role of adult neurogenesis in psychiatric and cognitive disorders. Brain Res. 2017;1655:270–276. 116. Sakai Y, Crandall JE, Brodsky J, McCaffery P. 13-cis retinoic acid (Accutane) suppresses hippocampal cell survival in mice. Ann NY Acad Sci. 2004;1021:436–440. 117. Crandall J, Sakai Y, Zhang J, Koul O, Mineur Y, Crusio WE et al. 13-cis-retinoic acid suppresses hippocampal cell division and hippocampal-dependent learning in mice. Proc Natl Acad Sci USA. 2004;101:5111–5116. 118. Griffin JN, Pinali D, Olds K, Lu N, Appleby L, Doan L et al. 13-Cis-retinoic acid decreases hypothalamic cell number in vitro. Neurosci Res. 2010;68:185–190. 119. Hu P, Wang Y, Liu J, Meng FT, Qi XR, Chen L, van Dam AM. Chronic retinoic acid treatment suppresses adult hippocampal neurogenesis, in close correlation with depressive-like behavior. Hippocampus. 2016;26:911–923. 120. Liu Y, Kagechika H, Ishikawa J, Hirano H, Matsukuma S, Tanaka K et al. Effects of retinoic acids on the dendritic morphology of cultured hippocampal neurons. J Neurochem. 2008;106:1104–1116. 121. Alzoubi KH, Khabour OF, Hassan RE, Qarqaz F, Al-Azzam S, Mhaidat N. The effect of genetic polymorphisms of RARA gene on the adverse effects profile of isotretinoin-treated acne patients. Int J Clin Pharmacol Ther. 2013;51:631–640. 122. Scarfi F, Arunachalam M. Lithium acne. CMAJ. 2013;185:1525. 123. Liechti FD, Stüdle N, Theurillat R, Grandgirard D, Thormann W, Leib SL. The mood-stabilizer lithium prevents hippocampal apoptosis and improves spatial memory in experimental meningitis. PLOS ONE. 2014;9:e113607. 124. Marsden J. Hyperlipidaemia due to isotretinoin and etretinate: Possible mechanisms and consequences. Br J Dermatol. 1986;114:401–407. 125. Sarkar T, Sarkar S, Patra A. Low-dose isotretinoin therapy and blood lipid abnormality: A case series with sixty patients. J Family Med Prim Care. 2018;7:171–174. 126. Standeven AM, Beard RL, Johnson AT, Boehm MF, Escobar M, Heyman RA et al. Retinoid-induced hypertriglyceridemia in rats is mediated by retinoic acid receptors. Fundam Appl Toxicol. 1996;33:264–271. 127. Melnik B, Bros U, Plewig G. Characterization of apoprotein metabolism and atherogenic lipoproteins during oral isotretinoin treatment. Dermatologica. 1987;175:158–168. 128. Kamagate A, Dong HH. FoxO1 integrates insulin signaling to VLDL production. Cell Cycle. 2008;7:3162–3170. Mechanism of Action of Isotretinoin 129. Kim DH, Zhang T, Ringquist S, Dong HH. Targeting FoxO1 for hypertriglyceridemia. Curr Drug Targets. 2011;12:1245–1255. 130. Pan X, Munshi MK, Iqbal J, Queiroz J, Sirwi AA, Shah S et al. Circadian regulation of intestinal lipid absorption by apolipoprotein AIV involves forkhead transcription factors A2 and O1 and microsomal triglyceride transfer protein. J Biol Chem. 2013;288:20464–20476. 131. Ashur-Fabian O, Har-Zahav A, Shaish A, Wiener Amram H, Margalit O, Weizer- Stern O et al. apoB and apobec1, two genes key to lipid metabolism, are transcriptionally regulated by p53. Cell Cycle. 2010;9:3761–3770. 132. Toossi P, Azizian Z, Yavari H, Fakhim TH, Amini SH, Enamzade R. Serum 25-hydroxy vitamin D levels in patients with acne vulgaris and its association with disease severity. Clin Cases Miner Bone Metab. 2015;12:238–242. 133. Yildizgören MT, Togral AK. Preliminary evidence for vitamin D deficiency in nodulocystic acne. Dermatoendocrinol. 2015;6:e983687. 134. Stewart TJ, Bazergy C. Hormonal and dietary factors in acne vulgaris versus controls. Dermatoendocrinol. 2018;10:e1442160. 135. Lim SK, Ha JM, Lee YH, Lee Y, Seo YJ, Kim CD et al. Comparison of vitamin D levels in patients with and without acne: A case-control study combined with a randomized controlled trial. PLOS ONE. 2016;11:e0161162. 136. El-Hamd MA, El Taieb MA, Ibrahim HM, Aly SS. Vitamin D levels in acne vulgaris patients treated with oral isotretinoin. J Cosmet Dermatol. 2019;18(1):16−20. 137. Ertugrul DT, Karadağ AS, Tutal E, Akin KO. Therapeutic hotline. Does isotretinoin have effect on vitamin D physiology and bone metabolism in acne patients? Dermatol Ther. 2011;24:291–295. 138. Maruyama R, Aoki F, Toyota M, Sasaki Y, Akashi H, Mita H et al. Comparative genome analysis identifies the vitamin D receptor gene as a direct target of p53-mediated transcriptional activation. Cancer Res. 2006;66:4574–4583. 139. Saramäki A, Banwell CM, Campbell MJ, Carlberg C. Regulation of the human p21(waf1/cip1) gene promoter via multiple binding sites for p53 and the vitamin D3 receptor. Nucleic Acids Res. 2006;34:543–554. 140. Zhou BP, Hung MC. Novel targets of Akt, p21(Cipl/WAF1), and MDM2. Semin Oncol. 2002;29:62–70. 141. Milne D, Kampanis P, Nicol S, Dias S, Campbell DG, Fuller-Pace F et al. A novel site of AKT-mediated phosphorylation in the human MDM2 onco-protein. FEBS Lett. 2004;577:270–276. 142. Mayo LD, Donner DB. The PTEN, Mdm2, p53 tumor suppressor-oncoprotein network. Trends Biochem Sci. 2002;27:462–467. 143. Heo SH, Kwak J, Jang KL. All-trans retinoic acid induces p53-depenent apoptosis in human hepatocytes by activating p14 expression via promoter hypomethylation. Cancer Lett. 2015;362:139–148. 144. Fu W, Ma Q, Chen L, Li P, Zhang M, Ramamoorthy S et al. MDM2 acts downstream of p53 as an E3 ligase to promote FOXO ubiquitination and degradation. J Biol Chem. 2009;284:13987–14000. 145. Reichrath J, Reichrath S, Heyne K, Vogt T, Roemer K. Tumor suppression in skin and other tissues via cross-talk between vitamin D- and p53-signaling. Front Physiol. 2014;5:166. 23 146. Heyne K, Heil TC, Bette B, Reichrath J, Roemer K. MDM2 binds and inhibits vitamin D receptor. Cell Cycle. 2015;14:2003–2010. 147. Uchida H, Hasegawa Y, Takahashi H, Makishima M. 1α-Dihydroxyvitamin D3 and retinoic acid increase nuclear vitamin D receptor expression in monocytic THP-1 cells. Anticancer Res. 2016;36:6297–6301. 148. Janik S, Nowak U, Łaszkiewicz A, Satyr A, Majkowski M, Marchwicka A et al. Diverse regulation of vitamin D receptor gene expression by 1,25-dihydroxyvitamin D and ATRA in murine and human blood cells at early stages of their differentiation. Int J Mol Sci. 2017;18:E1323. 149. Lisse TS, Hewison M. Vitamin D: A new player in the world of mTOR signaling. Cell Cycle. 2011;10:1888–1889. 150. Feng Z. p53 regulation of the IGF–1/AKT/mTOR pathways and the endosomal compartment. Cold Spring Harb Perspect Biol. 2010;2:a001057. 151. Werner H, Karnieli E, Rauscher FJ, LeRoith D. Wild-type and mutant p53 differentially regulate transcription of the insulinlike growth factor I receptor gene. Proc Natl Acad Sci USA. 1996;93:8318–8323. 152. Ren W, Yin J, Duan J, Liu G, Tan B, Yang G et al. mTORC1 signaling and IL–17 expression: Defining pathways and possible therapeutic targets. Eur J Immunol. 2016;46:291–299. 153. Agak GW, Qin M, Nobe J, Kim MH, Krutzik SR, Tristan GR et al. Propionibacterium acnes induces an IL-17 response in acne vulgaris that is regulated by vitamin A and vitamin D. J Invest Dermatol. 2014;134:366–373. 154. Mirdamadi Y, Thielitz A, Wiede A, Goihl A, Papakonstantinou E, Hartig R et al. Insulin and insulin-like growth factor-1 can modulate the phosphoinositide-3- kinase/Akt/FoxO1 pathway in SZ95 sebocytes in vitro. Mol Cell Endocrinol. 2015;415:32–44. 155. Mirdamadi Y, Thielitz A, Wiede A, Goihl A, Zouboulis CC, Bommhardt U et al. Effects of isotretinoin on the phosphoinositide-3-kinase/Akt/FoxO1 pathway and molecular functions of SZ95 sebocytes in vitro. J Clin Exp Dermatol Res. 2017;8:3. 156. Burney W, Bosanac SS, Nguyen C, Isseroff RR, Sivamani RK. Short-term exposure of human sebocytes to 13-cisretinoic acid induces acnegenic changes. Br J Dermatol. 2018;179:1201–1202. 157. Yahagi N, Shimano H, Matsuzaka T, Najima Y, Sekiya M, Nakagawa Y et al. p53 Activation in adipocytes of obese mice. J Biol Chem. 2003;278:25395–25400. 158. Parrales A, Iwakuma T. p53 as a regulator of lipid metabolism in cancer. Int J Mol Sci. 2016;17:E2074. 159. Zouboulis CC, Seltmann H, Neitzel H, Orfanos CE. Establishment and characterization of an immortalized human sebaceous gland cell line (SZ95). J Invest Dermatol. 1999;113:1011–1020. 160. Thiboutot D, Jabara S, McAllister JM, Sivarajah A, Gilliland K, Cong Z et al. Human skin is a steroidogenic tissue: Steroidogenic enzymes and cofactors are expressed in epidermis, normal sebocytes, and an immortalized sebocyte cell line (SEB-1). J Invest Dermatol. 2003;120:905–914. 161. McCormick F, Clark R, Harlow E, Tjian R. SV40 T antigen binds specifically to a cellular 53 K protein in vitro. Nature. 1981;292:63–65. 24 162. Dobbelstein M, Roth J. The large T antigen of simian virus 40 binds and inactivates p53 but not p73. J Gen Virol. 1998;79:3079–3083. 163. Wróbel A, Seltmann H, Fimmel S, Müller-Decker K, Tsukada M, Bogdanoff B et al. Differentiation and apoptosis in human immortalized sebocytes. J Invest Dermatol. 2003;120:175–181. 164. Bocchetta M, Eliasz S, De Marco MA, Rudzinski J, Zhang L, Carbone M. The SV40 large T antigen-p53 complexes bind and activate the insulin-like growth factor-I promoter stimulating cell growth. Cancer Res. 2008;68:1022–1029. 165. Melnik BC, John SM, Agamia NF, Chen W, De Vita V, Karadağ AS et al. Isotretinoin’s paradoxical effects in immortalized sebocytes. Br J Dermatol. 2019;180(4):957−958. 166. Plewig G. Follicular keratinization. J Invest Dermatol 1974;62:308–320. 167. Ganceviciene R, Zouboulis CC. Isotretinoin: State of the art treatment for acne vulgaris. J Dtsch Dermatol Ges. 2010;8:S47–S59. 168. Schroeder M, Zouboulis CC. All-trans-retinoic acid and 13-cis-retinoic acid: Pharmacokinetics and biological activity in different cell culture models of human keratinocytes. Horm Metab Res. 2007;39:136–140. 169. Guy R, Ridden C, Barth J, Kealey T. Isolation and maintenance of the human pilosebaceous duct: 13-cis retinoic acid acts directly on the duct in vitro. Br J Dermatol. 1993;128:242–248. 170. Wu NL, Lee TA, Tsai TL, Lin WW. TRAIL-induced keratinocyte differentiation requires caspase activation and p63 expression. J Invest Dermatol. 2011;131:874–883. 171. Zelickson AS, Strauss JS, Mottaz J. Ultrastructural changes in open comedones following treatment of cystic acne with isotretinoin. Am J Dermatopathol. 1985;7:241–244. 172. Elias PM, Fritsch PO, Lampe M, Williams ML, Brown BE, Nemanic M et al. Retinoid effects on epidermal structure, differentiation, and permeability. Lab Invest. 1981;44:531–540. 173. Melnik B, Kinner T, Plewig G. Influence of oral isotretinoin treatment on the composition of comedonal lipids. Implications for comedogenesis in acne vulgaris. Arch Dermatol Res. 1988;280:97–102. 174. Gilbert B, Ahmad K, Roos J, Lehmann C, Chiba T, UlrichRückert S et al. 5-Lipoxygenase is a direct p53 target gene in humans. Biochim Biophys Acta. 2015;1849:1003–1016. 175. Pan SC, Li CY, Kuo CY, Kuo YZ, Fang WY, Huang YH et al. The p53-S100A2 positive feedback loop negatively regulates epithelialization in cutaneous wound healing. Sci Rep. 2018;8:5458. 176. Lovászi M, Mattii M, Eyerich K, Gácsi A, Csányi E, Kovács D et al. Sebum lipids influence macrophage polarization and activation. Br J Dermatol. 2017;177:1671–1682. 177. Su Q, Grabowski M, Weindl G. Recognition of Propionibacterium acnes by human TLR2 heterodimers. Int J Med Microbiol. 2017;307:108–112. 178. Lheure C, Grange PA, Ollagnier G, Morand P, Désiré N, Sayon S et al. TLR-2 recognizes Propionibacterium acnes CAMP factor 1 from highly inflammatory strains. PLOS ONE. 2016;11:e0167237. 179. Kelhälä HL, Aho VTE, Fyhrquist N, Pereira PAB, Kubin ME, Paulin L et al. Isotretinoin and lymecycline treatments modify the skin microbiota in acne. Exp Dermatol. 2018;27:30–36. Retinoids in Dermatology 180. Dispenza MC, Wolpert EB, Gilliland KL, Dai JP, Cong Z, Nelson AM et al. Systemic isotretinoin therapy normalizes exaggerated TLR-2-mediated innate immune responses in acne patients. J Invest Dermatol. 2012;132:2198–2205. 181. Karadağ AS, Ertugrul DT, Bilgili SG, Takci Z, Akin KO, Calka O. Immunoregulatory effects of isotretinoin in patients with acne. Br J Dermatol. 2012;167:433–435. 182. Bergler-Czop B, Brzezińska-Wcisło L. Pro-inflammatory cytokines in patients with various kinds of acne treated with isotretinoin. Postepy Dermatol Alergol. 2014;31:21–28. 183. Papakonstantinou E, Aletras AJ, Glass E, Tsogas P, Dionyssopoulos A, Adjaye J et al. Matrix metalloproteinases of epithelial origin in facial sebum of patients with acne and their regulation by isotretinoin. J Invest Dermatol. 2005;125:673–684. 184. Kistowska M, Meier B, Proust T, Feldmeyer L, Cozzio A, Kuendig T et al. Propionibacterium acnes promotes Th17 and Th17/Th1 responses in acne patients. J Invest Dermatol. 2015;135:110–118. 185. Mucida D, Park Y, Kim G, Turovskaya O, Scott I, Kronenberg M et al. Reciprocal TH17 and regulatory T cell differentiation mediated by retinoic acid. Science. 2007;317:256–260. 186. Sardana K, Verma G. Propionibacterium acnes and the Th1/ Th17 axis, implications in acne pathogenesis and treatment. Indian J Dermatol. 2017;62:392–394. 187. Melnik BC, John SM, Chen W, Plewig G. T helper 17 cell/ regulatory T-cell imbalance in hidradenitis suppurativa/acne inversa: The link to hair follicle dissection, obesity, smoking and autoimmune comorbidities. Br J Dermatol. 2018;179:260–272. 188. Zhang S, Zheng M, Kibe R, Huang Y, Marrero L, Warren S et al. Trp53 negatively regulates autoimmunity via the STAT3-Th17 axis. FASEB J. 2011;25:2387–2398. 189. Kelhälä HL, Fyhrquist N, Palatsi R, Lehtimäki S, Väyrynen JP, Kubin ME et al. Isotretinoin treatment reduces acne lesions but not directly lesional acne inflammation. Exp Dermatol. 2016;25:477–478. 190. Lowe JM, Menendez D, Bushel PR, Shatz M, Kirk EL, Troester MA et al. p53 and NF-κB coregulate proinflammatory gene responses in human macrophages. Cancer Res. 2014;74:2182–2192. 191. Liu G, Park YJ, Tsuruta Y, Lorne E, Abraham E. p53 Attenuates lipopolysaccharide-induced NF-kappaB activation and acute lung injury. J Immunol. 2009;182:5063–5071. 192. Borovaya A, Dombrowski Y, Zwicker S, Olisova O, Ruzicka T, Wolf R et al. Isotretinoin therapy changes the expression of antimicrobial peptides in acne vulgaris. Arch Dermatol Res. 2014;306:689–700. 193. Leyden JJ, James WD. Staphylococcus aureus infection as a complication of isotretinoin therapy. Arch Dermatol. 1987;123:606–608. 194. Spear KL, Muller SA. Nonhealing erosions with granulation tissue in the treatment of acne lesions during isotretinoin therapy. Arch Dermatol. 1984;120:1142. 195. Spring LK, Krakowski AC, Alam M, Bhatia A, Brauer J, Cohen J et al. Isotretinoin and timing of procedural interventions: A systematic review with consensus recommendations. JAMA Dermatol. 2017;153:802–809. 196. Antoniades HN, Galanopoulos T, Neville-Golden J, Kiritsy CP, Lynch SE. p53 expression during normal tissue regeneration in response to acute cutaneous injury in swine. J Clin Invest. 1994;93:2206–2214. Mechanism of Action of Isotretinoin 197. Vollmar B, El-Gibaly AM, Scheuer C, Strik MW, Bruch HP, Menger MD. Acceleration of cutaneous wound healing by transient p53 inhibition. Lab Invest. 2002;82: ­ 1063–1071. 198. Tan M, Heizmann CW, Guan K, Schafer BW, Sun Y. Transcriptional activation of the human S100A2 promoter by wild-type p53. FEBS Lett. 1999;445:265–268. 199. Mueller A, Schäfer BW, Ferrari S, Weibel M, Makek M, Höchli M et al. The calcium-binding protein S100A2 interacts with p53 and modulates its transcriptional activity. J Biol Chem. 2005;280:29186–29193. 25 200. Simmons BJ, Chen L, Hu S. Pyogenic granuloma association with isotretinoin treatment for acne. Australas J Dermatol. 2016;57:e144–e145. 201. Armstrong K, Weinstein M. Pyogenic granulomas during isotretinoin therapy. J Dermatol Case Rep. 2011;5:5–7. 202. Park SH, Lee JH, Tak MS, Lee HJ, Choi HJ. A research of pyogenic granuloma genesis factor with immunohistochemical analysis. J Craniofac Surg. 2017;28:2068–2072. 203. Jeon HH, Yu Q, Lu Y, Spencer E, Lu C, Milovanova T et al. FOXO1 regulates VEGFA expression and promotes angiogenesis in healing wounds. J Pathol. 2018;245:258–264. 5 Mechanism of Action of Acitretin Kaitlyn Lam and Ronald Vender Introduction Acitretin is a systemic, second-generation monoaromatic retinoid and synthetic derivative of vitamin A. It replaced etretinate, its precursor drug, in 1998 due to its more favorable pharmacokinetic profile and wider therapeutic index (1,2). Comparative studies have shown that both drugs have similar efficacy and toxicity (3). Acitretin is more advantageous for therapeutic use because its higher water solubility decreases sequestration in deep fatty tissues, thus giving it a shorter elimination half-life of 50–60 hours compared to 120 days for etretinate (2,4); however, the advantage of acitretin has been limited by evidence that in vivo re-esterification, particularly induced by concomitant ethanol consumption, converts acitretin back into etretinate (5,6). Plasma samples from some patients being treated with acitretin have confirmed the presence of etretinate (7). Potential adverse effects of acitretin are generally dose-dependent and related to hypervitaminosis A, including elevated serum lipids and liver enzymes, mucocutaneous cheilitis, dryness, peeling, pruritis, and rarely hypoglycemia, depression, or hepatotoxicity. Despite the development of many biologic therapies, acitretin remains an important treatment option for patients in whom immunosuppression (e.g., infections, cancer-prone) may be contraindicated (8). standard therapy. Acitretin has shown therapeutic efficacy for the ­following conditions: • Severe psoriasis (5,9–12) • Generalized pustular psoriasis • Palmoplantar pustulosis • Exfoliative erythrodermic psoriasis • Severe psoriasis in HIV (13) • Other keratinization and inflammatory disorders • Darier disease (14,15) • Pityriasis rubra pilaris (16) • Lichen planus (17–19) • Cutaneous lupus erythematosus (20,21) • Lichen sclerosus (22) • Ichthyosis and keratodermas (23,24) • Systemic sclerosis and morphea (25) • Chemoprevention of malignancy • Prevention of premalignant and malignant nonmelanoma skin cancer in solid organ transplant patients (3,26,27) • Other off-label uses (6) Mechanism of Action Special Populations Acitretin is highly teratogenic, which makes inadvisable its use in women who are pregnant or intend to become pregnant. For women of childbearing age, acitretin can only be used with strict contraceptive measures 4 weeks before, during, and for at least 3 years after treatment cessation. Acitretin should be avoided in children due to risk of hypervitaminosis A, and may be associated with increased risks in geriatric patients (≥65 years of age). Alcohol consumption should be avoided during treatment and for 2 months after discontinuing treatment (5). Uses Due to its significant adverse effects, acitretin is reserved for use as second-line therapy to treat severe psoriasis and other keratinizing disorders that are unresponsive or intolerant to Acitretin’s mechanism of action has not been fully elucidated; however, it is known to have antiproliferative, anti-inflammatory, and anti-angiogenic effects (Figure 5.1). A lack of suitable experimental models to study acitretin’s pharmacodynamic properties has limited the investigation of its mechanism of action, and in vitro models using normal human fibroblasts have produced conflicting results (7). Studies using cultures from hyperproliferative conditions, such as psoriasis, have generally concluded that acitretin normalizes epidermopoiesis by inhibiting epidermal cell growth and proliferation and promoting keratinocyte ­differentiation (7,28). Acitretin is thought to modulate its cellular effects by binding to several cellular target receptor sites: 1. Cellular retinoic acid binding proteins (CRABPs): CRABP-I and CRABP-II make up a family of small cytosolic proteins that bind retinoic acid (RA). CRABP-II predominates in human epidermis and increases in expression with stimulation of epidermal 27 28 Retinoids in Dermatology FIGURE 5.1 Mechanism of action of acitretin. Acitretin (A) freely enters the cytosol to bind to CRABP-II, which complexes and transports the drug into the nucleus. Acitretin’s unknown metabolite (a) is thought to bind to RAR/RXRs, which then bind retinoic acid response elements (RARE) in the promoter region of target genes to alter their transcription. Notably, EGF expression is upregulated, causing cell type-specific effects. For example, acitretin promotes EGF-induced cell growth in normal fibroblasts, whereas it contributes to EGF’s cell growth inhibition in squamous carcinoma cell lines. Acitretin also inhibits EGF-induced ODC mRNA expression and activity, which hinders ODC-mediated cell growth and proliferative processes. Downstream effects include reduced epidermal cell growth and proliferation, increased keratinocyte differentiation, decreased VEGF production, decreased Th17 cell differentiation, increased Treg cells, and reduced neutrophil chemotaxis. Acitretin’s influence on these cellular mediators accounts for its anti-psoriatic, keratinolytic, antineoplastic, and anti-inflammatory properties. differentiation in vitro (29–31). It has also been found in high concentrations (800% compared to normal skin) in psoriatic plaques (29). Acitretin binds competitively to CRABP-II, which transports it from the cytosol to the nucleus, thereby increasing its availability to nuclear receptors (29). There has been conflicting evidence regarding acitretin’s effect on CRABP expression. Studies using skin equivalent culture models have reported that acitretin downregulates CRABP-II gene expression (29). In contrast, a study using 0.1% RA cream in vivo resulted in stimulation of CRABP-II gene expression (30). Similarly, treatment of normal skin with acitretin for 4 weeks doubled CRABP activity (32). Presumably, CRABP levels increase in response to the presence of synthetic retinoids in order to facilitate their transport to the nucleus. 2. Nuclear retinoic acid receptors (RARs) and retinoid X receptors (RXRs): Acitretin mediates its action by activating RARs (α, β, γ) and RXRs (α, β, γ) in the nucleus potentially through a metabolite, although the exact mechanism of binding is unknown (33–36). RXR-α/RXR-γ are the predominant retinoid receptors in adult skin which facilitate regulation of gene transcription by RA (37). Activated RARs/RXRs bind retinoid response elements in the promoter region of target genes to alter transcription of over 500 genes (38). For example, acitretin downregulates the transcription of type I and III procollagen, pro-inflammatory, and proliferative genes (39). 3. Epidermal growth factor (EGF): EGF receptors (EGFR) are tyrosine kinases (TK) found in the membranes of the proliferating basal layer of normal skin, where they modulate epidermal cell proliferation (40), keratinocyte differentiation (41), migration, increased cell survival, and resistance to apoptosis (42). They are also found in the non-proliferative suprabasal layer, suggesting that EGFR does not have proliferative action here (7). EGFR and/or its ligands are commonly overexpressed in hyperproliferative disorders and cutaneous cancers, such as squamous cell carcinoma (43). Acitretin appears to interfere with EGF gene expression rather than increasing EGF’s binding affinity to its receptor or the number of EGFRs (44). In normal human fibroblasts, acitretin potentiates EGF-induced cell growth (44). Conversely, EGF inhibits cell growth and proliferation in squamous carcinoma cell lines (45). As a result, acitretin produces an additive inhibitory effect in a concentration-dependent manner, making it an effective therapy for regression of hyperplasia (7,45). A case study in 2008 reported it useful in low doses to treat EGFR inhibitor-induced toxicity to c­ utaneous ­tissues (46). 29 Mechanism of Action of Acitretin 4. Ornithine decarboxylase (ODC): ODC has been implicated in the development of cutaneous carcinogenesis and hyperproliferative skin disorders through EGF signaling (47). EGF stimulates a dose-dependent increase in ODC mRNA and ODC activity as the rate-limiting enzyme in the biosynthesis of polyamines, crucial drivers of cell growth, and proliferation (47). Acitretin may exert a twofold antiproliferative effect of (i) partially inhibiting EGF induction of ODC by decreasing EGF binding or EGFR quantity, as demonstrated in SV40-transformed human keratinocytes, and (ii) inhibiting ODC mRNA expression independent of EGF stimulation (48). 5. Vascular endothelial growth factor (VEGF): VEGF is a key cytokine produced by keratinocytes and peripheral blood mononuclear cells (16,49–52). In the setting of inflammatory disorders like psoriasis, it drives pathogenic angiogenesis, as evidenced by significantly elevated VEGF and its receptors in psoriatic plaques (53). Retinoids are known to inhibit keratinocyte production of VEGF (54). Efficacy of acitretin against VEGF in psoriasis is genotype dependent, with the -460 VEGF polymorphism predicting better clinical responses (54). 6. Cyclic adenosine monophosphate (cAMP)-dependent protein kinases: cAMP has a growth-inhibitory effect which has been shown to be reduced in psoriatic fibroblasts compared to normal cells (55). Acitretin increases the expression and activity of cAMP-dependent protein kinases, in which human psoriatic fibroblasts are deficient, contributing to its anti-growth effects (7,55,56). Acitretin was also observed to promote differentiation of promyelocyte leukemia and myeloblast cell lines through this mechanism and the upregulation of phospholipase-sensitive, calcium-dependent protein ­ kinase and protamine kinase (57). Immunologic Action The pathogenesis of psoriasis primarily involves T-cell mediated pathology, including the induction of T-helper 17 (Th17) cells which secrete inflammatory cytokines that promote development of plaques (58). Acitretin inhibits interleukin 6 (IL-6)-driven induction of Th17 cells, while promoting the differentiation of T-regulatory (Treg) cells by increasing FoxP3 transcription factor expression (59). As a result, acitretin also reduces the stimulation of T-cell mediated cytotoxicity (7). In addition, acitretin exerts anti-inflammatory effects through its inhibition of neutrophil chemotaxis into the epidermis (60,61). Unlike biologics, acitretin does not suppress the immune system, making it a useful therapeutic candidate for those who are unable to tolerate immunosuppression or as a combination therapy with biologics (62). Conclusions Acitretin continues to play a significant role in the management of resistant psoriasis and other keratinizing disorders. Its interaction with various mediators of cell growth and replication account for its antiproliferative, anti-inflammatory, and antiangiogenic effects. Many of the reported cellular effects of acitretin are highly dependent on cell type, microenvironment, and experimental model. For instance, acitretin can stimulate or inhibit collagen synthesis, depending on culture conditions (39). Unfortunately, much of the definitive mechanism of action for acitretin remains to be elucidated. REFERENCES 1. Dunn LK, Gaar LR, Yentzer BA et al. Acitretin in dermatology: A review. J Drugs Dermatol. 2011;10:772–782. 2. Lucek RW, Colburn WA. Clinical pharmacokinetics of the retinoids. Clin Pharmacokinet. 1985;10:38–62. 3. Wolverton SE. Comprehensive Dermatologic Drug Therapy. 3rd ed. Elsevier, Canada; 2012; 1024 p. 4. DiGiovanna JJ, Zech LA, Ruddel ME et al. Etretinate. Persistent serum levels after long-term therapy. Arch Dermatol. 198;125:246–251. 5. Actavis Specialty Pharmaceuticals Co. Soriatane® Product Monograph. Markham, Ontario; 2016. 6. Sarkar R, Chugh S, Garg VK. Acitretin in dermatology. Indian J Dermatol Venereol Leprol. 2013;79:759–771. 7. Pilkington T, Brogden RN. Acitretin. A review of its pharmacology and therapeutic use. Drugs. 1992;43:597–627. 8. Booij MT, Van De Kerkhof PCM. Acitretin revisited in the era of biologics. J Dermatol Treat. 2011;22:86–89. 9. Kragballe K, Jansén CT, Geiger JM et al. A double-blind comparison of acitretin and etretinate in the treatment of severe psoriasis. Results of a Nordic multicentre study. Acta Derm Venereol. 1989;69:35–40. 10. Saurat JH, Geiger JM, Amblard P et al. Randomized doubleblind multicenter study comparing acitretin-PUVA, etretinatePUVA and placebo-PUVA in the treatment of severe psoriasis. Dermatologica. 1988;177:218–224. 11. Tosti A, Ricotti C, Romanelli P et al. Evaluation of the efficacy of acitretin therapy for nail psoriasis. Arch Dermatol. 2009;145:269–271. 12. Sbidian E, Maza A, Montaudié H et al. Efficacy and safety of oral retinoids in different psoriasis subtypes: A systematic literature review. J Eur Acad Dermatol Venereol. 2011;25:28–33. 13. Buccheri L, Katchen BR, Karter AJ, Cohen SR. Acitretin ­therapy is effective for psoriasis associated with human immunodeficiency virus infection. Arch Dermatol. 1997;133:711–715. 14. Christophersen J, Geiger JM, Danneskiold-Samsoe P et al. A double-blind comparison of acitretin and etretinate in the treatment of Darier’s disease. Acta Derm Venereol. 1992;72:150–152. 15. van Dooren-Greebe RJ, van de Kerkhof PC, Happle R. Acitretin monotherapy in Darier’s disease. Br J Dermatol. 1989;121:375–379. 16. Kirby B, Watson R. Pityriasis rubra pilaris treated with acitretin and narrow-band ultraviolet B (Re-TL-01). Br J Dermatol. 2000;142:376–377. 17. Laurberg G, Geiger JM, Hjorth N et al. Treatment of lichen planus with acitretin. A double-blind, placebo-controlled study in 65 patients. J Am Acad Dermatol. 1991;24:434–437. 18. Cribier B, Frances C, Chosidow O. Treatment of lichen planus. An evidence-based medicine analysis of efficacy. Arch Dermatol. 1998;134:1521–1530. 30 19. Jaime TJ, Jaime TJ, Guaraldi B de M et al. Disseminated hypertrophic lichen planus: Relevant response to acitretin. An Bras Dermatol. 2011;86:96–99. 20. Ruzicka T, Sommerburg C, Goerz G et al. Treatment of cutaneous lupus erythematosus with acitretin and hydroxychloroquine. Br J Dermatol. 1992;127:513–518. 21. Ruzicka T, Meurer M, Bieber T. Efficiency of acitretin in the treatment of cutaneous lupus erythematosus. Arch Dermatol. 1988;124:897–902. 22. Bousema MT, Romppanen U, Geiger JM et al. Acitretin in the treatment of severe lichen sclerosus et atrophicus of the vulva: A double-blind, placebo-controlled study. J Am Acad Dermatol. 1994;30:225–231. 23. Lacour M, Mehta-Nikhar B, Atherton DJ, Harper JI. An appraisal of acitretin therapy in children with inherited disorders of keratinization. Br J Dermatol. 1996;134:1023–1029. 24. Happle R, van de Kerkhof PC, Traupe H. Retinoids in disorders of keratinization: Their use in adults. Dermatologica. 1987;175:107–124. 25. Thomas RM, Worswick S, Aleshin M. Retinoic acid for treatment of systemic sclerosis and morphea: A literature review. Dermatol Ther. 2017;30(2): doi: 10.1111/dth.12455. 26. Tan SR, Tope WD. Effect of acitretin on wound healing in organ transplant recipients. Dermatol Surg. 2004;30:667–673. 27. Bavinck JN, Tieben LM, Van der Woude FJ et al. Prevention of skin cancer and reduction of keratotic skin lesions during acitretin therapy in renal transplant recipients: A double-blind, placebo-controlled study. J Clin Oncol. 1995;13:1933–1938. 28. Stadler R, Müller R, Detmar M, Orfanos CE. Retinoids and keratinocyte differentiation in vitro. Dermatologica. 1987;175:45–55. 29. Sanquer S, Eller MS, Gilchrest BA. Retinoids and state of differentiation modulate CRABP II gene expression in a skin equivalent. J Invest Dermatol. 1993;100:148–153. 30. Aström A, Tavakkol A, Pettersson U et al. Molecular cloning of two human cellular retinoic acid-binding proteins (CRABP). Retinoic acid-induced expression of CRABP-II but not CRABP-I in adult human skin in vivo and in skin fibroblasts in vitro. J Biol Chem. 1991;266:17662–17666. 31. Eller MS, Oleksiak MF, McQuaid TJ et al. The molecular cloning and expression of two CRABP cDNAs from human skin. Exp Cell Res. 1992;198:328–336. 32. Siegenthaler G, Saurat J-H. Therapy with a synthetic retinoid—(Ro 10-1670) Etretin—increases the cellular ­ ­retinoic acid-binding protein in nonlesional psoriatic skin. J Invest Dermatol. 1986;87:122–124. 33. Apfel C, Crettaz M, Siegenthaler G, Hunziker W. Synthetic retinoids: Differential binding to retinoic acid receptors1. Retin 10 Years On. 1991;110–120. 34. Benbrook D, Lernhardt E, Pfahl M. A new retinoic acid receptor identified from a hepatocellular carcinoma. Nature. 1988;333:669–672. 35. Petkovich M, Brand NJ, Krust A, Chambon P. A human retinoic acid receptor which belongs to the family of nuclear receptors. Nature. 1987;330:444–450. 36. Arechalde A, Saurat JH. Management of psoriasis: The position of retinoid drugs. BioDrugs Clin Immunother Biopharm Gene Ther. 2000;13:327–333. 37. Fisher GJ, Talwar HS, Xiao JH et al. Immunological identification and functional quantitation of retinoic acid and Retinoids in Dermatology 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. retinoid X receptor proteins in human skin. J Biol Chem. 1994;269:20629–20635. Balmer JE, Blomhoff R. Gene expression regulation by retinoic acid. J Lipid Res. 2002;43:1773–1808. Hein R, Mensing H, Müller PK et al. Effect of vitamin A and its derivatives on collagen production and chemotactic response of fibroblasts. Br J Dermatol. 1984;111:37–44. Kikuchi A, Amagai M, Hayakawa K et al. Association of EGF receptor expression with proliferating cells and of ras p21 expression with differentiating cells in various skin tumours. Br J Dermatol. 1990;123:49–58. Jost M, Kari C, Rodeck U. The EGF receptor - an essential regulator of multiple epidermal functions. Eur J Dermatol. 2000;10:505–510. Rodeck U, Jost M, Kari C et al. EGF-R dependent regulation of keratinocyte survival. J Cell Sci. 1997;110:113–121. Serewko MM, Popa C, Dahler AL et al. Alterations in gene expression and activity during squamous cell carcinoma development. Cancer Res. 2002;62:3759–3765. Harper RA. Specificity in the synergism between retinoic acid and EGF on the growth of adult human skin fibroblasts. Exp Cell Res. 1988;178:254–263. Ponec M, Weerheim A, Kempenaar J, Boonstra J. Proliferation and differentiation of human squamous carcinoma cell lines and normal keratinocytes: Effects of epidermal growth factor, retinoids, and hydrocortisone. In Vitro Cell Dev Biol. 1988;24:764–770. Pomerantz RG, Chirinos RE, Falo LD, Geskin LJ. Acitretin for treatment of EGFR inhibitor-induced cutaneous toxic effects. Arch Dermatol. 2008;144:949–950. Xue GZ, Zheng ZS, Chen RZ et al. Phorbol 12-myristate 13-acetate inhibits epidermal growth factor signalling in human keratinocytes, leading to decreased ornithine decarboxylase activity. Biochem J. 1996;319:641–648. Zheng ZS, Xue GZ, Prystowsky JH. Regulation of the induction of ornithine decarboxylase in keratinocytes by retinoids. Biochem J. 1995;309:159–165. Barnhill RL, Parkinson EK, Ryan TJ. Supernatants from cultured human epidermal keratinocytes stimulate angiogenesis. Br J Dermatol. 1984;110:273–281. Malhotra R, Stenn KS, Fernandez LA, Braverman IM. Angiogenic properties of normal and psoriatic skin associate with epidermis, not dermis. Lab Investig J Tech Methods Pathol. 1989;61:162–165. Thomas KA. Vascular endothelial growth factor, a potent and selective angiogenic agent. J Biol Chem. 1996;271:603–606. Watson CJ, Webb NJ, Bottomley MJ, Brenchley PE. Identification of polymorphisms within the vascular endothelial growth factor (VEGF) gene: Correlation with variation in VEGF protein production. Cytokine. 2000;12:1232–1235. Detmar M, Brown LF, Claffey KP et al. Overexpression of vascular permeability factor/vascular endothelial growth factor and its receptors in psoriasis. J Exp Med. 1994;180:1141–1146. Young HS, Summers AM, Read IR et al. Interaction between genetic control of vascular endothelial growth factor production and retinoid responsiveness in psoriasis. J Invest Dermatol. 2006;126:453–459. Mechanism of Action of Acitretin 55. Brion D, Raynaud F, Plet A et al. Effect of retinoids on cAMPmediated events in human psoriatic fibroblasts. In: Saurat J-H (ed), Retinoids: New Trends in Research and Therapy. Retinoid Symposium, Geneva, September 1984. Basel, Karger, 1985, pp. 189–193. doi: 10.1159/000429401. 56. Raynaud F, Leduc C, Anderson WB, Evain-Brion D. Retinoid treatment of human psoriatic fibroblasts induces an increase in cyclic AMP-dependent protein kinase activity. J Invest Dermatol. 1987;89:105–110. 57. Fontana JA, Reppucci A, Durham JP, Miranda D. Correlation between the induction of leukemic cell differentiation by various retinoids and modulation of protein kinases. Cancer Res. 1986;46:2468–2473. 58. Di Cesare A, Di Meglio P, Nestle FO. The IL-23/Th17 axis in the immunopathogenesis of psoriasis. J Invest Dermatol. 2009;129:1339–1350. 31 59. Mucida D, Park Y, Kim G et al. Reciprocal TH17 and regulatory T cell differentiation mediated by retinoic acid. Science. 2007;317:256–260. 60. Dubertret L, Lebreton C, Touraine R. Inhibition of ­neutrophil migration by etretinate and its main metabolite. Br J Dermatol. 1982;107:681–685. 61. Bauer R, Schütz R, Orfanos CE. Impaired motility and random migration of vital polymorphonuclears in vitro after therapy with oral aromatic retinoid in psoriasis. Int J Dermatol. 1984;23:72–77. 62. Gisondi P, Del Giglio M, Cotena C, Girolomoni G. Combining etanercept and acitretin in the therapy of chronic plaque psoriasis: A 24-week, randomized, controlled, investigator-blinded pilot trial. Br J Dermatol. 2008;158:1345–1349. 6 Mechanism of Action of Bexarotene Catherine M. Ludwig, Claire Wilson, Brandon Roman, and Maria M. Tsoukas Mechanism of Action Retinoids are naturally occurring and synthetically derived compounds related to vitamin A (all-trans retinol). Retinoids interact with intracellular retinoid acid receptors (RARs) and retinoid X receptors (RXRs) to enter the nucleus and modulate gene transcription. There are three subtypes each of the RAR and RXR genes. Through alternative splicing, these nuclear receptors can become incredibly diverse (1). Once retinoids bind, the receptors dimerize and are able to recruit cofactors for transactivation or transrepression of retinoid acid response elements (RAREs) in the DNA to modulate cellular proliferation and differentiation. In vivo, retinoids primarily facilitate heterodimerization of an RAR with an RXR, especially RXR-α, to complete their intranuclear effects (2). The direct transcriptional effect of retinoids is inhibition of cellular proliferation, because many RAREs regulate genes that are pro-apoptotic or cause cell cycle arrest (3). In addition to this classic mechanism leading to nuclear effects on RAREs for cell regulation, retinoids also have extranuclear effects within the cell. Retinoids play a role in mitogen-­activated protein kinase (MAPK) signaling pathways and the Janus kinase/ STAT5 signaling pathway when delivered by retinol binding proteins to the cell membrane (4,5). A portion of RAR-α can be found on lipid rafts of the cell membrane, where it forms complexes with G protein alpha Q (Gαq) in response to retinoic acid. These complexes of RAR-α and Gαq allow for the activation of p38 MAPK pathways. Malignant cells that are resistant to retinoic acid (RA) treatment have been shown to lack these complexes, implying the utility of RA’s activation of the p38 MAPK pathway in apoptosis (6). Retinoids may act as cytokines and activate the cell surface receptors known as “stimulated by retinoic acid 6” (STRA6), leading to the activation of a set of genes known as STATS (6). STATS are expressed independently of the RAR-target genes and are known to regulate the signaling effects of insulin (7). RXRs are able to form heterodimers with other intranuclear receptors besides RAR, including thyroid hormone, vitamin D3, and PPARs (8). The heterodimer of RXR and PPAR-δ/γ subunits acts as a transcriptional regulator for genes that play a role in cellular growth, proliferation, differentiation, and apoptosis. When bound by RXR, the PPAR-δ subunit promotes cellular growth by upregulating genes that modulate lipid and sugar metabolism and attenuate oxidative stress, especially in neurons (Figure 6.1) (9). Gene regulation by RXRs has significant effects in controlling cellular growth, proliferation, differentiation, and apoptosis. When bexarotene is administered with an RAR agonist, it leads to upregulation of transglutaminase I, an enzyme actively involved in the apoptotic cascade (10). RXRs can form both homodimers and heterodimers. Within heterodimers, RXR can serve as either an active or silent partner to its ligand. The active partner form of RXR will allow activation of the ligand receptor by RA leading to its gene transcription capabilities. As a silent partner, the heterodimer of RXR prevents its ligand from responding to RA (11). Through its on/off effects on the metabolism of fatty acids, cholesterol, amino acids, and carbohydrates, RXR has been said to be a “master regulator” of the metabolic effects of retinoids (11). Outside of the nucleus, RXR has been shown to modulate the nuclear export of the orphan receptor TR3, which plays a role in the regulation of apoptosis through its interaction with Bcl-2 (12). This is a distinguishing aspect of RXR-α function in particular, as cells without RXR-α are unable to export TR3 even in the presence of RA (13). Compounds capable of binding to RXRs are known as rexinoids and include 9-cis retinoic acid and bexarotene. The endogenous RXR substrate 9-cis retinoic acid is a panagonist that binds both RARs and RXRs. It is commonly used in the treatment of chronic hand dermatitis, but importantly it has been shown to accomplish this action by primarily activating RARs over RXRs (14). In contrast, bexarotene is a synthetic retinoid (Figure 6.2) that binds to all RXR subtypes with a higher affinity but does not bind to RARs or invoke transactivation of RAREs unless it is present in high concentrations (10). This makes bexarotene unique, because it can be used to selectively target the activation of RXRs over RARs, while most retinoids bind both receptor types. Bexarotene is FDA approved only for the treatment of cutaneous manifestations of cutaneous T-cell lymphoma (CTCL) in patients refractory to at least one previous systemic therapy. Resistance to bexarotene-induced apoptosis during the treatment of CTCL may result from either downregulation or lost expression of the RXR-α and RXR-β subtypes (15). While there are no studies fully describing the mechanism of action, current research suggests that bexarotene may induce apoptosis by assisting in the activation of caspase-3 and the cleavage of poly(ADP-ribose) polymerase (PARP). Bexarotene is also implicated in the downregulation of survivin, an inhibitor of apoptotic proteins (10). Bexarotene’s pro-apoptotic action makes it effective in treating neoplastic disorders. 33 34 Retinoids in Dermatology FIGURE 6.1 When bexarotene binds RXR, RXR becomes an active partner for heterodimerization with PPAR-δ/γ. The active heterodimer is able to enter the nucleus and recruit repressors and activators for gene expression of proteins important for metabolism and specifically peroxisome proliferation. FIGURE 6.2 Chemical structure of bexarotene. Clinical Uses of Oral Bexarotene Bexarotene is most often used in the treatment of CTCL, mycosis fungoides, and Sezary syndrome. There is no cure for this group of lymphomas, but the range of treatments to ameliorate clinical manifestations, induce remission, and postpone progression is wide. Corticosteroids, immunosuppressive drugs, and chemotherapy are also used to treat CTCL. Oral bexarotene is used as mono or adjuvant therapy in the treatment of CTCL and CD-30 positive lymphoproliferative diseases with multifocal lesions. The treatment regimen is initiated with 75 mg/day. The dosage can be increased until improvement is seen, and clinical trials have found that 300 mg/m2 is the dose at which response is maximized but adverse drug effects are still tolerable (16). The most common side effects of oral bexarotene are hypertriglyceridemia and hypothyroidism. As a result, bexarotene is often supplemented with a lipid-lowering agent and levothyroxine to prevent these untoward events. Hyperlipidemia is the most common side effect of bexarotene use and occurs in 45%–79% of CTCL patients during clinical trials (17). Modifiable risk factors predisposing patients to hyperlipidemia as an adverse effect include high-fat diet and lack of exercise. Hypertriglyceridemia is more common than hypercholesterolemia, but both can occur. Patients should be informed of the need for lowering dietary fat intake and increasing exercise 35 Mechanism of Action of Bexarotene prior to initiating bexarotene therapy. It is recommended to start a 2 g omega-3 fatty acid at 2 g BID one week prior to the start of bexarotene therapy even with normal fasting lipid panel. If LDL is increased, atorvastatin 20 or 40 mg/day should be added. If triglycerides are elevated, fenofibrate (145 mg/day) can be used or omega-3 fatty acids increased to three capsules BID (18). Patients prescribed two lipid-lowering agents (statins, fibrates, or omega-3 fatty acids) are usually able to tolerate higher dosing of bexarotene for a longer period. Specifically, when taken with both atorvastatin and fenofibrate, bexarotene is 42% more effective in achieving remission than when it is taken with a single lipid-­lowering agent (18). However, if a statin and fibrate are chosen as lipid-­lowering therapy, creatine kinase levels should be monitored because this drug interaction may cause myopathy and rhabdomyolysis. Central hypothyroidism is the second most common adverse side effect of oral bexarotene (19). Pituitary release of thyroid stimulating hormone was decreased in 29%–74% of patients due to bexarotene inhibition of thyrotropin secretion (17). Clinicians should obtain a baseline thyroid panel before initiating bexarotene therapy and monitor free thyroxine (free T4) levels for patients. Levothyroxine should be used to normalize free T4 when levels are low, as proper management of hypothyroidism in the context of bexarotene use also lessens the extent of hypertriglyceridemia (18). Other less common side effects of oral bexarotene include leukopenia, headaches, asthenia, neutropenia, diarrhea, nausea, pruritus, exfoliation, and transaminase elevation. Bexarotene has neuroprotective functions that have been used in the treatment of cerebral vascular accident and memory impairment disease processes. The buildup of amyloid-β is implicated in neuronal degeneration and as the leading cause of Alzheimer disease. Bexarotene has been found to bind directly to amyloid-β and lessen the concentration of free amyloid-β in neurons (20). Bexarotene’s ability to lower amyloid concentration in the cell has been proposed as preventing the formation of amyloid-β plaques in Alzheimer disease. Bexarotene may also have an ameliorating effect on neurological deficits after subarachnoid hemorrhage. By regulating the PPAR-γ/SIRT6/FoxO3a pathway, bexarotene invokes anti-­ neuroinflammatory processes in damaged neurons (21). Bexarotene’s apoptotic action has made it effective as an adjuvant therapy in treating non-small cell lung carcinoma (NSCLC) and advanced breast carcinoma. Bexarotene is thought to prevent resistance to other chemotherapies and enhance their effect. The addition of oral bexarotene to a chemotherapeutic regimen has helped to prevent or even overcome resistance to paclitaxel and gemcitabine resistance in NSCLC cell lines. When administered with weekly paclitaxel and monthly carboplatin, bexarotene has been shown to treat NSCLC (22). The addition of bexarotene to a cytotoxic treatment regimen has also been helpful in preventing and overcoming acquired drug resistance in advanced breast carcinoma regimens. Cells remained more chemosensitive when treated with bexarotene combined regimen as compared to the cells treated with paclitaxel, doxorubicin, and cisplatin only (23). Clinical Uses of Topical Bexarotene Bexarotene gel is also effective in treating CTCL lesions after other standard therapies fail (24). Topical corticosteroids are also TABLE 6.1 Clinical Applications of Bexarotene Clinical Applications of Bexarotene Cutaneous T-cell lymphoma (CTCL) CTCL lesions Side Effects Most common: Hypertriglyceridemia, hyperlipidemia, central hypothyroidism Least common: Leukopenia, headaches, asthenia, neutropenia, diarrhea, nausea, pruritus, exfoliation, elevation of liver enzymes Non-small cell lung carcinoma (NSCLC) Advanced breast carcinoma Chronic-severe hand dermatitis Mild to moderate plaque psoriasis Alopecia areata Strokes and memory impairment processes useful in treating CTCL lesions, but due to a limited duration of effective disease control, they are sometimes discontinued in favor of immunosuppression and chemotherapy. Bexarotene is available as a 1% formulation for topical use, which is effective in treating CTCL lesions when topical steroids are ineffective. It can be applied up to four times a day as tolerated, but BID is the most common dosage. Initially, it is recommended to apply bexarotene every other day to the affected areas for 1 week, and then increase by one application per day per week to a maximum of four times a day. With bexarotene gel use, the most common side effects are irritant dermatitis and erythema that increase with increased frequency of use (25). Topical bexarotene is also useful for chronic-severe hand dermatitis. Bexarotene gel has been shown to be effective in clearing eczematous lesions from at least 50% of the hand surface area in 79% of patients with atopic dermatitis (26). In patients with mild to moderate plaque psoriasis, bexarotene may reduce the hyperproliferation of keratinocytes that are key in forming the thickened epidermis of psoriatic plaques (27). Bexarotene is also able to enhance the effect of narrowband UVB phototherapy on psoriatic plaques; bexarotene gel used together with phototherapy is significantly more effective for treatment of moderate-severe psoriasis vulgaris than narrowband phototherapy alone (28). Bexarotene has also been effective in treating alopecia areata, due to its pro-apoptotic effect on T cells (29). Clinical applications of bexarotene are summarized in Table 6.1. Conclusions In addition to the classic retinoid mechanism of inducing RAR dimerization to activate RAREs in the DNA, bexarotene is able to induce a myriad of regulatory events due to its preference for the versatile RXR. Bexarotene is uniquely able to induce protective functions in the cell and has novel implications in the treatment of stroke and Alzheimer disease due to these mechanisms. 36 REFERENCES 1. Germain P, Chambon P, Eichele G et al. International Union of Pharmacology. LX. Retinoic acid receptors. Pharmacol Rev. 2006;58:712–725. 2. Genetic evidence that the retinoid signal is transduced by heterodimeric RXR/RAR functional units during mouse development [Internet]. [cited 2019 Mar 26]. Available from: http:// dev.biologists.org/content/124/2/313.long 3. Donato LJ, Noy N. Suppression of mammary carcinoma growth by retinoic acid: Proapoptotic genes are targets for retinoic acid receptor and cellular retinoic acid-binding protein II signaling. Cancer Res. 2005;65:8193–8199. 4. Alsayed Y, Uddin S, Mahmud N et al. Activation of Rac1 and the p38 mitogen-activated protein kinase pathway in response to all-trans-retinoic acid. J Biol Chem. 2001;276:4012–4019. 5. Berry DC, O’Byrne SM, Vreeland AC et al. Cross talk between signaling and vitamin a transport by the retinol-binding protein receptor STRA6. Mol Cell Biol. 2012;32:3164–3175. 6. Nuclear and extranuclear effects of vitamin A. Canadian Journal of Physiology and Pharmacology [Internet]. [cited 2019 Apr 2]. Available from: https://www.nrcresearchpress. com/doi/10.1139/cjpp-2014-0522#.XKPO3OtKiRs 7. Muenzner M, Tuvia N, Deutschmann C et al. Retinol-binding protein 4 and its membrane receptor STRA6 control adipogenesis by regulating cellular retinoid homeostasis and retinoic acid receptor α activity. Mol Cell Biol. 2013;33:4068–4082. 8. Larange A, Cheroutre H. Retinoic acid and retinoic acid receptors as pleiotropic modulators of the immune system. Ann Rev Immunol. 2016;34:369–394. 9. Palomer X, Capdevila-Busquets E, Botteri G et al. PPARβ/δ attenuates palmitate-induced endoplasmic reticulum stress and induces autophagic markers in human cardiac cells. Int J Cardiol. 2014;174:110–118. 10. Qu L, Tang X. Bexarotene: A promising anticancer agent. Cancer Chemother Pharmacol. 2010;65:201–205. 11. Bushue N, Wan Y-JY. Retinoid pathway and cancer therapeutics. Adv Drug Deliv Rev. 2010;62:1285–1298. 12. Cao X, Liu W, Lin F et al. Retinoid X receptor regulates Nur77/TR3-dependent apoptosis [corrected] by modulating its nuclear export and mitochondrial targeting. Mol Cell Biol. 2004;24:9705–9725. 13. Lin X-F. RXR acts as a carrier for TR3 nuclear export in a 9-cis retinoic acid-dependent manner in gastric cancer cells. J Cell Sci. 2004;117:5609–5621. 14. Dawson MI, Xia Z. The retinoid X receptors and their ligands. Biochim Biophys Acta. 2012;1821:21–56. 15. Lin JH, Kim EJ, Bansal A et al. Clinical and in vitro resistance to bexarotene in adult T-cell leukemia: Loss of RXRalpha receptor. Blood. 2008;112:2484–2488. 16. Duvic M, Martin AG, Kim Y et al. Phase 2 and 3 clinical trial of oral bexarotene (targretin capsules) for the treatment of refractory or persistent early-stage cutaneous T-cell lymphoma. Arch Dermatol. 2001;137:581–593. Retinoids in Dermatology 17. Schadt CR. Topical and oral bexarotene. Dermatol Therap. 2013;26:400–403. 18. Talpur R, Ward S, Apisarnthanarax N et al. Optimizing bexarotene therapy for cutaneous T-cell lymphoma. J Am Acad Dermatol. 2002;47:672–684. 19. Bagherani N, Smoller BR. An overview of cutaneous T cell lymphomas. F1000Res [Internet]. 2016 Jul 28;5. pii: F1000 [cited 2019 Apr 3]. Available from: https://www.ncbi.nlm.nih. gov/pmc/articles/PMC4965697/ 20. Mirza Z, Beg MA. Possible Molecular Interactions of Bexarotene—A Retinoid Drug and Alzheimer’s Aβ Peptide: A Docking Study [Internet]. Current Alzheimer Research. 2017 [cited 2019 Apr 3]. Available from: http://www.eurekaselect.com/147342/article 21. Zuo Y, Huang L, Enkhjargal B et al. Activation of retinoid X receptor by bexarotene attenuates neuroinflammation via PPARγ/SIRT6/FoxO3a pathway after subarachnoid hemorrhage in rats. J Neuroinflamm. 2019;16:47. 22. Dragnev KH, Whyman JD, Hahn CK et al. A phase I/II study of bexarotene with carboplatin and weekly paclitaxel for the treatment of patients with advanced non-small cell lung cancer. J Thorac Dis. 2018;10:5531–5537. 23. Yen W-C, Lamph WW. The selective retinoid X receptor agonist bexarotene (LGD1069, Targretin) prevents and overcomes multidrug resistance in advanced breast carcinoma. Mol Cancer Ther. 2005;4:824–834. 24. Beckenbach L, Baron JM, Merk HF et al. Retinoid treatment of skin diseases Retinoids in dermatology. Europ J Dermatol. 2015;25:384–391. 25. Breneman D, Duvic M, Kuzel T et al. Phase 1 and 2 trial of Bexarotene gel for skin-directed treatment of patients with cutaneous T-cell lymphoma. Arch Dermatol. 2002;138:325–332. 26. Hanifin JM, Stevens V, Sheth P et al. Novel treatment of chronic severe hand dermatitis with bexarotene gel. Br J Dermatol. 2004;150:545–553. 27. Smit JV, de Jong EMGJ, van Hooijdonk CAEM, Otero ME, Boezeman JBM, van de Kerkhof PCM. Systemic treatment of psoriatic patients with bexarotene decreases epidermal proliferation and parameters for inflammation, and improves differentiation in lesional skin. J Am Acad Dermatol. 2004;51:257–264. 28. Magliocco MA, Pandya K, Dombrovskiy V et al. A randomized, double-blind, vehicle-controlled, bilateral comparison trial of bexarotene gel 1% versus vehicle gel in combination with narrowband UVB phototherapy for moderate to severe psoriasis vulgaris. J Am Acad Dermatol. 2006;54:115–118. 29. Rajiv M, Singh N. Bexarotene gel: A new topical therapy for alopecia areata. Int J Trichol. 2010;2:66–67. 7 Mechanism of Action of Alitretinoin Ömer Faruk Elmas and Necmettin Akdeniz Introduction Mechanism of Action of Alitretinoin Alitretinoin, also known as 9-cis retinoic acid, was initially approved by the United States Food and Drug Administration (FDA) in 1999 for treatment of localized Kaposi sarcoma in the form of 0.1% topical gel, which represents the iso­ merization of tretinoin (Figure 7.1) (1). Alitretinoin has subsequently been used in many dermatologic diseases thought to be responsive to retinoids. Recalcitrant hand dermatitis is the first FDA-approved (2009) indication of systemic (oral) ­a litretinoin (2). Retinoids are vitamin A derivatives regulating cell differentiation, proliferation, and apoptosis. Retinoic acid and 9-cis retinoic acid are the active metabolites synthetized from retinol. The identification of the nuclear retinoic acid receptors resulted in remarkable progress in the exploration of the mechanism of action of retinoids (3). There are two main types of retinoid nuclear receptors (RNRs): the retinoic acid receptors (RAR) and retinoid X receptors (RXRs). The natural ligands for RAR and RXR are retinoic acid and 9-cis retinoic acid, respectively. Isotretinoin, acitretin, tazarotene, and adapalene are synthetic ligands of the RAR. Bexarotene is the synthetic ligand of the RXR. Alitretinoin is known to be the first panagonist synthetic ligand (3). Alitretinoin is a pan-retinoic acid agonist. It has the ability to bind and activate all subclasses of intracellular retinoid RAR and RXR receptors (RAR-α, RAR-β, RAR-γ, RXR-α, RXR-β, and RXR-γ). These receptors act as transcription factors to regulate the expression of genes that control cellular differentiation and proliferation. Several pharmacodynamic processes take place, and the expressed proteins cause the clinical and therapeutic effects of alitretinoin (4). The mechanism of action of alitretinoin can be considered under two main subheadings (1,4): • Antiproliferative-apoptotic effect • Immunomodulatory-anti-inflammatory effect The apoptotic and antiproliferative effect of alitretinoin has been used in the treatment of localized Kaposi sarcoma. While apoptotic activity is associated with RAR receptors, the anti­ proliferative effect is mediated by RXR receptors. After binding to these receptors, alitretinoin downregulates IL-6 receptors, lessening the expression of a viral encoded oncogene, which increases in Kaposi sarcoma lesions (5,6). Suppression of chemokine receptor expression and inhibition of chemotaxis represent the main mechanism of alitretinoin’s anti-inflammatory and immunomodulatory effects. Alitretinoin also reduces the number of macrophages and dendritic cells that are the main sources of the inflammatory cytokines, primarily TNF-α. IL-4, IL-1β, and IL12p40 are the other cytokines whose levels are reduced by alitretinoin. Indirect inhibition of nitric oxide production can be expressed as another anti-inflammatory effect of alitretinoin (1,7,8). Possible mechanism of action or alitretinoin in various skin diseases are summarized in Table 7.1. Topical Use FIGURE 7.1 Chemical structure of alitretinoin (9-cis retinoic acid) ((2E,4E,6Z,8E)-3,7-dimethyl-9-(2,6,6-trimethyl-1-cyclohexen-1-yl)2,4,6,8-nonatetraenoic acid). (Alitretinoin. Accession Number: DB00523 (APRD00017). DrugBank Release Version 5.1.3. 2019.) Alitretinoin has also been used in a 0.1% topical gel form for the treatment of cutaneous Kaposi sarcoma. Experimental ­studies have shown that alitretinoin inhibits neo-angiogenesis, proliferation of malignant Kaposi sarcoma cells, and keratinocyte ­cohesion (6,9). Pyogenic granuloma, also known as lobular capillary hemangioma, is a commonly encountered entity in dermatology practice characterized by proliferation of mature capillary structures. The topical gel formulation of alitretinoin may also be used in pyogenic granulomas in the context of similar histologic features 37 38 Retinoids in Dermatology TABLE 7.1 The Mechanism of Action of Alitretinoin in Various Skin Diseases Disease Possible Mechanism of Action Topical use Localized Kaposi sarcoma Pyogenic granuloma Photoaging Systemic use Chronic hand dermatitis Psoriasis Pityriasis rubra pilaris Atopic dermatitis Lichen planus Lichen simplex chronicus Darier’s disease Cutaneous T-cell lymphoma Keratosis-ichthyosisdeafness (KID) syndrome Inhibition of neo-angiogenesis, proliferation of the malignant Kaposi sarcoma cells and keratinocyte cohesion Antiproliferative effect and inhibition of neo-angiogenesis as in Kaposi sarcoma Stimulation of TGF-β releasing as the main mediator of collagen synthesis Activation of RXR receptors, stimulates Th2 immune functions Immunomodulatory properties of alitretinoin on keratinocytes, T cells, dendritic cells, fibroblasts, and mast cells. Suppression of inflammatory activity with chemotaxis inhibition and thus reduction in inflammation and psoriatic lesions Anti-inflammatory and immunomodulatory properties directed against keratinocytes and white blood cells Suppression of cytokine release at cellular level and inhibition of chemotaxis Immunomodulatory effects on basal keratinocytes and T cells, regulatory role on cell proliferation Immunomodulatory effect on the inflammatory cytokines associated with itching Regulatory effect for cell proliferation, differentiation, keratinization, and immunomodulation Antiproliferative, pro-apoptotic, and immunomodulatory effects Stimulation of connexin expression with Kaposi sarcoma. Topical alitretinoin 0.1% gel has been used successfully in two patients with pyogenic granuloma (10). The mechanism of action seems to be associated with the antiproliferative effect and inhibition of neo-angiogenesis, as it is in Kaposi sarcoma (1,10). Another condition where alitretinoin is found to be effective is photoaging. A 0.1% topical gel formulation of alitretinoin has been shown to be highly effective and safe in treating photo­ damaged skin and actinic keratosis, as well as seborrheic keratosis (11). It has been postulated that alitretinoin stimulates TGF-β releasing which is the main mediator of collagen synthesis, thus allowing photodamaged skin to be repaired (1). When reviewing the literature, it seems that there are no additional data about the use of alitretinoin in photoaging. Lack of such studies for this indication may be due to its high price. stimulate Th2 immune functions. This could alter the pathogenesis of the disease (12,13). Palmoplantar pustular psoriasis is another disease in which alitretinoin has been successfully used. The effect of alitretinoin in psoriasis is mainly related to its immunomodulatory properties on keratinocytes, T cells, dendritic cells, fibroblasts, and mast cells. Alitretinoin suppresses inflammatory activity, providing chemotaxis inhibition with reduction of inflammation in psoriatic lesions (14–19). One patient with recalcitrant pityriasis rubra pilaris responded well to 30 mg daily oral alitretinoin. The mechanism of action is related to the anti-inflammatory and immunomodulatory properties of the drug on keratinocytes and white blood cells, as it is in psoriasis (1,20). Atopic dermatitis develops mainly due to the pathogenetic Type I immediate and Type IV cell-mediated delayed hypersensitivity reactions. In a study involving six patients with atopic dermatitis, patients responded well to a 12-week oral alitretinoin regimen of daily 30 mg (21). The mechanism of action in atopic dermatitis can be explained by suppression of cytokine release at the cellular level and the inhibition of chemotaxis. Lichen planus is a T-cell-mediated autoimmune skin disease. There are two patients with lichen planus known to be successfully managed with oral alitretinoin (22). This may be attributed to its immunomodulatory effects on basal keratinocytes and T cells. The regulatory effect on cell proliferation is another aspect of the mechanism of action in lichen planus (1,22). The agent has been significantly effective in treating two patients with lichen planus and marked nail involvement (23). A patient with lichen simplex chronicus that had been resistant to conventional treatment responded to oral alitretinoin (24). The mechanism of action of alitretinoin may be due to its immunomodulatory effect on the inflammatory cytokines which are associated with itching (1,24). Darier disease is an autosomal dominant inherited dermatosis characterized by warty, dirty gray-colored papular lesions distributed in seborrheic areas. There are several studies reporting that alitretinoin is an effective option in treating patients with Darier disease (25–27). Alitretinoin may be considered as a regulator for cell proliferation, differentiation, keratinization, and immunomodulation (1). Bexarotene has also been approved by the FDA for the treatment of cutaneous T-cell lymphoma both topically and systemically. It has been postulated that it has apoptotic effects on malignant cells via RXR receptors. Two patients with cutaneous T-cell lymphoma have had good results with alitretinoin (28). Here, the mechanism of action of alitretinoin may be related to its antiproliferative, proapoptotic, and immunomodulatory effects (1,28). Keratosis-ichthyosis-deafness (KID) syndrome is a hereditary disorder associated with Connexin-26 gene mutation, which is a gap junctional protein (29) responding to alitretinoin with lessening of the skin lesions (30,31). The mechanism of action of alitretinoin is attributed to its ability for stimulating Connexin expression (1). Systemic Use Conclusions The mechanism of action of oral alitretinoin in chronic hand dermatitis is unclear, but the agent may activate RXR receptors and Alitretinoin is a unique synthetic retinoid capable of binding to all known retinoid receptors. Localized Kaposi sarcoma and Mechanism of Action of Alitretinoin recalcitrant hand dermatitis are the main indications for alitretinoin. The immunomodulatory effect on the different pathways of inflammation and the regulatory effect for cell proliferation, differentiation, and keratinization seem to be the key mechanisms of action. REFERENCES 1. Bubna AK. Alitretinoin in dermatology—an update. Indian J Dermatol Venereol Leprol. 2015;60:520. 2. Ruzicka T, Lynde CW, Jemec GBE et al. Efficacy and safety of oral alitretinoin (9-cis retinoic acid) in patients with severe chronic hand eczema refractory to topical corticosteroids: Results of a randomized, double-blind, placebo-controlled, multicentre trial. Br J Dermatol. 2008;158:808–817. 3. Berbis P. Retinoids: Mechanisms of action. Ann Dermatol Venereol. 2010;137:97–103. 4. Sami N, Harper JC. Topical retinoids. In: Wolverton SE, editor. Comprehensive Dermatologic Drug Therapy. 2nd ed. Philadelphia: Elsevier Saunders; 2007, pp. 625–641. 5. Duvic M, Friedman-Kien A, Looney D et al. Topical treatment of cutaneous lesions of acquired immune deficiency syndrome related Kaposi’s sarcoma using alitretinoin gel. Arch Dermatol. 2000;136:1461–1469. 6. Bodsworth N, Bloch M, Bower M et al. International Panretin gel study group. Phase III vehicle controlled, multi-centred study of topical alitretinoin gel 0.1% in cutaneous AIDS related Kaposi’s sarcoma. Am J Clin Dermatol. 2001;2:77–87. 7. Cheng C, Michaels J, Scheinfeld N. Alitretinoin: A comprehensive review. Expert Opin Investig Drugs. 2008;17:437–443. 8. Molin S, Ruzicka T. Alitretinoin: A new treatment option for chronic refractory hand eczema. Hautarzt. 2008;59:703–709. 9. Schwartz RA, Micali G, Nasca RM, Scuderi L. Kaposi sarcoma: A continuing conundrum. J Am Acad Dermatol. 2008;59:179–206. 10. Maloney DM, Schmidt JD, Duvic M. Alitretinoin gel to treat pyogenic granuloma. J Am Acad Dermatol. 2002;47:969–970. 11. Baumann L, Vujevich J, Halem M et al. Open label pilot study of alitretinoin gel 0.1% in the treatment of photoaging. Cutis. 2005;76:69–73. 12. Stephenson CB, Rasooly R, Jiang X et al. Vitamin A enhances in vitro Th2 development via retinoid X receptor pathway. J Immunol. 2002;168:4495–4503. 13. Ruzicka T, Larsen FG, Galewicz D et al. Oral alitretinoin (9-cis retinoic acid) therapy for chronic hand dermatitis in patients refractory to standard therapy. Arch Dermatol. 2004;140:1453–1459. 14. Irla N, Navarini AA, Yawalkar N. Alitretinoin abrogates innate inflammation in palmoplantar pustular psoriasis. Br J Dermatol. 2012;167:1170–1174. 15. Sorenson S, Solvsten H, Politi Y, Kragballe K. Effects of vitamin D3 on keratinocyte proliferation and differentiation in vitro: Modulation by ligands for retinoic acid and retinoid X receptors. Skin Pharmacol. 1997;10:144–152. 16. Xiao R, Kanekura T, Yoshida N et al. 9-cis retinoic acid exhibits anti fibrotic activity via induction of cyclooxygenase-2 expression and prostaglandin E2 production in scleroderma fibroblasts. Clin Exp Dermatol. 2008;33:484–490. 39 17. Ko J, Yun CY, Lee JS, KiM DH, Yuk JE, Kim IS. Differential regulation of CC chemokine receptors by 9-cis retinoic acid in human mast cell line, HMC-1. Life Sci. 2006;79:1293–1300. 18. Zapata-Gonzalez F, Rueda F, Petriz J et al. 9-cis retinoic acid (9cRA), a retinoid X receptor (RXR) ligand, exerts immunosuppressive effects on dendritic cells by RXR-dependent activation: Inhibition of peroxisome proliferator-activated receptor gamma blocks some of the 9cRA activities and precludes them to mature phenotype development. J Immunol. 2007;178:6130–6139. 19. Dawson HD, Collins G, Pyle R et al. Direct and indirect effects of retinoic acid on human Th2 cytokine and chemokine expression by human T lymphocytes. BMC Immunol. 2006;7:27. 20. Molin S, Ruzicka T. Treatment of refractory pityriasis rubra pilaris with oral alitretinoin: Case report. Br J Dermatol. 2010;163:221–222. 21. Grahovac M, Molin S, Prinz JC, Ruzicka T, Wollenberg A. Treatment of atopic eczema with oral alitretinoin. Br J Dermatol. 2010;162:217–218. 22. Molin S, Ruzicka T. Oral alitretinoin in lichen planus: Two case reports. Acta Derm Venereol. 2010;90:523–524. 23. Alsenaid A, Eder I, Ruzicka T, Braun-Falco M, Wolf R. Successful treatment of nail lichen planus with alitretinoin: Report of 2 cases and review of the literature. Dermatology. 2014;229:293–296. 24. D’Emre AM, Milanesi N, Agnoletti AF, Maio V, Massi D. Efficacy of treatment with oral alitretinoin in patient suffering from lichen simplex chronicus and severe atopic dermatitis of the hands. Dermatol Ther. 2014;27:21–23. 25. Zamiri M, Munro CS. Successful treatment with oral ­alitretinoin in women of child bearing potential with Darier’s ­disease. Br J Dermatol. 2013;169:709–710. 26. Barnstedt SE. Successful treatment of Darier disease with oral alitretinoin. Hautarzt. 2012;63:139–141. 27. Anuset D, Goutorbe C, Bernard P, Reguiai Z. Efficacy of oral alitretinoin for the treatment of Darier disease: A case report. J Am Acad Dermatol. 2014;71:46–48. 28. Molin S, Ruzicka T. Possible benefit of oral alitretinoin in T-lymphoproliferative diseases: A report of two patients with palmoplantar hyperkeratotic rhagadiform skin changes and mycosis fungoides or Sezary syndrome. Br J Dermatol. 2009;169:1420–1421. 29. Mazereeuw-Hautier J, Bitoun E, Chevrant-Breton J. Keratitisichthyosis-deafness syndrome: Disease expression and ­spectrum of connexin 26 (GJB2) mutations in 14 patients. Br J Dermatol. 2007;156:1015–1019. 30. Werchau S, Toberer F, Enk A, Helmbold P. Keratitisichthyosis-deafness syndrome: Response to alitretinoin and review of literature. Arch Dermatol. 2011;147:993–995. 31. Prasad SC, Bygum A. Successful treatment with alitretinoin of dissecting cellulitis of the scalp in keratitis-ichthyosis-deafness syndrome. Acta Derm Venereol. 2013;93:473–474. 32. Alitretinoin. Accession Number: DB00523 (APRD00017). DrugBank Release Version 5.1.3. 2019. 8 Effects of Retinoids at the Cellular Level (Differentiation, Apoptosis, Autophagy, Cell Cycle Regulation, and Senescence) Jelena Popovic Introduction On the cellular level, vitamin A and its major active metabolite, all-trans-retinoic acid (RA), which acts as a morphogen (1), enable transcriptional regulation of RA-responsive genes through a wellknown RA signaling pathway (2). This evolutionary-conserved signaling pathway maintains homeostasis through regulation of genes that are responsible for control of a variety of cellular processes, including cell proliferation, cell differentiation, cell cycle, autophagy, and senescence (3,4). The best-known role of RA is growth inhibition exerted by induction of these processes alone or in combination; however, RA occasionally does not inhibit cellular growth but instead enhances proliferation and survival. The entry of RA into the nucleus, where binding to receptors occurs, depends upon the retinoid binding proteins. These cytosolic proteins include cellular retinol-binding proteins (RBP): RBP1, RBP2, cellular retinoic acid-binding protein 1 and 2 (CRABP1, CRABP2), and fatty acid-binding protein 5 (FABP5), which are responsible for cellular transport of poorly soluble retinoids during uptake, metabolism, and function (5). The effects of RA on cells are mediated by RA responsive receptors (RAR): retinoic acid receptor alpha (RARA or RARα), beta (RARB or RAR-β), and gamma (RARG or RAR-γ) and the peroxisome proliferator-activated receptor beta and delta (PPARB or PPAR-β and PPARD or PPAR-δ) which belong to the nuclear receptor superfamily (6). They function as RA liganddependent transcription factors which form heterodimers with the retinoid X receptors (RXRs), and mediate transcription by binding to DNA. Heterodimers RAR/RXR bind to cis acting RA response elements (RAREs), while PPAR/RXR heterodimers bind to peroxisome proliferator response element (PPRE) (Figure 8.1) (7–9). The precise control of RARs is necessary for the correct balance between self-renewal and differentiation of tissue stem cells. The loss, accumulation, mutations, or aberrant modifications of RARs results in oncogenic transformation with disturbance in differentiation and uncontrolled proliferation of cells (10). The targets of RA and RARs/PPAR-β/δ include many structural genes, oncogenes, transcription factors, and cytokines. When RA binds to RARs, a conformational change is induced, and the receptors dissociate themselves from co-repressors to bind with co-activators (11). Similarly, the binding of RXR to RA as its ligand further induces the RAR/RXR-mediated transcription of the retinoid-regulated genes (12,13) (Figure 8.1). RA signaling is a tremendously complex and highly regulated process, being responsible for many aspects of cellular function. This chapter summarizes the essential cellular processes dependent on this signaling pathway. Retinoic Acid Signaling and Cell Differentiation Differentiation is the process whereby a single stem cell changes its characteristics to become a more specialized cell type. This occurs during the embryonic development of a multicellular organism and results in development of a complex system of tissues and cell types enabling the proper function of the organism. This process continues into adulthood, when adult stem cells contribute to tissue repair and the cellular renewal of tissues and organs. Differentiation is a highly controlled molecular process with numerous molecular and cellular events. One of the major signaling pathways responsible for orchestrating these processes leads to differentiation through RA signaling (8,14). One of the most important roles of RA is its role in central nervous system development (15). During neural differentiation, RA downregulates pluripotency factors and activates proneural and neurogenic genes (15,16). Studies in cultured embryonic stem cells (ESC) (17,18) and embryonal carcinoma stem cells (19,20) provide insight into the roles of retinoids in neural cell differentiation. One of the best characterized model systems for human neural differentiation in vitro is the NT2/D1 cell line (Figure 8.2a), derived from testicular teratocarcinoma (21). This embryonal carcinoma cell line resembles embryonic stem cells in morphology, antigen expression patterns, biochemistry, differentiation potential, and gene regulation (21). In the presence of RA, NT2/D1 cells differentiate into mature neurons (Figures 8.2b and 8.3), providing a good in vitro model for studying human genes that promote and regulate neural differentiation (21). Terminally differentiated NT2/D1 neurons exhibit properties of post-mitotic polarized cells that express neurofilaments; generate action potentials and calcium spikes; express, secrete and respond to neurotransmitters; and form functional synapses (22–24). Activation of RAR and PPAR by RA is crucial for induction of neuronal differentiation, and various target genes have been reported to be involved in this process (25,26). RA, through its effectors, directly regulates expression of subset of homeotic genes (Hox) Hoxa-1, Hoxb-2, and Wnt-1 (27). These master control genes specify the body plan and regulate the development 41 42 Retinoids in Dermatology FIGURE 8.1 Schematic representation of RA binding to retinoic acid receptors (RARs). RA is transported to the nucleus by cellular retinoic acid-binding proteins (CRABP) or fatty acid-binding protein (FABP5), while binding to cytochrome P450 26A1 (CYP26) leads to its degradation. Once successfully in the nucleus, RAs induce formation of heterodimers RAR/RXR which bind to cis-acting RA response elements (RAREs), and/or heterodimers PPAR/RXR which bind to peroxisome proliferator response element (PPRE), displacing co-repressors and recruiting co-activators of the transcription of target genes that are involved in regulation of various crucial cellular processes. FIGURE 8.2 Neural differentiation of NT2/D1 cells upon treatment with RA. (a) Undifferentiated NT2/D1 cells. (b) Differentiated NT2/D1 cells develop into neurons in response to treatment with 10 µM RA for 4 weeks. Neurons can be mechanically detached from the still non-differentiated NT2/D1 cells and seeded on Matrigel® (Thermo Fisher Scientific)-coated surface in the presence of mitotic inhibitors. Neurons prepared through this approach have the tendency to aggregate and form synapses (arrows) in vitro. (a) (b) (c) FIGURE 8.3 Immunocytochemical detection of microtubule-associated protein 2 (MAP2) (red), marker of mature neurons in terminally differentiated NT2/D1 neurons. Cell nuclei were counterstained with DAPI (blue). Scale bar 100 µm. Effects of Retinoids at the Cellular Level (Differentiation, Apoptosis, Autophagy, Cell Cycle Regulation, and Senescence) and morphogenesis of higher organisms. In addition, RA also indirectly regulates achaete-scute family bHLH transcription factor 1 gene (ASCL1), Neurogenin 1 (NEUROG1), neuronal differentiation 1 (NeuroD1), N-cadherin/cadherin 2 (CDH2), and pre-B-cell leukemia transcription factors or PBX homeobox genes (Pbx) (7). Genes activated by RA are members of different signaling pathways including TGF-β pathway (genes left-right determination factor 2 [LEFTY2], BMP and activin membrane bound inhibitor [BAMBI], Follistatin [FST]), homeodomain pathway (genes HoxD1, MEIS1, MEIS2), gastrulation brain homeobox 2 (GBX2), insulin growth factor (IGF) pathway (genes IGFBP3, IGFBP6, CTGF), Notch pathway (genes manic fringe [MFNG] and metallopeptidase domain 11 [ADAM11]), Hedgehog pathway (gene Patched [PTCH]) and Wnt pathway (genes FRAT2 and secreted frizzled-related protein 1 [SFRP1]) (19). In addition, transcription factors from Sry-related HMG box (SOX) gene family are upregulated during the RA induced neural differentiation, such as SOX3, one of the earliest neural markers (28). It has been postulated that cumulative regulation of SOX target genes during neurogenesis is the result of a fine balance between gene expression control regulated by members of SOXB1 (SOX1, SOX2, SOX3) and SOXB2 (SOX14 and SOX21) gene subfamilies (29–31). The increase in SOXB2 protein levels activates proneural proteins, which subsequently interfere with SOXB1 function, leading to differentiation of a neural progenitor towards neuronal phenotype (29). Members of SOXB subfamily are directly (32–34) and indirectly (35–37) regulated by RA and RA effector signaling. SOXB protein expression changes during the course of differentiation (20), which makes them a group of genes that participate in RA mediated proliferation-differentiation switches. In addition, many genes associated with cell adhesion, cytoskeletal and matrix remodeling, growth suppression, and intracellular signaling cascades are also activated by RA (7). Conversely, the majority of genes repressed by RA are involved in protein/RNA processing and turnover or metabolism, such as ZIC, Geminin (GMNN), NOTCH, and FOXD4L1, reviewed in Janesick et al. (15). RA signaling also includes examples of epigenetic regulation, such as upregulation and downregulation of small non-coding RNA molecules, especially microRNAs, which through their target genes regulate differentiation process (38). For example, miR-219 is an important contributor in transmission of RA effects (39). In the presence of RA, miR-219 is upregulated and suppresses expression of mRNAs for Forkhead box J3 (FOXJ3) and zinc finger and BTB domain containing 18 (ZBTB18) genes, known as blockers of neural differentiation. In addition, RA stabilizes tumor suppressor protein p53 in human ESCs. In its turn, p53 activates expression of miR-34a and miR-145, which repress expression of mRNAs for OCT4, KLF4, LIN28A, and SOX2 and accelerate embryonic stem cell differentiation (40). These findings suggest that microRNAs are particularly important in regulation of RA associated differentiation of embryonic stem cells. In other tissue and organ systems, RA is similarly involved in differentiation and maturation of cells, such as retinal cells of the eye (41), blood cells (42,43), sperm (44,45), and so on. RA has long been known to modulate cell growth and differentiation in many epithelial tissues, including the epidermis. When human keratinocytes are grown on fabricated collagen lattices as 43 dermal equivalent, physiologic concentrations (1–10 nm) of RA induce keratinocyte differentiation and formation of epithelium, similar to that in normally keratinized epidermis. Higher concentration (>0.1 µm) of RA reduces epidermal maturation and produces parakeratosis, while deficiency of RA leads to hyperkeratosis (46). Excess of vitamin A can induce transdifferentiation of chick embryonic epidermis to a mucous epithelium, and this process is mediated via Gbx1 homeobox genes which is a direct target of RA (47). The proper response to RA treatment of various skin conditions highly depends on thyroid hormone (TH) status. TH receptors modulate skin response to retinoids, and an insufficient amount of TH bound to its receptors affects modulation of both the proliferative response to retinoids and their inhibitory effects on skin differentiation (48). Complex interplay between RA, its target genes, and downstream effectors indicates that the process of cell differentiation by RA is precisely controlled and remarkably complex. Lack of RA during development results in severe developmental defects, while loss of RA signaling in adulthood causes cell dedifferentiation and development of cancer. Although vitamin A derivatives play a crucial role in embryonic development, retinoids are highly teratogenic, especially during early pregnancy. Fetal deformity induced by retinoid administration include central nervous system malformations, craniofacial dysmorphisms, heart defects, and defects of the thymic or parathyroid gland (49). Therefore, therapeutic administration of retinoids in treatment of various skin conditions should be carefully considered, which includes effective contraception during the treatment of women of childbearing age, even months after the end of therapy. The Role of Retinoids in Apoptosis Programmed cell death, or apoptosis, is a precisely regulated cellular process which enables proper organogenesis during embryonic development and maintenance of normal tissue homeostasis in adulthood. Deregulation of apoptosis results in developmental defects, autoimmune diseases, and malignancies. Phenomena that differentiate apoptosis from necrotic cell death include cell shrinkage, chromatin condensation, and DNA fragmentation (50). Apoptosis can be conducted via intrinsic or extrinsic pathways which differ in types of receptors responsible for receiving apoptotic signals. An intrinsic pathway is initiated in response to cell stress caused by DNA damage or growth factor deficiency. It is mediated by changes in permeability of the mitochondrial outer membrane which is regulated through interactions between pro- and anti-apoptotic members of the Bcl-2 family of proteins. This results in release of mitochondrial factors, most importantly cytochrome C, leading to loss of mitochondrial functions and initiation of a cascade of caspase protease activities and cell death, reviewed in Elmore (50); Noy (51); Tait and Green (52). An extrinsic apoptosis pathway is activated upon binding of extracellular ligands, such as TNF-α, Fas cell surface death receptor (FAS), and TRAIL, to the corresponding death receptors localized on cell membrane. Activation of death receptors and recruitment of adaptor proteins activate effectors of apoptosis such as procaspase 8 and induce downstream apoptotic signaling (53). 44 Control of development mediated by RA depends on regulation of apoptosis as much as it does on differentiation. On the molecular level, apoptosis induction by RA occurs through the signaling cascade, including cellular RA-binding protein 2 (CPABP2) and retinoic acid receptor (RAR). Delivery of RA to RAR by CRABP2 enhances transcriptional activity of genes involved in cell death and cell cycle arrest (51). Apoptosis regulators, regulated by RAR, are numerous. They include caspases, Bcl-2, and numerous transcription factors that regulate apoptosis etc. For example, the initiator of apoptosis caspase 9 is a direct target of RAR in mammary carcinoma cells (54). In keratinocytes, RA upregulates the expression of caspases 3, 6, 7, and 9 and contributes to their apoptosis in response to UV light or doxorubicin (55). RA modulates the expression of both proapoptotic and antiapoptotic Bcl-2 proteins, as well as the tumor suppressor p53. RA upregulates the expression of p53 in several cancer cell types, such as pancreatic (56), metastatic melanoma (57,58), myeloblastic leukemia, (59) and cervical cancer cells (60). Also, activating or overexpressing PPAR-β/δ induces cell differentiation through p53- and SOX2-dependent signaling pathways in neuroblastoma cells and tumors (61). Recognition of intrinsic apoptosis triggers such as DNA damage leads to activation of tumor suppressor protein p53; at the same time, upregulation of the p53 gene is also induced by RA. While this is one of the ways in which RA can support p53-­ mediated steps of apoptosis, it is not the only way in which RA can contribute to p53 activity. For example, another RA upregulated gene, such as SOX14, leads to stabilization of the p53 protein in other cell types (cervical carcinoma), making the complex picture even more complex (62). Further work is needed in order to understand the extent to which RA-induced genes, important in development, participate in p53 stabilization and contribute to induction of apoptosis and overcoming of the cancer phenotype. Cellular differentiation, cell cycle arrest, and apoptosis can all stall or even abolish growth of tumors. Each of these processes can be triggered by RA, and this makes it a promising pharmacologic agent for cancer therapy. RA is clinically used for treatment of several malignancies, such as promyelocytic leukemia, Kaposi sarcoma, neuroblastoma, and premalignancies, including leukoplakia, actinic keratosis, and xeroderma pigmentosum (26,63,64). Combination treatments with RA and different chemotherapeutics, such as taxoids, kinase inhibitors, HER2 inhibitors, proteasome inhibitors, and nanoformulations of tretinoin, have demonstrated additive or synergistic anticancer effects. The mechanisms by which the compounds act in synergy with RA depend on the tumor and the cell type. Often, when the synergistic cell killing was observed, the predominant effect of RA on cells was induction of differentiation (65); nevertheless, it is known that growth inhibition by RA is cell-type specific and in some carcinoma cells RA induces proliferation and promotes cell survival. The major molecular mechanism responsible for this dual effect of RA is based on relative expression levels of the two RA-binding proteins CRABP2 (which shuttles RA to RAR) and FABP5 (which transports it to PPAR-β/δ). RA induces apoptosis in cells that express a high CRABP2/FABP5 ratio and thus efficiently activate RAR. RA functions as a survival factor in cells in which the binding protein ratio is low, enabling gene activation mediated by PPAR-β/δ (Figure 8.4). PPAR-β/δ gene targets activate cell survival pathways and genes involved in cell proliferation, as reviewed in Noy (51) and Napoli (66). Retinoids in Dermatology FIGURE 8.4 Growth inhibition versus growth enhancement induced by RA is mediated by relative expression levels of the two RA-binding proteins CRABP2, which shuttles RA to RAR, and FABP5, which transports it to PPAR-β/δ. RA induces apoptosis in cells that have high CRABP2/FABP5 ratio, while cell survival is improved in cells where this binding protein ratio is low. Retinoic acid has been found to have inhibitory effects on growth of murine melanomas (67) and colony formation of human melanomas (68). In addition to inhibiting growth, retinoic acid has been found to inhibit human melanoma tumor cell invasion (69). Retinoic acid has also been indicated to inhibit highly metastatic B16F10 melanoma cells by downregulating the cell surface integrin receptors against extracellular matrix proteins, specifically laminin and vitronectin (70). Epidermal growth factor receptor (EGFR) is a crucial player in epithelial cells in both growth and migration/invasion, and its expression is regulated by retinoic acid as well (71). Taken together, the role of retinoids in regulation of different aspects of cellular death is remarkable; nevertheless, special precautions must be undertaken due to the limitation of the use of RA as a chemotherapeutic agent which can possibly develop RA resistance (72,73). Retinoids are useful in prevention of precancer lesions in skin and in the treatment of acne and psoriasis. 13-cis RA inhibits growth and induces apoptosis in SEB-1 sebocytes (74). 13-cis RA causes significant dose-dependent and time-dependent decreases in viable SEB-1 sebocytes by cell cycle arrest as confirmed by decreased DNA synthesis, increased p21 protein expression, and decreased cyclin D1. The mechanism of action also includes apoptosis in SEB-1 sebocytes as shown by increased cleaved caspase 3 protein and detection of early apoptotic marker phosphatidylserine. This mechanism of action is confirmed only for 13-cis RA but not to 9-cis or all-trans-RA. Finally, induction of apoptosis by 13-cis RA does not appear to involve RAR nuclear receptors (74). In keratinocytes, it is highly important to maintain the process of apoptosis properly in order to maintain skin homeostasis and formation of stratum corneum. Deregulation of keratinocyte apoptosis is, besides the autoimmune aspect, the major hallmark Effects of Retinoids at the Cellular Level (Differentiation, Apoptosis, Autophagy, Cell Cycle Regulation, and Senescence) of psoriasis—chronic inflammatory skin disease characterized by hyperproliferation with incomplete differentiation of epidermal keratinocytes and decreased apoptosis. The process by which keratinocytes undergo apoptosis is a multistep program mediated by binding of specific death ligands to death receptors or by the release of effector cell granules (75). Expression analysis of p53 and Bcl-2 revealed that Bcl-2 does not appear to play an important role in the apoptotic process in psoriasis, while p53 expression likely plays an important role in etiology of this condition (76). The microarray analysis used to identify RA target genes in primary human epidermal keratinocytes revealed that many psoriatic genes are deregulated upon treatment with RA (77). Namely, of the 146 known psoriasis-associated genes, 28 were not expressed in primary human keratinocytes. Of the remaining genes, 86 were regulated by RA, 29 were induced, 42 suppressed, and 15 both induced and suppressed but at different time points. Among the 29 induced and 42 suppressed genes, 54 were specified in the literature either as induced or as suppressed in psoriasis (77). The role of retinoids in maintenance of skin homeostasis is noteworthy. The use of retinoids and their special formulations in prevention and cure of various skin conditions has been an important field of research for many decades, which resulted in the clinical use of different types of therapeutics (78). The Role of Retinoids in Cell Cycle Regulation The role of RA in cell cycle regulation is tightly connected with cell differentiation and apoptosis. Molecular mechanisms, which lead to cell cycle arrest induced by RA, have been studied mostly in various types of malignances, and results of these studies suggest that cyclin-dependent kinases (CDK) are major effectors of RA response in cell cycle regulation. The role of RA in cell cycle regulation was reported in ­promyelocytic leukemia and U-937 cells, derived from histiocytic lymphoma, where RA treatment induced G0/G1 arrest. Corresponding gene expression changes included downregulation of c-Myc and cyclin E, increased expression of p21WAF1/CIP1, and increased stability of p27Kip1 (79,80). Treatment with RA also affects CDK5 activity, and several papers described how RA induces cell cycle arrest (81–83). CDK5, together with its activator p35, is important for induction of neuronal differentiation (84). CDK5 also regulates the growth of various cancers, such as thyroid (85), cervical (86), and prostate (87). Activation of CDK5 leads to upregulation of p27, which is the main effector in RA-mediated cell cycle regulation (82). In addition, cell cycle progression upon treatment with RA is dependent on the cyclin family of proteins, in particular Cyclin C expression. As a partner of cyclin-dependent kinase 3 (CDK3), Cyclin C controls cellular proliferation and, together with CDK8, represses gene transcription. Cyclin C gene is a direct target for RA in HEK293 human embryonal kidney cells, containing two RAR binding sites (88). As contradictory effects of RA can be noted in conjunction with apoptosis, the same is true for RA in cell cycle progression. While its effects on cell cycle are mostly inhibitory, RA can sometimes show a pro-proliferation mode of action. In the liver, 45 the RA treatment accelerates its regeneration by induction of cell cycle, and this process is triggered by binding of RAR-β/RXR-α to CDK1, CDK2, Cyclin D, and CDK6 genes (89). The Role of Retinoids in Autophagy Autophagy is an evolutionarily conserved intracellular pathway for degradation and recycling of cytoplasmic proteins, macromolecules, and organelles with the purpose of preserving cellular homeostasis (90). This is a catabolic process during which macromolecules and damaged organelles are sequestered, along with a portion of cytosol, into a double or multi-membrane structure known as a phagophore, which elongates, closes, and forms a vesicular structure known as the autophagosome (90). The autophagosome is further fused with lysosomes and degraded by the autophagosomal-lysosomal pathway (90,91). Autophagy plays a critical role in processes of inflammation, autoimmunity, and cellular differentiation. It predominantly acts as a barrier against conditions that initiate tumorigenesis, but it can also have a pro-survival role in already established tumors, particularly during tumor invasion and drug resistance (91). Autophagy has been linked with keratinocyte differentiation and melanocyte survival, as well as with the pathogenesis of diverse skin disorders including systemic lupus erythematosus, systemic sclerosis, psoriasis, vitiligo, infectious skin diseases, and skin cancer, as reviewed in (92,93). In addition to many other stimuli, RA signaling is known as a trigger of autophagy. The role of RA in this complex process was elucidated mostly by analyzing different health conditions, such as cancer (mostly leukemia) and the immune response to microbial infection. Specifically, RA promotes autophagosome maturation through a pathway independent from the classic nuclear retinoid receptors (94). It redistributes the cation-independent mannose-6-­phosphate receptor from the trans-Golgi region to maturing autophagosomal structures which in turn induces their acidification (95). In acute myeloid leukemia, immature blood cells are accumulated in bone marrow, where autophagy is a key component for RA-induced differentiation of such cells (96). In addition, RA upregulates autophagy-related proteins, microtubule-associated protein 1 light chain 3 (LC3-I, LC3-II), and Beclin-1 in promyeloid leukemia (97). In studies of liver ischemia and reperfusion injury, RA pretreatment was found to reduce this injury by inducing autophagy. The molecular mechanism involved in this process is based upon RAR-α activation which enhances FOXO3 and AKT serine/threonine kinase 1 (AKT1) expression. The FOXO3/ AKT1/FOXO1 pathway has previously been shown to promote autophagy (98); by activating RAR-α, RA regulates this pathway and helps to reduce liver ischemia and reperfusion injury (99). RA is a very important molecule for the regulation of the process of autophagy in various cells and conditions. Because autophagy presents a potential therapeutic target for skin and many other diseases, more investigations are needed for optimizing strategies to inhibit or enhance autophagy using RA for clinical efficacy. Aging is a complex process which is not fully understood in the context of autophagy. The process of aging is accompanied with cellular stress having a significant impact on skin. A recent study (100) demonstrated that according to transmission electron 46 microscopy analyses, the number of autophagosomes per 1 µm2 cytoplasmic area was similar between young and aged fibroblasts. The amount of LC3-II, a form associated with autophagic vacuolar membranes, was also similar between the groups. Although residual bodies were more common in aged dermal fibroblasts, LC3 turnover and p62 assay showed little difference in the rate of lysosomal proteolysis between the young and old. The authors postulated that with a higher speed and amount of waste production in aged cells, autophagic flux may not be sufficient in keeping the old cells “clean,” resulting in skin aging. Autophagy plays a crucial role in counteracting aging, and strategies aimed at its modulation should hold promise for the prevention of skin aging (100). The Role of Retinoids in Senescence Cellular senescence is the process which leads to irreversible cell cycle arrest and is induced by different types of stressors. In addition to exiting the cell cycle, senescent cells have many other phenotypic alterations, such as metabolic reprogramming, chromatin rearrangements, or autophagy modulation (101). Transition of cells into senescence is the process which can affect a variety of physiologic and pathologic processes, including cancer and age-related diseases. Efforts to find pro-senescence and anti-senescence therapeutics are founded in the notion that if senescence could be regulated, cures for many diseases would be discovered. Retinoids, known as differentiation agents, are often studied in this context. RA induces several features of cellular senescence, including irreversible G1 arrest, morphologic changes, increased senescence-associated β-galactosidase, and the presence of heterochromatin foci (102). The main mechanism of RA-induced senescence seems to be p21 induction. This small protein is a direct target of RA, as it contains two consecutive retinoid X response elements in the promoter, which are responsible for RXR ligand-dependent p21 upregulation (103). In addition, RA upregulates levels of p16 and p21 via promoter hypomethylation and downregulation of DNA methyltransferases 1, 3a, and 3b. This facilitates binding of Ets1/2 to the p16 promoter and p53 to the p21 promoter, resulting in upregulation of their expression and subsequent support for induction of cellular senescence in liver cancer cells. These effects are mediated by RAR-β2, whose promoter is also hypomethylated in the presence of RA (104). Telomerase activity is also linked to retinoid-induced cell senescence (105). The shortening of telomeres and decreased telomerase complex activity leads to gene instability, activation of p53, and induction of senescence in p53-dependent manner (106). The importance of understanding mechanisms of cellular senescence induced by RA is immense. Manipulation of this process could be helpful in the battle against cancer as well as for various age-related chronic diseases. Skin aging is influenced by many factors, including genetics, environmental exposure (mainly UV radiation, xenobiotics, and mechanical stress), hormonal changes, and metabolic processes. All those factors together act on the alterations of skin structure, function, and appearance. The single major factor responsible for skin aging is solar UV radiation (107). Retinoids in Dermatology Contrary to the mechanism of action described for liver cancer cells, it is known that skin senescence can be partly prevented by topical application of various retinoids (108). Topical application of RA results in histologic improvements including increased dermal collagen synthesis (109) and blocking of collagenase activity, thus preventing collagen degradation. This is the main molecular mechanism of antiaging efficacy induced by RA (110). On the other hand, all-trans retinols induce epidermal thickening and enhance expression of CRABPII (111). Despite its promising antiaging effects, RA treatment causes skin irritation such as burning, scaling, and dermatitis, limiting its application for some patients, which argues its careful administration in antiaging therapy. Using retinol in treatment resulted in fewer signs of erythema and skin irritations compared to RA (112). Retinol was effective in producing retinoid-mediated histological changes, such as keratinocyte proliferation. Conclusions The involvement of retinoids and retinoic acid, as their final effector in regulation of most of the critical cellular processes, is crucial, and the evidence of the complexity of RA signaling regulation and the interplay between its different downstream targets is continually developing. There is no cellular process which is not, at least in part, controlled by RA. A comprehensive understanding of RA signaling and associated pathways is of high priority, because it provides important insights into cell biology and pathology, and it promises new developments for the use of RA in prevention and therapy of cancer and numerous chronic diseases. REFERENCES 1. Schilling TF, Sosnik J, Nie Q. Visualizing retinoic acid morphogen gradients. Methods Cell Biol. 2016;133:139–163. 2. Kang S. The mechanism of action of topical retinoids. Cutis. 2005;75:10–13. 3. Coyle KM, Sultan M, Thomas ML et al. Retinoid signaling in cancer and its promise for therapy. J Carcinogene Mutagene. 2013;S7:006. 4. Gudas LJ, Wagner JA. Retinoids regulate stem cell differentiation. J Cell Physiol. 2011;226:322–330. 5. Napoli JL. Functions of intracellular retinoid binding-­proteins. Subcell Biochem. 2016;81:21–76. 6. Sever R, Glass CK. Signaling by nuclear receptors. Cold Spring Harb Perspect Biol. 2013;5:a016709. 7. Balmer JE, Blomhoff R. Gene expression regulation by retinoic acid. J Lipid Res. 2002;43:1773–1808. 8. Bayha E, Jorgensen MC, Serup P et al. Retinoic acid signaling organizes endodermal organ specification along the entire antero-posterior axis. PLOS ONE. 2009;4:e5845. 9. Chambon P. A decade of molecular biology of retinoic acid receptors. FASEB J. 1996;10:940–954. 10. Duong V, Rochette-Egly C. The molecular physiology of nuclear retinoic acid receptors. From health to disease. Biochim Biophys Acta. 2011;1812:1023–1031. 11. Lefebvre P, Martin PJ, Flajollet S et al. Transcriptional activities of retinoic acid receptors. Vitam Horm. 2005;70:199–264. Effects of Retinoids at the Cellular Level (Differentiation, Apoptosis, Autophagy, Cell Cycle Regulation, and Senescence) 12. Forman BM, Umesono K, Chen J et al. Unique response pathways are established by allosteric interactions among nuclear hormone receptors. Cell. 1995;81:541–550. 13. Westin S, Kurokawa R, Nolte RT et al. Interactions controlling the assembly of nuclear-receptor heterodimers and coactivators. Nature. 1998;395:199–202. 14. Rhinn M, Dolle P. Retinoic acid signalling during development. Development. 2012;139:843–858. 15. Janesick A, Wu SC, Blumberg B. Retinoic acid signaling and neuronal differentiation. Cell Mol Life Sci. 2015;72:1559–1576. 16. Blumberg B, Bolado J, Jr., Moreno TA et al. An essential role for retinoid signaling in anteroposterior neural patterning. Development. 1997;124:373–379. 17. Yang J, Wu C, Stefanescu I et al. Analysis of retinoic acidinduced neural differentiation of mouse embryonic stem cells in two and three-dimensional embryoid bodies. J Vis Exp. 2017;122. doi:10.3791/55621. 18. Rochette-Egly C. Retinoic acid signaling and mouse embryonic stem cell differentiation: Cross talk between genomic and nongenomic effects of RA. Biochim Biophys Acta. 2015;1851:66–75. 19. Freemantle SJ, Kerley JS, Olsen SL et al. Developmentallyrelated candidate retinoic acid target genes regulated early during neuronal differentiation of human embryonal carcinoma. Oncogene. 2002;21:2880–2889. 20. Popovic J, Stanisavljevic D, Schwirtlich M et al. Expression analysis of SOX14 during retinoic acid induced neural differentiation of embryonal carcinoma cells and assessment of the effect of its ectopic expression on SOXB members in HeLa cells. PLOS ONE. 2014;9:e91852. 21. Andrews PW. Retinoic acid induces neuronal differentiation of a cloned human embryonal carcinoma cell line in vitro. Dev Biol. 1984;103:285–293. 22. Guillemain I, Alonso G, Patey G et al. Human NT2 neurons express a large variety of neurotransmission phenotypes in vitro. J Comp Neurol. 2000;422:380–395. 23. Hartley RS, Margulis M, Fishman PS et al. Functional synapses are formed between human NTera2 (NT2N, hNT) neurons grown on astrocytes. J Comp Neurol. 1999;407:1–10. 24. Pleasure SJ, Page C, Lee VM. Pure, postmitotic, polarized human neurons derived from NTera 2 cells provide a system for expressing exogenous proteins in terminally differentiated neurons. J Neurosci. 1992;12:1802–1815. 25. Maden M. Retinoic acid in the development, regeneration and maintenance of the nervous system. Nat Rev Neurosci. 2007;8:755–765. 26. Soprano DR, Teets BW, Soprano KJ. Role of retinoic acid in the differentiation of embryonal carcinoma and embryonic stem cells. Vitam Horm. 2007;75:69–95. 27. Gehring WJ, Affolter M, Burglin T. Homeodomain proteins. Annu Rev Biochem. 1994;63:487–526. 28. Stevanovic M. Modulation of SOX2 and SOX3 gene expression during differentiation of human neuronal precursor cell line NTERA2. Mol Biol Rep. 2003;30:127–132. 29. Sandberg M, Kallstrom M, Muhr J. Sox21 promotes the progression of vertebrate neurogenesis. Nat Neurosci. 2005;8:995–1001. 30. Uchikawa M, Kamachi Y, Kondoh H. Two distinct subgroups of Group B Sox genes for transcriptional activators and repressors: Their expression during embryonic organogenesis of the chicken. Mech Dev. 1999;84:103–120. 47 31. Whittington N, Cunningham D, Le TK et al. Sox21 ­regulates the progression of neuronal differentiation in a dose-­dependent manner. Dev Biol. 2015;397:237–247. 32. Mojsin M, Grujicic NK, Nikcevic G et al. Mapping of the RXRalpha binding elements involved in retinoic acid induced transcriptional activation of the human SOX3 gene. Neurosci Res. 2006;56:409–418. 33. Nikcevic G, Kovacevic-Grujicic N, Mojsin M et al. Regulation of the SOX3 gene expression by retinoid receptors. Physiol Res. 2011;60:S83–S91. 34. Nikcevic G, Savic T, Kovacevic-Grujicic N et al. Up-regulation of the SOX3 gene expression by retinoic acid: Characterization of the novel promoter-response element and the retinoid receptors involved. J Neurochem. 2008;107:1206–1215. 35. Kovacevic-Grujicic N, Mojsin M, Popovic J et al. Cyclic AMP response element binding (CREB) protein acts as a positive regulator of SOX3 gene expression in NT2/D1 cells. BMB Rep. 2014;47:197–202. 36. Krstic A, Mojsin M, Stevanovic M. Regulation of SOX3 gene expression is driven by multiple NF-Y binding elements. Arch Biochem Biophys. 2007;467:163–173. 37. Mojsin M, Popovic J, Kovacevic Grujicic N et al. TG-interacting factor (TGIF) downregulates SOX3 gene expression in the NT2/D1 cell line. J Genet Genomics. 2012;39:19–27. 38. Nervi C, Grignani F. RARs and microRNAs. Subcell Biochem. 2014;70:151–179. 39. Wu H, Zhao J, Fu B et al. Retinoic acid-induced upregulation of miR-219 promotes the differentiation of embryonic stem cells into neural cells. Cell Death Dis. 2017;8:e2953. 40. Jain AK, Allton K, Iacovino M et al. p53 regulates cell cycle and microRNAs to promote differentiation of human embryonic stem cells. PLOS Biol. 2012;10:e1001268. 41. Kelley MW, Turner JK, Reh TA. Retinoic acid promotes differentiation of photoreceptors in vitro. Development. 1994;120:2091–2102. 42. Cabezas-Wallscheid N, Buettner F, Sommerkamp P et al. Vitamin A-retinoic acid signaling regulates hematopoietic stem cell dormancy. Cell. 2017;169:807–823. e819. 43. Ronn RE, Guibentif C, Moraghebi R et al. Retinoic acid regulates hematopoietic development from human pluripotent stem cells. Stem Cell Reports. 2015;4:269–281. 44. Brocard J, Kastner P, Chambon P. Two novel RXR alpha isoforms from mouse testis. Biochem Biophys Res Commun. 1996;229:211–218. 45. Jauregui EJ, Mitchell D, Topping T et al. Retinoic acid receptor signaling is necessary in steroidogenic cells for normal spermatogenesis and epididymal function. Development. 2018;145:pii:dev160465. 46. Asselineau D, Bernard BA, Bailly C et al. Retinoic acid improves epidermal morphogenesis. Dev Biol. 1989;133:322–335. 47. Akimoto Y, Miyaji M, Morimoto-Kamata R et al. Retinoic acid-induced epidermal transdifferentiation in skin. J Dev Biol. 2014;2:158–173. 48. Garcia-Serrano L, Gomez-Ferreria MA, Contreras-Jurado C et al. The thyroid hormone receptors modulate the skin response to retinoids. PLOS ONE. 2011;6:e23825. 49. Lammer EJ, Chen DT, Hoar RM et al. Retinoic acid embryopathy. N Engl J Med. 1985;313:837–841. 50. Elmore S. Apoptosis: A review of programmed cell death. Toxicol Pathol. 2007;35:495–516. 48 51. Noy N. Between death and survival: Retinoic acid in regulation of apoptosis. Annu Rev Nutr. 2010;30:201–217. 52. Tait SWG, Green DR. Mitochondrial regulation of cell death. Cold Spring Harb Perspect Biol. 2013;5. 53. Walczak H, Krammer PH. The CD95 (APO-1/Fas) and the TRAIL (APO-2L) apoptosis systems. Exp Cell Res. 2000;256:58–66. 54. Donato LJ, Noy N. Suppression of mammary carcinoma growth by retinoic acid: Proapoptotic genes are targets for retinoic acid receptor and cellular retinoic acid-binding protein II signaling. Cancer Res. 2005;65:8193–8199. 55. Mrass P, Rendl M, Mildner M et al. Retinoic acid increases the expression of p53 and proapoptotic caspases and sensitizes keratinocytes to apoptosis: A possible explanation for tumor preventive action of retinoids. Cancer Res. 2004;64:6542–6548. 56. Li J, Orr B, White K et al. Chmp 1A is a mediator of the antiproliferative effects of all-trans retinoic acid in human pancreatic cancer cells. Mol Cancer. 2009;8:7. 57. Guruvayoorappan C, Pradeep CR, Kuttan G. 13-cis-retinoic acid induces apoptosis by modulating caspase-3, bcl-2, and p53 gene expression and regulates the activation of transcription factors in B16F-10 melanoma cells. J Environ Pathol Toxicol Oncol. 2008;27:197–207. 58. Zhang H, Rosdahl I. Expression profiles of p53, p21, bax and bcl-2 proteins in all-trans-retinoic acid treated primary and metastatic melanoma cells. Int J Oncol. 2004;25:303–308. 59. Zheng A, Mantymaa P, Saily M et al. p53 pathway in apoptosis induced by all-trans-retinoic acid in acute myeloblastic leukaemia cells. Acta Haematol. 2000;103:135–143. 60. Um SJ, Kim EJ, Hwang ES et al. Antiproliferative effects of retinoic acid/interferon in cervical carcinoma cell lines: Cooperative growth suppression of IRF-1 and p53. Int J Cancer. 2000;85:416–423. 61. Yao PL, Chen L, Dobrzanski TP et al. Peroxisome ­proliferator-activated receptor-beta/delta inhibits human neuroblastoma cell tumorigenesis by inducing p53- and SOX2mediated cell differentiation. Mol Carcinog. 2017;56:1472–1483. 62. Stanisavljevic D, Petrovic I, Vukovic V et al. SOX14 activates the p53 signaling pathway and induces apoptosis in a cervical carcinoma cell line. PLOS ONE. 2017;12:e0184686. 63. Altucci L, Gronemeyer H. The promise of retinoids to fight against cancer. Nat Rev Cancer. 2001;1:181–193. 64. Ni X, Hu G, Cai X. The success and the challenge of all-trans retinoic acid in the treatment of cancer. Crit Rev Food Sci Nutr. 2018:1–10. 65. Schultze E, Collares T, Lucas CG et al. Synergistic and additive effects of ATRA in combination with different anti-tumor compounds. Chem Biol Interact. 2018;285:69–75. 66. Napoli JL. Cellular retinoid binding-proteins, CRBP, CRABP, FABP5: Effects on retinoid metabolism, function and related diseases. Pharmacol Ther. 2017;173: 9–33. 67. Lotan R, Giotta G, Nork E et al. Characterization of the inhibitory effects of retinoids on the in vitro growth of two malignant murine melanomas. J Natl Cancer Inst. 1978;60:1035–1041. 68. Meyskens FL, Jr., Salmon SE. Inhibition of human melanoma colony formation by retinoids. Cancer Res. 1979;39:4055–4057. 69. Wood WR, Seftor EA, Lotan D et al. Retinoic acid inhibits human melanoma tumor cell invasion. Anticancer Res. 1990;10:423–432. Retinoids in Dermatology 70. Sengupta S, Ray S, Chattopadhyay N et al. Effect of retinoic acid on integrin receptors of B16F10 melanoma cells. J Exp Clin Cancer Res. 2000;19:81–87. 71. Yongshan Y, DeBauche DM, Stanley WS. Epidermal growth factor receptor expression in a retinoic acid-treated human melanoma cell line. Cancer Genet Cytogenet. 1990;46:261–269. 72. Alonso S, Jones RJ, Ghiaur G. Retinoic acid, CYP26, and drug resistance in the stem cell niche. Exp Hematol. 2017;54:17–25. 73. Campos B, Weisang S, Osswald F et al. Retinoid resistance and multifaceted impairment of retinoic acid synthesis in glioblastoma. Glia. 2015;63:1850–1859. 74. Nelson AM, Gilliland KL, Cong Z et al. 13-cis Retinoic acid induces apoptosis and cell cycle arrest in human SEB-1 sebocytes. J Invest Dermatol. 2006;126:2178–2189. 75. Kastelan M, Prpic-Massari L, Brajac I. Apoptosis in psoriasis. Acta Dermatovenerol Croat. 2009;17:182–186. 76. Moorchung N, Vasudevan B, Dinesh Kumar S et al. Expression of apoptosis regulating proteins p53 and bcl-2 in psoriasis. Indian J Pathol Microbiol. 2015;58:423–426. 77. Lee DD, Stojadinovic O, Krzyzanowska A et al. Retinoidresponsive transcriptional changes in epidermal keratinocytes. J Cell Physiol. 2009;220:427–439. 78. Beckenbach L, Baron JM, Merk HF et al. Retinoid treatment of skin diseases. Eur J Dermatol. 2015;25:384–391. 79. Dimberg A, Bahram F, Karlberg I et al. Retinoic acid-induced cell cycle arrest of human myeloid cell lines is associated with sequential down-regulation of c-Myc and cyclin E and posttranscriptional up-regulation of p27(Kip1). Blood. 2002;99:2199–2206. 80. Hu XT, Zuckerman KS. Role of cell cycle regulatory molecules in retinoic acid- and vitamin D3-induced differentiation of acute myeloid leukaemia cells. Cell Prolif. 2014;47:200–210. 81. Lee JH, Kim KT. Induction of cyclin-dependent kinase 5 and its activator p35 through the extracellular-signal-regulated kinase and protein kinase A pathways during retinoic-acid mediated neuronal differentiation in human neuroblastoma SK-N-BE(2)C cells. J Neurochem. 2004;91:634–647. 82. Lin E, Chen MC, Huang CY et al. All-trans retinoic acid induces DU145 cell cycle arrest through Cdk5 activation. Cell Physiol Biochem. 2014;33:1620–1630. 83. Shah K, Lahiri DK. Cdk5 activity in the brain—multiple paths of regulation. J Cell Sci. 2014;127:2391–2400. 84. Tsai LH, Delalle I, Caviness VS, Jr. et al. p35 is a neural-­ specific regulatory subunit of cyclin-dependent kinase 5. Nature. 1994;371:419–423. 85. Lin H, Chen MC, Chiu CY et al. Cdk5 regulates STAT3 activation and cell proliferation in medullary thyroid carcinoma cells. J Biol Chem. 2007;282:2776–2784. 86. Kuo HS, Hsu FN, Chiang MC et al. The role of Cdk5 in retinoic acid-induced apoptosis of cervical cancer cell line. Chin J Physiol. 2009;52:23–30. 87. Chen MC, Huang CY, Hsu SL et al. Retinoic Acid Induces Apoptosis of Prostate Cancer DU145 Cells through Cdk5 Overactivation. Evid Based Complement Alternat Med. 2012;2012:580736. 88. Makkonen KM, Malinen M, Ropponen A et al. Cell cycle regulatory effects of retinoic Acid and forskolin are mediated by the cyclin C gene. J Mol Biol. 2009;393:261–271. 89. Liu HX, Ly I, Hu Y et al. Retinoic acid regulates cell cycle genes and accelerates normal mouse liver regeneration. Biochem Pharmacol. 2014;91:256–265. Effects of Retinoids at the Cellular Level (Differentiation, Apoptosis, Autophagy, Cell Cycle Regulation, and Senescence) 90. Klionsky DJ. Autophagy: From phenomenology to molecular understanding in less than a decade. Nat Rev Mol Cell Biol. 2007;8:931–937. 91. Levine B, Kroemer G. Autophagy in the pathogenesis of disease. Cell. 2008;132:27–42. 92. Li L, Chen X, Gu H. The signaling involved in autophagy machinery in keratinocytes and therapeutic approaches for skin diseases. Oncotarget. 2016;7:50682–50697. 93. Sil P, Wong SW, Martinez J. More than skin deep: Autophagy is vital for skin barrier function. Front Immunol. 2018;9:1376. 94. Rajawat Y, Hilioti Z, Bossis I. Autophagy: A target for retinoic acids. Autophagy. 2010;6:1224–1226. 95. Rajawat Y, Hilioti Z, Bossis I. Retinoic acid induces autophagosome maturation through redistribution of the cationindependent mannose-6-phosphate receptor. Antioxid Redox Signal. 2011;14:2165–2177. 96. Orfali N, O’Donovan TR, Nyhan MJ et al. Induction of autophagy is a key component of all-trans-retinoic acid-induced differentiation in leukemia cells and a potential target for pharmacologic modulation. Exp Hematol. 2015;43:781–793 e782. 97. Mansour AH, Anwer R, Darwish A et al. All-trans-retinoid acid (ATRA) induced upregulation of autophagy related proteins (LC3–1, II and Beclin 1) in acute promyelocytic leukemia. Int J Pharmacol. 2014:315–321. 98. Zhou J, Liao W, Yang J et al. FOXO3 induces FOXO1dependent autophagy by activating the AKT1 signaling pathway. Autophagy. 2012;8:1712–1723. 99. Zhong C, Pu LY, Fang MM et al. Retinoic acid receptor alpha promotes autophagy to alleviate liver ischemia and reperfusion injury. World J Gastroenterol. 2015;21:12381–12391. 100. Kim HS, Park SY, Moon SH et al. Autophagy in human skin fibroblasts: Impact of age. Int J Mol Sci. 2018;19. 101. Aravinthan A. Cellular senescence: A hitchhiker’s guide. Human Cell 2015;28:51–64. 102. Park SH, Lim JS, Jang KL. All-trans retinoic acid induces cellular senescence via upregulation of p16, p21, and p27. Cancer Lett. 2011;310:232–239. 49 103. Tanaka T, Suh KS, Lo AM et al. p21WAF1/CIP1 is a common transcriptional target of retinoid receptors: Pleiotropic regulatory mechanism through retinoic acid receptor (RAR)/retinoid X receptor (RXR) heterodimer and RXR/RXR homodimer. J Biol Chem. 2007;282:29987–29997. 104. Lim JS, Park SH, Jang KL. All-trans retinoic acid induces cellular senescence by up-regulating levels of p16 and p21 via promoter hypomethylation. Biochem Biophys Res Commun. 2011;412:500–505. 105. Bednarek A, Shilkaitis A, Green A et al. Suppression of cell proliferation and telomerase activity in 4-(hydroxyphenyl)retinamide-treated mammary tumors. Carcinogenesis. 1999;20:879–883. 106. Feldser DM, Greider CW. Short telomeres limit tumor progression in vivo by inducing senescence. Cancer Cell. 2007;11:461–469. 107. Rittie L, Fisher GJ. UV-light-induced signal cascades and skin aging. Ageing Res Rev. 2002;1:705–720. 108. Mukherjee S, Date A, Patravale V et al. Retinoids in the treatment of skin aging: An overview of clinical efficacy and safety. Clin Interv Aging. 2006;1:327–348. 109. Griffiths CE, Russman AN, Majmudar G et al. Restoration of collagen formation in photodamaged human skin by tretinoin (retinoic acid). N Engl J Med. 1993;329:530–535. 110. Fisher GJ, Datta SC, Talwar HS et al. Molecular basis of sun-induced premature skin ageing and retinoid antagonism. Nature. 1996;379:335–339. 111. Kang S, Duell EA, Fisher GJ et al. Application of retinol to human skin in vivo induces epidermal hyperplasia and cellular retinoid binding proteins characteristic of retinoic acid but without measurable retinoic acid levels or irritation. J Invest Dermatol. 1995;105:549–556. 112. Kong R, Cui Y, Fisher GJ et al. A comparative study of the effects of retinol and retinoic acid on histological, molecular, and clinical properties of human skin. J Cosmet Dermatol. 2016;15:49–57. 9 Effects of Retinoids at the Systemic Level Sandra Maria Barbalho and Letícia Maria Pescinini-Salzedas Introduction The most commonly known biologic function of vitamin A (VA) is related to its participation in the visual cycle; however, this vitamin is also linked to a plethora of other physiologic and metabolic processes essential for homeostasis. VA is fundamental for the synthesis of some glycoproteins; in the modulation of cell differentiation and growth; in the production of mucus, bone formation, immune response, and cognitive development; and in endocrine function. VA is also relevant as an antioxidant and anti-inflammatory agent. A decrease of VA in blood levels has been linked to many diseases and age-related complications (1,2). VA is obtained as carotenoids from plants or as retinol or retinyl esters from animal sources. It is mainly stored in the liver and is metabolized to retinoic acid (RA), its main biologically active form. Among the five possible RA isomers, all-trans-RA (ATRA) is the main biologically active molecule (3). ATRA exerts many effects by stimulation of RA receptors (RARs), while 9-cis RA, another isomer, may also stimulate the retinoid X receptors (RXRs). These stimuli may lead to the regulation of over 500 responsive genes and can affect actions in many tissues, as shown in Figure 9.1 (4,5). VA and the Immune System In steady-state conditions, RA is released from the dendritic cells (DC) in the intestines and induces tolerance at the mucosal surfaces due to enhancement of tolerogenic DC and T regulatory cells. With infection or autoimmune responses, it may stimulate inflammatory DC and affect the T-cell responses. RA interferes with the homing of CD4+ and CD8+ T cells due to augmenting the release of molecules that induce preferred migration to the gut-associated lymphoid tissue. The RA produced by DC in the mucosa associated with TGF-β may activate the differentiation of naive T cells into FOXP3+ regulatory T cells, causing a balance in the production of anti-inflammatory cytokines that are related to the immune tolerance. These actions also occur in the alveolar macrophages of the lungs, resulting in respiratory tolerance due to the release of RA and TGF-β. RA is also capable of suppressing T helper 17 (TH17) and TH1 cell differentiation (6,7). In the bowel, RA, together with transforming growing factor-β (TGF-β), enhances the expression of Forkhead box P3 (FOXP3) (Figure 9.1), necessary to the role of Treg cells. In addition, it reduces the differentiation of T cells into TH-1 and TH17 and increases the expression of the antiinflammatory interleukin-10 (IL-10). With decreased amounts of RA, CD4+ T cells differentiate into TH1 lineage, resulting in the release of interferon-γ (IFN-γ) that is related to inflammation. These actions of RA modulate the inflammatory processes and prevent autoimmune T-cell stimulation (8). In B cells, the central immune regulatory role of RA is related to immunoglobulin class switching. The RA produced in DC in enterocytes induces the generation of IgA+ producing B cell and redoubles memory B-cell differentiation. These actions result in a severe increase both in the intestinal and serum IgA levels. RA also downregulates TH2 and IgE immune responses (9). Vitamin A and the Cardiovascular System RA is necessary to the embryonic and fetal cardiovascular development, including differentiation into adult cardiac muscle. Elevated or reduced levels of this compound may be related to congenital malformations of the heart and additional teratogenic effects on the cardiac system development (10). RA regulates the expression of several genes inducing the production of many proteins in the heart. The acceleration in the expression of cardiac-specific genes augments the development and differentiation of cardiomyocytes (Figure 9.1). It plays an essential function in the homeostasis of the structure and functions of this organ throughout life. The deficiency of RA results in thin myocardial walls in animal models, and heart failure. In excess, RA induces congenital disabilities in early stages of cardiogenesis, dilated cardiomyopathy, and cardiomyocyte abnormalities. For these reasons, RA seems to be crucial for the development and maintenance of the normal phenotype of the cardiomyocytes (10,11). ATRA is related to the modulation of the synthesis of collagen via TGF-β and can reduce hypoxia-induced injury in renal cells. It has the ability to inhibit hypertrophy and fibrosis in hypertensive rats, following myocardial infarction or carotid injury (12,13). RA is related to the induction of genes associated with the expression of renin-angiotensin system (RAS) components. As a result, in insufficient amounts, it may be related to myocardial infarction, cardiac hypertrophy, and cerebrovascular events. There is evidence that RA regulates the gene expression of such RAS components as renin and angiotensin-converting enzymes (10,14). 51 52 Retinoids in Dermatology FIGURE 9.1 Carotenoids and retinyl-esters from plant and animal sources with uptake by enterocytes. Bioactive metabolites are produced (ATRA and 9-cis RA) and play different effects in the immune system, heart, pancreas, and thyroid. (a) In the immune system, RA is related to downregulation of TH2 and TH17 and upregulation of Treg cells, IL-10, and TGF-β. (b) RA promotes beneficial effects on the heart, including the protection of endothelial cells. (c) In the pancreas, RA induces the secretion of insulin and activation of tyrosine-kinase enzymes. (d) In the thyroid, RA is associated with balance in the production of TSH and T4. The ligands of the RXR have been linked to cardioprotective effects by reducing inflammation, preventing atherosclerosis, and improving insulin resistance regulation of hyperglycemia and hyperinsulinemia in animal models with type 2 diabetes. RXR exerts an adverse regulatory action on platelet functioning, permitting formation of thrombi (15). of the brain vasculature and is responsible for regulating the flux of molecules and ions. It confers protection on the brain and helps to maintain homeostasis. RA, in pharmacologic concentrations, is capable of inducing tight junction expression in endothelial cells of the human brain, producing pluripotent stem cells and stimulating the RXR pathway (16,17). Vitamin A and the Blood-Brain Barrier Vitamin A and the Endocrine System RA may also play a physiologic role in the development of the blood-brain barrier. This barrier represents multiple properties VA is not regulated by the endocrine system, but it plays crucial roles in many endocrine activities, as discussed in the following sections. 53 Effects of Retinoids at the Systemic Level Pancreas Retinol dehydrogenase enzyme (RDH10) is necessary for the production of RA in the embryo, and it is vital for pancreas and endocrine cell differentiation. Modifications in the action of RDH10 has been shown to result in a smaller pancreas with reduced α and β cells, leading to a reduction in the body weight, hypoglycemia, and increased mortality. The effects on the pancreatic cells indicate that this enzyme could be part of the terminal differentiation of endocrine cells (18). ATRA also influences insulin liberation during acute exposure, probably via a non-genomic pathway (i.e., activation of tyrosine kinases) that is independent of transcriptional regulation stimulated by nuclear RAR (19). In β cells, ATRA augments the transcription of pre-proinsulin genes, glucokinase, and GLUT-2, as well as inducing the secretion of insulin (Figure 9.1) (20). VA, Hypothalamus, and Thyroid The hypothalamus, as well as the pituitary and peripheral glands, possess enzymes that participate in RA metabolism and present RAR- and RARE-bearing genes, indicating that they interfere in the function of these tissues (20). RA seems to be related to the maintenance of the thyroid cells, but it is not related to the organogenesis of this gland. A scarcity of VA may lead to thyroid hypertrophy, and profoundly modifies its metabolism. In humans, lower RA levels create higher thyroid-stimulating hormone (TSH) and thyroxine (T4) levels, and thyroid volume (Figure 9.1) (21). ATRA may also reduce iodine uptake, but an isomer, 13-cis RA, augmented iodine uptake, indicating that the different isomers may exert antagonist effects on thyrocyte functions. Another effect of RA is its potential therapeutic approach in thyroid cancer due to its ability to balance cell differentiation or to reverse this differentiation in some models of cancer (22). VA and the Hypothalamo–Pituitary– Adrenal (HPA) Axis and Gonads The enzymes that participate in RA metabolism and RA itself are found in the hypothalamic neurons, suggesting it may influence the functions of the hypothalamus. Additionally, it may regulate the secretion of the basal levels of corticosterone (20). RA may decrease the expression of glucocorticoid receptors, modify the signaling of glucocorticoid in a neuronal model, and modulate the HPA axis activity. It may play a role in the creation of pituitary and adrenal tumors (23). The formation of the gonads requires the presence of RA for maintenance of fertility. It stimulates the production of gonadal hormones and estrogen, and in breast cancer cells, plays opposite roles on cell proliferation (24). Conclusions Studies have shown that VA and its metabolites, such as ATRA and 9-cis RA, are involved in a plethora of mechanisms related to the regulation of the immune system and heart protection, as well as maintenance and organogenesis of the thyroid cells, β-cell function, and secretion of insulin. For these reasons it is crucial for the maintenance of homeostasis of several processes at a systemic level, suggesting its potential in the prevention and treatment of different pathologies. REFERENCES 1. Giordano E, Quadro L. Lutein, zeaxanthin, and mammalian development: Metabolism, functions, and implications for health. Arch Biochem Biophys. 2018;647:33–40. 2. Zuma MK, Kolanisi U, Modi AT. The potential of integrating provitamin A-biofortified maize in smallholder farming systems to reduce malnourishment in South Africa. Int J Environ Res Public Health. 2018;15(4). pii:E805. 3. Bando Y, Yamamoto M, Sakiyama K, Sakashita H, Taira F, Miyake G, Iseki S, Owada Y, Amano O. Retinoic acid regulates cell-shape and the death of E-FABP (FABP5)immunoreactive septoclasts in the growth plate cartilage of mice. Histochem Cell Biol. 2017;148:229–238. 4. Watson J, Lee M, Garcia-Casal MN. Consequences of inadequate intakes of vitamin A, vitamin B12, vitamin D, calcium, iron, and folate in older persons. Curr Geriatr Rep. 2018;7:103–113. 5. Chen J, Cao X, An Q et al. Inhibition of cancer stem cell like cells by a synthetic retinoid. Nat Commun. 2018;11(9):1406. 6. Hufnagl K, Jensen-Jarolim E. Vitamin A and D in allergy: From experimental animal models and cellular studies to human disease. Allergo J Int. 2018;27:72–78. 7. Liu ZM, Wang KP, Ma J, Guo Zheng S. The role of all-trans retinoic acid in the biology of Foxp3+ regulatory T cells. Cell Mol Immunol. 2015;12:553–557. 8. Raverdeau M, Mills KHG. Modulation of T cell and innate immune responses by retinoic acid. J Immunol. 2014;192:2953–2958. 9. Larange A, Cheroutre H. Retinoic acid and retinoic acid receptors as pleiotropic modulators of the immune system. Annu Rev Immunol. 2016;34:369–394. 10. Pan J, Baker KM. Retinoic acid and the heart. Vitam Horm. 2007;75:257–283. 11. Bilbija D, Haugen F, Sagave J, Baysa A, Bastani N, Levy FO, Sirsjö A, Blomhoff R, Valen G. Retinoic acid signalling is activated in the postischemic heart and may influence remodelling. PLOS ONE. 2012;7:e44740. 12. Silva RAC, Gonçalves AF, Dos Santos PP, Rafacho B, Claro RFT, Minicucci MF, Azevedo PS, Polegato BF, Zanati SG, Fernandes AA, Paiva SAR, Zornoff LAM. Cardiac remodeling induced by all-trans retinoic acid is detrimental in normal rats. Cell Physiol Biochem. 2017;4:1449–1459. 13. Choudhary R, Palm-Leis A, Scott RC, Guleria RS, Rachut E, Baker KM, Pan J. All-trans retinoic acid prevents development of cardiac remodeling in aortic banded rats by inhibiting the renin-angiotensin system. Am J Physiol Heart Circ Physiol. 2008;294:H633–H644. 14. Dechow C, Morath C, Peters J, Lehrke I, Waldherr R, Haxsen V, Ritz E, Wagner, J. Effects of all-trans retinoic acid on renin-angiotensin system in rats with experimental nephritis. Am J Physiol Renal Physiol. 2001;281:F909–F919. 15. Unsworth AJ, Flora GD, Sasikumar P, Bye AP, Sage T, Kriek N, Crescente M, Gibbins JM. RXR ligands negatively regulate thrombosis and hemostasis. Arterioscler Thromb Vasc Biol. 2017;37:812–822. 54 16. Mizee MR, Wooldrik D, Lakeman KA, van het Hof B, Drexhage JA, Geerts D, Bugiani M et al. Retinoic acid induces blood-brain barrier development. J Neurosci. 2013;33:1660–1671. 17. Bonney S, Siegenthaler JA. Differential effects of retinoic acid concentrations in regulating blood-brain barrier properties. eNeuro. 2017;4(3). doi:10.1523/ENEURO.0378-16.2017. 18. Arregi I, Climent M, Iliev D, Strasser J, Gouignard N, Johansson JK, Singh T et al. Retinol dehydrogenase-10 regulates pancreas organogenesis and endocrine cell differentiation via paracrine retinoic acid signaling. Endocrinology. 2016;157:4615–4631. 19. Amisten S, Mohammad Al-Amily I, Soni A, Hawkes R, Atanes P, Persaud SJ, Rorsman P, Salehi A. Anti-diabetic action of all-trans retinoic acid and the orphan G protein coupled receptor GPRC5C in pancreatic β-cells. Endocr J. 2017;64:325–338. Retinoids in Dermatology 20. Brossaud J, Pallet V, Corcuff JB. Vitamin A, endocrine tissues and hormones: Interplay and interactions. Endocr Connect. 2017;6:R121–R130. 21. Zimmermann MB, Wegmuller R, Zeder C, Chaouki N, Torresani T. The effects of vitamin A deficiency and vitamin A supplementation on thyroid function in goitrous children. J Clin Endocrinol Metabol. 2004;89:5441–5447. 22. Kogai T, Taki K, Brent GA. Enhancement of sodium/iodide symporter expression in thyroid and breast cancer. Endoc Relat Cancer. 2006;13:797–826. 23. Marissal-Arvy N, Hamiani R, Richard E, Moisan MP, Pallet V. Vitamin A regulates hypothalamic-pituitary-adrenal axis status in LOU/C rats. J Endocrinol. 2013;219:21–27. 24. Ombra MN, Di Santi A, Abbondanza C, Migliaccio A, Avvedimento EV, Perillo B. Retinoic acid impairs estrogen signaling in breast cancer cells by interfering with activation of LSD1 via PKA. Biochim Biophys Acta. 2013;1829:480–486. 10 New Aspects of Isotretinoin Teratogenicity Bodo C. Melnik Introduction Teratogenicity is the most severe side effect of oral retinoids, affecting 1 in 57 women ingesting over 10,000 IUs daily of preformed vitamin A (1). Isotretinoin (13-cis retinoic acid), the most effective drug for the treatment of severe nodulocystic acne (2), is a well-known teratogen (3) associated with an estimated 25-fold increase of the risk of malformation (4). The majority of malformations induced by isotretinoin treatment during pregnancy primarily affect neural crest cells (NCCs), leading to craniofacial dysmorphic features involving facial, thymic, cardiac, and central nervous system structures (4–10). Initiation of craniofacial morphogenesis is marked by the appearance of the paired pharyngeal arches. The first pair is divided into mandibular and maxillary prominences, which together with the frontonasal prominence constitute the five facial primordia. The neural crest arises from the embryonic ectoderm and develops from the neural tube after its closure (11). The neural crest is a stem/progenitor cell population that contributes to a wide variety of derivatives, including sensory and autonomic ganglia, cartilage and bone of the face, and pigment cells of the skin (12). Cranial NCCs are stem cell-line cells, which delaminate from the dorsal edge of the developing brain and drive the budding of the five primordia (13–15). In NCCs, NCC-derived neuroblastoma cells as well as sebocytes, isotretinoin is intracellularly isomerized to all-trans-retinoic acid (ATRA) (4,8,16,17). Pigtail monkeys exposed to ATRA during gestation exhibit craniofacial dysmorphic features as seen in human during gestational isotretinoin exposure (18,19). During craniofacial development, massive cell death occurs in vertebrates (20). In the developing nervous system, a well-regulated balance of apoptotic signaling ensures appropriate cell differentiation and maturation (21,22). Neural crest apoptosis is of critical importance for craniofacial patterning (23,24). Bone morphogenetic protein (BMP-4) is a member of the transforming growth factor (TGF-β) family and is involved in various functions, including apoptosis during neural ectoderm development. BMP-4 plays a key role in the regulation of neural crest morphogenetic cell death (23). BMP-4 induces apoptosis in a p53-dependent manner (25,26). Augmented BMP signaling in the neural crest inhibited nasal cartilage morphogenesis by inducing p53-mediated apoptosis (27). Isotretinoin-treated NCCs often became rounded or spindle-shaped, separated from their neighbors, and frequently detached from the substrate or clumped together (28). Animal studies have confirmed that administration of isotretinoin increases apoptosis of NCCs (29–31). It has recently been suggested that isotretinoin’s major desired and adverse drug effects including teratogenicity are related to apoptosis, such as sebocyte and NCC apoptosis, respectively (32,33). There is accumulating evidence for isotretinoin-mediated overexpression of p53 (34). Isotretinoin-Induced p53 and Apoptosis In sebocytes, increased expression of the pro-apoptotic proteins tumor necrosis factor-related apoptosis-inducing ligand (TRAIL), TRAIL-receptor 1 (DR4), and insulin-like growth factor-binding protein 3 (IGFBP3) have been related to ­isotretinoin-mediated sebocyte apoptosis (32,35). TRAIL-receptor 1 expression is upregulated by ATRA (36). Increased expression of pro-apoptotic IGF binding protein 3 (IGFBP3) has been reported in ATRA-treated NCCs (37). p53 upregulates the expression of TRAIL, TRAIL-receptor 1 (DR4), TRAIL-receptor 2 (DR5), and IGFBP3, respectively (38–42). ATRA functions as a potent inducer of p53 in keratinocytes, glioma, and melanoma cells. (43–45). In HepG2 cells, ATRA induces p53-dependent apoptosis via upregulation of p14 (ARF) (46). Increased binding of p14 to mouse double minute 2 (MDM2), the E3 ubiquitin ligase that inactivates p53 via proteasomal degradation, inhibits the action of MDM2 and thus enhances cellular p53 levels (46). In human primary keratinocytes, isotretinoin increased the expression of p53 (47). p53 also stimulates the expression of Bax, thereby promoting the mitochondrial pathway of apoptosis (48). Thus, translational and posttranslational effects of isotretinoin/ATRA increase p53 signaling, which induces p53-mediated extrinsic and intrinsic pathways of apoptosis (Figure 10.1). The Role of p53 in Neural Crest Cell Homeostasis In the mouse, p53 knockout embryos displayed broad craniofacial defects in skeletal, neuronal, and muscle tissues. In the chick, p53 is expressed in cranial neural crest (CNC) progenitors, and its expression decreases with their delamination from the neural tube. Stabilization of p53 protein using a pharmacologic inhibitor of its negative regulator, MDM2, resulted in fewer migrating CNC cells and in craniofacial defects (49). Isotretinoin alters the expression of the transcription factors PAX-2 and KROX-20 in macaque embryo NCCs (50). Notably, the expression pattern of 55 56 Retinoids in Dermatology FIGURE 10.1 Isotretinoin-p53-mediated apoptosis of neural crest cells, the molecular basis for isotretinoin’s teratogenicity. Isotretinoin (13-cis retinoic acid) intracellularly isomerizes to all-trans-retinoic acid (ATRA), which activates retinoic acid receptor (RAR)-mediated expression of p53 and HOX transcription factors. RAR as well as HOX activate the TP53 promoter. p53 promotes the expression of tumor necrosis factor-related apoptosis-inducing ligand (TRAIL), death receptors (DR4/5), and Bax thereby stimulates the extrinsic and intrinsic pathway of apoptosis resulting in activation of caspase 3. In addition, p53 attenuates pro-survival signaling via suppression of insulin-like growth factor 1 receptor (IGF1R), mechanistic target of rapamycin complex 1 (mTORC1), sterol regulatory element-binding protein 1 (SREBP1) as well as survivin, a key negative regulator of caspase 3. p53 induces the expression of FoxO1, FoxO3a, phosphatase and tensin (PTEN) homolog, IGF binding protein 3 (IGFBP3), and sestrins, which activate AMP-activated protein kinase, the key negative regulator of mTORC1. Thus, ATRA-induced overexpression of p53 attenuates pro-survival signaling and promotes pro-apoptotic signaling. Increased p53-dependent neural crest cell apoptosis during embryogenesis explains isotretinoin’s teratogenicity. PAX-2 is maintained after isotretinoin treatment. PAX-2 positive NCCs migrating to the second pharyngeal arch are substantially reduced in numbers in treated embryos (50). Alteration in the otic anlage included delayed invagination, abnormal relationship with the adjacent hindbrain epithelium, and altered expression boundaries for PAX-2. Isotretinoin-associated changes in the pharyngeal arch region included truncation of the distal portion of the first arch and reduction in the size of the second arch. These alterations in hindbrain, neural crest, otic anlage, and pharyngeal arch morphogenesis contribute to the craniofacial malformations in the macaque fetus exposed to isotretinoin (50). Remarkably, PAX2 has been identified as a target gene of p53 (51); thus, isotretinoin-mediated upregulation of p53 and PAX-2 may explain the NCC abnormalities reported in isotretinoin exposed macaque embryos. Hox genes play an important part in the patterning of limbs, vertebrae, and craniofacial structures by providing an ordered molecular system of positional values, termed the Hox code. ATRA alters hindbrain Hox code and induces transformation of rhombomeres 2/3 into a 4/5 identity (51). HOX transcription factors, which are induced by ATRA (52–54), play a crucial role in NCC-dependent branchial arch pattering (55–58). ATRA induces Hox gene expression, a regulatory mechanism related to ATRA’s teratogenic activity (53). Intriguingly, HOX binding sites have been identified on the TP53 promoter and compromised HOXA5 function limited p53 expression (59). As a result, ATRAinduced HOX gene expression may further enhance p53 expression, explaining the interplay between ATRA, HOX, and p53 in isotretinoin teratogenicity (Figure 10.1). Isotretinoin-stimulated overactivation of p53-mediated apoptosis of NCCs may represent the molecular basis for craniofacial abnormalities associated with isotretinoin embryopathy. Isotretinoin Embryopathy Resembles Craniofacial Abnormalities Associated with Increased p53 Expression Treacher Collins syndrome (TCS), CHARGE (coloboma of the eye, heart defects, atresia of the choanae, retardation of growth/ or development, genital and/or urinary abnormalities, ear abnormalities and deafness) syndrome, DiGeorge syndrome, and fetal alcohol syndrome resemble retinoid embryopathy and share intriguing overlapping of craniofacial abnormalities (Table 10.1) (60–70). Abnormalities of the secondary palate were studied in an animal model in which features of TCS were induced by acute maternal exposure to isotretinoin (71). TCS is a congenital disorder of craniofacial development arising from mutations in TCOF1 gene, which encodes the nucleolar phosphoprotein Treacle. TCOF1-related molecular networks in TCS involve p53 (72). Haploinsufficiency of TCOF1 perturbs mature ribosome biogenesis, resulting in stabilization of p53 and cyclin G1-mediated cell-cycle arrest that underpins the specificity of neuroepithelial apoptosis and NCC hypoplasia characteristic of TCS (73,74). In an animal study, inhibition of p53-­dependent apoptosis restored NCCs and prevented TCS craniofacial anomalies (75). 57 New Aspects of Isotretinoin Teratogenicity TABLE 10.1 Overlapping Clinical Features of Isotretinoin Embryopathy, Treacher Collins Syndrome, CHARGE Syndrome, DiGeorge Syndrome, Fetal Alcohol Spectrum Disorders, and Mutant Hyperactive p53 Mouse Phenotypic Features Isotretinoin Heart defects Ear defects/deafness Cleft palate Mandibular hypoplasia Thymus aplasia/hypoplasia Bone/cartilage defects Overactivated p53 + + + + + + Predicted TCS CHARGE DiGeorge FASD p53* Mouse + + + + + + + + + + + + + + + + + TBX1-p53 (+) + (+) + + + + + + + + + + + + + TCS, Treacher Collins syndrome; CHARGE, coloboma of the eye, heart defects, atresia of the choanae, retardation of growth/or developAbbreviations: ment, genital and/or urinary abnormalities, ear abnormalities and deafness syndrome; DiGeorge, DiGeorge syndrome; FASD, fetal alcohol spectrum disorders; p53*, mutant hyperactive p53 mouse. Overactivation of p53 induces features of CHARGE syndrome exhibiting loss-of-function gene mutations of the chromatin remodeling protein CHD7 (76) that is necessary for proper craniofacial development (77). CHD7 binding to the TP53 promoter suppresses p53 expression. CHD7 loss in mouse NCC or samples from patients with CHARGE syndrome results in p53 activation (78). Overactivated mutant p53 during murine embryogenesis triggered cell-cycle arrest and apoptosis causing CHARGE phenotypes (76). Apoptosis also underlies ethanol-induced craniofacial malformations (79). Ethanol exposure causes increased mRNA levels of p53 in both cranial and trunk NCCs (80). Upregulation of Siah1 by ethanol triggers apoptosis in NCCs through p38 MAPKmediated activation of p53 (81). Alcohol exposure negatively affects NCC development in the chick, associated with increased expression of BMP-4 (82), a known suppressor of p53 (20,21). DiGeorge syndrome, a 22q11.2 deletion syndrome, is another neurocristopathy resembling retinoid embryopathy (83). The most studied gene of interest in the 22q11.2 deletion region is TBX1, encoding a T-box transcription factor (83). Tbx1-/- mice had a high incidence of cardiac outflow tract anomalies, hypoplasia of the thymus and parathyroid glands, abnormal facial structures, abnormal vertebrae, and cleft palate, leading to the conclusion that Tbx1 in humans is a key gene in the etiology of DiGeorge syndrome (84–86). Tbx1 controls cardiac NCC migration during arch artery development by regulating GBX2 expression in the pharyngeal ectoderm (87). Tbx1 haploinsufficiency in the DiGeorge syndrome region causes aortic arch defects in mice (86). In accordance, half dosage of this gene in humans causes most of the features of the DiGeorge or velocardiofacial syndrome phenotypes, including aortic arch and cardiac outflow tract abnormalities (88). Recently, a strong genetic interaction between Tbx1 and p53 has been found. Intriguingly, genetic ablation of TP53, or pharmacological inhibition of p53, rescues significantly the cardiovascular defects of Tbx1 heterozygous and hypomorphic mutants (88). As a result, disturbed Tbx1-p53 signaling is involved in the pathogenesis of DiGeorge syndrome. p53 plays a key role for NCC development in the zebra fish (89). The zebra fish eif3ba mutant exhibits a hypogenesis of cranial NCCs associated with marked upregulation p53 and pronounced apoptosis in the cranial area (89). p53 hyperactivity has recently been related to defective craniofacial development in NCC-mTOR knockout mice (90). Overactivation of p53 is the underlying mechanism for exaggerated NCC apoptosis promoting dysmorphic craniofacial features in humans and experimental animal models, which all exhibit overlapping clinical features of isotretinoin embryopathy associated with a hyperactive state of p53 (Table 10.1). Conclusions Translational and clinical evidence derived from human neurocristopathies and mouse models, as well as developmental studies in the zebra fish, allow the conclusion that hyperactivation of p53 is the mechanistic converging point that exaggerates NCC apoptosis causing craniofacial abnormalities closely resembling isotretinoin embryopathy. The teratogenicity of isotretinoin can be regarded as the result of upregulated p53 signaling in NCCs, promoting inappropriate excessive NCC apoptosis during embryogenesis. REFERENCES 1. Hunt JR. Teratogenicity of high vitamin A intake. N Engl J Med. 1996;334:1197. 2. Peck GL, Olsen TG, Yoder FW et al. Prolonged remissions of cystic and conglobate acne with 13-cis-retinoic acid. N Engl J Med. 1979;300:329–333. 3. Nau H. Teratogenicity of isotretinoin revisited: Species variation and the role of all-trans-retinoic acid. J Am Acad Dermatol. 2001;45:183–187. 4. Lammer EJ, Chen DT, Hoar RM et al. Retinoic acid embryopathy. N Engl J Med. 1985;313:837–841. 5. Fernhoff PM, Lammer EJ. Craniofacial features of isotretinoin embryopathy. J Pediatr. 1984;105:595–597. 6. Rappaport EB, Knapp M. Isotretinoin embryopathy—a continuing problem. J Clin Pharmacol. 1989;29:463–465. 7. Lynberg MC, Khoury MJ, Lammer EJ et al. Sensitivity, specificity, and positive predictive value of multiple malformations in isotretinoin embryopathy surveillance. Teratology. 1990;42:513–519. 8. Coberly S, Lammer E, Alashari M. Retinoic acid embryopathy: Case report and review of literature. Pediatr Pathol Lab Med. 1996;16:823–836. 9. Centers for Disease Control and Prevention (CDC). Accutaneexposed pregnancies—California, 1999. MMWR Morb Mortal Wkly Rep. 2000;49:28–31. 58 10. Holst H, Muhari-Stark E, Lava SA. Teratogenicity of systemic isotretinoin. Minerva Pediatr. 2018;70:107–109. 11. Simões-Costa M, Bronner ME. Insights into neural crest development and evolution from genomic analysis. Genome Res. 2013;23:1069–1080. 12. Simões-Costa M, Bronner ME. Establishing neural crest identity: A gene regulatory recipe. Development. 2015;142:242–257. 13. Achilleos A, Trainor PA. Neural crest stem cells: Discovery, properties and potential for therapy. Cell Res. 2012;22:288–304. 14. Bronner ME, Simões-Costa M. The neural crest migrating into the twenty-first century. Curr Top Dev Biol. 2016;116:115–134. 15. Mayor R, Theveneau E. The neural crest. Development. 2013;140:2247–2251. 16. Veal G, Rowbotham S, Boddy A. Pharmacokinetics and pharmacogenetics of 13-cis-retinoic acid in the treatment of neuroblastoma. Therapie. 2007;62:91–93. 17. Tsukada M, Schröder M, Roos TC et al. 13-cis retinoic acid exerts its specific activity on human sebocytes through selective intracellular isomerization to all-trans retinoic acid and binding to retinoid acid receptors. J Invest Dermatol. 2000;115:321–327. 18. Newell-Morris L, Sirianni JE, Shepard TH et al. Teratogenic effects of retinoic acid in pigtail monkeys (Macaca nemestrina). II. Craniofacial features. Teratology. 1980;22:87–101. 19. Yip JE, Kokich VG, Shepard TH. The effect of high doses of retinoic acid on prenatal craniofacial development in Macaca nemestrina. Teratology. 1980;21:29–38. 20. Shuler CF. Programmed cell death and cell transformation in craniofacial development. Crit Rev Oral Biol Med. 1995;6:202–217. 21. Miura M. Apoptotic and non-apoptotic caspase functions in neural development. Neurochem Res. 2011;36:1253–1260. 22. Yamaguchi Y, Miura M. Programmed cell death in neurodevelopment. Dev Cell. 2015;32:478–490. 23. Graham A, Koentges G, Lumsden A. Neural crest apoptosis and the establishment of craniofacial pattern: An honorable death. Mol Cell Neurosci. 1996;8:76–83. 24. Graf D, Malik Z, Hayano S, Mishina Y. Common mechanisms in development and disease: BMP signaling in craniofacial development. Cytokine Growth Factor Rev. 2016;27:129–139. 25. Fukuda N, Saitoh M, Kobayashi N, Miyazono K. Execution of BMP-4-induced apoptosis by p53-dependent ER dysfunction in myeloma and B-cell hybridoma cells. Oncogene. 2006;25:3509–3517. 26. Kim SG, Chae CH, Cho BO et al. Apoptosis of oral epithelial cells in oral lichen planus caused by upregulation of BMP-4. J Oral Pathol Med. 2006;35:37–45. 27. Hayano S, Komatsu Y, Pan H, Mishina Y. Augmented BMP signaling in the neural crest inhibits nasal cartilage morphogenesis by inducing p53-mediated apoptosis. Development. 2015;142:1357–1367. 28. Smith-Thomas L, Lott I, Bronner-Fraser M. Effects of isotretinoin on the behavior of neural crest cells in vitro. Dev Biol. 1987;123:276–281. 29. Johnston MC, Bronsky PT. Animal models for human craniofacial malformations. J Craniofac Genet Dev Biol. 1991;11:277–291. 30. Watanabe T, Goulding EH, Pratt RM. Alterations in craniofacial growth induced by isotretinoin (13-cis-retinoic acid) in mouse whole embryo and primary mesenchymal cell culture. J Craniofac Genet Dev Biol. 1988;8:21–33. Retinoids in Dermatology 31. Lammer EJ, Armstrong DL. Malformations in hindbrain structures among humans exposed to isotretinoin (13-cis-retinoic acid) during early embryogenesis. In: Morriss-Kay G, editor. Retinoids in Normal Development and Teratogenesis. New York: Oxford University Press, 1991; pp. 281–295. 32. Nelson AM, Cong Z, Gilliland KL, Thiboutot DM. TRAIL contributes to the apoptotic effect of 13-cis retinoic acid in human sebaceous gland cells. Br J Dermatol. 2011;165:526–533. 33. Melnik BC. Apoptosis may explain the pharmacological mode of action and adverse effects of isotretinoin, including teratogenicity. Acta Derm Venereol. 2017;97:173–181. 34. Melnik BC. Overexpression of p53 explains isotretinoin’s teratogenicity. Exp Dermatol. 2018;27:91–93. 35. Nelson AM, Zhao W, Gilliland KL et al. Neutrophil gelatinase-associated lipocalin mediates 13-cis retinoic acid-induced apoptosis of human sebaceous gland cells. J Clin Invest. 2008;118:1468–1478. 36. Dhandapani L, Yue P, Ramalingam SS et al. Retinoic acid enhances TRAIL-induced apoptosis in cancer cells by upregulating TRAIL receptor 1 expression. Cancer Res. 2011;71:5245–5254. 37. Williams SS, Mear JP, Liang HC et al. Large-scale reprogramming of cranial neural crest gene expression by retinoic acid exposure. Physiol Genomics. 2004;19:184–197. 38. Kuribayashi K, Krigsfeld G, Wang W et al. TNFSF10 (TRAIL), a p53 target gene that mediates p53-dependent cell death. Cancer Biol Ther. 2008;7:2034–2038. 39. Buckbinder L, Talbott R, Velasco-Miguel S et al. Induction of the growth inhibitor IGF-binding protein 3 by p53. Nature. 1995;377:646–649. 40. Bertherat J. Insulin-like growth factor binding protein 3 (IGFBP-3): A novel target of the tumor suppressor p53 inhibiting cell growth. Eur J Endocrinol. 1996;134:426–427. 41. Liu X, Yue P, Khuri FR, Sun SY. p53 upregulates death receptor 4 expression through an intronic p53 binding site. Cancer Res. 2004;64:5078–5083. 42. Pappas K, Xu J, Zairis S et al. p53 maintains baseline expression of multiple tumor suppressor genes. Mol Cancer Res. 2017;15:1051–1062. 43. Mrass P, Rendl M, Mildner M et al. Retinoic acid increases the expression of p53 and proapoptotic caspases and sensitizes keratinocytes to apoptosis: A possible explanation for tumor preventive action of retinoids. Cancer Res. 2004;64:6542–6548. 44. Lu J, Zhang F, Yuan Y et al. All-trans retinoic acid upregulates the expression of p53 via Axin and inhibits the proliferation of glioma cells. Oncol Rep. 2013;29:2269–2274. 45. Guruvayoorappan C, Pradeep CR, Kuttan G. 13-cis-retinoic acid induces apoptosis by modulating caspase-3, bcl-2, and p53 gene expression and regulates the activation of transcription factors in B16F-10 melanoma cells. J Environ Pathol Toxicol Oncol. 2008;27:197–207. 46. Heo SH, Kwak J, Jang KL. All-trans retinoic acid induces p53-depenent apoptosis in human hepatocytes by activating p14 expression via promoter hypomethylation. Cancer Lett. 2015;362:139–148. 47. Shi G, Liao PY, Cai XL et al. FoxO1 enhances differentiation and apoptosis in human primary keratinocytes. Exp Dermatol. 2018;27:1254–1260. 48. Miyashita T, Reed JC. Tumor suppressor p53 is a direct transcriptional activator of the human bax gene. Cell. 1995;80:293–299. 59 New Aspects of Isotretinoin Teratogenicity 49. Rinon A, Molchadsky A, Nathan E et al. p53 coordinates cranial neural crest cell growth and epithelial-mesenchymal transition/ delamination processes. Development. 2011;138:1827–1838. 50. Makori N, Peterson PE, Wei X et al. 13-cis-Retinoic acid alters neural crest cells expressing Krox-20 and Pax-2 in macaque embryos. Anat Rec. 1999;255:142–154. 51. Saifudeen Z, Liu J, Dipp S et al. A p53-Pax2 pathway in kidney development: Implications for nephrogenesis. PLOS ONE. 2012;7:e44869. 52. Marshall H, Nonchev S, Sham MH et al. Retinoic acid alters hindbrain Hox code and induces transformation of rhombomeres 2/3 into a 4/5 identity. Nature. 1992;360:737–741. 53. Whiting J. Craniofacial abnormalities induced by the ectopic expression of homeobox genes. Mutat Res. 1997;396:97–112. 54. Huang M, Miller ML, McHenry LK et al. Generating trunk neural crest from human pluripotent stem cells. Sci Rep. 2016;6:19727. 55. Hunt P, Whiting J, Muchamore I et al. Homeobox genes and models for patterning the hindbrain and branchial arches. Dev Suppl. 1991;1:187–196. 56. Trainor PA, Krumlauf R. Hox genes, neural crest cells and branchial arch patterning. Curr Opin Cell Biol. 2001;13:698–705. 57. Vieux-Rochas M, Mascrez B, Krumlauf R, Duboule D. Combined function of HoxA and HoxB clusters in neural crest cells. Dev Biol. 2013;382:293–301. 58. Kam MK, Lui VC. Roles of Hoxb5 in the development of vagal and trunk neural crest cells. Dev Growth Differ. 2015;57:158–168. 59. Raman V, Martensen SA, Reisman D et al. Compromised HOXA5 function can limit p53 expression in human breast tumours. Nature. 2000;405:974–978. 60. Sulik KK, Johnston MC, Smiley SJ et al. Mandibulofacial dysostosis (Treacher Collins syndrome): A new proposal for its pathogenesis. Am J Med Genet. 1987;27:359–372. 61. Dixon MJ. Treacher Collins syndrome. Hum Mol Genet. 1996;5:1391–1396. 62. Marszałek B, Wójcicki P, Kobus K, Trzeciak WH. Clinical features, treatment and genetic background of Treacher Collins syndrome. J Appl Genet. 2002;43:223–233. 63. Trainor PA, Dixon J, Dixon MJ. Treacher Collins syndrome: Etiology, pathogenesis and prevention. Eur J Hum Genet. 2009;17:275–283. 64. Dixon J, Brakebusch C, Fässler R, Dixon MJ. Increased levels of apoptosis in the prefusion neural folds underlie the craniofacial disorder, Treacher Collins syndrome. Hum Mol Genet. 2000;9:1473–1480. 65. Bergman JE, Janssen N, Hoefsloot LH et al. CHD7 mutations and CHARGE syndrome: The clinical implications of an expanding phenotype. J Med Genet. 2011;48:334–342. 66. Hsu P, Ma A, Wilson M et al. CHARGE syndrome: A review. J Paediatr Child Health. 2014;50:504–511. 67. Wong MT, Schölvinck EH, Lambeck AJ, van RavenswaaijArts CM. CHARGE syndrome: A review of the immunological aspects. Eur J Hum Genet. 2015;23:1451–1459. 68. Sulik KK, Cook CS, Webster WS. Teratogens and craniofacial malformations: Relationships to cell death. Development. 1988;103:213–231. 69. Webster WS, Ritchie HE. Teratogenic effects of alcohol and isotretinoin on craniofacial development: An analysis of animal models. J Craniofac Genet Dev Biol. 1991;11:296–302. 70. Cartwright MM, Smith SM. Stage-dependent effects of ethanol on cranial neural crest cell development: Partial basis for 71. 72. 73. 74. 75. 76. 77. 78. 79. 80. 81. 82. 83. 84. 85. 86. 87. 88. 89. 90. the phenotypic variations observed in fetal alcohol syndrome. Alcohol Clin Exp Res. 1995;19:1454–1462. Sulik KK, Smiley SJ, Turvey TA et al. Pathogenesis of cleft palate in Treacher Collins, Nager, and Miller syndromes. Cleft Palate J. 1989;26:209–216. Dai J, Si J, Wang M et al. Tcof1-related molecular networks in Treacher Collins syndrome. J Craniofac Surg. 2016;27:1420–1426. Fumagalli S, Thomas G. The role of p53 in ribosomopathies. Semin Hematol. 2011; 8:97–105. Laue K, Pogoda HM, Daniel PB et al. Craniosynostosis and multiple skeletal anomalies in humans and zebrafish result from a defect in the localized degradation of retinoic acid. Am J Hum Genet. 2011;89:595–606. Jones NC, Lynn ML, Gaudenz K et al. Prevention of the neurocristopathy Treacher Collins syndrome through inhibition of p53 function. Nat Med. 2008;14:125–133. Van Nostrand JL, Brady CA, Jung H et al. Inappropriate p53 activation during development induces features of CHARGE syndrome. Nature. 2014;514:228–232. Sperry ED, Hurd EA, Durham MA et al. The chromatin remodeling protein CHD7, mutated in CHARGE syndrome, is necessary for proper craniofacial and tracheal development. Dev Dyn. 2014;243:1055–1066. Van Nostrand JL, Attardi LD. Guilty as CHARGED: p53’s expanding role in disease. Cell Cycle. 2014;13:3798–3807. Sulik KK. Genesis of alcohol-induced craniofacial dysmorphism. Exp Biol Med (Maywood). 2005;230:366–375. Wentzel P, Eriksson UJ. Altered gene expression in neural crest cells exposed to ethanol in vitro. Brain Res. 2009;1305:50–60. Yuan F, Chen X, Liu J et al. Up-regulation of Siah1 by ethanol triggers apoptosis in neural crest cells through p38 MAPKmediated activation of p53 signaling pathway. Arch Toxicol. 2017;91:775–784. Zhang P, Wang G, Lin Z et al. Alcohol exposure induces chick craniofacial bone defects by negatively affecting cranial neural crest development. Toxicol Lett. 2017;281:53–64. McDonald-McGinn DM, Sullivan KE, Marino B et al. 22q11.2 deletion syndrome. Nat Rev Dis Primers. 2015;1:15071. Jerome LA, Papaioannou VE. DiGeorge syndrome phenotype in mice mutant for the T-box gene, Tbx1. Nat Genet. 2001;27:286–291. Merscher S, Funke B, Epstein JA et al. TBX1 is responsible for cardiovascular defects in velo-cardio-facial/DiGeorge syndrome. Cell. 2001;104:619–629. Lindsay EA, Vitelli F, Su H et al. Tbx1 haploinsufficieny in the DiGeorge syndrome region causes aortic arch defects in mice. Nature. 2001;410:97–101. Calmont A, Ivins S, Van Bueren KL et al. Tbx1 controls cardiac neural crest cell migration during arch artery development by regulating Gbx2 expression in the pharyngeal ectoderm. Development. 2009;136:3173–3183. Caprio C, Baldini A. p53 Suppression partially rescues the mutant phenotype in mouse models of DiGeorge syndrome. Proc Natl Acad Sci USA. 2014;111:13385–13390. Xia Z, Tong X, Liang F et al. Eif3ba regulates cranial neural crest development by modulating p53 in zebrafish. Dev Biol. 2013;381:83–96. Nie X, Zheng J, Ricupero CL et al. mTOR acts as a pivotal signaling hub for neural crest cells during craniofacial development. PLOS Genet. 2018;14:e1007491. 11 Mucocutaneous Side Effects Tugba Kevser Uzuncakmak and Ayse Serap Karadag Introduction Retinoids are derivates of natural and synthetic analogs of vitamin A that have a wide variety of pharmaco-physiologic effects (1). Following their first approval in the treatment of hyperkeratotic skin diseases in the 1940s, they have become major therapeutic agents for a wide spectrum of skin diseases, with good therapeutic results and minimal toxicity ratios (1– 11). With the use of such a wide spectrum, many side effects can be seen in different systems during retinoid therapies. Most of these side effects are acute, dose-dependent in incidence, with variable severity, usually well-tolerated, reversible on discontinuation of treatment, and most commonly affecting the skin and mucous membranes. The side effect profile and severity of these agents may change according to the nature of the molecule. While mucosal dryness is more common with isotretinoin use, acitretin is associated with higher incidences of alopecia and palmoplantar peeling, in addition to mucocutaneous and ocular side effects that are milder with bexarotene as compared to other retinoids (3–9). Effect of Retinoids on the Skin and Mucous Membranes The role of vitamin A on growth and differentiation of epithelial cells was first reported a century ago (2). The replacement of differentiated mature epithelium with squamous, keratinizing epithelial cells was first shown in 1925 in vitamin A−de­ficient rats (12). While the researchers observed hyperkeratosis in the skin, hyperplastic and metaplastic changes were found in the epithelia of mucous membranes in these rats. Vitamin A influences the differentiation of epithelial cells, from the normal, simple, and pseudostratified phenotype to squamous and/or metaplastic lesions. In the 1930s, phrynoderma, as a distinct form of follicular hyperkeratosis, was reported in patients who also had night blindness and xerophthalmia (2). In the 1950s, the changes from keratinized to mucus-producing tissue with treatment with retinol or retinyl acetate were observed in the epidermis. In more recent years, there has been a focus on determining the pharmaco-physiologic effects of retinoids on the skin. Side Effects of Retinoids on Skin and Mucous Membranes Dryness The most common side effect of retinoids is dryness of the skin and mucous membranes which most commonly create xerosis, cheilitis, xerophthalmia, and epistaxis (13). Dryness of skin is related to decreased sebum production, reduced stratum corneum thickness, and altered skin barrier function. This side effect may be seen with both topical (tretinoin, adapalene, tazoretene, alitretinoin, and bexarotene) and systemic retinoids (isotretinoin, acitretin, bexarotene, and alitretinoin). Topical retinoids bind to specific receptors that result in different efficacy and tolerability. For this reason, in acne treatment when there is low efficacy or severe intolerance, changing to another retinoid is useful. Side effects of topical retinoids may include xerosis, photosensitivity, erythema, and irritation that may be experienced by many patients undergoing retinoid therapy. These untoward effects may last up to 2−3 weeks, by which time the skin has adapted to the applications of the retinoid and side effects become minimized. As a rule, such cosmetic procedures as significant waxing, dermabrasion, laser surgery, or chemical peelings should be postponed for approximately 6 months following the cessation of retinoid use (14–16). The initial side effect of systemic retinoid use involves dryness and tingling that may begin within the first 7 days of treatment in 90% of patients, but it can occur at any time during treatment. They appear in an average dose of 0.2–1 mg/kg/day, increasing when used more than 0.5 mg/kg/day, but it also may arise anytime during the treatment (14). Such erythema, hemorrhagic crusting, fissuring, and cheilitis may be due to alterations of keratinocyte differentiation, promoting shedding and leading to skin thinning. In addition, a decrease in the thickness of stratum corneum may lead to poor barrier function and photosensitivity (Figure 11.1). Stomatitis, gingivitis, and gustatory impairment can occur but are extremely rare findings with retinoids. Some side effects of retinoids, such as cheilitis, may be an indication of sufficient bioavailability and even a tool for dosage adjustment (13). Barrier creams, lip balms, or topical corticosteroids may be helpful (14,17,18). Dryness of the mouth, accompanied by thirst, is another common side effect of retinoids. It affects almost 30% of patients (14). 61 62 Retinoids in Dermatology FIGURE 11.1 Erythema, fissuring, and exfoliation on lips during isotretinoin therapy. Cessation or reduction in the retinoid therapy will alleviate the complaint within a few days. Dryness of the anogenital mucosa may lead to vulvar-rectal pruritus, bleeding, and dyspareunia that may require discontinuation of the therapy. Candidal v­ aginitis has developed during acitretin therapy (19). Xerophthalmia is another dose-dependent side effect of systemic retinoids, possibly occurring in upwards of one-third of patients receiving isotretinoin (14). The condition is related to meibomian gland atrophy and dysfunction which leads to reduction in the lipid component of the cornea, with evaporation of basal tears and dry eye syndrome (20). Blepharoconjunctivitis, with varying degrees of severity, visual changes, refractive changes, abnormalities in dark adaptation, decreased accommodation, and corneal ulceration or opacity are rare complications of systemic retinoids (21,22). Dry eye syndrome is usually reversible but may persist in 1% of patients after cessation of the therapy. This will interfere with using contact lenses. Corneal opacities may develop, and they usually resolve within 6–8 weeks after cessation of therapy (14). Epistaxis is the other common side effect of retinoids and is related to dry nasal mucosa, occurring in 25%–40% of patients (23). Symptoms are usually mild and self-limiting, without requiring any additional treatment such as packing or electrocautery. Lubrication of the anterior nares may be helpful. Irritation and Irritant Dermatitis One of the most common side effects of retinoids is skin irritation, which may occur during topical or systemic retinoid therapies (24). The main pathogenic mechanisms in retinoid-induced dermatitis include (22): 1. Alteration of the expression of the toll-like receptor 2 (TLR2) 2. Reduction of the thickness of the skin by enhanced cellular turnover, which results in alteration of the skin barrier permeability 3. Alterations of desmosomes 4. Reduction of tonofilaments in the spinous layer 5. Reduction of the dermal matrix degradation FIGURE 11.2 therapy. Erythema, scaling, and xerosis on face during acitretin Clinically, retinoid-induced dermatitis is characterized by e­rythema, scaling, pruritus, burning, stinging, and dryness (Figure 11.2). It usually occurs within the first month of treatment and generally affects the face, extensor surface of the extremities, and rarely, the genital region (Figure 11.2) (25). Such dermal toxicity may become treatment-limiting due to the intense erythema, edema, and vesiculation. Adverse events are usually mild to moderate in severity and disappear, so therapy should not be discontinued (26,27). Reducing the frequency and/or amount of retinoid application will lessen or even eliminate the problem, along with the application of topical corticosteroids and moisturizers. Oral retinoids may create palmoplantar peeling, particularly with acitretin, with an incidence of 36% (14). Topical emollients are usually enough in the treatment of this side effect. Ulceration There are sporadic case reports of scrotal ulceration, associated with daily oral all-trans-retinoic acid (ATRA) administration in patients with leukemia (28). It was first reported in Japan and China, but sporadic cases have appeared elsewhere (29,30). Oral ulcerations and gastrointestinal tract ulcerations may occur with treatment using ATRA and isotretinoin (31,32). Although the onset of ulcerations may usually occur at a median of 22 days (range 17–29 days) of treatment, they may be found even in the first week of treatment (31). The probable pathogenic mechanisms are retinoid-induced activation and release of cytokines such as TNF-α, granulocyte–macrophage colony-stimulating factor, interleukins 1, 3, 6, and/or superoxide production, inhibition of epithelial cell growth, induction of apoptosis, lymphocyte migration, and immunomodulation leading to leucocyte activation and tissue damage (28). Discontinuation of the treatment may be required in these patients. Topical or systemic antibiotherapies may be beneficial in infected cutaneous ulcerations. Intraoral or peroral administration of liquid sucralfate may be beneficial in the treatment of oral and gastrointestinal ulcerations. 63 Mucocutaneous Side Effects of product, vehicle, retinoid concentration, dosage and wavelength of the light, and photoirradiation time (35,36). Photo-induced lesions may be found on the face, anterior V of the chest, nape, dorsal surface of the hands, extensor surfaces of the forearms, and anterior portion of the legs. They appear as acute dermatitis or sunburn, with erythema, edema, and blister formation in severe cases (37). Topical corticosteroids and sunblocks are helpful in the treatment. Alopecia Retinoid-induced effluvium is known to occur (38,39). Although the role of the offending retinoids is poorly understood in human in vivo studies, their role in the hair follicle cycle is better known in experimental studies with transgenic mice. The excessive expression of retinoid receptors within the basal cell layer and the outer root sheath may lead to progressive alopecia (Figures 11.4 and 11.5) (40). Delayed anagen phase via retinoic acid signal retention and increased passage to anagen from the telogen phase are the main pathogenic mechanisms (41). Increased premature catagen phase intensity has been shown to develop via significant inhibition of keratinocyte proliferation FIGURE 11.3 therapy. Erythematous pustular eruption on face during isotretinoin Bacterial Infections Retinoids may stimulate the rate of mucocutaneous Staphylococcus aureus colonization, which is unrelated to the dose of isotretinoin (Figure 11.3). Changes may be attributed to impaired skin barrier function leading to increased skin fragility, allowing S. aureus to grow, especially in patients who have an atopic predisposition. Such colonization has been reported in various mucosal surfaces and may lead to folliculitis, furunculosis, sinusitis, facial or vulval cellulitis, and even endocarditis (33,34). Such infections are usually delayed for several weeks; however, there is the occasional patient in whom S. aureus created a problem early on. FIGURE 11.4 therapy. Newly developed alopecia on eyebrows during acitretin Interaction of Retinoids with UV Radiation Retinoid associated photochemical reactions are an issue of concern in several research fields including photochemistry, spectroscopy, and photobiology (35). Such reactions may be classified as photoisomerization, photopolymerization, photooxidation, or photodegradation and may present as photoallergic, photoirritant, and phototoxic clinical responses. The knowledge about the exact mechanism is very limited; however, many patients complain about a decreased tolerance to UV radiation shortly after sun exposure during treatment with retinoids (36). Such photosensitivity is more common with isotretinoin and etretinate and probably is related to the reduction in the thickness of the stratum corneum. Also, the incidence and severity of these reactions are dependent on different factors, including the type FIGURE 11.5 Newly developed alopecic plaque on right forearm during acitretin therapy. 64 Retinoids in Dermatology and a slight stimulation of apoptosis in the matrix of anagen hair bulbs in cultured hair follicles with the exogenous retinoid intake (40). The incidence of alopecia has been observed in 15%−87.5% of patients receiving acitretin, 4%−76% of patients receiving etretinate, and 8%−10% of patients receiving isotretinoin (41). Besides their effect on the follicle cycle, retinoids may also change the hair color, including repigmentation and texture (42,43). Diffuse thinning of the hair usually occurs in patients taking isotretinoin and acitretin. These findings usually appear within the first 8 weeks of the therapy and usually heal by 8 weeks’ time after the agent is stopped. Although these manifestations are usually reversible and heal with either dose reduction or cessation of treatment, an occasional patient may have a continued hair problem (44). Nail Disorders Retinoids are one of the main agents for treating some nail disorders due to psoriasis, lichen planus, or chronic hand der­matitisinduced nail dystrophy, even though they may also induce some nail changes during therapy (45–49). The most common alterations of the nails include loss of the shiny appearance of the nails, thinning, fragility, and softening (49). These side effects are usually dose-dependent and associated with alteration of the keratinization or production process of the nail plate through influencing nail matrix function. Additional retinoid-induced changes of the nail unit are the development of excessive granulation tissue formation, redness, and swelling of the skinfold around the nail. These findings may be termed paronychia-like changes, pyogenic granuloma-like changes, and onycholysis (Figures 11.6 and 11.7) (50–52). While these alterations usually appear in the first 12 weeks of therapy with retinoids, occasionally the problems may appear 6 months after initiation of therapy or later, even after the withdrawal of FIGURE 11.7 therapy. Pyogenic granuloma-like changes during isotretinoin the drugs, as explained by the long elimination half-life of retinoids (50). These unwanted findings may be due to promotion of the early stages of wound healing, leading to the accumulation of mononuclear cells in the dermis, stimulation of collagen synthesis, and activation of angiogenic factors. Keloid Formation In several clinical trials, retinoid therapy demonstrated diminution of proliferative scars; however, there are also case reports of retinoid-induced keloid formation associated with argon laser treatment or dermabrasion of acne scar, when retinoids had not been discontinued sufficiently before the procedures (53–55). Retinoid-induced suppression of collagenase synthesis, more than that of collagen synthesis, has been demonstrated in fibroblast cultures, which may promote keloid formation in vivo (53). As normal tissue healing is observed following laser hair removal, ablative laser application, dermaroller, and microneedling during treatment with oral isotretinoin, the occurrence of hypertrophic scars or keloids in patients using oral isotretinoin is considered an individual response and may be related to the inflammatory acne process (54). Pigmentary Disorders Retinoids also play a role in the regulation of skin pigmentation, which may lead to dyschromia during isotretinoin therapy. This occurs due to decreasing pigmentation through inhibition of tyrosinase, induction of melanocyte apoptosis, and acceleration of epidermal cell turnover (55,56). Although these effects are widely used in skin lightening therapies, they may also be considered an undesirable side effect. Temporary hyper- or hypopigmentation has been reported with repeated application of tretinoin and isotretinoin (27,57). Slate-gray hyperpigmentation may also occur after UVB exposure during topical retinoid applications (37). Allergic Reactions FIGURE 11.6 Paronychia-like changes during acitretin therapy. Allergic cutaneous reactions are infrequent. Hypersensitivity adverse reactions, including urticaria, have been observed with Mucocutaneous Side Effects topical tazarotene (58), and urticaria has been reported in patients using isotretinoin (57). Anaphylactic reactions have been rarely reported with systemic retinoids and even infrequently with previous topical exposure. True contact allergy to topical tretinoin is known but rarely encountered (27). Serious cases of allergic vasculitis, often with purpura (bruises and red patches) of the extremities and extracutaneous involvement, require discontinuation of treatment. Severe allergic reactions necessitate interruption of therapy and careful monitoring (59). Rare Unwanted Mucocutaneous Effects Acne, skin nodules, maculopapular eruption, pustular eruption, serous drainage, vesicles, and bullae have been observed with patients receiving the bexarotene capsule (60). Erythema multiforme-like eruptions, sticky palms, and nodular prurigolike eruptions are known with etretinate therapy (61–63), while the list of unwanted effects is much longer for oral isotretinoin: acne fulminans, bruising, eruptive xanthomas, erythema multiforme, flushing, hirsutism, pruritus, sweating, vasculitis (including Wegener granulomatosis), and even abnormal wound healing (57). One patient with atopic dermatitis developed a herpetic paronychia while on isotretinoin therapy (64). Generally, such mucocutaneous adverse events are not lifethreatening; however, exfoliative erythroderma, occurring in one patient receiving isotretinoin, is a serious event, as is the limited association with bexarotene and acitretin. The United States Food and Drug Administration (FDA) requires the isotretinoin label to include a notice of carrying a risk for SJS/TEN (60,65,66). Conclusions Since their first use in the mid-twentieth century, topical and oral retinoids have been used with great success for treating several dermatologic disorders. Despite their great therapeutic effect, major and minor side effects may decrease the quality of life for these patients. Being aware of these adverse events and the factors that lead to them is important in order to achieve the most effective results and avoid unnecessary studies. Acknowledgment The photographs were selected from the archives of the Department of Dermatology, Istanbul Medeniyet University. REFERENCES 1. Futoryan T, Gilchrest BA. Retinoids and the skin. Nutr Rev. 1994;52:299–310. 2. Zouboulis CC. Retinoids—Which dermatological indications will benefit in the near future? Skin Pharmacol Appl Skin Physiol. 2001;14:303–315. 3. Gollnick HP, Dümmler U. Retinoids. Clin Dermatol. 1997;15:799–810. 4. Bravo BS, Azulay DR, Luiz RR et al. Oral isotretinoin in photoaging: Objective histological evidence of efficacy and durability. An Bras Dermatol. 2015;90:479–486. 65 5. Vasudevan B, Verma R, Badwal S et al. Hailey-Hailey disease with skin lesions at unusual sites and a good response to acitretin. Indian J Dermatol Venereol Leprol. 2015;81:88–91. 6. Moreno AC, Santi CG, Gabbi TV et al. IgA pemphigus: Case series with emphasis on therapeutic response. J Am Acad Dermatol. 2014;70:200–201. 7. Kang HY, Valerio L, Bahadoran P, Ortonne JP. The role of topical retinoids in the treatment of pigmentary disorders: An evidence-based review. Am J Clin Dermatol. 2009;10:251–260. 8. Hall JA, Grainger JR, Spencer SP, Belkaid Y. The role of retinoic acid in tolerance and immunity. Immunity. 2011;35:13–22. 9. Iorizzo M. Nail lichen planus closed—a possible new indication for oral alitretinoin. J Eur Acad Dermatol Venereol. 2016;30:509–510. 10. Milanesi N, D’Erme AM, Gola M. Nail improvement during alitretinoin treatment: Three case reports and review of the literature. Clin Exp Dermatol. 2015;40:533–536. 11. Nickle SB, Peterson N, Peterson M. Updated physician’s guide to the off-label uses of oral isotretinoin. J Clin Aesthet Dermatol. 2014;7:22–34. 12. Wolbach SB, Howe PR. Tissue changes following deprivation of fat soluble A vitamin. J Exp Med. 1925;42:753–777. 13. Blasiak RC, Stamey CR, Burkhart CN et al. High-dose isotretinoin treatment and the rate of retrial, relapse, and adverse effects in patients with acne vulgaris. JAMA Dermatol. 2013;149:1392–1398. 14. Shalita AR. Mucocutaneous and systemic toxicity of retinoids: Monitoring and management. Dermatologica. 1987;175:151–157. 15. Zaenglein AL, Pathy AL, Schlosser BJ et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74:945–973. 16. Nast A, Dréno B, Bettoli V et al. European evidencebased (S3) guideline for the treatment of acne­ — update 2016—short version. J Eur Acad Dermatol Venereol. 2016;30:1261–1268. 17. Mansouri P, Azizian Z, Hejazi S et al. Evaluation the efficacy of trichloroacetic acid (TCA) 33% in treatment of oral retinoidinduced cheilitis compared with placebo (Vaseline): A randomized pilot study. J Dermatolog Treat. 2018;29:694–697. 18. Goforoushan F, Azimi H, Goldust M. Efficacy of vitamin E to prevent dermal complications of isotretinoin. Pak J Biol Sci. 2013;16:548–550. 19. Sturkenboom MC, Middelbeek A, de Jong van den Berg LT et al. Vulvo-vaginal candidiasis associated with acitretin. J Clin Epidemiol. 1995;48:991–997. 20. Moy A, McNamara NA, Lin MC. Effects of isotretinoin on Meibomian glands. Optom Vis Sci. 2015;92:925–930. 21. Ellies P, Dighiero P, Legeais JM et al. Persistent corneal opacity after oral isotretinoin therapy for acne. Cornea. 2000;19:238–239. 22. Weiss J, Degnan M, Leupold R, Lumpkin LR. Bilateral corneal opacities. Occurrence in a patient treated with oral isotretinoin. Arch Dermatol. 1981;117:182–183. 23. Brecher AR, Orlow SJ. Oral retinoid therapy for dermatologic conditions in children and adolescents. J Am Acad Dermatol 2003;49:171–182. 24. Foti C, Romita P, Borghi A et al. Contact dermatitis to topical acne drugs: A review of the literature. Dermatol Ther. 2015;28:323–329. 66 25. Alli N, Yorulmaz A. An unusual side effect of isotretinoin: Retinoid dermatitis affecting external urethral meatus. Cutan Ocul Toxicol. 2015;34:176–177. 26. Panretin® (alitretinoin) gel 0.1%. https://www.accessdata.fda. gov/drugsatfda_docs/label/1999/20886lbl.pdf. 27. Retin-A (tretinoin) prescribing information. https://www. accessdata.fda.gov/drugsatfda_docs/label/2002/16921s21 s22s25lbl.pdf. 28. Lee HY, Ang AL, Lim LC et al. All-trans retinoic acidinduced scrotal ulcer in a patient with acute promyelocytic leukaemia. Clin Exp Dermatol. 2010;35:91–92. 29. Mori A, Tamura S, Katsuno T et al. Scrotal ulcer occurring in patients with acute promyelocytic leukemia during treatment with all-trans retinoic acid. Oncol Rep 1999;6:55–58. 30. Sutherland J, Kempton CL, Curry MA. Continuation of all-trans retinoic acid despite the development of scrotal ulcerations in a black male. J Oncol Pharm Pract. 2015;21:393–395. 31. Riganti J, Caviedes MP, Torre AC et al. Lingual ulceration associated with retinoic acid syndrome during treatment of acute promyelocytic leukemia. Int J Dermatol. 2014;53:912–916. 32. Tankurt E, Doğanay L, Yücetürk TE. Esophageal ulcers: A possible adverse effect of isotretinoin. Turk J Gastroenterol. 2013;24:562–563. 33. Graham ML 2nd, Corey R, Califf R, Phillips H. Isotretinoin and Staphylococcus aureus infection. A possible association. Arch Dermatol. 1986;122:815–817. 34. Boffa MJ, Dave VK. Facial cellulitis during oral isotretinoin treatment for acne. J Am Acad Dermatol. 1994;31:800–802. 35. Fu PP, Cheng SH, Coop L et al. Photoreaction, phototoxicity, and photocarcinogenicity of retinoids. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2003;21:165–197. 36. Yan J, Xia Q, Cherng SH et al. Photo-induced DNA ­damage and photocytotoxicity of retinyl palmitate and its photodecomposition products. Toxicol Ind Health. 2005; 21:167–175. 37. Lankerani L, Baron ED. Photosensitivity to exogenous agents. J Cutan Med Surg. 2004;8:424–431. 38. Patel M, Harrison S, Sinclair R. Drugs and hair loss. Dermatol Clin 2013;31:67–73. 39. Ozlu E, Karadag AS, Akdeniz N, Uzuncakmak TK. Acitretininduced alopecia areata: A case report. Cutan Ocul Toxicol. 2015;34:248–250. 40. Foitzik K, Spexard T, Nakamura M et al. Towards dissecting the pathogenesis of retinoid-induced hair loss: All-trans ­retinoic acid induces premature hair follicle regression (catagen) by upregulation of transforming growth factor-beta 2 in the dermal papilla. J Invest Dermatol. 2005;124:1119–1126. 41. İslamoğlu ZGK, Altınyazar HC. Effects of isotretinoin on the hair cycle. J Cosmet Dermatol. 2019;18:647–651. 42. Seckin D, Yildiz A. Repigmentation and curling of hair after acitretin therapy. Australas J Dermatol 2009;50:214–216. 43. Bunker CB, Maurice PD, Dowd PM. Isotretinoin and curly hair. Clin Exp Dermatol. 1990;15:143–145. 44. Charakida A, Mouser PE, Chu AC. Safety and side effects of the acne drug, oral isotretinoin. Expert Opin Drug Saf. 2004;3:119–129. Retinoids in Dermatology 45. Ricceri F, Pescitelli L, Tripo L et al. Treatment of severe nail psoriasis with acitretin: An impressive therapeutic result. Dermatol Ther. 2013;26:77–78. 46. Iorizzo M. Nail lichen planus—a possible new indication for oral alitretinoin. J Eur Acad Dermatol Venereol. 2016;30:509–510. 47. Milanesi N, D’Erme AM, Gola M. Nail improvement during alitretinoin treatment: Three case reports and review of the literature. Clin Exp Dermatol. 2015;40:533–536. 48. Piraccini BM, Iorizzo M, Tosti A. Drug-induced nail abnormalities. Am J Clin Dermatol. 2003;4:31–37. 49. Zweegers J, Bovenschen HJ. Acitretin-induced transverse leukonychia. Int J Dermatol. 2014;53:221–222. 50. Gaudiello F, Scalvenzi M, Gallo L, Balato N. Excess granulation tissue and hair loss following acitretin. Dermatol Reports. 2011;3:e2. 51. Armstrong K, Weinstein M. Pyogenic granulomas during isotretinoin therapy. J Dermatol Case Rep. 2011;5:5–7. 52. Onder M, Oztaş MO, Oztaş P. Isotretinoin-induced nail fragility and onycholysis. J Dermatolog Treat. 2001;12:115–116. 53. Dogan G. Possible isotretinoin-induced keloids in a patient with Behçet’s disease. Clin Exp Dermatol. 2006;31:535–537. 54. Guadanhim LR, Gonçalves RG, Bagatin E. Observational retrospective study evaluating the effects of oral isotretinoin in keloids and hypertrophic scars. Int J Dermatol. 2016;55:1255–1258. 55. Lowenstein EB, Lowenstein EJ. Isotretinoin systemic therapy and the shadow cast upon dermatology’s downtrodden hero. Clin Dermatol. 2011;29:652–661. 56. Kaufman BP, Aman T, Alexis AF. Postinflammatory hyperpigmentation: Epidemiology, clinical presentation, ­ pathogenesis and treatment. Am J Clin Dermatol. 2018;19: 489–503. 57. ACCUTANE® (isotretinoin) Capsules. Drug prescription. https://www.rxlist.com/accutane-drug.htm#side_effects. 58. TAZORAC® (tazarotene) gel prescribing information. https:// www.allergan.com/assets/pdf/tazorac_gel. 59. Toctino 10 mg soft capsules, alitretinoin, package inserts. https://www.medicines.org.uk/emc/product/6364/smpc. 60. Targretin® (bexarotene) capsules, 75 mg. https://www.accessdata.fda.gov/drugsatfda_docs/label/1999/21055lbl.pdf. 61. David M, Sandbank M, Lowe NJ. Erythema multiformelike eruptions associated with etretinate therapy. Clin Exp Dermatol. 1989;14:230–232. 62. Boer J, Smeenk G. Nodular prurigo-like eruptions induced by etretinate. Br J Dermatol. 1987;116:271–274. 63. Higgins EM, Pembroke AC. Sticky palms—an unusual side-effect of etretinate therapy. Clin Exp Dermatol. 1993;18:389–390. 64. Stetson CL, Butler DF, Rapini RP. Herpetic whitlow during isotretinoin therapy. Int J Dermatol. 2003;42:496–498. 65. Ahdout J, Mandel H, Chiu M. Erythroderma in a patient taking acitretin for plaque psoriasis. J Drugs Dermatol. 2008;7:391–394. 66. Mahé E, Descamps V, Baïkian B et al. Acitretin-induced erythroderma in a psoriatic patient. J Eur Acad Dermatol Venereol. 2006;20:1133–1134. 12 Ophthalmologic Side Effects Remzi Karadag and Fehim Esen Introduction While retinoids provide a good therapeutic outcome for many dermatologic conditions, adverse effects can be disturbing for patients and physicians alike. The ocular surface and other parts of the eye are among the most commonly affected tissues by retinoids, with the most frequent ocular adverse effect being dry eye disease, reported in 30%−60% of patients in various studies (1–3). These findings usually develop due to excessive evaporation of the tear film due to deficiency of the lipid layer, and not due to a lack of secretions. The oldest and most commonly used retinoid compound is isotretinoin, and most of the experiences on the adverse effects of retinoids have been associated with isotretinoin treatment. There have been many reports describing the various ocular pathologies occurring with isotretinoin use (4–7). A comprehensive review of 2449 documented reports of ocular adverse events according to the World Health Organization (WHO) Classification System for Causality Assessment of Suspected Adverse Events provides an understanding for a level of evidence associated with adverse events found with isotretinoin use (4). Such confirmed and possible associated adverse events with isotretinoin use in this analysis are listed in Table 12.1. Isotretinoin changes the structure of the meibomian glands by decreasing the density of goblet cells and increasing the thickness and keratinization of the meibomian gland ducts at the histologic level in rabbits, leading to a lower lipid content and smaller acini (13). Human meibomian glands also become less dense and atrophic in shape after isotretinoin treatment, which can be demonstrated noninvasively with meibomiography. This condition further induces changes in the thickness of meibum, a decrease in the volume of secreted meibum, and increased tear osmolarity (14). Representative clinical images of a patient with meibomian gland dysfunction (MGD) are seen in Figure 12.1. Increase in tear osmolarity is a component of dry eye disease which can stimulate corneal cold thermoreceptors (12) and further contribute to the dryness sensation at the ocular surface (15). Many patients experience a temporary increase in dry eye disease and related ocular surface discomfort along with increased blepharitis (Figure 12.1a,c) in 36% of the patients receiving isotretinoin treatment (16). Tear secretion does not decrease after discontinuing isotretinoin; however, the basal tear secretion and tear breakup time do decrease. Conjunctival damage is seen during isotretinoin treatment at the histologic level with transiently TABLE 12.1 Causality Assessment of Suspected Ocular-Adverse Events According to the WHO Classification System Blepharoconjunctivitis, Meibomian Gland Dysfunction, and Dry Eye Disease Meibomian glands are modified sebaceous glands located within the tarsal plate of the eyelids, and secrete a lipid and protein mixture called meibum. Lipids secreted by the meibomian glands constitute the lipid layer of the tear film and reduce evaporation of the aqueous tear layer. As meibomian glands are structurally larger, modified sebaceous glands, isotretinoin reduces their secretions in a similar fashion to the sebaceous glands in the skin, leading to evaporative dry eye disease (8). Isotretinoin alters the gene expression pattern in meibomian gland epithelial cells, leading to inhibition of cell proliferation and increased cell death (9). Isotretinoin also augments expression of IL-1β and matrix metallopeptidase 9 (9), two important inflammatory mediators that have been implicated in the development of other forms of dry eye disease (10,11). As a result, isotretinoin treatment has the potential to induce inflammation of the meibomian glands and ocular surface, which has a wellestablished association with dry eye disease (12). Certain Abnormal meibomian gland secretion Blepharoconjunctivitis Corneal opacities Decreased dark adaptation Decreased tolerance to contact lens Decreased vision Increased tear osmolarity Keratitis Meibomian gland atrophy Myopia Ocular discomfort Photophobia Ocular sicca Teratogenic ocular abnormalities Probable/Likely Decreased color vision (reversible) Permanent loss of dark adaptation Possible Corneal ulcers Diplopia Eyelid edema Idiopathic intracranial hypertension with optic disk edema Optic neuritis Permanent sicca-like syndrome Subconjunctival hemorrhage Sources: Fraunfelder FT et al. Am J Ophthalmol. 2001;132:299–305; Gartaganis SP et al. Skin Pharmacol Appl Skin Physiol. 2002;15:200–204. 67 68 Retinoids in Dermatology (b) (c) (a) FIGURE 12.1 (a) Blepharitis under isotretinoin treatment. (b) Obstructive meibomian gland orifice changes (black arrows). (c) Some of the meibomian gland orifices are obstructed and scarred. increased conjunctival impression cytology scores during isotretinoin treatment (16). The impact of these histologic changes can also be observed clinically during slit lamp examination of the ocular surface with rose bengal staining which marks the degenerated and dead cells. Subsequently, such patients tend to complain of ocular surface discomfort, which can be documented by increased Ocular Surface Disease Index scores. Fortunately, these ocular surface disorders disappear in most patients 1 month following cessation of treatment (16). Contact lens wear affects meibomian gland morphology and function (17), and MGD is further associated with contact lens intolerance (18). Both isotretinoin use and contact lens wear can exacerbate MGD; therefore, contact lens intolerance is a common finding among contact lens users (19). Contact lens use should be questioned before starting isotretinoin treatment. Cessation of contact lens use is a successful option in preventing contact lens discomfort during treatment. With the development of better surface moistening technologies for modern contact lenses, some patients can actually continue wearing their lenses during treatment (19). Close ophthalmologic follow-up is recommended, and preservative-free artificial teardrops may be used in these patients during contact lens wear. Acitretin is also associated with similar ocular surface changes, with the main findings being blepharoconjunctivitis and dry eye disease (5). Contact lens intolerance can also occur during the use of acitretin due to a component of r­etinoid-induced ocular surface changes (20). There is no detailed report for the association of bexarotene or alitretinoin treatment with dry eye disease or other ocular surface problems; however, package inserts of these two retinoids also describe these ocular s­ urface conditions and dry eye disease as common adverse events (21,22). There is no specific treatment to reverse retinoid-associated MGD; however, patients can benefit from standard methods used in the management of MGD. Warm compresses, eyelid massage, eyelid hygiene, and promotion of meibum secretion are very helpful. Hydration of the ocular surface with artificial tears and lubricants will further reduce the effects of evaporative dry eye disease. Artificial tears with lipid content are very helpful, as they target the underlying pathology. There is some evidence that oral antimicrobials (doxycycline 100 mg bid, tetracycline 250 mg bid, or azithromycin 500 mg/day for 3 days in 7-day intervals for 4 weeks) may improve the fatty acid composition of the meibum and relieve MGD-associated symptoms (8); however, the success of these antibiotic treatment protocols has not been specifically tested in the setting of retinoid-associated MGD. Corneal Opacities, Keratitis, and Photophobia Development of corneal opacities is an exceedingly rare adverse effect of isotretinoin use, but it is a relatively serious condition (4). These lesions occur on the superficial stroma as fine, rounded, white to grayish, numerous, small dots (usually around hundreds or thousands) at the peripheral part of the cornea. If these lesions are observed, isotretinoin treatment should be immediately discontinued (23). Most of these lesions are reversible after discontinuation of isotretinoin (1), but some patients may develop irreversible corneal opacities (23). Punctate epithelial erosions or superficial punctate keratitis (Figure 12.2) is a finding associated with dry eye disease, reflecting the damaged ocular surface with dryness on the corneal epithelium. Although the association of keratitis with isotretinoin FIGURE 12.2 Superficial punctate keratitis. 69 Ophthalmologic Side Effects use was previously listed as certain (4), these older reports probably represented dryeye disease–associated punctate epithelial erosions, not the full-blown clinical picture of keratitis (24). There is no detailed study describing the association of these corneal findings with other retinoids; however, the package inserts of other retinoid compounds (acitretin, bexarotene, and alitretinoin) also describe corneal involvement and visual disturbances among rare side events (21,22,25). Photophobia (ocular discomfort or pain associated with light exposure) is a symptom that is associated with a wide spectrum of ocular or extraocular pathologies, such as migraine headaches. Photophobia is commonly seen in association with various ocular inflammatory conditions such as uveitis, keratitis, allergic conjunctivitis, and dry eye disease. UVA exposure of isotretinoin results with its photoisomerization to other retinoic acid products and photolysis to other degradation products which is a possible mechanism for explaining the photosensitivity (26). Development of dry eye disease is obviously an important contributing factor for the development of photophobia associated with this treatment; however, it is unclear whether the photosensitizing property of the isotretinoin molecule under UVA exposure is linked with photophobia in the eyes, as well. Management of this disturbing finding includes treatment of the underlying pathology (such as dry eye disease) and the use of sunglasses. Idiopathic Intracranial Hypertension and Optic Disk Edema Idiopathic intracranial hypertension (IIHT) is a relatively rare but important adverse effect of retinoid treatments (34). Tetracyclines may also contribute to the risk of developing IIHT (35). Headache is the most common symptom, and papilledema is the most important sign for the diagnosis of IIHT. Although late-stage papilledema can easily be observed by direct ophthalmoscopic examination, indirect ophthalmoscopy is required in all suspected cases to allow stereoscopic visualization of the optic disc in order not to miss early stages of papilledema. Clinical images of a healthy optic disc and a papilledematous optic disc swelling secondary to IIHT are described in Figure 12.3. An examination by an ophthalmologist and/or neurologist is important if a patient complains of a headache during isotretinoin treatment. After the cessation of treatment, a re-challenge with isotretinoin may cause recurrence of IIHT and related symptoms (36). Similarly, acitretin use is also associated with the development of IIHT and papilledema in some cases as a rare complication (20). This complication also necessitates the discontinuation of acitretin treatment. There is no published report studying the influence of other retinoid compounds (bexarotene and alitretinoin) on papilledema development; however, idiopathic intracranial hypertension is also listed as an associated adverse event in the package insert of alitretinoin (22). Photoreceptors and Retinal Nerve Fiber Layer Some patients may experience decreased dark adaptation and night blindness during retinoid treatment, but this is reversible. Isotretinoin can cause reversible abnormalities in the function of rod cells in rats that can be documented with electroretinography (27). Administration of high dose isotretinoin to rats (40 mg/kg) slows recovery of rod signaling after bleaching by slowing down the regeneration of rhodopsin (a complex protein sensitive to light that contains another vitamin A derivative, 11-cis retinal, as cofactor) in the visual cycle; however, rod functions become normal after dark adaptation, when enough time is allowed for the delayed recovery of rhodopsin and no histological damage occurs at the retinal tissue (28). Decreased color vision may occur during isotretinoin treatment but this is also reversible (4). The incidence of this adverse effect is very low and could not be repeated in some studies (27,29). Both isotretinoin and acitretin treatments are also associated with a reduction in contrast sensitivity (5,30). There is no detailed study on the influence of acitretin, bexarotene, and alitretinoin on dark adaptation; however, package inserts of acitretin and alitretinoin also list night blindness among the adverse events (22,25). Retinal nerve fiber layer (RNFL) analysis of patients under isotretinoin has been followed for the evaluation of possible toxicity on retinal ganglion cells. There is no global decrease in RNFL or retinal ganglion cell layers after isotretinoin treatment (29,31); however, some reports suggest that some localized changes in the RNFL may develop after isotretinoin treatment (32,33), but these reports have statistical limitations of small sample sizes and lack of correction for multiple testing. Myopia The most rapid phase of myopic progression occurs during adolescence and young adults (37). This time period also coincides with the age group where isotretinoin use is most commonly needed. In most cases, it is difficult to determine whether this is an isotretinoin-associated adverse event or the expected pattern of myopia progression in young adults. There are some clear reports that do not match with the regular pattern of myopia progression (38,39). There is an additional report describing a reversible progression of myopia and reversal of myopic progression after re-challenge with isotretinoin (40). It is also quite possible to miss many cases of isotretinoin-induced myopia progression that are within the expected range of myopia progression and not further investigated. There is no prospective study on this topic, and the mechanism of action of this adverse event is unclear. Normally, the eye has an emmetropization mechanism that balances the growth of the eye in a way that the light would be focused on the retina. Peripheral visual stimuli are associated with scleral growth and emmetropization (41). We hypothesize that the previously mentioned metabolic effects of isotretinoin on the retinol cycle might affect the influence of peripheral visual stimuli on the retina. We have not found any published report studying the influence of other retinoid compounds on myopia progression. Other Ocular Adverse Effects Teratogenic adverse events associated with retinoid treatments are well documented and have been known for a very long period of 70 Retinoids in Dermatology (a) (c) (b) (d) (e) (f ) FIGURE 12.3 (a) The margins of the optic nerve head are clearly visible in the healthy optic disc. (b) In papilledema secondary to idiopathic intracranial hypertension, the margins of the optic disc are unclear. (c) Optical coherence tomography (OCT) images of the same healthy optic disc reveal a normal, a flat optic disc anatomy in the 3D reconstruction image, and (d) a normal optic cup in the horizontal section. (e) OCT imaging of the same papilledematous disc reveals disc edema in the 3D reconstruction image, and (f) the loss of optic cup in the horizontal sections. time (42). Maternal isotretinoin use is also associated with various congenital ocular abnormalities such as microphthalmos, orbital hypertelorism, optic nerve hypoplasia, and cortical blindness (1). Fortunately, these adverse events are not seen today, with the advent of programs like iPledge and more awareness of their teratogenicity. All retinoid compounds should be avoided during pregnancy. There are also some case reports describing the association of some rare adverse events such as optic neuritis, diplopia, and subconjunctival hemorrhage with isotretinoin treatment (4,43,44). An examination of these individual cases does not indicate whether the unwanted events are coincidental or actually retinoid induced. The package insert of bexarotene explains that this medication can increase the rate of cataract development as a side event (21); however, this is not a very worrying adverse event for an antineoplastic medication, because cataracts are relatively benign conditions compared to the dangers of the neoplasms, considering that modern cataract surgery can provide excellent visual outcomes. Conclusions Retinoid treatments are associated with various ocular adverse events that should be monitored during treatment with an ophthalmologic consultation as an option. The most common adverse event associated with this treatment is meibomian gland dysfunction and dry eye disease, which should be told to patients, and the use of lubricant eye drops may be recommended. Patients should be asked about their use of contact lenses. Corneal opacities or idiopathic intracranial hypertension are rare, but important adverse events and require immediate discontinuation of isotretinoin treatment. REFERENCES 1. Fraunfelder FT, LaBraico JM, Meyer SM. Adverse ocular reactions possibly associated with isotretinoin. Am J Ophthalmol. 1985;100:534–537. 2. Hull PR, Demkiw-Bartel C. Isotretinoin use in acne: Prospective evaluation of adverse events. J Cutan Med Surg. 2000;4:66–70. 3. McLane J. Analysis of common side effects of isotretinoin. J Am Acad Dermatol. 2001;45:188–194. 4. Fraunfelder FT, Fraunfelder FW, Edwards R. Ocular side effects possibly associated with isotretinoin usage. Am J Ophthalmol. 2001;132:299–305. 5. Gartaganis SP, Mela EK, Georgakopoulos CD et al. Effects of oral acitretin on contrast sensitivity and tear film function: A prospective study. Skin Pharmacol Appl Skin Physiol. 2002;15:200–204. Ophthalmologic Side Effects 6. Santaella RM, Fraunfelder FW. Ocular adverse effects associated with systemic medications: Recognition and management. Drugs 2007;67(1):75–93. 7. Bergler-Czop B, Bilewicz-Stebel M, Stańkowska A et al. Side effects of retinoid therapy on the quality of vision. Acta Pharm 2016;66(4):471–478. 8. Moy A, McNamara NA, Lin MC. Effects of isotretinoin on meibomian glands. Optom Vis Sci. 2015;92:925–930. 9. Ding J, Kam WR, Dieckow J, Sullivan DA. The influence of 13-cis retinoic acid on human meibomian gland epithelial cells. Invest Ophthalmol Vis Sci. 2013;54:4341–4350. 10. Solomon A, Dursun D, Liu Z et al. Pro- and anti-inflammatory forms of interleukin-1 in the tear fluid and conjunctiva of patients with dry-eye disease. Invest Ophthalmol Vis Sci. 2001;42:2283–2292. 11. Luo L, Li DQ, Doshi A et al. Experimental dry eye stimulates production of inflammatory cytokines and MMP-9 and activates MAPK signaling pathways on the ocular surface. Invest Ophthalmol Vis Sci. 2004;45:4293–4301. 12. Craig JP, Nichols KK, Akpek EK et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15:276–283. 13. Kremer I, Gaton DD, David M et al. Toxic effects of systemic retinoids on meibomian glands. Ophthalmic Res. 1994;26:124–128. 14. Mathers WD, Shields WJ, Sachdev MS et al. Meibomian gland morphology and tear osmolarity: Changes with Accutane therapy. Cornea. 1991;10:286–290. 15. Parra A, Gonzalez-Gonzalez O, Gallar J et al. Tear fluid hyperosmolality increases nerve impulse activity of cold thermoreceptor endings of the cornea. Pain. 2014;155:1481–1491. 16. Karalezli A, Borazan M, Altinors DD et al. Conjunctival impression cytology, ocular surface, and tear-film changes in patients treated with systemic isotretinoin. Cornea. 2009;28:46–50. 17. Villani E, Ceresara G, Beretta S et al. In vivo confocal microscopy of meibomian glands in contact lens wearers. Invest Ophthalmol Vis Sci. 2011;52:5215–5219. 18. Arita R, Fukuoka S, Morishige N. Meibomian Gland dysfunction and contact lens discomfort. Eye Contact Lens. 2017;43:17–22. 19. Arman A, Demirseren DD, Akoglu G. Tolerance to systemic isotretinoin therapy in two patients using highly wettable contact lenses. Case Rep Ophthalmol Med. 2014;2014:452462. 20. Katz HI, Waalen J, Leach EE. Acitretin in psoriasis: An overview of adverse effects. J Am Acad Dermatol. 1999;41:7–12. 21. Targretin-(bexarotene). Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/1999/21055lbl.pdf. 22. Toctino-(alitretinoin). Available from: https://ca.gsk.com/ media/1352344/toctino-product-monograph.pdf. 23. Ellies P, Dighiero P, Legeais JM et al. Persistent corneal opacity after oral isotretinoin therapy for acne. Cornea. 2000;19:238–239. 24. Neudorfer M, Goldshtein I, Shamai-Lubovitz O et al. Ocular adverse effects of systemic treatment with isotretinoin. Arch Dermatol. 2012;148:803–808. 25. Soriatane-(acitretin). Available from: https://www.accessdata. fda.gov/drugsatfda_docs/label/2015/019821s027lbl.pdf. 71 26. Tashtoush BM, Jacobson EL, Jacobson MK. UVA is the major contributor to the photodegradation of tretinoin and isotretinoin: Implications for development of improved pharmaceutical formulations. Int J Pharm. 2008;352:123–128. 27. Weleber RG, Denman ST, Hanifin JM et al. Abnormal retinal function associated with isotretinoin therapy for acne. Arch Ophthalmol. 1986;104:831–837. 28. Sieving PA, Chaudhry P, Kondo M et al. Inhibition of the visual cycle in vivo by 13-cis retinoic acid protects from light damage and provides a mechanism for night blindness in isotretinoin therapy. Proc Natl Acad Sci USA. 2001;98:1835–1840. 29. Kapti BH, Aslan G, Yavruoglu MA. Evaluation of retinal nerve fiber layer changes with oral isotretinoin treatment. Ophthalmol Ther. 2013;2:19–23. 30. Polat M, Kukner S. The effect of oral isotretinoin on visual contrast sensitivity and amount of lacrimation in patients with acne vulgaris. Cutan Ocul Toxicol. 2017;36:35–38. 31. Bakbak B, Gedik S, Koktekir BE et al. Structural and functional assessment in patients treated with systemic isotretinoin using optical coherence tomography and frequency-doubling technology perimetry. Neuroophthalmology. 2013;37:100–103. 32. Ucak H, Aykut V, Ozturk S et al. Effect of oral isotretinoin treatment on retinal nerve fiber layer thickness. J Cutan Med Surg. 2014;18:236–242. 33. Yilmaz U, Kucuk E, Koc C et al. Investigation of the effects of systemic isotretinoin treatment on retinal nerve fiber layer and macula. J Dermatolog Treat. 2017;28:314–317. 34. Friedman DI. Medication-induced intracranial hypertension in dermatology. Am J Clin Dermatol. 2005;6:29–37. 35. Lee AG. Pseudotumor cerebri after treatment with tetracycline and isotretinoin for acne. Cutis. 1995;55:165–168. 36. Fraunfelder FW, Fraunfelder FT, Corbett JJ. Isotretinoinassociated intracranial hypertension. Ophthalmology. 2004;111:1248–1250. 37. Cooper J, Tkatchenko AV. A review of current concepts of the etiology and treatment of myopia. Eye Contact Lens. 2018;44:231–247. 38. Martinez-Gonzalez MC, Garcia-Silva J, Sanchez MA et al. Acute myopia while on oral isotretinoin treatment. J Eur Acad Dermatol Venereol. 2007;21:977–978. 39. Saraswat A. Sudden irreversible worsening of myopia with isotretinoin treatment. Indian J Dermatol Venereol Leprol. 2011;77:611–612. 40. Palestine AG. Transient acute myopia resulting from isotretinoin (accutane) therapy. Ann Ophthalmol. 1984;16:660–662. 41. Karabas L, Esen F, Celiker H et al. Decreased subfoveal choroidal thickness and failure of emmetropisation in patients with oculocutaneous albinism. Br J Ophthalmol. 2014;98:1087–1090. 42. Lammer EJ, Chen DT, Hoar RM et al. Retinoic acid embryopathy. N Engl J Med. 1985;313:837–841. 43. Perez-Perez L, Garcia-Gavin J, Allegue F et al. Optic neuritis probably induced by isotretinoin. Actas Dermosifiliogr. 2012;103:843–844. 44. Alam MS, Agarwal S. Presumed isotretinoin-induced extraocular myopathy. J Pharmacol Pharmacother. 2016;7:187–189. 13 Musculoskeletal Side Effects Filiz Cebeci Kahraman, Vefa Aslı Turgut Erdemir, and Melek Aslan Kayıran Introduction Osteoporosis and Fractures The term retinoid is used to describe natural derivatives of retinaldehyde, retinoic acid, and retinyl esters or synthetic analogs of vitamin A. Synthetic analogs of vitamin A mainly include acitretin, isotretinoin, bexarotene, and alitretinoin (1,2). Isotretinoin, acitretin, and bexarotene have been approved by the US Food and Drug Administration (FDA) for acne vulgaris, psoriasis, and mycosis fungoides, respectively (2) Their clinical usage is often limited due to unwanted clinical findings (3). Hypervitaminosis A is a serious and life-threatening condition. In developed countries, there is a growing concern of subtoxicity of excessive vitamin A, due to the lack of sensitive markers for toxicity of serum retinol concentrations. Acute and chronic toxicity is dose-dependent and well documented in the literature. The acute form occurs as a result of excessive intake of vitamin A over a short period, even a few hours or days. The chronic form occurs over months and years of ingestion of vitamin A doses (4). Many patients with genodermatoses are exposed to synthetic retinoid toxicity because they require lifelong therapy with retinoids and hence become chronic toxicity candidates. Hepatic, skeletal, and cardiovascular systems are the most affected systems from chronic synthetic retinoid toxicity (5). Musculoskeletal changes include osteoporosis, spinal ligament ossification, diffuse idiopathic skeletal hyperostosis (DISH), sacroiliitis, myalgia and cramping, increased muscle tone, axial muscle rigidity, myopathy, spontaneous fractures, and temporary pain in the rib cage (6–12). Acitretin is a second-generation retinoid and the active metabolite of etretinate with a shorter half-life (13). Etretinate was the first oral retinoid approved for the treatment of psoriasis. It was later phased out in 1998 due to its unfavorable pharmacokinetic profile, and was replaced by acitretin. Acitretin had been approved by the FDA the previous year for the treatment of psoriasis (14). The many undesirable effects associated with the use of acitretin are dose related, usually reversible, and resolve on dose reduction or discontinuation, although the adverse effects on bone appear to be irreversible (15). The first reported side effect of isotretinoin related to the skeletal system was premature closure of proximal tibial epiphyses, in 1982 (16). Hyperostosis, anterior and posterior longitudinal ligament ossification, proliferative enthesopathy, and bone mineral density decrease were subsequently observed (17–19). Bone modeling is a process that changes both the size and the shape of the bone. This process sometimes occurs as bone resorption but not following bone formation and sometimes bone formation without previous bone resorption (20). Stromal cells/osteoblasts are responsible for the macrophage colony-­ stimulating factor (M-CSF) and receptor activator of nuclear factor κB ligand (RANKL) production, which play key roles in osteoclast regulation. M-CSF helps osteoclast survival and regulation, and RANKL is necessary for progenitor differentiation to osteoclasts (21). Recently, an animal study, conducted to determine retinoid induced bone resorption, showed increased RANKL, mRNA, and protein expression (22). The activation of osteoclasts was studied in thyroparathyroidectomized rats by using retinoid ethyl p-benzoate. The results showed that retinoids affected Ca metabolism directly on bone resorption. This situation leads to Ca changes in plasma, 1.25 (OH) 2 D levels, Ca absorption, and excretion (23). Also, there are some experimental studies resulting with cortical bone thinning due to stimulation of subperiosteal resorption with a high dose of retinoids (24). Observational and epidemiologic studies to determine a possible association between vitamin A and osteoporosis and/or fractures have produced controversial results (25). A cross-­sectional study showed 1500 mg daily dietary retinol intake causes an increase in hip fractures, with reduced bone mineral density at the femoral neck, lumbar spine, and total body compared with 500 mg daily intake (26). Postmenopausal women, examined for vitamin A intake and related hip fractures and high vitamin A intake (>3000 microgram/d) had increased risk for fractures (1.48 fold), when compared to a lower vitamin A intake (27). In other studies measuring bone mineral density (BMD), no relationship with retinol or provitamin A carotenoids from foods or supplements were observed (28,29). Similar controversial results are also available for etretinate and acitretin. In a cross-sectional comparative study, 15 patients treated with etretinate in the long term showed significantly decreased BMD values at the femoral neck, Wards triangle, trochanter, and radius. The lumbar spine was not affected (8). Another study with 13 psoriatic patients who were taking longterm (average 3.7 years) etretinate showed a decrease of BMD in the lumbar spine (30). These two studies found no association between etretinate dose and BMD (8,30). A case control study compared 124,655 patients with bone fractures and 124,655 controls. The results showed no increased 73 74 Retinoids in Dermatology risk of fractures in the acitretin patient group (31). In a more recent study of 30 patients who were taking acitretin for a median of 3.6 years, there was no significant bone mineral loss with acitretin therapy (32). Based on current data and the accumulated clinical evidence, it no longer appears reasonable to link acitretin to increased osteoporosis risk and fractures; therefore, it is no longer recommended to perform bone tests before or during treatment, except when a history of bone disease makes this advisable (33). These controversial results are also available for isotretinoin. Some studies report that the use of high dose isotretinoin has negative effects on BMD, as well as some other studies indicating that there is no change or a slight reduction before and after treatment (34–36). It is also claimed that vitamin D deficiency may increase bone resorption with isotretinoin treatment (37). In a study of 50 acne patients, serum calcium and 25 hydroxy vitamin D levels were found significantly lower while 1,25 dihydroxy vitamin D, parathormone, and bone-specific alkaline phosphatase (ALP) levels were found significantly high (38). The early effects on bone turnover with the nodulocystic acne patients taking isotretinoin were studied. A significant decrease was observed in the serum carboxyterminal propeptide of type I collagen, bone-specific ALP, the carboxyterminal telopeptide of type I collagen, calcium, osteocalcin and urine levels of calcium and hydroxyproline within 5 days of treatment. Serum parathyroid hormone levels were found to be significantly high; however, all the abnormal levels returned to normal in the fourteenth day of the treatment. As a result, the effects of the drug on bone turnover, except the increase in parathyroid hormone levels, were directly attributed to the inhibitory effects of the drug on bone (39). Diffuse Idiopathic Skeletal Hyperostosis The diffuse idiopathic skeletal hyperostosis (DISH) created by retinoids constitutes the main effect on the bones, and these effects usually occur over a 10-year period with prolonged and high doses of retinoid use. The disease is characterized by the enthesal ossification of the anterolateral portion of the thoracic spine (40). Resnick and Niwayama diagnostic criteria are used in the diagnosis, which include (41): • Calcification and ossification of the anterolateral parts of at least four contiguous vertebrae • Lack of radiographic changes of the degenerative disc disease and preservation of disc height • The absence of apophyseal joint bone ankylosis and sacroiliac disease The mechanism of DISH is unclear. Some metabolic disturbances, like hyperlipidemia, hyperuricemia, and diabetes mellitus, have been shown to be related to the disease (42). Retinoic acid is obligatory for mesenchymal cell differentiation and embryonic skeletal development. Development of DISH due to retinoids may be associated with mesenchymal stem cell proliferation that gives rise to osteoblastic differentiation in the entheses (43). The thoracic and cervical vertebra section is frequently affected, but extraspinal hyperostosis can also be seen (44). In congenital lamellar ichthyosis, which requires long-term retinoid treatment, there may be iliolumbar vertebra ossification (45). Interosseous membrane calcification has been described in a patient with pityriasis rubra pilaris following the use of acitretin (46). Acitretin was prescribed for 13 years in a patient with severe psoriasis who developed periosteal hyperostosis and a bridging deformity between the acetabulum and the large femoral trochanter (47). There are additional controversial reports. In a single center, retrospective study with 49 patients who had received acitretin treatment for more than 1 year, there was no association of the DISH syndrome (48). In two prospective studies involving 128 and 380 patients who showed worsening of preexisting skeletal bone deposition, only fewer than 1% of patients showed new bony pathologies (49). There is a need for controlled and prospective studies, because not only is the literature controversial, but it does not provide a sufficient link between acitretin and DISH syndrome. Imaging studies are recommended when there are entheses signs, thoracic pain, and stiffness. Skeletal hyperostosis has been seen 1 year after starting treatment in patients who had received 2 mg/kg isotretinoin per day in keratinization disorders. Such hyperostosis became permanent over time (50). Hyperostosis may become a serious side effect with long-term, high-dose isotretinoin treatment (51). Such patients should have skeletal x-rays at the beginning and on the sixth and twelfth months if prolonged treatment is planned (52). Short-term use of isotretinoin reduces the risk of hyperostosis (53). Retinoid hyperostosis is dependent on age, dose, and duration of treatment (2). This risk increases for long-term, high-dose use and for older patients. There is no need to stop isotretinoin in the case of hyperostosis but if the treatment is necessary, surgical intervention may be preferred since bisphosphonates are ineffective (54). Premature Early Epiphyseal Closure Chondrogenesis is responsible for bone elongation at the growth plate, consisting of chondrocyte proliferation, hypertrophy, and extracellular matrix secretion. In addition to multiple paracrine factors, vitamin D/retinoid X receptor activation is important for chondrocyte transition from the resting to proliferative zone within the growth plate (55). Animal models have demonstrated epiphyseal closure in the tibia and femur which is treated with high doses of vitamin A. Besides these findings, markedly reduced longitudinal bone growth even before premature growth plate closure has been observed. These animal models showed retinoic acid receptor agonist activity alone is sufficient for ­retinoid-induced epiphyseal closure (56). Patients sometimes receive vitamin A and its derivates to treat acne, ichthyotic skin disease, and psoriasis. Retinoids may be used in the treatment of neuroblastoma. Isotretinoin induces cytodifferentiation and apoptosis, and it also inhibits angiogenesis and oncogene expression (57). Premature epiphyseal closure is a side effect of isotretinoin, related to young age at exposure, with subsequent long treatment duration. While most side effects are reversible after treatment discontinuation, there can be persistent 75 Musculoskeletal Side Effects harmful effects on the developing skeleton (58). Early premature epiphyseal closure has been reported with etretinate (59). Due to the rarity of this complication, x-ray follow-up is not recommended for children and adolescents taking retinoids for acne treatment unless they become symptomatic. Muscular Disease Drug-induced myopathies are often ignored, but early recognition and discontinuation of the drug may lead to prompt healing. Manifestations of myopathies include mild muscle pain, cramps, severe weakness, rhabdomyolysis, and even renal failure that may be fatal. Laboratory studies may show increased creatinine phosphokinase (CPK) levels and myoglobinuria. Electromyographic (EMG) and histologic changes may be seen. There are different mechanisms for myotoxicity. Muscle organel damage or inflammatory and immunologic reaction with muscle antigens as well as some nutritional and electrolyte imbalances can result in muscle dysfunction (60). Few case reports about muscular involvement with the oral administration of acitretin and etretinate exist. Three patients taking etretinate had muscle involvement in a report, but the physicians detected electromyographic and histopathologic evidence of muscle damage in only one patient. Two of them developed muscular weakness and pain at the third month, and the third one developed those symptoms at the seventh month of treatment. CPK levels were increased but returned to normal after discontinuing the treatment (61). Another patient taking acitretin for psoriasis developed severe myopathy in the fourteenth day of treatment. CPK levels were elevated and the patient complained about muscle weakness and swelling. The side effects resolved 2 months after discontinuing treatment (10). Axial muscle rigidity (63) and increased muscle tone (64) have also been reported while receiving etretinate. Although the data about the relationship between acitretin (etretinate) and muscle involvement are inconclusive, it is recommended that while on therapy, patients should avoid intense physical exercise to prevent muscular pain (13). If pain develops, CPK levels should be checked, and an EMG examination should be considered. The most common adverse effects of isotretinoin related to the muscles are myalgia, muscle tenderness, and stiffness. Fifteen percent to fifty percent of patients prescribed isotretinoin complain about myalgia and muscle stiffness (65). These symptoms usually resolve spontaneously after discontinuation of treatment, but a few patients have prolonged findings after stopping isotretinoin (66). In a retrospective study of a 5-year follow-up investigating the side effects of isotretinoin, 38.78% of 3525 patients complained of myalgia, and 12.28% had arthralgia (51). In another study of 89 patients, only 5 patients had elevated levels of CPK, and only one had myalgia. Two weeks after discontinuing the treatment, CPK levels returned to normal (65). There was no significant correlation between high levels of CPK and myalgia in these studies (51,68–70). In summary, there is no need to control CPK levels in patients with mild myalgia. In cases of severe myalgia, CPK levels and renal function tests should be examined to eliminate the risk of rhabdomyolysis (71). The high levels of CPK are usually related to extreme exercise in isotretinoin administered patients (72). This condition may be seen in patients with high muscle activity (71). Other possible reasons are intramuscular injections before blood analysis or concomitant viral infections (66,73,74). It would be wise to recommend that patients avoid extreme exercise during isotretinoin therapy. In a study of rat liver, the mitochondrial membrane may deteriorate rapidly, leading to cytochrome C release and apoptosis in hepatocytes in the presence of isotretinoin. Cytochrome C depletion, which is a part of the mitochondrial respiratory chain, may be associated with exercise intolerance, leading to recurrent myoglobinuria (75,76). A true myopathy developing during the use of isotretinoin is extremely rare. The clinical findings of fatigue, myalgia, muscle stiffness, and weakness should be confirmed by histopathologic examination showing a slight decrease in the muscle fibers, and needle electromyography before making such a diagnosis. These patients will usually complain of fatigue, myalgia, muscle stiffness, and weakness. When the retinoid is discontinued and has been the culprit, the patient will recover completely within 1 or 2 months (77). Acute rhabdomyolysis is the most severe and serious side effect associated with isotretinoin treatment. Generalized muscle pain, fatigue, profound weakness, and a fivefold increase in CPK levels are the landmarks for the diagnosis, and myoglobin can be detected in the urine. Acute renal failure may occur due to myoglobinuria-induced renal tubular obstruction, if untreated. Fortunately, this rare side effect has only been reported in two patients taking isotretinoin, and the side effect entirely resolved upon discontinuation of therapy (71,78). Arthropathy Arthralgia, arthritis, and sacroiliitis are known in patients receiving etretinate, acitretin, and isotretinoin, but there are little published data. Arthritis occurs due to damage and the immunomodulatory effects of retinoids upon the lysosomal membranes of synovial cells (79). The mechanisms for such sacroiliitis is unknown. One possibility may be abnormal cytokine balance induced by retinoids, and another is the detergent-like effects of retinoids inducing alterations of lysosomal membrane of the cells, leading to synovial cell obliteration and bony structure deformation (80). In a case report, a patient with psoriasis developed temporomandibular arthritis. Although the increased incidence of temporomandibular joint disturbances in psoriasis had been published previously, in this instance, the authors considered this as an adverse effect of etretinate, because the patient’s findings regressed completely after withdrawal of the drug (81). In another case report, spondyloarthropathic changes were detected in a patient with keratosis follicularis receiving acitretin. Sacroiliac pain, along with limited hip joint and lumbar spinal movements, was observed with approximately 4 1/2 months of treatment. On pelvic radiography, grade 1 sacroiliitis and enthesitis in bilateral heels were detected (80). Arthritis usually starts after 2−10 weeks of isotretinoin treatment (82). Patients with sacroiliitis receiving isotretinoin usually 76 complain of increased nocturnal back pain along with morning stiffness, which is decreased with motion. The pain is generally acute and sudden and usually spreads to the hips and under the lumbar region, although it may involve the groin, lower abdomen, lumbar area, the leg, and even the foot (83). Polyneuropathy has also been reported in some patients with sacroiliitis (83,84). Unilateral sacroiliitis, when reported, is usually observed in patients with short-term drug use, while bilateral sacroiliitis has been observed more frequently in patients with isotretinoin given for 2 years or longer (86). In a study of 73 acne patients receiving isotretinoin, 50.7% had lethargy, 42.5% had myalgia, and 49.3% had back pain. Pain often started during the second or third month of the treatment. Acute sacroiliitis was detected in 8.2% of these patients by magnetic resonance imaging (MRI). The patients had mild relief with taking nonsteroidal anti-inflammatory drugs (NSAIDs) during treatment and complete relief after the third month of finishing treatment (83). Achilles enthesopathy was also reported as a side effect in another study (18). Patients with acne fulminans may also have sacroiliitis as part of synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome; however, these patients may also have sacroiliitis related to isotretinoin (67,85). As a result, patients with SAPHO syndrome should be followed for the development of a possible sacroiliitis during systemic isotretinoin treatment. Direct x-ray findings are not sufficient for the assessment of sacroiliitis. Bone scintigraphy with technetium, computerized tomography, or MRI would be necessary in suspected cases. Such examinations may be helpful in assessing the severity of the disease. Human leukocyte antigen B27 may be detected in some of these patients (62,85), raising the questions of a genetic tendency to the development of sacroiliitis (86). Treatment involves discontinuing the isotretinoin and prescribing NSAIDs for the sacroiliitis. Oral corticosteroids may also be necessary, and physical therapy should be considered (67). Conclusions Many controversial studies and case reports about retinoids and their musculoskeletal side effects exist. The muscular effects are reversible with cessation of the drug. At the inception of treatment, patients should be told of possible myalgias and asked to avoid intense physical activity. CPK levels and renal function tests should be ordered to eliminate the risk of rhabdomyolysis in cases of severe myalgia. Patients with a history of myotoxic drug use (such as statins, corticosteroids, colchicine, penicillamine, and alcohol) require closer observation. The relationship between retinoids and osteoporosis or fractures is unclear, so we do not recommend performing BMD before or during retinoid treatment. Well-defined adverse bone effects include sacroiliitis with isotretinoin that usually resolves upon discontinuation of the drug. DISH is an irreversible but non-symptomatic adverse effect of retinoids that resolves with surgical intervention, if necessary. Musculoskeletal system side effects of retinoids in the pediatric population remain a mystery. As a result, children receiving long-term and/or high-dose isotretinoin should be monitored for early epiphyseal closure. Retinoids in Dermatology REFERENCES 1. Khalil S, Bardawil T, Stephan C et al. Retinoids: A journey from the molecular structures and mechanisms of action to clinical uses in dermatology and adverse effects. J Dermatolog Treat. 2017;28:684–696. 2. Mortazavi H, Aghazadeh N, Ghiasi M et al. A review of three systemic retinoids in dermatology: Acitretin, isotretinoin and bexarotene. J Dermatol. 2013;16:144–158. 3. Ormerod AD, Campalani E, Goodfield MJ. British Association of Dermatologists guidelines on the efficacy and use of acitretin in dermatology. Br J Dermatol. 2010;162:952–963. 4. Penniston KL, Tanumihardjo SA. The acute and chronic toxic effects of vitamin A. Am J Clin Nutr. 2006;83:191–201. 5. Vahlquist A. Long-term safety of retinoid therapy. J Am Dermatol. 1992;27:29–33. 6. Kilcoyne RF. Effects of retinoids in bone. J Am Acad Dermatol. 1988;19:212–216. 7. Sameem F, Semira. Isotretinoin-induced acute severe myopathy involving pelvic girdle muscles: A case report. Indian J Pharmacol. 2016;48:601–603. 8. Di Giovanna JJ, Sollitto RB, Abangan DL et al. Osteoporosis is a toxic effect of long-term etretinate therapy. Arch Dermatol. 1995;131:1263–1267. 9. Halkier-Sörensen L, Laurberg G, Andersen J. Bone changes in children on long-term treatment with etretinate. J Am Acad Dermatol. 1987;16:999–1006. 10. Lister RK, Lecky BRF, Lewis-Jones MS et al. Acitretininduced myopathy. Br J Dermatol. 1996;134:989–990. 11. Çakır T, Subaşı V, Bilgili A et al. A case with bilateral sacroiliitis and polyneuropathy development due to ısotretinoin use. Arch Rheumatol. 2014;29:304–308. 12. Karadağ Köse Ö, Hız Ö, Gökalp H et al. Development of acute sacroileitis due to the use of oral isotretinoin in patients with acne vulgaris: Four case presentations. Van Med J. 2017;24:372–377. 13. Bollag W. The development of retinoids in experimental and clinical oncology and dermatology. J Am Acad Dermatol. 1983;9:797–805. 14. Lee CS, Li K. A review of acitretin for the treatment of psoriasis. Expert Opin Drug Saf. 2009;8:769–779. 15. Carretero G, Ribera M, Belinchón I et al. Guidelines for the use of acitretin in psoriasis. Actas Dermosifiliogr. 2013;104:598–616. 16. Milstone LM, McOuire J, Ablow RC. Premature epiphyseal closure in a child receiving oral 13-cis-retinoic acid. J Am Acad Dermatol. 1982;7:663–666. 17. Erdogan BS, Yuksel D, Aktan S et al. The effects of isotretinoin treatment on bone mineral density in patients with nodulocystic acne. J Eur Acad Dermatol Venereol. 2006;20:1006–1007. 18. Alkan S, Kayiran N, Zengin O et al. Isotretinoin-induced spondyloarthropathy-related symptoms: A retrospective study. J Rheumatol. 2015;42:2106–2109. 19. Scuderi AJ, Datz FL, Valdivia S, Morton KA. Enthesopathy of patellar tendon insertion associated with isotretinoin therapy. The J Nuclear Med. 1993;34:455–457. 20. Martin TJ, Seeman E. Bone remodeling: Its local regulation and the emergence of bone fragility. Best Pract Res Clin Endocrinol Metab. 2008;22:701–722. 21. Takayanagi H. Osteoimmunology and the effects of the immune system on bone. Nat Rev Rheumatol. 2009;5:667–676. Musculoskeletal Side Effects 22. Conaway HH, Lerner UF. Retinoids and bone. In: Evanthia Diamanti-Kandarakis, editor. Contemporary Aspects of Open. Endocrinology. ISBN: 978-953-307-357-6. Intech­ Ava i lable f rom: ht t p://w w w.i nt e chop en.com / b o ok s / contemporary-aspects-of-endocrinology/retinoids-and-bone. 23. Trechsel U, Stutzer A, Fleisch H. Hypercalcemia induced with an arotinoid in thyroparathyroidectomized rats. New model to study bone resorption in vivo. J Clin Invest. 1987;80:1679–1686. 24. Kneissel M, Studer A, Cortesi R et al. Retinoid-induced bone thinning is caused by subperiosteal osteoclast activity in adult rodents. Bone. 2005;36:202–214. 25. Conaway HH, Henning P, Lerner UH. Vitamin A metabolism, action and role in skeletal homeostasis. Endocr Rev. 2013;34:766–797. 26. Melhus H, Michaelsson K, Kindmark A et al. Excessive dietary intake of vitamin A is associated with reduced bone mineral density and increased risk for hip fracture. Ann Intern Med. 1998;129:770–778. 27. Feskanich D, Singh V, Willett WC et al. Vitamin A intake and hip fractures among postmenopausal women. JAMA. 2002;287:47–54. 28. Wolf RL, Cauley JA, Pettinger M et al. Lack of a relation between vitamin and mineral antioxidants and bone mineral density: Results from the Women’s Health Initiative. Am J Clin Nutr. 2005;82:581–588. 29. Kaptoge S, Welch A, McTaggart A et al. Effects of dietary nutrients and food groups on bone loss from the proximal femur in men and women in the 7th and 8th decades of age. Osteoporos Int. 2003;14:418–428. 30. Okada N, Nomura M, Morimoto S et al. Bone mineral density of the lumbar spine in psoriatic patients with long-term etretinate therapy. Dermatol. 1994;21:308–311. 31. Vestergaard P, Rejnmark L, Mosekilde L. High-dose treatment with vitamin a analogues and risk of fractures. Arch Dermatol. 2010;146:478–482. 32. McMullen EA, McCarron P, Irvine AD et al. Association between long-term acitretin therapy and osteoporosis: No evidence of increased risk. Clin Exp Dermatol. 2003;28:307–309. 33. Paul C, Gallini A, Maza A et al. Evidence-based recommendations on conventional systemic treatments in psoriasis: Systematic review and expert opinion of a panel of dermatologists. J Eur Acad Dermatol Venereol. 2011;2:2–11. 34. Cantürk F, Saraç N, Aydın F et al. Bone mineral density in patients receiving isotretinoin and acitretin. TURKDERMARCH TURK D. 2004;38:191–194. 35. DiGiovanna JJ, Langman CB, Tschen EH et al. Effect of a single course of isotretinoin therapy on bone mineral density in adolescent patients with severe, recalcitrant, nodular acne. J Am Acad Dermatol. 2004;51:709–717. 36. Leachman SA, Insogna KL, Katz L et al. Bone densities in patients receiving isotretinoin for cystic acne. Arch Dermatol. 1999;135:961–965. 37. Saadi H, Afandi B, Houssami L et al. Effects of isotretinoin on bone turnover markers and bone mineral density in women with acne vulgaris and vitamin D deficiency: A preliminary study. Int J Diabetes Metab. 2008;16:107–112. 38. Ertuğrul DT, Karadağ AS, Tutal E et al. Does isotretinoin have effect on vitamin D physiology and bone metabolism in acne patients. Dermatologic Therapy 2011;24:291–295. 77 39. Kindmark A, Rollman O, Mallmin H et al. Oral isotretinoin therapy in severe acne induces transient suppression of biochemical markers of bone turnover and calcium homeostasis. Acta Derm Venereol. 1998;78:266–269. 40. Zhao S, Goodson NJ. Diffuse idiopathic skeletal hyperostosis and isotretinoin in cystic acne. BMJ Case Rep. 2015; 2015:bcr2015209775. 41. Resnick D, Niwayama G. Radiographic and pathologic features. Radiology. 1976;119:559–568. 42. Vezyroglou G, Mitropoulos A, Antoniadis C. A metabolic syndrome in diffuse idiopathic skeletal hyperostosis. A controlled study. J Rheumatol. 1996;23:672–676. 43. Troillet N, Gerster JC. [Forestier disease and metabolism disorders. A prospective controlled study of 25 cases]. [Article in French] Rev Rhum Ed Fr. 1993;60:274–279. 44. Brandt JR, Mick TJ. Extraspinal enthesopathy caused by isotretinoin therapy. J Manipulative Physiol Ther. 1999;22:417–420. 45. Rood MJ, Lavrijsen SP, Huizinga TW. Acitretin-related ossification. J Rheumatol. 2007;34:837–838. 46. Van Dooren-Greebe RJ, Van de Kerkhof PC. Extensive extraspinal hyperostosis after long-term oral retinoid treatment in a patient with pityriasis rubra pilaris. J Am Acad Dermatol. 1995;32:322–325. 47. Vincent V, Zabraniecki L. Acitretin-induced enthesitis in a patient with psoriatic arthritis. Joint Bone Spine. 2005; 2:326–329. 48. Lee E, Koo J. Single-center retrospective study of longterm use of low-dose acitretin (Soriatane) for psoriasis. J Dermatolog Treat. 2004;15:8–13. 49. Pang ML, Murase JE, Koo J. An updated review of acitretin-a systemic retinoid for the treatment of psoriasis. Expert Opin Drug Metab Toxicol. 2008;4:953–964. 50. Pennes DR, Martel W, Ellis CN, Voorhees JJ. Evolution of skeletal hyperostoses caused by 13-cis-retinoic acid therapy. AJR Am J Roentgenol. 1988;151:967–973. 51. Brzezinski P, Borowska K, Chiriac A et al. Adverse effects of isotretinoin: A large, retrospective review. Dermatol Therapy. 2017;30:1–6. 52. Brzezinski P, Sinjab AT. Low doses isotretinoin in the treatment of acne vulgaris. Practical Dermatology. 2012;3:1–54. 53. Ellis CN, Pennes DR, Hermann RC et al. Long-term radiographic follow-up after isotretinoin therapy. J Am Acad Dermatol. 1988;18:1252–1261. 54. Di Giovanna JJ. Isotretinoin effects on bone. J Am Acad Dermatol. 2001;45:176–182. 55. Lui JC, Andrade AC, Forcinito P et al. Spatial and temporal regulation of gene expression in the mammalian growth plate. Bone. 2010;46:1380–1390. 56. Standeven AM, Davies PJ, Chandraratna RA et al. Retinoidinduced epiphyseal plate closure in guinea pigs. Fundam Appl Toxicol. 1996;34:91–98. 57. Miller WH Jr. The emerging role of retinoids and retinoic acid metabolism blocking agents in the treatment of cancer. Cancer. 1998;83:1471–1482. 58. Noyes JJ, Levine MA, Belasco JB et al. Premature epiphyseal closure of the lower extremities contributing to short stature after cis-retinoic acid therapy in medulloblastoma: A case report. Horm Res Paediatr. 2016;85:69–73. 59. Glover MT, Atherton DJ. Etretinate and premature epiphyseal closure in children. J Am Acad Dermatol. 1987;17:853–854. 78 60. Valiyil R, Christopher-Stine L. Drug-related myopathies of which the clinician should be aware. Curr Rheumatol Rep. 2010;12:213–220. 61. Hodak E, David M, Gadoth N et al. Etretinate-induced skeletal muscle damage. Br J Dermatol. 1987;116:623–626. 62. Elías LM, Gómez MI, Torrelo A et al. Acne fulminans and bilateral seronegative Sacroileitis triggered by isotretinoin. J Dermatol. 1991;18:366–367. 63. Albin RL, Silverman AK, Ellis CN et al. A new syndrome of axial muscle rigidity associated with etretinate therapy. Mov Disord. 1988;3:70–76. 64. Ellis CN, Gilbert M, Cohen KA et al. Increased muscle tone during etretinate therapy. J Am Acad Dermatol. 1986;14: 907–909. 65. Dicken CH. Retinoids: A review. J Am Acad Dermatol. 1984;11:541–552. 66. Bigby M, Stern RS. Adverse reactions to isotretinoin. J Am Acad Dermatol. 1988;18:543–552. 67. Levinson M, Gibson A, Stephenson G. Sacroileitis secondary to isotretinoin. Australas J Dermatol. 2012;53:298–300. 68. Kaymak Y. Creatine phosphokinase values during isotretinoin treatment for acne. Int J Dermatol. 2008;47:398–401. 69. Bettoli V, Tosti A, Capobianco C et al. Creatine kinase values during isotretinoin treatment. Dermatologica. 1990;180:54–55. 70. Lipinsky JT, Schwimmer B. Elevated CPK and isotretinoin. J Am Acad Dermatol. 1985;12:581–582. 71. Guttman-Yassky E, Hayek T, Muchnick L et al. Acute rhabdomyolysis and myoglobinuria associated with isotretinoin treatment. Int J Dermatol. 2003;42:499–500. 72. Tillman DM, White SI, Aitchinson TC. Isotretinoin, creatine kinase, and exercise. Br J Dermatol. 1990;123:22–23. 73. Landau M, Mesterman R, Ophir J et al. Clinical significance of markedly elevated serum creatine kinase levels in patients with acne on isotretinoin. Acta Derm Venereol. 2001;81:350–352. Retinoids in Dermatology 74. Shalita AR, Cunningham WJ, Leyden JJ et al. Isotretinoin treatment of acne and related disorders: An update. J Am Acad Dermatol. 1983;9:629–638. 75. Rigobello MP, Scutari G, Friso A et al. Mitochondrial permeability transition and release of cytochrome c induced by retinoid acids. Biochem Pharmacol. 1999;58:665–670. 76. Di Mauro S. Mitochondrial myopathies. Curr Opin Rheumatol. 2006;18:636–641. 77. Fiallo P, Tagliapietra A-G. Severe acute myopathy induced by isotretinoin. Arch Dermatol. 1996;132:1521–1522. 78. Trauner MA, Ruben BS. Isotretinoin-induced rhabdomyolysis? A case report. Dermatol Online J. 1999;5:2. 79. Ellis CN, Krach KJ. Uses and complications of isotretinoin therapy. J Am Acad Dermatol. 2001;45:150–157. 80. Gündoğdu B, Karadağ AS. Spondyloarthritic changes during acitretin treatment. T Klin J Case Reports. 2019;27:54–58. 81. Yamamoto T, Watanabe K, Nishioka K. Temporomandibular arthritis in a patient with psoriasis vulgaris under systemic etretinate therapy. Dermatology. 2004;209:77. 82. Matsuoka LY, Wortsman J, Pepper JJ. Acute arthritis during isotretinoin treatment for acne. Arch Intern Med. 1984;144:1870–1871. 83. Slobodin G, Rimar D, Boulman N et al. Acute Sacroileitis. Clin Rheumatol. 2016;35:851–856. 84. Eksioglu E, Oztekin F, Unlu E et al. Sacroileitis and polyneuropathy during isotretinoin treatment. Clin Exp Dermatol 2008;33:122–124. 85. Dinçer Ü, Çakar E, Kıralp MZ et al. Can isotretinoin induce sacroileitis: Three cases. Arch Rheumatol. 2008;23: 157–159. 86. Baykal Selçuk L, Aksu Arıca D, Baykal Şahin H et al. The prevalence of sacroileitis in patients with acne vulgaris using isotretinoin. Cutan Ocul Toxicol. 2017;36:176–179. 14 Neurologic Side Effects Evren Burakgazi-Dalkilic Introduction Idiopathic Intracranial Hypertension Oral retinoids have been used in the treatment of refractory acne and some other dermatoses for decades. Retinoids have an important role in cell growth, maturation, differentiation, and apoptosis in central nervous system. In addition to systemic side effects of retinoids and hypervitaminosis, adverse effects on the central and peripheral nervous system have been well documented. This chapter will focus on the adverse effects of retinoids on central and peripheral nervous system and muscles. Vitamin A is a retinol with a hydrocarbon chain containing isoprenoid with a hydroxyl group at one end. It is available in both vegetarian (provitamin A) and animal diets (1–3). β-carotene is the leading source of vitamin A in vegetables, and retinol esters occur in animals (4,5). After absorption through the gut, retinol and retinoids must bind to proteins to be soluble in the blood and cytosol (6). Vitamin A plays essential roles in the regulation of cell proliferation, differentiation, and maturation leading to organogenesis (7–11). Retinoids are either natural or synthetic compounds with functional properties of vitamin A. Retinoid receptors are located in the cell nucleus, similar to steroids, vitamin D, and thyroid hormone receptors (12). Alterations in DNA transcription is the primary mechanism of their biologic effects. In binding to the regulatory regions of DNA, they modify the transcription of many genes. Retinoids may affect cell growth and differentiation, immunomodulation, tumor promotion, and malignant potential of cells (13). Retinoids are known to exert pleiotropic effects on the development, differentiation, and metabolism of skeletal muscle cells, with a possible mechanism through the induction of oxidative stress (14). The main site of vitamin A storage in mammals is the liver, but it is also possible to find vitamin esters in adipose tissue (4). Oral retinoids (vitamin A derivatives) have been the mainline treatment option in the management of chronic severe dermatoses (16,17). Oral isotretinoin (13-cis retinoic acid) is a first-­generation retinoid. It has been widely used as a first-line medication in the systemic treatment of severe acne and rosacea (18). Oral acitretin is a second-generation retinoid and considered to be useful in the management of severe psoriasis and other keratinization disorders (19,20). Consumption of vitamin A and vitamin A−related pharmacologic therapies may elevate cerebrospinal fluid (CSF) pressure in adults (21–25). One proposed theory about how retinoids lead to idiopathic intracranial hypertension (IIH) is related to the change in genetic expression of arachnoid cap cells and an associated decrease in absorption of CSF by arachnoid villi (26). Because retinol is hydrophobic, it needs to be carried by retinol-binding protein (RBP) and transthyretin (TTR) in systemic circulation and CSF. TTR and RBP are produced abundantly in the choroid plexus. After uptake of retinol into the cell, it is metabolized into retinaldehyde and then to all-trans-retinoic acid (ATRA). The meninges and choroid plexus are thought to be the primary sites of ATRA production in the adult brain. It is known that retinoic acid may also induce expression of aquaporin-4 in vitro, and aquaporin-4 null mice have raised intracranial pressure and ventricular dilation. Aquaporin-4 may be found in ependyma and astrocytes, and there is evidence that these cells take up CSF, possibly balancing the role of ­aquaporin-1 in the production of CSF in the choroid plexus (27). Vitamin A is fat-soluble, adipose tissue actively involved in retinoid homeostasis. Therefore body mass index (BMI), as a reflection of fat deposition, correlates positively with the risk of IIH (25,26). A review of 331 case reports of ocular side effects associated with retinoids (isotretinoin, etretinate, acitretin) found 21 cases of intracranial hypertension. It is important to note that six of these patients were using tetracycline or minocycline antibiotics, which are possible instigators of intracranial hypertension (28). Patients on retinoids should still be counseled for the signs and symptoms of IIH (headache, diplopia, nausea, vomiting). If IIH is suspected, ophthalmoscopic examination can be done to evaluate for papilledema. If it is present the retinoid should be discontinued. Systemic retinoids should not be taken concomitantly with tetracycline class antibiotics. Cranial Neuropathies Diplopia and strabismus have been reported in several patients taking retinoids, including acitretin. Oculomotor dysfunctions 79 80 were most often due to cranial sixth nerve palsy (29–31). It is not clear whether sixth nerve palsy occurred due to a direct effect of isotretinoin and acitretin or as a consequence of IIH (31). Given the high frequency of cranial sixth nerve palsy in the general population of IIH, a clear, definite causal relationship between sixth nerve palsy and systemic retinoid treatment may be difficult to establish. Myalgias/Myopathies Myalgias, muscle tenderness, and stiffness may be associated with the use of retinoids. Co-administration of other myotonic medications and heavy exertion as in physical training may increase the risk of muscle damage. Frequently, these manifestations are accompanied by elevated creatine phosphokinase levels with or without evidence of myopathy. Such muscle effects have been reported with isotretinoin and acitretin therapy (32–37). Severe and potentially life-threatening adverse effect on muscles, namely acute rhabdomyolysis, has been reported with use of oral isotretinoin. It is characterized by generalized muscle pain, fatigue, profound weakness, a fivefold or more significant increase in serum CPK levels, and myoglobinuria (32–35). Although true myopathy is a rare side effect of retinoids, few cases have been reported with use of isotretinoin and acitretin (36,37). The most commonly reported findings are weakness, muscle pain, stiffness, and fatigue. The diagnosis was confirmed with needle electromyography, and a muscle biopsy demonstrated variation and decrease in the size of muscle fibers. With discontinuation of the retinoid, patients had full recovery, most often within 1–2 months following drug discontinuation. Stiff-Person Syndrome Stiff-person syndrome (SPS) is a rare disorder of unknown etiology. SPS is characterized by muscle rigidity and intermittent spasms involving the axial and limb muscles. Clinical diagnostic features of SPS are axial and proximal extremity muscle stiffness, painful muscle cramps, lumbar hyperlordosis, and continuous firing of normal motor unit potentials that can be suppressed by diazepam on electromyography. In 60%–70% of patients, antibodies against glutamic acid decarboxylase (GAD) are present. Due to the presence of GAD antibodies and other autoantibodies such as anti-amphiphysin antibodies, SPS has been associated with autoimmune and paraneoplastic disorders (38). Because gamma aminobutyric acid (GABA) is the major inhibitory neurotransmitter in the nervous system, decrease in GABA concentrations induced by the anti-GAD antibodies will lead to increased muscle excitability and hyperactivity observed in SPS. In cases of SPS caused by retinoids, significant improvement was reported after discontinuation of isotretinoin treatment (39). SPS has not been reported with use of acitretin. Retinoids in Dermatology Peripheral Neuropathies Prospective and retrospective studies demonstrated neurotoxicity of isotretinoin and acitretin on peripheral nerves. Neurophysiologic evaluations of the patients were consistent with distal sensory neuropathy, mainly with axonal features. Occasional patients were found to have demyelinating f­ eatures. In most instances, symptoms of neuropathy began about 2–3 months after the initiation of retinoids (40–43). In the majority of cases, patients experienced cessation of symptoms after discontinuation of retinoids. There have been two known patients who developed Guillain-Barré syndrome (GBS) in temporal relationship to oral isotretinoin treatment (15,44). Conclusions Monitoring of these adverse effects is critical, because the adverse effects associated with retinoids are generally reversible upon discontinuation of treatment. Before treatment, patient counseling about expectations from treatment and possible adverse side effects is essential. Detailed informed consent should be obtained. Careful monitoring of possible adverse effects by clinical history, physical examination, and laboratory studies are essential to improve clinical outcomes and minimize potential adverse events. REFERENCES 1. Olson J. Vitamin A. Present Knowledge in Nutrition. The Nutrition Foundation, Washington, DC, 1993; pp. 176–191. 2. Napoli JL. Retinoic acid: Its biosynthesis and metabolism. Prog Nucleic Acid Res Mol Biol. 1999;63:139–188. 3. Napoli JL. Physiological insights into all-trans-retinoic acid biosynthesis. Biochim Biophys Acta. 2012;821:152–167. 4. Van Loo-Bouwman CA, Naber TH, Schaafsma GG. A review of vitamin A equivalency of β-carotene in various food matrices for human consumption. Br J Nutr. 2014;111:2153–2166. 5. Von Lintig J. Provitamin A metabolism and functions in mammalian biology. Am J Clin Nutr. 2012;96:1234–1244. 6. Noy N. Retinoid-binding proteins: Mediators of retinoid action. Biochem J. 2000;348:481–495. 7. Iskunov A, Al Tanoury Z, Rochette-Egly C. Nuclear and extra-nuclear effects of retinoid acid receptors: How they are interconnected. Subcell Biochem. 2014;70:103–127. 8. Das BC, Thapa P, Karki R et al. Retinoic acid signaling pathways in development and diseases. Bioorg Med Chem. 2014;22:673–683. 9. Rochette-Egly C. Retinoic acid signaling and mouse embryonic stem cell differentiation: Cross-talk between genomic and non-genomic effects of RA. Biochim Biophys Acta. 2015;1851:66–75. 10. Zetterstrom RH, Lindqvist E, Mataq de Urquiza A et al. Role of retinoids in the CNS: Differential expression of retinoid binding proteins and receptors and evidence for presence of retinoic acid. Eur J Neurosci. 1999;11:407–416. 11. Maden M. Role and distribution of retinoic acid during CNS development. Int Rev Cytol. 2001;209:1–77. Neurologic Side Effects 12. Kawaguchi R, Yu J, Honda J et al. A membrane receptor for retinol binding protein mediates cellular uptake of vitamin A. Science. 2007;315:820–825. 13. Xiao Y, Grieshammer U, Rosenthal N. Regulation of a muscle transgene by retinoic acid. J Cell Biol. 1995;129:1345–1354. 14. Amengual J, Ribot J, Bonet ML et al. Retinoic acid treatment increases lipid oxidation capacity in skeletal muscle of mice. Obesity. 2008;16:585–591. 15. Van Doorn PA. What’s new in Guillain-Barré syndrome in 2007–2008? J Peripher Nerv Syst. 2009;14:72–74. 16. Tsambaos D. Retinoids: A new chapter in dermatotherapy. Derm Beruf Umwelt. 1996;44:182–183. 17. Goldfarb MT, Ellis CN. The uses of retinoids in dermatology. Curr Opin Dermatol. 1997;4:236–240. 18. Ruzicka T, Larsen FG, Galewicz D et al. Oral alitretinoin (9-cis-retinoic acid) therapy for chronic hand dermatitis in patients refractory to standard therapy: Results of a randomized, double-blind, placebo-controlled, multicenter trial. Arch Dermatol. 2004;140:1453–1459. 19. McNamara IR, Muir J, Galbraith AJ. Acitretin for prophylaxis of cutaneous malignancies after cardiac transplantation. J Heart Lung Transplant. 2002;21:1201–1205. 20. Kuan YZ, Hsu HC, Kuo TT et al. Multiple verrucous carcinomas treated with acitretin. J Am Acad Dermatol. 2007;56:29–32. 21. Markey KA, Mollan SP, Jensen RH, Sinclair AJ. Understanding idiopathic intracranial hypertension: Mechanisms, management, and future directions. Lancet Neurol. 2016;15:78–91. 22. Mollan SP, Ali F, Hassan-Smith G et al. Evolving evidence in adult idiopathic intracranial hypertension: Pathophysiology and management. J Neurol Neurosurg Psychiatry. 2016;87: 982–992. 23. Gerber A, Raab AP, Sobel AE. Vitamin A poisoning in adults; with description of a case. Am J Med. 1954;16:729–745. 24. Fraunfelder FW, Fraunfelder FT. Evidence for a probable causal relationship between tretinoin, acitretin, and etretinate and intracranial hypertension. J Neuroophthalmol. 2004;24: 214–216. 25. Fraunfelder FW, Fraunfelder FT, Corbett JJ. Isotretinoinassociated intracranial hypertension. Ophthalmology. 2004;111:1248–1250. 26. Noy N, Xu ZJ. Interactions of retinol with binding proteins: Implications for the mechanism of uptake by cells. Biochemistry. 1990;29:3878–3883. 27. Bloch O, Auguste KI, Manley GT, Verkman AS. Accelerated progression of kaolin-induced hydrocephalus in aquaporin-4-deficient mice. J Cereb Blood Flow Metab. 2006;26(12):1527–1537. 81 28. Libien J, Blaner WS. Retinol and retinol-binding protein in cerebrospinal fluid: Can vitamin A take the “idiopathic” out of idiopathic intracranial hypertension? J Neuroophthalmol. 2007;27:253–257. 29. Fraunfelder ET, Fraunfelder FW, Edwards R. Ocular side effects possibly associated with isotretinoin usage. Am J Ophthalmol. 2001;132:299–305. 30. Arnault J-P, Petitpain N, Granel-Brocard F et al. Acitretin and sixth nerve palsy. J Eur Acad Dermatol Venereol. 2007;21:1258–1259. 31. Rush JA, Younge BR. Paralysis of cranial nerves III, IV, and VI: Cause and prognosis in 1000 cases. Arch Ophthalmol. 1981;99:76–79. 32. Hodak E, Gadoth N, David M et al. Muscle damage induced by isotretinoin. Br Med J. 1986;293:425–426. 33. Kaymak Y. Creatine phosphokinase values during isotretinoin treatment for acne. Int J Dermatol. 2008;47:398–401. 34. Landau M, Mesterman R, Ophir J et al. Clinical significance of markedly elevated serum creatine kinase levels in patients with acne on isotretinoin. Acta Derm Venereol. 2001;81:350–352. 35. Trauner MA, Ruben BS. Isotretinoin-induced rhabdomyolysis? A case report. Dermatol Online J. 1999;5:2. 36. Fiallo P, Tagliapietra A-G. Severe acute myopathy induced by isotretinoin. Arch Dermatol. 1996;132:1521–1522. 37. Lister RK, Lecky BRF, Lewis-Jones MS et al. Acitretininduced myopathy. Br J Dermatol. 1996;134:989–990. 38. Dalakas MC, Li M, Fujii M, Jacobowitz DM. Stiff person syndrome. Quantification, specificity, and intrathecal synthesis of GAD65 antibodies. Neurology. 2001;57:780–784. 39. Chroni E, Sakkis T, Georgiou S et al. Stiff-person syndrome associated with oral isotretinoin treatment. Neuromuscul Disord. 2002;12:886–888. 40. Chroni E, Pasmatzi E, Monastrili A et al. Short-term oral isotretinoin therapy does not cause clinical or subclinical peripheral neuropathy. J Dermatolog Treat. 2006;17:6–8. 41. Aydogan K, Karli N. Effects of oral isotretinoin therapy on peripheral nerve functions: A preliminary study. Clin Exp Dermatol. 2007;32:81–84. 42. Chroni E, Georgiou S, Monastirli A et al. Effects of shortterm oral acitretin therapy on peripheral nerve function: A prospective neurological and neurophysiological study. Acta Derm Venereol. 2001;81:423–425. 43. Tsambaos D, Sakkis T, Chroni E et al. Peripheral sensory neuropathy associated with short-term oral acitretin therapy. Skin Pharmacol Appl Skin Physiol. 2003;16:46–49. 44. Pritchard J, Appleton R, Howard R, Hughes RA. Guillain-Barré syndrome seen in users of isotretinoin. BMJ. 2004;328:1537. 15 Psychiatric Side Effects Joshua Schimmel, Evren Burakgazi-Dalkilic, and Hatice Burakgazi-Yilmaz Introduction Acne is the most common skin condition among adolescents. For mild and moderate disease, the first-line treatments may include topical retinoids and antimicrobials; however, for severe nodulocystic or recalcitrant acne, systemic retinoids are often required. Systemic retinoids are also used in severe cases of psoriasis. Topical retinoids have few significant adverse effects; however, the systemic forms can adversely affect many organ systems. The most common untoward effects include dry eyes, skin, and lips, facial erythema, increased serum triglycerides, and back pain (1,2). Neuropsychiatric effects are far less common but have been a highly controversial topic since the first oral retinoid, isotretinoin, was introduced in 1982 (3). History of Isotretinoin Isotretinoin was the first retinoid used in the treatment of recalcitrant acne vulgaris. Just 1 year after its release in 1982, a case series of 24 patients with acne treated with isotretinoin who developed depressive symptoms after drug initiation was reported. Many clinicians were skeptical of the results; however, over the next few years, several more reports were published showing an association between isotretinoin and adverse psychiatric disorders (3,4). In 1998, the US Food and Drug Administration (FDA) changed the warning label on the medication to include depression, psychosis, suicide ideation, suicide attempt, and suicide; however, since this warning was added, there has been a major controversy over the psychiatric side effects of isotretinoin. Neurobiology of Retinoids While there is no definitive proof of a causal relationship between retinoids and psychiatric effects, there are many well-supported theories on how retinoids structurally and functionally affect the brain. Retinoic acid (RA), a metabolite of vitamin A, is a biologic molecule found naturally in the human body, essential for cell growth and differentiation in many tissues, including the brain (6). RA binds to receptors in the brain, eliciting changes in gene transcription and neuronal protein expression. A detailed signaling pathway of RA can be found in Figure 15.1. Retinoids are a family of compounds derived from vitamin A and are structurally like RA. Isotretinoin is identical to RA other than the geometry of its double bond. Isotretinoin has a cis configuration, while RA is trans; however, there is evidence that the cis conformation of isotretinoin is isomerized to trans-RA in human tissues (7). Isotretinoin and other retinoids likely have similar effects on brain function and growth as RA. High concentrations of retinoic acid receptors (RAR) in the brain are found in the limbic system (6,8), the part of the brain responsible for motivation, emotion, learning, and memory. The hippocampus, prefrontal cortex, and striatum are all parts of the limbic system affected in depression, anxiety, bipolar disorder, suicide, and psychosis (9). The most widely accepted and supported mechanisms for the effects of RA on these regions of the brain are discussed. One mechanism by which the hippocampus is thought to be involved in mood regulation is through inhibition of neurogenesis by RA. Treatment of mice with 13-cis RA led to a decrease in the rate of hippocampal cell birth in multiple studies (10,11). Conversely, a separate study found significantly vitamin A-deficient rats had impairment of hippocampal long-term potentiation (11). These findings imply that both high and low levels of RA may impair hippocampal function, which could explain why some studies demonstrate worsening depression with RA treatment and others show improved depressive symptoms (5,12). Perhaps a study measuring vitamin A levels pre- and post-treatment is warranted. The effects of RA on dopamine within the striatum may also play a role in alterations in mood and emotion. Abnormal dopaminergic transmission is well known to play a role in depression and psychosis. Alterations in dopamine signaling could be due to decreased presynaptic release or impaired signal transduction (13). RA has been proven to increase dopamine signal transduction through the induction of various proteins in the developing striatum (14). Assuming these effects can be applied to the adult brain, this would indicate that RA has a role in improving dopaminergic transmission. This evidence supports the argument that RA may diminish depression rather than worsen it; however, the important consideration is the association RA has in a system proven to be central to the etiology of depression. Increased levels of dopaminergic signaling are found in patients with schizophrenia and psychosis, suggesting that improved dopaminergic transmission in the striatum could also explain the many reports of psychosis seen with retinoid treatment. 83 84 Retinoids in Dermatology FIGURE 15.1 Retinoid and retinoic acid signaling pathway. Retinol, bound to retinol-binding protein (RBP) and transthyretin (TTR), circulates in the blood. It binds to the transmembrane receptor STRA6 of target cells and is transported into the cytoplasm. Here, retinol binds cellular retinol binding proteins (CRBP) for stability. Retinol can then be oxidized to retinaldehyde in a reversible reaction mediated by an alcohol or retinol dehydrogenase (ADH/ RDH). Retinaldehyde is then irreversibly converted to retinoic acid by an aldehyde dehydrogenase (ALDH). RA may then either be transported to an adjacent cell, the extracellular space or into the nucleus by cellular retinoic acid binding proteins (CRABPs). Once in the nucleus, RA will bind to RA receptors (RAR) bound to retinoic acid response elements on DNA. Alternatively, in the cytoplasm, RA can be degraded into 4-oxo retinoic acid by cytochrome p 450 proteins (CYP26). (Created by author; data from Bremner JD et al. J Clin Psychiatry. 2012;73:37–50.) The prefrontal cortex is the anterior region of the frontal lobe responsible for personality, decision making, and controlling social behaviors. Individuals who suffer damage to this region typically experience significant dysregulation of emotional responses and goal-directed behavior. Both MRI studies and postmortem examination have found reduced volume and density of neurons in the orbitofrontal cortex, a region of the prefrontal cortex, among patients with major depression (9,15). Increased metabolism of the orbitofrontal lobe has been seen in patients with obsessive-compulsive disorder (OCD) (16). RA has been shown to affect the executive networks found in the frontal cortex of adult rat brains (17). Retinoid treatment could alter neuronal functioning in the prefrontal cortex and may be responsible for the psychiatric effects seen with therapy. A 2005 study (18) assessed the effects of isotretinoin on brain function using PET FDG imaging of brain metabolism. The study demonstrated a significant decrease in brain metabolism in the orbitofrontal cortex among subjects treated with isotretinoin versus antibiotics alone. No differences in the severity of depressive symptoms were found between groups. Despite being a small study (n = 28), it was the first study to show a quantifiable change in neuronal functioning among patients receiving retinoid treatment. The effect RA has on the brain is complex and not well understood. Retinoids most likely do not affect just one pathway or region of the brain. Any psychiatric effects seen from retinoid treatment are likely due to dysregulation of multiple regions of the brain, responsible for controlling emotion and behavior. If there is an exact link between retinoids and psychiatric disturbances, future studies will have to decide this. The Psychiatric Effects of Isotretinoin in Patients with Depressive Disorder and Suicidality Depression and suicide are the most well-studied side effects of isotretinoin treatment; yet, definitive proof of an association is still not clear. There have been large, comprehensive reviews published within the past few years that shine new light on the subject (5,19). Perhaps the most recent and well-supported evidence can be found in a 2017 systematic review and meta-analysis (5). The study analyzed 31 different reports on psychiatric effects seen with isotretinoin treatment. Of these 31, 6 were randomized controlled trials (RCT) and the rest were a combination of large-scale population-based studies, non-RCT, and prospective open-label studies. The review found 12 studies which failed to 85 Psychiatric Side Effects demonstrate an increased risk of depression or suicide with the drug. In fact, the authors found 11 studies which showed lessening of depression with isotretinoin treatment. The authors attribute this improvement to a more positive self-image following resolution of the acne. Conversely, the review only found 3 studies which showed worsening depression or suicide with treatment. The overall results of the meta-analysis of 31 studies showed no significant association with isotretinoin treatment and increased risk of depression (5). A separate 2018 review (12) demonstrated similar findings. While this review did not perform a meta-analysis, the authors reviewed 24 studies which included 4 case reports/ series, 3 database, 5 retrospective, and 12 prospective studies. Overall, either no association or, in some studies, improvement of depressive symptoms with isotretinoin treatment was found in prospective studies reviewed. Interestingly, the review reported an association between isotretinoin and depression in case reports, database studies, and retrospective studies (12). Despite comprehensive evidence from these two well-conducted systematic reviews, the effects of isotretinoin on depression and suicide remain unclear. It is possible the ambiguity of evidence may be due to the association of acne alone with adverse psychiatric side effects. There is evidence showing severe acne is associated with depression and suicide (20). Discerning if mood changes in patients with severe acne are a side effect of the medication or the disease itself is challenging. Resolution of severe acne findings with isotretinoin treatment may improve depressive symptoms; however, patients with a history of mental disorders or genetic predisposition may experience worsened depression despite symptom resolution (12). Another contributing factor to the controversy may be the temporal and dose-related correlation with psychiatric side effects and isotretinoin treatment. Patients on isotretinoin therapy who experience depression and suicide rarely develop these symptoms immediately, but 1–2 months after starting therapy (21). There is evidence that higher doses of isotretinoin correlate with increased cases of depression (21). As a result, the timing of studies and differences in patient dosages could have a significant impact on the measured association between isotretinoin and psychiatric side effects. Even with the overwhelming number of studies on this topic, there have been no high-quality studies to confirm the causal relationship (21,22). A large double-blind placebo-controlled study would be useful in establishing a relationship; however, in 2002 the FDA argued it would be too difficult to perform an adequately blinded study due to the blatant mucocutaneous adverse reactions subjects would experience (23). The superior efficacy of isotretinoin over antimicrobials causes ethical concerns when randomizing treatment arms. A 2018 feasibility study showed a successful design for a triple-blind RCT investigating the effects of isotretinoin on mood. The study demonstrates that patients will accept randomization with isotretinoin and antimicrobials despite the superior efficacy of isotretinoin (24). A high-quality study explaining the association of isotretinoin with depression and suicide is likely to be on the horizon. The Psychiatric Effects of Isotretinoin in Patients with Bipolar Disorders The psychiatric effects of isotretinoin in patients with bipolar disorder are limited to very few studies. To the authors’ knowledge, the largest study to date is a 2010 retrospective chart review of 10 patients with bipolar disorder treated with isotretinoin (25). The study found 9 of the 10 patients experienced worsening symptoms, 8 of which had a reversal of symptoms upon discontinuation of the drug. In addition, 3 patients experienced suicidal ideations. This study shows that patients with bipolar disorder are at risk for significant mood dysregulation upon treatment with isotretinoin. Because acne is a side effect of lithium treatment, patients with bipolar disorder often receive isotretinoin treatment. This study is limited by sample size and retrospective design; thus more studies are necessary to confirm the effects of isotretinoin treatment in bipolar disorder. Despite this, it is important that dermatologists consider the possibility of mood dysregulation when treating this patient population. The Psychiatric Effects of Isotretinoin in Patients with Anxiety Disorders The association between isotretinoin and anxiety disorders is not well understood. Most studies on the topic demonstrate improved anxiety following treatment. A 2013 prospective observational study of 364 patients with moderate acne found improvement in anxiety and depression using the Hospital Anxiety and Depression Scale (HADS) as a measurement tool (26). A separate prospective study of 43 patients with acne vulgaris found improved HADS scores with isotretinoin treatment (27). While most studies demonstrate lessening of anxiety symptoms, there have been case reports of patients developing panic attacks following initiation of isotretinoin treatment (28,29). In all of these case reports, attacks ceased once isotretinoin was discontinued, and there was no personal or family history of panic attacks. While it appears isotretinoin may improve anxiety, clinicians should monitor patients for panic attacks after isotretinoin initiation. The Psychiatric Effects of Isotretinoin in Patients with Obsessive-Compulsive Disorders Systemic retinoids have been thought to worsen obsessivecompulsive symptoms; however, the evidence on the topic is very limited. There has been one prospective study of 43 patients without a prior diagnosis of OCD who developed worsening obsessive-compulsive symptoms based on the Madsely Obsessive Compulsive Questionnaire (27). Large, controlled studies of OCD and isotretinoin treatment are necessary for a definitive conclusion to be made. The Psychiatric Effects of Isotretinoin in Patients with Psychosis Evidence for an association between isotretinoin and psychosis is found in several reported cases of hypervitaminosis A associated with psychotic symptoms (21). Because retinoic acid is a metabolite of vitamin A, it is reasonable to believe an association may exist. A 2005 study (30) of 500 soldiers being treated with isotretinoin reported 5 patients who developed manic psychosis within 8 months of drug initiation; however, these findings are questionable, considering a history of OCD, neurologic insult, or family history of psychiatric illnesses, were present in all cases. 86 Several other studies have demonstrated similar findings, suggesting an association between psychosis and systemic retinoid treatment is likely in some individuals (31,32). The Psychiatric Effects of Other Systemic Retinoids Some authors argue other systemic retinoids could have similar psychiatric effects as isotretinoin due to their similar structure (21). Other systemic retinoids include etretinate, acitretin, alitretinoin, bexarotene, and all-trans-retinoic acid. There have been case reports of adverse psychiatric events with these retinoids. Similar to isotretinoin, the most common case reports of psychiatric disturbances are related to depression and suicide (33). There are also reports of panic attack, delirium, schizophreniform disorder, body dysmorphic disorder, and behavioral disorders (33). However, unlike isotretinoin, there have been no formal studies on the association between psychiatric adverse events and other systemic retinoid treatments. Regardless, clinicians should consider the possibility of psychiatric disturbances when prescribing any systemic retinoid until future studies provide more clarification. Management Systemic retinoids are used to treat severe, recalcitrant acne. These drugs influence cell cycle progression and differentiation, reduce sebaceous gland size, inhibit new comedogenesis, reduce growth of Propionibacterium acnes, and decrease inflammation (34). No other medications have been shown to treat all these etiologic causes of acne. As a result, systemic retinoids have become the treatment of choice for recalcitrant acne, despite their adverse side effect profile. With the inconclusive evidence surrounding the psychiatric effects of systemic retinoids, a clear association exists in some predisposed individuals, especially those with a history of mood disorders. Dermatologists should consider referring a patient to a mental health professional if any psychiatric changes are noted after a patient has initiated therapy. A personal or family history of depression or mental illness is not a contraindication to starting treatment (35). Patients with such a history should be monitored closely for any suicidal thoughts or worsening depressive symptoms after starting systemic therapy. If psychiatric symptoms develop, discontinuation of the medication should be considered depending on severity. Conclusions The controversy surrounding the psychiatric effects of systemic retinoids has been ongoing for over 30 years. The most current evidence shows no association between isotretinoin use and depression or suicide. In fact, treatment of acne more often lessens symptoms of depression. Further studies are necessary for a definitive conclusion to be made on the psychiatric effects of isotretinoin in bipolar and anxiety disorders as well as OCD and psychosis. There is limited evidence on the psychiatric effects of systemic retinoids other than isotretinoin, but several Retinoids in Dermatology case reports suggest the effects are like those seen with isotretinoin. It is clear that some patients are more prone to worsening psychiatric symptoms when starting systemic retinoids, thus closely monitoring patients for changes in mood or behavior is recommended. REFERENCES 1. Lee JW, Yoo KH, Park KY et al. Effectiveness of conventional, low-dose and intermittent oral isotretinoin in the treatment of acne: A randomized, controlled comparative study. Br J Dermatol. 2011;164:1369–1375. 2. McLane J. Analysis of common side effects of isotretinoin. J Am Acad Dermatol. 2001;45:188–194. 3. Strahan JE, Raimer S. Isotretinoin and the controversy of psychiatric adverse effects. Int J Dermatol. 2006;45:789–799. 4. Bruno NP, Beacham BE, Burnett JW. Adverse effects of isotretinoin therapy. Cutis. 1984;33:484–486, 489. 5. Huang YC, Cheng YC. Isotretinoin treatment for acne and risk of depression: A systematic review and meta-analysis. J Am Acad Dermatol. 2017;76:1068–1076. 6. Luo T, Wagner E, Grün F, Dräger UC. Retinoic acid signaling in the brain marks formation of optic projections, maturation of the dorsal telencephalon, and function of limbic sites. J Comp Neurol. 2004;470:297–316. 7. Tsukada M, Èder MS, Roos TC et al. 3-Cis retinoic acid exerts its specific activity on human sebocytes through selective intracellular isomerization to all-trans retinoic acid and binding to retinoid acid receptors. J Invest Dermatol. 2000;115:321–327. 8. Bremner JD, McCaffery P. The neurobiology of retinoic acid in affective disorders. Prog Neuro Psychopharmacol Biol Psychiatry. 2008;32:315–331. 9. Bremner JD, Vythilingam M, Vermetten E et al. Reduced volume of orbitofrontal cortex in major depression. Biol Psychiatry. 2002;51:273–279. 10. Crandall J, Sakai Y, Zhang J et al. 3-Cis-retinoic acid suppresses hippocampal cell division and hippocampaldependent learning in mice. Proc Natl Acad Sci USA. 2004;101:5111–5116. 11. Misner DL, Jacobs S, Shimizu Y et al. Vitamin A deprivation results in reversible loss of hippocampal long-term synaptic plasticity. Proc Natl Acad Sci USA. 2001;98:11714–11719. 12. Oliveira JM, Sobreira G, Velosa J et al. Association of isotretinoin with depression and suicide: A review of current literature. J Cutan Med Surg. 2018;22:58–64. 13. Dunlop BW, Nemeroff CB. The role of dopamine in the pathophysiology of depression. Arch Gen Psychiatry. 2007;64:327–337. 14. Wang H-F, Liu F-C. Regulation of multiple dopamine signal transduction molecules by retinoids in the developing striatum. Neuroscience. 2005;134:97–105. 15. Rajkowska G, Miguel-Hidalgo JJ, Wei J et al. Morphometric evidence for neuronal and glial prefrontal cell pathology in major depression. Biol Psychiatry. 1999;45:1085–1098. 16. Rauch SL, Jenike MA, Alpert NM et al. Regional cerebral blood flow measured during symptom provocation in obsessive-compulsive disorder using oxygen 15-labeled carbon dioxide and positron emission tomography. Arch Gen Psychiatry. 1994;51:62–70. Psychiatric Side Effects 17. Wagner E, Luo T, Sakai Y et al. Retinoic acid delineates the topography of neuronal plasticity in postnatal cerebral cortex. Eur J Neurosci. 2006;24:329–340. 18. Bremner JD, Fani N, Ashraf A et al. Functional brain imaging alterations in acne patients treated with isotretinoin. Am J Psychiatry. 2005;162:983–991. 19. Roberto De Oliveira M. The neurotoxic effects of vitamin A and retinoids. An Acad Bras Cienc. 2015;1361–1373. 20. Halvorsen JA, Stern RS, Dalgard F et al. Suicidal ideation, mental health problems, and social impairment are increased in adolescents with acne: A population-based study. J Invest Dermatol. 2010;131:363–370. 21. Bremner JD, Shearer KD, McCaffery PJ. Retinoic acid and affective disorders. J Clin Psychiatry. 2012;73:37–50. 22. Kontaxakis VP, Skourides D, Ferentinos P et al. Isotretinoin and psychopathology: A review. Ann Gen Psychiatry. 2009;8:2. 23. Drug Safety and Availability—Isotretinoin (marketed as Accutane) Capsule Information. 2018. https://www.fda.gov/ Drugs/DrugSafety/ucm094305.htm 24. Rea S, Tucker S, Frittelli V, Gunnarsson R. A feasibility study for a triple-blind randomized controlled trial investigating the effects of oral isotretinoin on mood and quality of life in patients with acne vulgaris. Clin Exp Dermatol. 2018;43:54–56. 25. Schaffer LC, Schaffer CB, Hunter S, Miller A. Psychiatric reactions to isotretinoin in patients with bipolar disorder. J Affect Disord. 2010;122:306–308. 87 26. Marron S, Tomas-Aragones L, Boira S. Anxiety, depression, quality of life and patient satisfaction in acne patients treated with oral isotretinoin. Acta Derm Venereol. 2013;93:701–706. 27. YesIlova Y, Bez Y, ArI M et al. Effects of isotretinoin on obsessive compulsive symptoms, depression, and anxiety in patients with acne vulgaris. J Dermatolog Treat. 2012;23:268–271. 28. Poblete AC, Herskovic MV, Eva CP. [Panic attacks in a patient treated with isotretinoin for acne. Report of one case]. [Article in Spanish] Rev Med Chil. 2006;134:1565–1567. 29. Alcalá Partera JA. Depression and panic attack in acne treated with isotretinoin. Semergen. 2012;38:188–191. 30. Barak Y, Wohl Y, Greenberg Y et al. Affective psychosis following Accutane (isotretinoin) treatment. Int Clin Psychopharmacol. 2005;20:39–41. 31. Ludot M, Mouchabac S, Ferreri F. Inter-relationships between isotretinoin treatment and psychiatric disorders: Depression, bipolar disorder, anxiety, psychosis and suicide risks. World J Psychiatry. 2015;5:222–227. 32. Rajagopal S. Acute psychosis induced by isotretinoin. Indian J Psychiatry. 2014;56:295–297. 33. Le Moigne M, Fournier J-P, Bulteau S et al. Psychiatric disorders with systemic retinoids: A systematic review of case reports. Br J Dermatol. 2018;178:278–280. 34. Layton A. The use of isotretinoin in acne. Dermatoendocrinol. 2009;1:162–169. 35. Prevost N, English JC. Isotretinoin: Update on controversial issues. J Pediatr Adolesc Gynecol. 2013;26:290–293. 16 Gastrointestinal Side Effects Esra Adışen, Burcu Beksaç, and Mehmet Ali Gürer Introduction Retinoic acid receptors are widely distributed throughout the body, and systemic retinoid treatment is associated with several adverse effects, most of which are dose-dependent and reversible (1,2). They are metabolized in the liver and excreted through renal and hepatic routes (3,4). Although not as common as mucocutaneous side effects, systemic retinoid treatment may lead to gastrointestinal adverse events. Among the rare side effects of systemic retinoids, nausea, vomiting, abdominal pain, weight loss, anorexia, esophagitis, gastritis, colitis, hepatitis, elevated liver function tests, and cirrhosis have been described (1,2). Notably, topical retinoids do not cause gastrointestinal side effects. Elevated Liver Enzymes/Hepatotoxicity Systemic retinoids may cause transient elevation of liver enzymes in a dose-dependent manner in about one-third of the patients treated (5). The elevation is transient and usually subsides with dose reduction or after drug discontinuation (1). Severe hepatotoxic reactions due to retinoid treatment are rare and of idiosyncratic nature (6). Data on Hepatotoxicity of Acitretin Data including 1877 patients receiving oral acitretin revealed chemical hepatitis in only 0.26% (5). In another study evaluating hepatotoxicity through pre- and post-treatment histopathologic examination of liver biopsies on 128 patients, 83% improvement or no deterioration in liver pathology during treatment with acitretin was reported (5). In a real-life study involving 41 patients on acitretin treatment, 9.8% had elevated AST/ALT and 7.3% had elevated gamma-glutamyl transpeptidase levels, which resolved after dose reduction or drug discontinuation (7). A case of severe hepatotoxicity leading to liver cirrhosis caused by acitretin treatment was reported in 1990 (6). isotretinoin and control groups, abnormal blood tests including liver enzyme and serum lipid levels represented only 2% of the adverse events related to isotretinoin. Two patients (0.5%) randomized to isotretinoin withdrew from trials included in this systematic review due to elevated liver enzymes (9). To date, no cases with irreversible hepatotoxicity due to isotretinoin treatment have been reported (10). Patients receiving acitretin should be routinely monitored for their liver function tests. An initial evaluation followed by testing at 1- to 2-week intervals until stable, then at clinically indicated intervals, is recommended for acitretin (3). Recent reports suggest that in healthy patients with normal baseline lipid panel and liver function test results, repeated studies should be performed after 2 months of isotretinoin therapy. If findings are normal, no further testing should be required (11,12). In cases of abnormal liver function tests at the baseline or after the second month control, more frequent monitoring is recommended (11). Concurrent use of systemic retinoids with other hepatotoxic drugs and alcohol should be avoided if possible, and in cases of concurrent use, more frequent laboratory monitoring might be necessary. Alcoholics, diabetics, and obese patients have a higher risk of hepatotoxicity (4). Pancreatitis Another gastrointestinal adverse event related to systemic retinoid use is pancreatitis due to seriously elevated serum triglyceride levels, or as an idiosyncratic reaction without elevated serum triglycerides (12). This is a rare but serious adverse event, with potentially fatal results. A few case reports of pancreatitis induced during isotretinoin and acitretin treatment have been published (3,12–14). Diabetic, obese, and alcoholic patients are at a higher risk for increased serum triglycerides during systemic retinoid therapy. Elevated serum lipid levels should be controlled by dietary changes, dose reduction, or anti-hyperlipidemic drug treatment (4). Patients receiving systemic retinoids should be advised to promptly report signs and symptoms related to pancreatitis, including severe abdominal pain or emesis (5). Data on Hepatotoxicity of Isotretinoin In a study involving patients using systemic isotretinoin for acne treatment, 12.9% had elevation in ALT, 5.7% had elevation in AST, and 2.9% in GGT at any time during treatment (8). In a recent systematic review involving data from eleven randomized controlled trials and a total of 760 patients randomized into Gastrointestinal Discomfort and Nausea Acitretin may cause gastrointestinal upset and nausea in some patients. It is known to cause nausea in 1.7% of pediatric psoriasis patients (15). Nonspecific side effects, such as nausea, 89 90 diarrhea, constipation, and abdominal pain, have also been reported in patients on systemic isotretinoin (2,8). These adverse events will subside once treatment is completed, but gastrointestinal discomfort in general is not a cause for dose reduction or drug discontinuation. Rectal Bleeding Rectal hemorrhage was reported in one patient using acitretin, resulting from mucosal inflammation due to acitretin treatment (16). Anal fissuring and rectal bleeding may also occur during systemic isotretinoin therapy (17,18). In the reported patients, when the systemic retinoid treatment was discontinued the side effects subsided within a few weeks. When there is concern, a diet rich in fiber may be recommended to keep stools soft and thus reduce the possibility of rectal bleeding. Inflammatory Bowel Disease Another gastrointestinal side effect of systemic retinoids, especially isotretinoin, is a possible increase in the risk of flaring inflammatory bowel disease (IBD) in patients already diagnosed with IBD. The debate about isotretinoin and IBD is not a new issue. In 1983, the Dermatologic Drugs Advisory Committee of the US Food and Drug Administration (FDA), taking into account the reports of nine patients diagnosed with IBD during or after isotretinoin treatment, decided that it would be necessary to state the presence of isotretinoin-related IBD cases in the adverse event section of the drug insert (19). The first case report claiming a possible causal relationship between isotretinoin treatment and IBD was described in 1987 in a patient treated with acne vulgaris for 5 months and who subsequently developed ulcerative colitis (20). This adverse effect had not previously been found in the efficacy and safety studies of the drug (21). Since then, several case reports and case series have been published involving patients with exacerbations of previous IBD or the development of new IBD, which did or did not regress after drug discontinuation (21–25). There are also reports of patients who had had a diagnosis of IBD prior to isotretinoin treatment and with no change during treatment (26–29). There are no published reports of IBD associated with acitretin. There is a case control study pointing to a minimally increased risk of ulcerative colitis after isotretinoin use, and another study which depicted a strong correlation between isotretinoin and ulcerative colitis, but not Crohn’s disease (30,31). One of these studies was the only one in the literature suggesting an increased risk of IBD associated with higher isotretinoin doses (31); however, a 2014 study demonstrated a decreased risk of IBD in patients with isotretinoin exposure (32). A 2011 research commentary analyzed and compared prior case control studies about isotretinoin therapy and IBD. The authors observed that 2977 patients would need to be treated to find one patient with an ulcerative colitis (the “number needed to harm”) (33). In three other large studies, there was no increased risk of patients developing IBD when receiving isotretinoin in comparison with patients not exposed (34–36). An additional Retinoids in Dermatology study identified the existence of disproportionate attorney-initiated reporting of IBD associated with isotretinoin in the Food and Drug Administration Adverse Event Reporting system, with the conclusion that attorney-initiated reports inflated the pharmacovigilance signal of isotretinoin-induced IBD, presumably caused by a conflict of interest (37). In 2011, the American Academy of Dermatology published its Position Statement on Isotretinoin in which it reported that current evidence is insufficient to prove either an association or a causal relationship between isotretinoin use and IBD in the general population (38). Although the mechanism by which isotretinoin may induce IBD is unknown, there are some hypotheses, including inhibition of epithelial cell growth resulting in ulceration and inflammation of the gut mucosa, inhibition of glycoprotein synthesis affecting the integrity of the mucosal wall, and stimulation of killer T cells, leading to epithelial cell injury and a resultant inflammatory response. The proposed pathophysiologic mechanisms in isotretinoin induced IBD are as follows (21,36,39): 1. Disturbance of epithelial cell maturation resulting in inflammation and mucosal ulceration, alterations in glycoprotein metabolism compromising the colonic mucosal integrity, and induction of killer T-cell activity. 2. The immunomodulatory effects and role in lymphocyte migration in isotretinoin. Th17 and Treg cell formation is controlled by retinoic acid. Retinoic acid also induces integrins and chemokine receptors that result in abnormal lymphocyte migration to intestinal mucosa. 3. The phenotypic expression by colonic epithelial cells with retinoids, serving as a stimulus for an inflammatory response. 4. Effect of retinoids on neutrophil chemotaxis, which plays a key role in Crohn’s disease pathogenesis. These potential pathways remain theoretical and have not been directly studied in the case of IBD and isotretinoin. In addition, although the effect of isotretinoin on cutaneous glandular cells is well known, no alteration has been observed in intestinal Goblet cells of rectal biopsy specimens that were taken from IBD patients following isotretinoin use. There is little robust evidence supporting strong associations between specific medications and IBD incidence or disease activity. Because IBD is a markedly heterogenous disease, and it is likely that certain triggers are only relevant in certain patients, there are not convincing associations between medication use and IBD. Hypothetically, if isotretinoin were to cause IBD, the expected incidence of IBD among such patients would be still expected to be low, and prospective studies (either randomized, controlled trials, or prospective cohort studies) are not feasible owing to issues of cost and sample size. The most ideal retrospective format is a population-based study with the power to capture as many events as possible. There are three significant studies conducted in an effort to support or exclude a link between isotretinoin use and IBD. Two of these studies (35,36) reported no significant association between isotretinoin use and IBD; a third (31) supported an increased risk of ulcerative colitis with prior isotretinoin exposure. Gastrointestinal Side Effects Because there are no large-scale studies definitively depicting a causal relationship between isotretinoin and IBD, clinicians should not be discouraged from prescribing this medication in severe acne. Novel population-based studies are warranted to enlighten this subject (23,30,39). Conclusions While serious gastrointestinal side effects of retinoids are relatively rare, they should nevertheless be taken into consideration. Patients receiving acitretin should be routinely monitored with liver function tests. Severe hepatotoxicity is rare, and elevations in liver enzymes can usually be controlled by dose reduction or, if necessary, drug discontinuation. Pancreatitis is a very rare but potentially fatal adverse event associated with severely elevated serum triglyceride levels. Patients started on systemic retinoids should be advised to promptly report symptoms related to pancreatitis. Elevated serum lipid levels may be controlled by dietary changes, dose reduction, or antihyperlipidemic drug treatment. Acitretin may cause gastrointestinal upset and nausea in some patients, but this is not a cause for dose reduction or drug discontinuation. A diet rich in fiber to avoid constipation may be recommended to avoid rectal bleeding in patients using systemic retinoids. Although a direct causal relationship between isotretinoin use and inflammatory bowel disease has not been proven, patients should be cautioned prior to the therapy about promptly reporting abdominal symptoms that may occur during systemic isotretinoin treatment. REFERENCES 1. Subedi S, Yu Q, Chen Z et al. Management of pediatric psoriasis with acitretin: A review. Dermatol Ther. 2018;31. doi: 10.1111/dth.12571. 2. Charakida A, Mouser PE, Chu AC. Safety and side effects of the acne drug, oral isotretinoin. Expert Opin Drug Saf. 2004;3:119–129. 3. Lowenstein EB, Lowenstein EJ. Isotretinoin systemic therapy and the shadow cast upon dermatology’s downtrodden hero. Clin Dermatol. 2011;29(6):652–661. 4. Guenther LC, Kunynetz R, Lynde CW et al. Acitretin use in dermatology. J Cutan Med Surg. 2017;21:2S–12S. 5. Katz HI, Waalen J, Leach EE. Acitretin in psoriasis: An overview of adverse effects. J Am Acad Dermatol. 1999;41:S7–S12. 6. van Ditzhuijsen TJ, van Haelst UJ, van Dooren-Greebe RJ et al. Severe hepatotoxic reaction with progression to cirrhosis after use of a novel retinoid (acitretin). J Hepatol. 1990;11:185–188. 7. Chiricozzi A, Panduri S, Dini V et al. Optimizing acitretin use in patients with plaque psoriasis. Dermatol Ther. 2017;30. 8. Tabanlioglu Onan D, Hazar Tantoglu B, Alli N et al. Evaluation of the gastrointestinal findings of nodulocystic acne patients during systemic isotretinoin therapy. Turk J Med Sci. 2016;46:820–824. 9. Vallerand IA, Lewinson RT, Farris MS et al. Efficacy and adverse events of oral isotretinoin for acne: A systematic review. Br J Dermatol. 2018;178:76–85. 10. Pratt DS, Kaplan MM. Evaluation of abnormal liverenzyme results in asymptomatic patients. N Engl J Med. 2000;342:1266–1271. 91 11. Hansen TJ, Lucking S, Miller JJ et al. Standardized laboratory monitoring with use of isotretinoin in acne. J Am Acad Dermatol. 2016;75:323–328. 12. Opel D, Kramer ON, Chevalier M et al. Not every patient needs a triglyceride check, but all can get pancreatitis: A systematic review and clinical characterization of isotretinoinassociated pancreatitis. Br J Dermatol. 2017;177:960–966. 13. Acute pancreatitis linked to isotretinoin. Prescrire Int. 2015;24:46. 14. Tejedor Tejada J, Torres Yuste R, Garcia Pajares F. Acute pancreatitis secondary to treatment with isotretinoin. Gastroenterol Hepatol. 2019;42:256. 15. Ergun T, Seckin Gencosmanoglu D, Alpsoy E et al. Efficacy, safety and drug survival of conventional agents in pediatric psoriasis: A multicenter, cohort study. J Dermatol. 2017;44:630–634. 16. Fairhurst DA, Clark SM. Rectal bleeding following acitretin therapy for discoid lupus erythematosus. Dermatology. 2005;211:385. 17. Erpolat S, Gorpelioglu C, Sarifakioglu E. Isotretinoin associated anal fissure and rectal bleeding: A rare complication. Int J Dermatol. 2012;51:358–359. 18. Gungor S, Gokdemir G. Anal fissure and rectal bleeding as a complication of systemic isotretinoin therapy: Dermatologists know this side-effect, what about proctologists? Colorectal Dis. 2013;15:1187–1188. 19. ACCUTANE (isotretinoin) CAPSULES FDA product information. NDA 18-662/S054. 2000. Roche Laboratories Inc. https://www.accessdata.fda.gov/drugsatfda_docs/label/ 2004/18662s054lbl.pdf. 20. Martin P, Manley PN, Depew WT, et al. Isotretinoin-associated proctosigmoiditis. Gastroenterology. 1987;93:606–609. 21. Reniers DE, Howard JM. Isotretinoin-induced inflammatory bowel disease in an adolescent. Ann Pharmacother. 2001;35:1214–1216. 22. Bharmal R, Anderson SH. Exacerbation of inflammatory bowel disease with isotretinoin. JRSM Short Rep. 2010;1:58. 23. Passier JL, Srivastava N, van Puijenbroek EP. Isotretinoininduced inflammatory bowel disease. Neth J Med. 2006;64:52–54. 24. Reddy D, Siegel CA, Sands BE et al. Possible association between isotretinoin and inflammatory bowel disease. Am J Gastroenterol. 2006;101:1569–1573. 25. Spada C, Riccioni ME, Marchese M et al. Isotretinoin-associated pan-enteritis. J Clin Gastroenterol. 2008;42:923–925. 26. Rosen T, Unkefer RP. Treatment of pyoderma faciale with isotretinoin in a patient with ulcerative colitis. Cutis. 1999;64:107–109. 27. Razeghi S, Halvorson CR, Gaspari AA et al. Successful treatment of localized pyoderma faciale in a patient with Crohn’s disease. Gastroenterol Hepatol (N Y). 2013;9:541–543. 28. McHenry PM, Hudson M, Smart LM et al. Pyoderma faciale in a patient with Crohn’s disease. Clin Exp Dermatol. 1992;17:460–462. 29. Tsianos EV, Dalekos GN, Tzermias C et al. Hidradenitis suppurativa in Crohn’s disease. A further support to this association. J Clin Gastroenterol. 1995;20:151–153. 30. Etminan M, Bird ST, Delaney JA et al. Isotretinoin and risk for inflammatory bowel disease: A nested case-control study and meta-analysis of published and unpublished data. JAMA Dermatol. 2013;149:216–220. 92 31. Crockett SD, Porter CQ, Martin CF et al. Isotretinoin use and the risk of inflammatory bowel disease: A case-control study. Am J Gastroenterol. 2010;105:1986–1993. 32. Rashtak S, Khaleghi S, Pittelkow MR et al. Isotretinoin exposure and risk of inflammatory bowel disease. JAMA Dermatol. 2014;150:1322–1326. 33. Popescu CM, Popescu R. Isotretinoin therapy and inflammatory bowel disease. Arch Dermatol. 2011;147:724–729. 34. Lee SY, Jamal MM, Nguyen ET et al. Does exposure to isotretinoin increase the risk for the development of inflammatory bowel disease? A meta-analysis. Eur J Gastroenterol Hepatol. 2016;28:210–216. 35. Alhusayen RO, Juurlink DN, Mamdani MM et al. Isotretinoin use and the risk of inflammatory bowel disease: A populationbased cohort study. J Invest Dermatol. 2013;133:907–912. Retinoids in Dermatology 36. Bernstein CN, Nugent Z, Longobardi T et al. Isotretinoin is not associated with inflammatory bowel disease: A population-based case-control study. Am J Gastroenterol. 2009;104:2774–2778. 37. Stobaugh DJ, Deepak P, Ehrenpreis ED. Alleged isotretinoinassociated inflammatory bowel disease: Disproportionate reporting by attorneys to the Food and Drug Administration Adverse Event Reporting System. J Am Acad Dermatol. 2013;69:393–398. 38. Dermatology AAo. Position statement on isotretinoin 2011. Available from: http://www.aad.org/Forms/Policies/Uploads/ PS/PS-Isotretinoin.pdf. 39. Sewell JL, Mahadevan U. Of blemishes and bowels: Isotretinoin and inflammatory bowel disease. Gastroenterology. 2010;138:392–394. 17 Endocrine and Metabolic Side Effects Ayse Serap Karadag, Emin Ozlu, and Bodo C. Melnik Introduction Vitamin A (retinol) is a micronutrient that plays a critical role in cell proliferation and differentiation, vision, reproduction, and embryonic morphogenesis, has an impact on hormonal and metabolic regulations (1–4) and is an important micronutrient for the skin and cutaneous homeostasis (5,6). Retinoids, which are structural and functional derivatives of vitamin A, are used successfully in topical and systemic forms for the treatment of various skin diseases including acne vulgaris, psoriasis vulgaris, various disorders of keratinization, chronic hand dermatitis, cutaneous T-cell lymphoma, and chemoprevention of non-melanoma skin cancer (7–17). Retinol is metabolized to all-trans-retinoic acid (ATRA), which partially isomerizes to 13-cis retinoic acid and 9-cis retinoic acid in the liver (1–4). Synthetic retinoids have been derived from retinol and classified into three groups according to their molecular structure as first-, second-, and third-generation retinoids: ATRA and 13-cis retinoic acid (isotretinoin) belong to the first generation, whereas etretinate and acitretin are ­monoaromatic second-generation retinoids, followed by polyaromatic third-generation compounds known as arotenoids such as bexarotene. Alitretinoin, 9-cis retinoic acid, is the latest retinoid introduced for the treatment of chronic hand dermatitis (18). Physiologic Impact of Natural Retinoids on Endocrine Systems Vitamin A is a lipophilic micronutrient that plays a critical role in embryo and child development. Retinoic acid signaling plays a key role in the embryonic development of the epidermis, the extremities, and the secondary palate (19). Vitamin A is derived from animal (all-trans retinol or retinyl esters) and vegetable (carotenoids) foods taken with the diet (1–4). Vitamin A deficiency is especially correlated with infection and mortality in children and is a marker of malnutrition (20). In adults, vitamin A and its metabolites play a key role in vision, immune system, brain function, and metabolism (1–4). The physiologic effects of retinoids are regulated by retinoic acid receptors (RAR-α, -β, and -γ isoforms) and retinoid X receptor (RXR-α, -β, and -γ isoforms) (21) (Table 17.1). RAR and RXR are members of a broad family of nuclear receptors including steroid, thyroid hormone, vitamin D, liver X receptor (LXR), and peroxisome proliferator-activated receptors (PPARs). They act as ligand-dependent transcription factors. Many tissues are targeted by retinoids through different heterodimeric complexes (3). Importantly, retinoids have also a significant impact on stem cell differentiation (22). ATRA induces differentiation primarily by binding to RARs, which are the transcription factors that associate with RXRs and bind retinoic acid response elements (RAREs) in the nucleus. Binding of ATRA (22): 1. Initiates changes in interactions of RAR/RXRs with co-repressor and co-activator proteins, activating transcription of primary target genes. 2. Alters interactions with proteins that induce epigenetic changes. 3. Induces transcription of genes encoding transcription factors and signaling proteins that further modify gene expression and induce a secondary gene response (e.g., upregulation of p53, FoxO1, FoxO3, TRAIL) and results in alterations in estrogen receptor α signaling (3,20). Proteins that bind at or near RAREs include Sin3a, N-CoR1, PRAME, Trim24, NRIP1, Ajuba, Zfp423, and MN1/TEL. Interactions among retinoids, RARs/ RXRs, and these proteins explain in part the powerful effects of retinoids on stem cell differentiation. Retinoids also exert epigenetic effects (22,23). ATRA alters interactions of the RARs with various protein components of the transcription complex at numerous genes in stem cells, and some of these protein components of the transcription complex then either place or remove epigenetic marks on histones or on DNA, altering chromatin structure and leading to an exit from the self-renewing, pluripotent stem cell state (22–24). Epigenetic regulation of endocrine signaling is a recent focus of research (25). ATRA is a potent agent capable of inducing alterations in epigenetic modifications that produce various effects on the phenotype (26). Vitamin A is also involved in extranuclear and nontranscriptional effects, such as the activation of kinase cascades, which are integrated in the nucleus via the phosphorylation of several actors of ATRA signaling. Notably, vitamin A itself proved recently to be active and RARs present in the cytosol regulate translation and cell plasticity (27). Vitamin A and its metabolites affect the hormonal system. Retinoids play a role in the development and function of the hypothalamus, the pituitary gland, and the peripheral glands (3). In vivo studies have shown that modifications develop in the hypothalamic–pituitary–peripheral gland axis with retinoid 93 94 Retinoids in Dermatology TABLE 17.1 Nuclear Receptors and Their Natural and Synthetic Ligands Nuclear Receptors Natural and Synthetic Ligands Retinoic acid receptor (RAR), α,β,γ All-trans-retinoic acid, 9-cis retinoic acid (alitretinoin), etretinate, acitretin Retinoid X receptor (RXR), α,β,γ 9-cis retinoic acid, bexarotene Liver X receptor (LXR), α,β Peroxisome proliferator-activated receptor (PPAR) α,β,γ Thyroid hormone receptor (TR) Vitamin D receptor (VDR) Oxysterols Pregnane X receptor (PXR) Farnesoid receptor (FXR) Estrogen receptor α,β Glucocorticoid receptor Mineralocorticoid receptor Androgen receptor Fatty acids, leukotriene B4, fibrates, thiazolidinediones Thyroid hormone 1,25 Dihydroxy-vitamin D3 (calcitriol) Xenobiotics Chenodeoxycholic acid, bile acids Estradiol Cortisol, corticosteroids Aldosterone, spironolactone Dihydrotestosterone, testosterone deficiency or treatment (1,28,29). ATRA is not involved in thyroid organogenesis, but it may play a role in the maintenance of the developed thyroid cell phenotype (3). A very important finding on this topic is the coexistence of vitamin A and iodine deficiency in developing countries and the occurrence of goiter and vitamin A deficiency in more than 30% of children (30). In children with vitamin A deficiency, thyroid-stimulating hormone (TSH), total T4 level, and thyroid volume increase (3). Retinoids have also been used in the treatment of thyroid cancers due to their key role in the pathogenesis of thyroid pathology; however, the current data on this topic are less promising than expected earlier (31). ATRA appears to be effective on the hypothalamic–pituitary– adrenal (HPA) axis as well (3,32). One of the most important pieces of evidence related to this topic is the increase in basal corticosterone levels in rats with long-term treatment of ATRA (33). The current data are mostly concerned with the use and role of ATRA in pituitary and adrenal gland tumors. ATRA plays a critical role in gonadal development in men (1,35). ATRA also stimulates steroidogenesis in Leydig and ovarian cells (3,36). In addition, ATRA has been proposed to reduce cell proliferation by affecting the estrogen pathway in breast cancer (37). ATRA is likely to play a role in somatotropic hormone differentiation. In developed somatotrophs, retinoids affect growth hormone (GH) secretion (38,39). In some skin models, the synthesis of insulinlike growth factors 1 and 2 (IGF1 and IGF2) is increased by retinoids (40). The ATRA signaling pathway is involved in pancreatic development and maintenance of glucose-stimulated insulin secretion and β-cell mass (41,42); however, vitamin A plasma concentrations are higher in individuals with glucose intolerance. In addition, ATRA has a restorative effect on insulin secretion function in rats that are deprived of vitamin A. The pancreas is one of the few tissues with endogenous production of 9-cis RA (43). There is recent interest in the functions of vitamin A and in the regulation of lipid and glucose metabolism (2,44–46). In conclusion, vitamin A, ATRA, and its metabolites play an important gene-regulatory and epigenetic role in the development and function of endocrine glands. Most of our knowledge on this topic is about the effect of vitamin A on thyroid functions. With a better understanding of the mechanisms of action of ATRA and its metabolites, the effect of ATRA on normal and malignant endocrine tissues through various receptors is revealed. Effects of Synthetic Retinoids on Endocrine and Metabolic Homeostasis In contrast to the physiologic concentrations of vitamin A and its natural derivatives, concentrations and dosages of synthetic retinoids administered for the treatment of skin diseases by far outnumber physiologic retinoid levels. Therapeutic doses of retinoids evoke aberrant gene-regulatory and epigenetic reactions that often adversely affect endocrine and metabolic systems. Isotretinoin (13-cis retinoic acid) plays a key role in the treatment of severe acne (9,10). In sebocytes, neuroblastoma cells, and others, 13-cis retinoic acid is isomerized to all-trans-­retinoic acid (47). Isotretinoin represents the prodrug of RAR-active ATRA (48). Alitretinoin has beneficial effects in the treatment of chronic hand dermatitis (14) and is a pan-receptor agonist that binds to both RAR and RXR (49–51). Acitretin is effective in psoriasis and other disorders of keratinization (12,13,15) and activates RAR (52). Bexarotene, routinely used for the treatment of cutaneous T-cell lymphoma (16), selectively activates RXR (16,53,54). RAR-α/RXR synergism potentiates retinoid responsiveness in cutaneous T-cell lymphoma cell lines (55). Recent docking simulations suggest that ATRA could also bind to RXR (56). There is also evidence that the RXR agonist UAB30 upregulates genes responsible for the biosynthesis of ATRA in human epidermis (57). Several layers of retinoid ligand and RAR/RXR interaction have an impact on gene expression. To understand the gene-regulatory effects of synthetic retinoids on endocrine and metabolic regulation, RXR heterodimerization should be considered with other nuclear receptors that affect the endocrine and metabolic signaling of the cell (58) (Table 17.1). Some of the heterodimers (PPAR/RXR, LXR/RXR, FXR/RXR) are “permissive,” as they become transcriptionally active in the sole presence of either an RXR-selective ligand (“rexinoid”) or a nuclear receptor partner ligand. In contrast, “nonpermissive” heterodimers (including RAR/RXR, VDR/RXR, and TR/RXR) are unresponsive to rexinoids alone but these agonists superactivate transcription by synergizing with partner agonists (59). Transactivation of some of these other nuclear receptors, such as PPAR and LXR, may induce adverse metabolic and endocrine effects such as disturbances of lipid metabolism. The Effects of Synthetic Retinoids on the Hypothalamus-Pituitary System Most of our knowledge on the effects of retinoids on the hypothalamic–pituitary axis is about isotretinoin. Treatment ­ of GT1-7 hypothalamic cells with 10 µM isotretinoin for 48 h decreased cell growth to 45.6 ± 13% of control (60). Treatment with the RAR-antagonist AGN 193109 blocked the ability of 13-cis retinoic acid to decrease cell number. Three months of 95 Endocrine and Metabolic Side Effects isotretinoin treatment in acne patients significantly decreases thyroid-stimulating hormone (TSH), luteinizing hormone (LH), prolactin, adrenocorticotropic hormone (ACTH), and growth hormone (GH) (61,62). These changes were associated with decreases of serum morning cortisol, free triiodothyronine (T3) and total testosterone levels, insulin-like growth factor-binding protein 3, and insulin-like growth factor 1 (IGF-1) (61–63). Isotretinoin enhances nuclear expression of FoxO1 (64–66). FoxO1 plays a critical role in the regulation of pro-opiomelanocortin (POMC) gene expression. Phospho-STAT3 activates POMC promoter in response to leptin signaling through a mechanism that requires a specific protein 1 (SP1)-binding site in the POMC promoter. FoxO1 binds to STAT3 and prevents STAT3 from interacting with the SP1POMC promoter complex, and consequently inhibits STAT3mediated leptin action (67,68). Isotretinoin-induced nuclear FoxO1 may thus impair POMC expression, explaining reduced expression of ACTH in acne patients. FoxO1 suppresses the expression of hepatic GH receptor (GHR) (69), which plays a key role for the hepatic synthesis of IGF-1 (69,70). GHR-knockout pigs that lack GHR exhibited markedly reduced serum IGF-1 levels and reduced IGFBP3 activity (70). This animal model mimics the endocrine deviations observed in IGF-1-deficient patients with Laron syndrome (71), who do not develop acne when untreated (72). FoxO1 also suppresses PPAR-γ (73), which mediates hepatic secretion of IGF-1 (74). Isotretinoin via upregulation of FoxO1 in acne suppresses the hypothalamus-pituitary system at various levels. Little is known about the effects of retinoids other than isotretinoin on the hypothalamic–pituitary axis. Acitretin treatment affects only free T4 levels in patients with psoriasis, whereas pituitary hormones are not affected (75). Another study confirmed that acitretin does not affect serum LH, FSH, testosterone, cortisol, GH, and IGF-I levels, whereas a significant decrease in TSH levels and free T3 (FT3) has been observed (29). In a case of mycosis fungoides, reversible pituitary insufficiency secondary to bexarotene has been reported (76). In conclusion, although isotretinoin is thought to be effective in the treatment of acne involving the hypothalamus-pituitary axis, the effects and side effects of other systemic retinoids on the hypothalamus-pituitary axis are less characterized and require further investigations. The Effects of Synthetic Retinoids on the Thyroid Axis Synthetic retinoids have an endocrine effect on the thyroid axis. Bexarotene, approved since 1999 as a second-line treatment for late stage cutaneous T-cell lymphomas, has been shown to induce significant hypothyroidism through TSH suppression (77–81). Bexarotene through RXR suppresses the expression of TSH β-gene and to a lesser degree of α-TSH and TRH gene leading to central hypothyroidism, which is observed in nearly 100% of patients treated with daily doses of 150 mg/m2 (82). Bexarotene also differently affects the gene expression of deiodinases 1 and 2 as well as the peripheral clearance of thyroxine by inducing glucuronyl transferase and sulfotransferase enzymes (79,83). As a result, hypothyroid patients on bexarotene require a higher replacement dose (up to two times) of levothyroxine, and TSH concentrations cannot be used to monitor the treatment dose due to the suppression (82). Hypothyroidism, which starts a few days after bexarotene treatment, disappears in all patients after discontinuation of the drug (82). Alitretinoin (9-cis retinoic acid), which binds to RXR, also exhibits promoter suppression of the TSH β-gene in thyrotrophs in vitro (79). Notably, a TSH-suppressing effect has been observed in two of four patients treated with oral alitretinoin for congenital ichthyosis (84). Central hypothyroidism has not been observed in patients treated with oral isotretinoin, which does not interact with RXR. The role of isotretinoin on TSH is controversial, showing no change, decreases, or increases of serum levels during treatment (61,85–88), whereas all studies confirmed a significant decrease of T3 during isotretinoin treatment (61,62,85–87). Therapeutic intervention is usually not required. The Effects of Synthetic Retinoids on Glucose Homeostasis The effects of isotretinoin on glucose metabolism are complex. Most studies of isotretinoin are derived from acne patients with indirect determination of serum glucose, insulin, and HOMAIndex measurements. Direct studies of isotretinoin on hepatocytes, adipocytes, and skeletal muscle cells under in vivo conditions are still missing. In addition, acne and androgenrelated syndromes are frequently associated with pre-existing insulin resistance (89). The anti-inflammatory activity of isotretinoin may have an impact on inflammation-induced insulin resistance (90). Some studies suggest that isotretinoin does not increase insulin resistance (91–94), whereas other studies suggest the opposite (95–97). The role of FoxO1 in the regulation of glucose homeostasis is also complex. FoxO1, the transcription factor of starvation, induces hepatic gluconeogenesis (98–101). Transgenic mice overexpressing constitutively active FoxO1 specifically in the pancreas had impaired glucose tolerance, and some of them developed diabetes due to the reduction of β-cell mass (102). Adipocytes from insulin-resistant mice show reduced phosphorylation and increased nuclear accumulation of FoxO1, which is coupled to lowered expression of endogenous PPAR-γ target genes. The innate FoxO1 transrepression function enables insulin to augment PPAR-γ activity, which in turn leads to insulin sensitization, and this feed-forward cycle represents positive reinforcing connections between insulin and PPAR-γ signaling (73). In contrast, reduced FoxO1 expression protects FoxO1haploinsufficient mice against obesity-related insulin resistance with marked improvement not only in hepatic insulin sensitivity but also in skeletal muscle insulin action. FoxO1 haploinsufficiency also has resulted in increased PPAR-γ gene expression in adipose tissue, with enhanced expression of PPAR-γ target genes known to influence metabolism (103). FoxO1 regulates glucose metabolism in skeletal muscle. Dominant negative FoxO1 transfected by electroporation into mouse tibialis anterior muscle attenuated glucose uptake, GLUT4 protein, and subunits of the oxidative phosphorylation cascade (104). As FoxO1 is an ubiquitous regulator of glucose homeostasis affecting β-cell 96 insulin secretion, hepatic gluconeogenesis, and glucose uptake of adipose tissue and skeletal muscle, a conclusive prediction of isotretinoin-mediated FoxO1 expression on glucose homeostasis is not possible. Isotretinoin via isomerization to ATRA increases the expression of transcription factor p53 (105), which has been confirmed in primary human keratinocytes (65). p53, the guardian of the genome, plays a key role in metabolism, diabetes, pancreatic function, glucose homeostasis, and insulin resistance (106). p53 regulates multiple biochemical processes such as glycolysis, oxidative phosphorylation, lipolysis, lipogenesis, β-oxidation, gluconeogenesis, and glycogen synthesis. Notably, p53-mediated metabolic effects are totally dependent upon the results of insulin action (107). Prominent signs of its actions have been observed in muscles, liver, pancreas, and adipose tissue, being associated with attenuation of insulin signaling (107,108). Upregulation of p53 in adipose tissue caused an inflammatory response that led to insulin resistance (108). Remarkably, p53 increases the expression of FoxO1 (109), linking upregulated p53 and FoxO1 expression with insulin resistance. Impaired glucose tolerance has also been reported in hypertensive rats after systemic administration of ATRA (110). The effects of acitretin treatment on insulin are also controversial. One study suggested that acitretin enhances insulin sensitivity (111), whereas another study indicated that it causes insulin resistance (112). In vitro studies indicate that alitretinoin (9-cis retinoic acid) attenuates insulin secretion of pancreatic β-cells (113,114). In contrast, treatment of cardiomyocytes with 9-cis retinoic acid increased insulin- and metabolic stress−stimulated glucose transport (115). Notably, activation of RXR-α, which binds to the promoter of insulin receptor substrate 1 (IRS-1) alleviates insulin resistance by increasing IRS-1 expression (116). Alitretinoinmediated suppression of insulin secretion appears to be balanced by enhanced insulin sensitization. Bexarotene may enhance insulin sensitivity, and thus monitoring of plasma glucose is recommended (117). Rexinoids function as RXR heterodimer-selective agonists, activating RXR:PPAR-γ and RXR:LXR dimers. PPAR-γ is a target for antidiabetic agents. In mouse models of noninsulin-dependent diabetes mellitus (NIDDM) and obesity, RXR agonists function as insulin sensitizers (118). In Zucker diabetic fatty (ZDF) rats treated with LGD1069 (RXR agonist bexarotene) improved glucose tolerance and insulin resistance has been reported (119). In combined administration of bexarotene with agents that stimulate insulin sensitivity, an accelerated treatment effect with an increased risk of hypoglycemia should be expected. In conclusion, the effects of RAR-and RXR-agonists on glucose homeostasis are complex and affect both insulin secretion and peripheral glucose uptake. In the majority of patients, retinoidinduced deviations of glucose metabolism are not a serious problem and do not require dose reduction or termination of treatment. Effect of Oral Retinoids on Lipid and Lipoprotein Metabolism All retinoids in clinical use, i.e., isotretinoin, alitretinoin, acitretin, and bexarotene, may negatively affect lipid and lipoprotein metabolism, primarily increasing the risk of Retinoids in Dermatology hypertriglyceridemia, especially in individuals predisposed for hypertriglyceridemia (120–123). Increased low-density lipoprotein cholesterol (LDL-C) and decreased high-density lipoprotein cholesterol (HDL-C) levels are also commonly seen with retinoid use (120–123). The increase in serum triglycerides (TG) by oral isotretinoin is primarily the result of enhanced hepatic TG synthesis and increased secretion of TG-rich very low-density lipoproteins (VLDL) (85,95). Pretreatment values of VLDL apoprotein B significantly increased 25% during treatment supporting hepatic oversecretion of TG-rich VLDL (125). A comparative study in Sprague-Dawley rats demonstrated that intraperitoneal injection of ATRA induced a much stronger hypertriglyceridemia than 13-cis retinoic acid, the drug precursor of ATRA (126). Oral gavage of male Fischer rats with 13-cis retinoic acid for 6 days caused a rapid and sustained increase in serum TG at least in part mediated by RARs (127). Isotretinoin-mediated upregulation of p53 and FoxO1 may explain isotretinoin-induced hypertriglyceridemia. In studying human hepatocytes, ATRA activates the p14-MDM2-p53 pathway stabilizing p53 (128), which promotes the expression of FoxO1 (109). Each VLDL molecule contains one apoB-100, which is required for TG loading onto the VLDL particle. ApoB-100 and apoB-48 are created by a premature stop codon by apoB mRNA-editing enzyme complex 1 (apobec1). Notably, p53 response elements (p53RE) in the genes encoding for apoB and apobec1 have been detected. Both genes are transcriptionally regulated by p53 (129). Increased ATRA-p53 signaling may thus explain enhanced hepatic synthesis of VLDL apoB. Hepatic VLDL synthesis is also controlled by FoxO1. Augmented FoxO1 activity promotes hepatic VLDL overproduction and predisposes to the development of hypertriglyceridemia (130). TG loading to apoB-100 is facilitated by microsomal TG transfer protein (MTP), which is activated by FoxO1 (131,132). Isotretinoin-mediated upregulation of p53 in the liver may explain p53- and FoxO1-induced VLDL hypertriglyceridemia. Remarkably, individuals who develop hypertriglyceridemia during isotretinoin therapy for acne, as well as their parents, are at increased risk for future hyperlipidemia and the metabolic syndrome (133). Hypertriglyceridemia is also an adverse effect of the RAR agonist acitretin (134–137). Daily fish oil supplements containing 3 gm of omega-3 fatty acids (1.8 gm of eicosapentaenoic acid 20:5 omega 3, and 1.2 gm of docosahexaenoic acid 22:6 omega 3) were found to be effective in reducing hypertriglyceridemia (134). Evidence derived from rats indicates that RAR and RXR ligands can act synergistically to induce hypertriglyceridemia through distinct mechanisms of action (138). DrugBank screening revealed alitretinoin and bexarotene are liver X receptor (LXR) modulators (139). Both retinoids are able to induce hypertriglyceridemia (49,117,141). Dose-response studies demonstrated that plasma concentrations observed in clinical trials are sufficient for LXR activation and thus could account for LXR-mediated side effects such as hyperlipidemia (139). Many liver LXR/RXR-related genes including Scd-1 and Srebf1 are associated with increased TG and were highly expressed in rat liver after bexarotene administration (143). Studies in mice confirmed that hypertriglyceridemic action of bexarotene occurs via the RXR/LXR heterodimer and show that RXR heterodimers Endocrine and Metabolic Side Effects can act with a selective permissivity on target genes of specific metabolic pathways in the liver (144). Another target gene of RXR agonists is apolipoprotein C-III (apoC-III) (145). apoC-III promotes the assembly and secretion of TG-rich VLDL particles from hepatic cells under lipid-rich conditions (146). In addition, apoC-III strongly inhibits hepatic uptake of VLDL and intermediate density lipoproteins (IDL), overriding the opposite influence of apolipoprotein E when both are present (147). Patients using retinoids should be consulted for possible elevation in TG and cholesterol levels, and treatment strategies should be established if hyperlipidemia develops. In very rare cases, severe hypertriglyceridemia may induce acute pancreatitis (148– 150). Serum TG should be monitored and should not exceed 400 mg/dL. Caloric, carbohydrate, and alcohol restriction, along with dietary supplementation including omega-3 fatty acids, can be helpful. 97 change of gene expression and plasma concentration of adiponectin but elevated expression of leptin (158). Adipocyte cell culture revealed that endogenous and synthetic retinoic acid receptor (RAR) α- and RAR-γ-selective agonists, as well as a synthetic RXR agonist, efficiently reduced adiponectin expression (159). Human sebaceous glands express adiponectin, leptin, IL6, resistin, serpin E1, and visfatin (160). SZ95 sebocytes responded to isotretinoin with an enhancement of the expression and secretion of leptin and with a reduction of adiponectin mRNA levels (160). Sebaceous gland and sebocytes express adiponectin receptor (161). Adiponectin strongly upregulates lipid synthesis in sebocytes (161). Isotretinoin-mediated suppression of adiponectin in sebaceous glands may thus contribute to isotretinoin’s sebum-suppressive effect. Epicardial adipose tissue displays p53 mRNA expression that is negatively correlated with adiponectin expression (162). Isotretinoin-mediated upregulation of p53 may thus suppress lipogenic adiponectin signaling in sebocytes in acne patients. Effect of Oral Retinoids on Adipocytokines White adipose tissue acts as an endocrine organ producing a variety of hormones (adipocytokines), including adiponectin, leptin, tumor-necrosis factor alpha, and angiotensin II, which influence lipid metabolism, systemic insulin sensitivity, and inflammation. Adiponectin is the most abundant peptide secreted by adipocytes, whose reduction plays a central role in obesity-related diseases, including insulin resistance/type 2 diabetes and cardiovascular disease. In addition to adipocytes, other cell types, such as skeletal and cardiac myocytes and endothelial cells, can also produce this adipocytokine. Adiponectin performs many metabolic functions that link to energy metabolism (151,152). The hormone leptin is also a hormone predominantly secreted by adipose cells that helps to regulate energy balance by inhibiting hunger acting on receptors in the arcuate nucleus of the hypothalamus. In obesity, a decreased sensitivity to leptin occurs resulting in an inability to detect satiety despite high energy stores and high levels of leptin. The primary function of the hormone leptin is the regulation of adipose tissue mass through central h­ ypothalamus− mediated effects on hunger, food energy use, physical exercise, and energy balance (153,154). After isotretinoin treatment of acne patients, serum leptin levels decreased, whereas adiponectin levels increased significantly (94). Increased serum adiponectin levels have been confirmed by three studies of isotretinoin-treated acne patients (94,155,156), while one study reported that isotretinoin therapy did not affect the mean adiponectin and leptin levels (97). The increase in adiponectin during isotretinoin therapy correlated with baseline TG levels (96). In patients with psoriasis vulgaris, post-treatment adiponectin levels were increased after acitretin therapy (111). In contrast, no change of adiponectin levels during acitretin treatment was reported in another study, while resistin levels fell within the normal range (112). Adiponectin lowers serum TG through enhancement of the catabolism of TG-rich lipoproteins (157), a potential compensatory mechanism of retinoid-induced hypertriglyceridemia. Serum adipocytokine levels reported in clinical studies differ substantially from results obtained in cell culture and tissues. A short-term study with therapeutic isotretinoin doses on metabolism of epididymal fat tissue of Wistar rats showed no significant Effect of Oral Retinoids on Skin Barrier Function Synthetic retinoids affect epidermal barrier homeostasis. As a result, dry skin is a common adverse effect of oral isotretinoin treatment associated with increased transepidermal water loss often leading to retinoid dermatitis (163,164). RAR-γ-RXR mediated pathways in the skin are important pathophysiologic triggers for increased skin TSLP expression. Synthetic agonists of the VDR and RAR-γ as well as the natural agonist ATRA increased TSLP expression in the skin (165). Application of ATRA onto the ear lobes of mice selectively induces TSLP production without inducing apparent inflammation (166). RAR-α and RAR-γ subtypes possess different roles in the skin and may be of relevance for the autoregulation of endogenous retinoid signaling in skin (167). Aquaporin 3 (AQP3) is a key regulator of transepidermal water traffic and responds to isotretinoin and ATRA resulting in enhanced the expression of AQP3 in human keratinocytes and human skin (168,169). Elevated expression levels of AQP3 result in impaired barrier integrity and increased proinflammatory cytokine production mimicking the pathological conditions in Notch-deficient mice and in atopic dermatitis (170). The expression of AQP3 is induced by p53 (170,171). A dose-dependent induction of dry skin has also been reported for acitretin (172). ATP-binding cassette subfamily A, member 1 (ABCA1) is a membrane transporter responsible for cholesterol efflux and plays a pivotal role in regulating cellular cholesterol levels. ABCA1 is expressed in keratinocytes, where it is negatively regulated by a decrease in cellular cholesterol levels or altered permeability barrier requirements and positively regulated by activators of LXR, PPARs, and RXR or increases in cellular cholesterol levels (173). In an animal model of Alzheimer disease, the RXR agonist of bexarotene induced the expression of ABCA1 and promoted cellular cholesterol efflux (174). Daily oral application of 30 mg alitretinoin in patients with chronic hand eczema increased Ki-67-positive cells in the suprabasal layer and a normalized dysregulated expression of various skin barrier genes (claudin 1, loricrin, filaggrin, and cytokeratin 10) and TSLP (175). Alitretinoin is also negative regulator of 98 Retinoids in Dermatology TSLP expression in airway epithelial cells (176). Inhibition of IL-1β-dependent genes by active RXRs involves antagonism of NF-κB signaling (177). In conclusion, retinoids in clinical use for the treatment of skin disease have various effects on critical determinants of epidermal barrier function depending on their specific nuclear receptor binding and signaling (178). Although it has been proposed that the use of vitamin E with retinoids may reduce side effects, current data suggest that vitamin E supplementation does not provide clinical improvement (34,140). In conclusion, the relationship between retinoids and vitamins is highly complex. Vitamin D supplementation in acne in patients with proven vitamin D deficiency may even enhance the effects of the isotretinoin therapy. The Effects of Synthetic Retinoids on Sex Hormones and Fertility Conclusions Retinoids may affect the menstrual cycle, but there is no comprehensive study on this topic. Isotretinoin is associated with menorrhagia, delayed menstruation, hypermenorrhea, postcoital bleeding, and even amenorrhea. In addition, the effects of isotretinoin on anti-Müllerian hormones, ovarian volume, ovarian reserves, and antral follicle counts suggest that isotretinoin may have negative effects on ovarian reserves (8). In contrast, in a rat study, the negative effect of isotretinoin on ovarian reserves was found to be reversible (179); however, the number of ovarian follicles with apoptotic granulosa cells was increased in isotretinoin-treated rats (180). Upregulation of p53 accompanies granulosa cell apoptosis (181), which may be promoted by isotretinoin treatment (182). Human studies investigating the effects of isotretinoin on female fertility have shown that isotretinoin affects the levels of ovarian hormones (183–186). There is no comprehensive study on the effects of other retinoids on female sex hormones and fertility. The effects of retinoids on male fertility have also been investigated. Acitretin treatment does not affect spermatogenesis in rats and humans (187); however, isotretinoin may disrupt spermatogenesis and cause testicular degeneration in animal models and, in contrast, increase sperm density and motility in humans. There are no reported cases of infertility induced by isotretinoin or acitretin (188). In rare cases, gynecomastia has developed after isotretinoin treatment (189,190). It is difficult to reach a definitive judgment of the effects of retinoids on sex hormones and fertility without the benefit of more directed studies. The Association between Retinoids and Vitamins Vitamin B12 and folic acid deficiencies have similar side effects. Isotretinoin may cause hyperhomocysteinemia by reducing holotranscobalamin, vitamin B12, and folate levels (191,192). Vitamin D has an important role in the regulation of sebaceous gland activity (193) by regulating both sebocyte proliferation and differentiation. It also has anticomedogenic and antioxidant effects. Following 3 months of isotretinoin treatment, 25-hydroxy-­ vitamin D decreases significantly, whereas 1,25 dihydroxy vitamin D increases significantly (194). A recent study found increased serum levels of 25-hydroxy-vitamin D after isotretinoin treatment in acne patients (195). Interestingly, vitamin D receptor (VDR), which is under regulatory control of p53 (196), maintains a significant molecular cross-talk with p53 in the skin (142). Bexarotenemediated activation of RXR is also associated with activation of p53 (124). Synthetic retinoids are indispensable drugs used in the treatment of many dermatologic diseases. Retinoids have important roles in the development and function of the hormonal system and are critical regulators of gene expression. While topical retinoids are not expected to cause endocrine and metabolic side effects, synthetic retinoids may alter the hypothalamic–­pituitary–adrenal (HPA) and thyroid axis, lipoprotein and epidermal lipid metabolism, and the skin barrier function. Side effects of systemic retinoids on the endocrine system are substantial and require intervention to control such retinoid-induced adverse effects as bexarotene-induced central hypothyroidism and retinoidinduced hyperlipidemia. REFERENCES 1. Clagett-Dame M, Knutson D. Vitamin A in reproduction and development. Nutrients. 2011;3:385–428. 2. Yasmeen R, Jeyakumar SM, Reichert B et al. The contribution of vitamin A to autocrine regulation of fat depots. Biochim Biophys Acta. 2012;1821:190–197. 3. Brossaud J, Pallet V, Corcuff JB. Vitamin A, endocrine tissues and hormones: Interplay and interactions. Endocr Connect. 2017;6:121–130. 4. Blaner WS. Vitamin A signaling and homeostasis in obesity, diabetes, and metabolic disorders. Pharmacol Ther. 2019;197:153–178. 5. Elewa RM, Zouboulis CC. Vitamin A and the skin. In: Pappas A, editor. Nutrition and Skin: Lessons for Anti-aging, Beauty and Healthy Skin, 1st ed. Springer Science+Business Media, 2011: pp. 7–23. 6. Liakou AI, Theodorakis MJ, Melnik BC et al. Nutritional clinical studies in dermatology. J Drugs Dermatol. 2013;12:1104–1109. 7. Chapman MS. Vitamin A: History, current uses, and controversies. Semin Cutan Med Surg. 2012;31:11–16. 8. Karadag AS, Topaloglu Demir F. Systemic retinoids. Turkiye Klinikleri J Dermatol-Special Topics. 2014;7:54–70. 9. Karadag AS, Kalkan G, Lin YT, Chen W. Update of oral isotretinoin in acne treatment. In: Neena K, Raj K, editors. World Clinics Dermatology Acne. 1st ed. New Delhi, India: Jaypee Brothers Medical Publishers Ltd, 2014: pp. 169–201. 10. Karadag AS. Systemic retinoids in treatment of acne vulgaris. Turkiye Klinikleri J Dermatol-Special Topics. 2016;9:63–76. 11. Chien A. Retinoids in acne management: Review of current understanding, future considerations, and focus on topical treatments. J Drugs Dermatol. 2018;17:51–55. 12. Lee CS, Li K. A review of acitretin for the treatment of psoriasis. Expert Opin Drug Saf. 2009;8:769–779. 13. Subedi S, Yu Q, Chen Z, Shi Y. Management of pediatric psoriasis with acitretin: A review. Dermatol Ther. 2018;31(1). Endocrine and Metabolic Side Effects 14. Blair HA, Scott LJ. Alitretinoin: A review in severe chronic hand eczema. Drugs. 2016;76:1271–1279. 15. Happle R, van de Kerkhof PC, Traupe H. Retinoids in disorders of keratinization: Their use in adults. Dermatologica. 1987;175:107–124. 16. Huen AO, Kim EJ. The role of systemic retinoids in the treatment of cutaneous T-cell lymphoma. Dermatol Clin. 2015;33:715–729. 17. Bettoli V, Zauli S, Virgili A. Retinoids in the chemoprevention of non-melanoma skin cancers: Why, when and how. J Dermatolog Treat. 2013;24:235–237. 18. Bissonnette R, Worm M, Gerlach B et al. Successful retreatment with alitretinoin in patients with relapsed chronic hand eczema. Br J Dermatol. 2010;162:420–426. 19. Mammadova A, Zhou H, Carels CE, Von den Hoff JW. Retinoic acid signalling in the development of the epidermis, the limbs and the secondary palate. Differentiation. 2016;92:326–335. 20. Wiseman EM, Bar-El Dadon S, Reifen R. The vicious cycle of vitamin a deficiency: A review. Crit Rev Food Sci Nutr. 2017;57:3703–3714. 21. Rochette-Egly C, Germain P. Dynamic and combinatorial control of gene expression by nuclear retinoic acid receptors (RARs). Nucl Recept Signal. 2009;7:e005. 22. Gudas LJ, Wagner JA. Retinoids regulate stem cell differentiation. J Cell Physiol. 2011;226:322–330. 23. Gudas LJ. Retinoids induce stem cell differentiation via epigenetic changes. Semin Cell Dev Biol. 2013;24:701–705. 24. Urvalek AM, Gudas LJ. Retinoic acid and histone deacetylases regulate epigenetic changes in embryonic stem cells. J Biol Chem. 2014;289:19519–19530. 25. Zhang X, Ho SM. Epigenetics meets endocrinology. J Mol Endocrinol. 2011;46:11–32. 26. Bar-El Dadon S, Reifen R. Vitamin A and the epigenome. Crit Rev Food Sci Nutr. 2017;57:2404–2411. 27. Al Tanoury Z, Piskunov A, Rochette-Egly C. Vitamin A and retinoid signaling: Genomic and nongenomic effects. J Lipid Res. 2013;54:1761–1775. 28. Zimmermann MB. Interactions of vitamin A and iodine deficiencies: Effects on the pituitary-thyroid axis. Internat J Vitamin Nutr Res. 2007;77:236–240. 29. Angioni AR, Lania A, Cattaneo A et al. Effects of chronic retinoid administration on pituitary function. J Endocrin Invest. 2005;28:961–964. 30. Zimmermann MB, Jooste PL, Mabapa NS et al. Vitamin A supplementation in iodine-deficient African children decreases thyrotropin stimulation of the thyroid and reduces the goiter rate. Am J Clin Nutr. 2007;86:1040–1044. 31. Grünwald F, Pakos E, Bender H et al. Redifferentiation therapy with retinoic acid in follicular thyroid cancer. J Nucl Med. 1998;39:1555–1558. 32. Marissal-Arvy N, Hamiani R, Richard E et al. Vitamin A regulates hypothalamic-pituitary-adrenal axis status in LOU/C rats. J Endocrinol. 2013;219:21–27. 33. Cai L, Yan XB, Chen XN et al. Chronic all-trans retinoic acid administration induced hyperactivity of HPA axis and behavioral changes in young rats. Eur Neuropsychopharmacol. 2010;20:839–847. 34. Kus S, Gün D, Demirçay Z, Sur H. Vitamin E does not reduce the side-effects of isotretinoin in the treatment of acne vulgaris. Int J Dermatol. 2005;44:248–251. 99 35. Livera G, Rouiller-Fabre V, Pairault C et al. Regulation and perturbation of testicular functions by vitamin A. Reproduction. 2002;124:173–180. 36. Wickenheisser JK, Nelson-DeGrave VL, Hendricks KL et al. Retinoids and retinol differentially regulate steroid biosynthesis in ovarian theca cells isolated from normal cycling women and women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2005;90:4858–4865. 37. Ombra MN, Di Santi A, Abbondanza C et al. Retinoic acid impairs estrogen signaling in breast cancer cells by interfering with activation of LSD1 via PKA. Biochim Biophys Acta. 2013;1829:480–486. 38. Cheng Y, Xiang Y, Lin Y et al. Retinoic acid and dexamethasone induce differentiation and maturation of somatotroph cells at different stages in vitro. Endocrine J. 2011;58:177–184. 39. Mallo F, Lamas JA, Casanueva FF, Dieguez C. Effect of retinoic acid deficiency on in vivo and in vitro GH responses to GHRH in male rats. Neuroendocrinol. 1992;55:642–647. 40. Shim JH, Shin DW, Lee TR et al. The retinoic acid-induced upregulation of insulin-like growth factor 1 and 2 is associated with prolidase-dependent collagen synthesis in UVA-irradiated human dermal equivalents. J Dermatol Sci. 2012;66:51–59. 41. Kam RK, Deng Y, Chen Y, Zhao H. Retinoic acid synthesis and functions in early embryonic development. Cell Biosci. 2012;2:11. 42. Brun PJ, Grijalva A, Rausch R et al. Retinoic acid receptor signaling is required to maintain glucose-stimulated insulin secretion and beta-cell mass. FASEB J. 2015;29:671–683. 43. Kane MA, Folias AE, Pingitore A et al. Identification of 9-cis retinoic acid as a pancreas-specific autacoid that attenuates glucose-stimulated insulin secretion. PNAS USA. 2010;107: 21884–21889. 44. Bonet ML, Ribot J, Palou A. Lipid metabolism in mammalian tissues and its control by retinoic acid. Biochim Biophys Acta. 2012;1821:177–189. 45. Berry DC, Noy N. All-trans-retinoic acid represses obesity and insulin resistance by activating both peroxisome proliferation-activated receptor beta/delta and retinoic acid receptor. Mol Cell Biol. 2009;29:3286–3296. 46. Cadoudal T, Glorian M, Massias A et al. Retinoids upregulate phosphoenolpyruvate carboxykinase and glyceroneogenesis in human and rodent adipocytes. J Nutr. 2008;138:1004–1009. 47. Tsukada M, Schröder M, Roos TC et al. 13-cis retinoic acid exerts its specific activity on human sebocytes through selective intracellular isomerization to all-trans retinoic acid and binding to retinoid acid receptors. J Invest Dermatol. 2000;115:321–327. 48. Schroeder M, Zouboulis CC. All-trans-retinoic acid and 13-cis-retinoic acid: Pharmacokinetics and biological activity in different cell culture models of human keratinocytes. Horm Metab Res. 2007;39:136–140. 49. Miller VA, Rigas JR, Benedetti FM et al. Initial clinical trial of the retinoid receptor pan agonist 9-cis retinoic acid. Clin Cancer Res. 1996;2:471–475. 50. Allenby G, Janocha R, Kazmer S et al. Binding of 9-cis-retinoic acid and all-trans-retinoic acid to retinoic acid receptors alpha, beta, and gamma. Retinoic acid receptor gamma binds all-trans-retinoic acid preferentially over 9-cis-retinoic acid. J Biol Chem. 1994;269:16689–16695. 51. Allenby G, Bocquel MT, Saunders M et al. Retinoic acid receptors and retinoid X receptors: Interactions with endogenous retinoic acids. Proc Natl Acad Sci USA. 1993;90:30–34. 100 52. Pilkington T, Brogden RN. Acitretin: A review of its pharmacology and therapeutic use. Drugs. 1992;43:597–627. 53. Miller VA, Benedetti FM, Rigas JR et al. Initial clinical trial of a selective retinoid X receptor ligand, LGD1069. J Clin Oncol. 1997;15:790–795. 54. Chitranshi N, Dheer Y, Kumar S et al. Molecular docking, dynamics, and pharmacology studies on bexarotene as an agonist of ligand-activated transcription factors, retinoid X receptors. J Cell Biochem. 2019 Feb 11. doi: 10.1002/jcb.28455. [Epub ahead of print]. 55. Wang L, DeMarco SS, Peaks MS et al. RARα/RXR synergism potentiates retinoid responsiveness in cutaneous T-cell lymphoma cell lines. Exp Dermatol. 2017;26:1004–1011. 56. Tsuji M, Shudo K, Kagechika H. Docking simulations suggest that all-trans retinoic acid could bind to retinoid X receptors. J Comput Aided Mol Des. 2015;29:975–988. 57. Wu L, Chaudhary SC, Atigadda VR et al. Retinoid X receptor agonists upregulate genes responsible for the biosynthesis of all-trans-retinoic acid in human epidermis. PLOS ONE. 2016;11:e0153556. 58. Evans RM, Mangelsdorf DJ. Nuclear receptors, RXR, and the big bang. Cell. 2014;157:255–266. 59. Pérez E, Bourguet W, Gronemeyer H, de Lera AR. Modulation of RXR function through ligand design. Biochim Biophys Acta. 2012;1821:57–69. 60. Griffin JN, Pinali D, Olds K et al. 13-Cis-retinoic acid decreases hypothalamic cell number in vitro. Neurosci Res. 2010;68:185–190. 61. Karadag AS, Ertugrul DT, Tutal E, Akin KO. Isotretinoin influences pituitary hormone levels in acne patients. Acta Derm Venereol. 2011;91:31–34. 62. Karadag AS, Takci Z, Ertugrul DT et al. The effect of different doses of isotretinoin on pituitary hormones. Dermatology. 2015;230:354–359. 63. Karadag AS, Ertugrul DT, Tutal E, Akin KO. Short-term isotretinoin treatment decreases insulin-like growth factor-1 and insulin-like growth factor binding protein-3 levels: Does isotretinoin affect growth hormone physiology? Br J Dermatol. 2010;162:798–802. 64. Melnik BC. Isotretinoin and FoxO1: A scientific hypothesis. Dermatoendocrinol. 2011; 3:141–165. 65. Shi G, Liao PY, Cai XL et al. FoxO1 enhances differentiation and apoptosis in human primary keratinocytes. Exp Dermatol. 2018;27:1254–1260. 66. Agamia NF, Hussein OM, Abdelmaksoud RE et al. Effect of oral isotretinoin on the nucleo-cytoplasmic distribution of FoxO1 and FoxO3 proteins in sebaceous glands of patients with acne vulgaris. Exp Dermatol. 2018;27:1344–1351. 67. Yang G, Lim CY, Li C et al. FoxO1 inhibits leptin regulation of pro-opiomelanocortin promoter activity by blocking STAT3 interaction with specificity protein 1. J Biol Chem. 2009;284:3719–3727. 68. Ma W, Fuentes G, Shi X et al. FoxO1 negatively regulates leptin-induced POMC transcription through its direct interaction with STAT3. Biochem J. 2015;466:291–298. 69. Dong XC, Copps KD, Guo S et al. Inactivation of hepatic Foxo1 by insulin signaling is required for adaptive nutrient homeostasis and endocrine growth regulation. Cell Metab. 2008;8:65–76. 70. Hinrichs A, Kessler B, Kurome M et al. Growth hormone receptor-deficient pigs resemble the pathophysiology of human Laron syndrome and reveal altered activation of signaling cascades in the liver. Mol Metab. 2018;11:113–128. Retinoids in Dermatology 71. Laron Z. Lessons from 50 years of study of Laron syndrome. Endocr Pract. 2015;21:1395–402. 72. Ben-Amitai D, Laron Z. Effect of insulin-like growth factor-1 deficiency or administration on the occurrence of acne. J Eur Acad Dermatol Venereol. 2011;25:950–954. 73. Fan W, Imamura T, Sonoda N et al. FOXO1 transrepresses peroxisome proliferator-activated receptor gamma transactivation, coordinating an insulin-induced feed-forward response in adipocytes. J Biol Chem. 2009;284:12188–12197. 74. Wan X, Wang S, Xu J et al. Dietary protein-induced hepatic IGF-1secretion mediated by PPARγ activation. PLOS ONE. 2017;12:e0173174. 75. Karadag AS, Ozlu E, Kostek O et al. Effect of low-dose acitretin treatment on pituitary hormones in psoriasis vulgaris: A retrospective study. Indian J Dermatol Venereol Leprol. 2019;85(3):300–304. 76. Atmaca H, Islek I, Sentürk N. Reversible pituitary insufficiency due to bexarotene therapy in a patient with mycosis fungoides. Pituitary. 2014;17:492–493. 77. Cohen O, Flynn TR, Wondisford FE. Ligand-dependent antagonism by retinoid X receptors of inhibitory thyroid hormone response elements. J Biol Chem. 1995;270:13899–13905. 78. Takeda T, Nagasawa T, Miyamoto T et al. The function of retinoid X receptors on negative thyroid hormone response elements. Mol Cell Endocrinol. 1997;128:85–96. 79. Sherman SI, Gopal J, Haugen BR et al. Central hypothyroidism associated with retinoid X receptor-selective ligands. N Engl J Med. 1999;340:1075–1079. 80. Macchia PE, Jiang P, Yuan YD et al. RXR receptor agonist suppression of thyroid function: Central effects in the absence of thyroid hormone receptor. Am J Physiol Endocrinol Metab. 2002;283:326–331. 81. Sherman SI. Etiology, diagnosis, and treatment recommendations for central hypothyroidism associated with bexarotene therapy for cutaneous T-cell lymphoma. Clin Lymphoma. 2003;3:249–252. 82. Graeppi-Dulac J, Vlaeminck-Guillem V, Perier-Muzet M et al. Endocrine side-effects of anti-cancer drugs: The impact of retinoids on the thyroid axis. Eur J Endocrinol. 2014;170:R253–R262. 83. Smit JW, Stokkel MP, Pereira AM et al. Bexarotene-induced hypothyroidism: Bexarotene stimulates the peripheral metabolism of thyroid hormones. J Clin Endocrinol Metab. 2007;92:2496–2499. 84. Gånemo A, Sommerlund M, Vahlquist A. Oral alitretinoin in congenital ichthyosis: A pilot study shows variable effects and a risk of central hypothyroidism. Acta Derm Venereol. 2012;92:256–257. 85. Marsden JR, Trinick TR, Laker MF, Shuster S. Effects of isotretinoin on serum lipids and lipoproteins, liver and thyroid function. Clin Chim Acta. 1984;143:243–251. 86. Uyar B, Solak A, Saklamaz A et al. Effects of isotretinoin on the thyroid gland and thyroid function tests in acne patients: A preliminary study. Indian J Dermatol Venereol Leprol. 2016;82:587–588. 87. Yıldırım N, Doğan S, Atakan N. Evaluation of thyroid function tests of acne vulgaris patients treated with systemic isotretinoin. J Dermatolog Treat. 2017;28:141–144. 88. Aksoy B. Systemic retinoids and thyrotoxicosis in (multi) nodular goiter: Side effect or coincidence? Indian J Dermatol. 2018;63:270–272. Endocrine and Metabolic Side Effects 89. Melnik BC, John SM, Plewig G. Acne: Risk indicator for increased body mass index and insulin resistance. Acta Derm Venereol. 2013;93:644–649. 90. Akash MSH, Rehman K, Liaqat A. Tumor necrosis factor-alpha: Role in development of insulin resistance and pathogenesis of type 2 diabetes mellitus. J Cell Biochem. 2018;119:105–110. 91. Stoll D, Binnert C, Mooser V, Tappy L. Short-term administration of isotretinoin elevates plasma triglyceride concentrations without affecting insulin sensitivity in healthy humans. Metabolism. 2004;53:4–10. 92. Ertugrul DT, Karadag AS, Tutal E, Akin KO. Isotretinoin does not induce insulin resistance in patients with acne. Clin Exp Dermatol. 2011;36:124–128. 93. Cetinözman F, Aksoy DY, Elçin G, Yıldız BO. Insulin sensitivity, androgens and isotretinoin therapy in women with severe acne. J Dermatolog Treat. 2014;25:119–122. 94. Karadag AS, Ertugrul DT, Takci Z et al. The effect of isotretinoin on retinol-binding protein 4, leptin, adiponectin and insulin resistance in acne vulgaris patients. Dermatology. 2015;230:70–74. 95. Koistinen HA, Remitz A, Gylling H et al. Dyslipidemia and a reversible decrease in insulin sensitivity induced by therapy with 13-cis-retinoic acid. Diabetes Metab Res Rev. 2001;17:391–395. 96. Heliövaara MK, Remitz A, Reitamo S et al. 13-cis-Retinoic acid therapy induces insulin resistance, regulates inflammatory parameters, and paradoxically increases serum adiponectin concentration. Metabolism. 2007;56:786–791. 97. Soyuduru G, Özsoy Adışen E, Kadıoğlu Özer İ, Aksakal AB. The effect of isotretinoin on insulin resistance and adipocytokine levels in acne vulgaris patients. Turk J Med Sci. 2019;49:238–244. 98. Zhang W, Patil S, Chauhan B et al. FoxO1 regulates multiple metabolic pathways in the liver: Effects on gluconeogenic, glycolytic, and lipogenic gene expression. J Biol Chem. 2006;281:10105–10117. 99. Oh KJ, Han HS, Kim MJ, Koo SH. CREB and FoxO1: Two transcription factors for the regulation of hepatic gluconeogenesis. BMB Rep. 2013;46:567–574. 100. Langlet F, Haeusler RA, Lindén D et al. Selective inhibition of FOXO1 activator/repressor balance modulates hepatic glucose handling. Cell. 2017;171:824–835. 101. Unterman TG. Regulation of hepatic glucose metabolism by FoxO proteins, an integrated approach. Curr Top Dev Biol. 2018;127:119–147. 102. Kikuchi O, Kobayashi M, Amano K et al. FoxO1 gain of function in the pancreas causes glucose intolerance, polycystic pancreas, and islet hypervascularization. PLOS ONE. 2012;7:e32249. 103. Kim JJ, Li P, Huntley J, Chang JP et al. FoxO1 haploinsufficiency protects against high-fat diet-induced insulin resistance with enhanced peroxisome proliferator-activated receptor gamma activation in adipose tissue. Diabetes. 2009;58:1275–1282. 104. Lundell LS, Massart J, Altıntaş A et al. Regulation of glucose uptake and inflammation markers by FOXO1 and FOXO3 in skeletal muscle. Mol Metab. 2019;20:79–88. 105. Melnik BC. p53: Key conductor of all anti-acne therapies. J Transl Med. 2017;15:195. 106. Kung CP, Murphy ME. The role of the p53 tumor suppressor in metabolism and diabetes. J Endocrinol. ­ 2016;231:61–75. 101 107. Strycharz J, Drzewoski J, Szemraj J, Sliwinska A. Is p53 involved in tissue-specific insulin resistance formation? Oxid Med Cell Longev. 2017;2017:9270549. 108. Minamino T, Orimo M, Shimizu I et al. A crucial role for adipose tissue p53 in the regulation of insulin resistance. Nat Med. 2009;15:1082–1087. 109. Pappas K, Xu J, Zairis S, Resnick-Silverman L et al. p53 maintains baseline expression of multiple tumor suppressor genes. Mol Cancer Res. 2017;15:1051–1062. 110. Krupková M, Janků M, Liska F et al. Pharmacogenetic model of retinoic acid-induced dyslipidemia and insulin resistance. Pharmacogenomics. 2009;10:1915–1927. 111. Karadag AS, Ertugrul DT, Kalkan G et al. The effect of acitretin treatment on insulin resistance, retinol-binding protein-4, leptin, and adiponectin in psoriasis vulgaris: A noncontrolled study. Dermatology. 2013;227:103–108. 112. Corbetta S, Angioni R, Cattaneo A et al. Effects of retinoid therapy on insulin sensitivity, lipid profile and circulating adipocytokines. Eur J Endocrinol. 2006;154:83–86. 113. Miyazaki S, Taniguchi H, Moritoh Y et al. Nuclear hormone retinoid X receptor (RXR) negatively regulates the glucosestimulated insulin secretion of pancreatic ß-cells. Diabetes. 2010;59:2854–2861. 114. Kane MA, Folias AE, Pingitore A et al. Identification of 9-cisretinoic acid as a pancreas-specific autacoid that attenuates glucose-stimulated insulin secretion. Proc Natl Acad Sci USA. 2010;107:21884–218849. 115. Montessuit C, Papageorgiou I, Lerch R. Nuclear receptor agonists improve insulin responsiveness in cultured cardiomyocytes through enhanced signaling and preserved cytoskeletal architecture. Endocrinology. 2008;149:1064–1074. 116. Lee SE, Koo YD, Lee JS et al. Retinoid X receptor α overexpression alleviates mitochondrial dysfunction-induced insulin resistance through transcriptional regulation of insulin receptor substrate 1. Mol Cells. 2015;38:356–361. 117. Scarisbrick JJ, Morris S, Azurdia R et al. U.K. consensus statement on safe clinical prescribing of bexarotene for patients with cutaneous T-cell lymphoma. Br J Dermatol. 2013;168:192–200. 118. Mukherjee R, Davies PJ, Crombie DL et al. Sensitization of diabetic and obese mice to insulin by retinoid X receptor agonists. Nature. 1997;386:407–410. 119. Guleria RS, Singh AB, Nizamutdinova IT et al. Activation of retinoid receptor-mediated signaling ameliorates diabetesinduced cardiac dysfunction in Zucker diabetic rats. J Mol Cell Cardiol. 2013;57:106–118. 120. Staels B. Regulation of lipid and lipoprotein metabolism by retinoids. J Am Acad Dermatol. 2001;45:158–167. 121. Klör HU, Weizel A, Augustin M et al. The impact of oral vitamin A derivatives on lipid metabolism—What recommendations can be derived for dealing with this issue in the daily dermatological practice? J Dtsch Dermatol Ges. 2011 9:600–606. 122. Lilley JS, Linton MF, Fazio S. Oral retinoids and plasma lipids. Dermatol Ther. 2013;26:404–410. 123. Neal JM. Retinoid-induced hypertriglyceridemia. Endocr Pract. 2003 9:168. 124. Nieto-Rementería N, Pérez-Yarza G, Boyano MD et al. Bexarotene activates the p53/p73 pathway in human cutaneous T-cell lymphoma. Br J Dermatol. 2009;160:519–526. 125. Melnik B, Bros U, Plewig G. Characterization of apoprotein metabolism and atherogenic lipoproteins during oral isotretinoin treatment. Dermatologica. 1987;175:158–168. 102 126. Gerber LE, Erdman JW Jr. Comparative effects of all-trans and 13-cis retinoic acid administration on serum and liver lipids in rats. J Nutr. 1980;110:343–351. 127. Standeven AM, Beard RL, Johnson AT et al. Retinoidinduced hypertriglyceridemia in rats is mediated by retinoic acid receptors. Fundam Appl Toxicol. 1996;33:264–271. 128. Heo SH, Kwak J, Jang KL. All-trans retinoic acid induces p53–depednent apoptosis in human hepatocytes by activating p14 expression via promoter hypomethylation. Cancer Lett. 2015;362:139–148. 129. Ashur-Fabian O, Har-Zahav A, Shaish A et al. apoB and apobec1, two genes key to lipid metabolism, are transcriptionally regulated by p53. Cell Cycle. 2010;9:3761–3770. 130. Kamagate A, Dong HH. FoxO1 integrates insulin signaling to VLDL production. Cell Cycle. 2008;7:3162–3170. 131. Kim DH, Zhang T, Ringquist S, Dong HH. Targeting FoxO1 for hypertriglyceridemia. Curr Drug Targets. 2011;12:1245–1255. 132. Pan X, Munshi MK, Iqbal J et al. Circadian regulation of intestinal lipid absorption by apolipoprotein AIV involves forkhead transcription factors A2 and O1 and microsomal triglyceride transfer protein. J Biol Chem. 2013;288:20464–20476. 133. Rodondi N, Darioli R, Ramelet AA et al. High risk for hyperlipidemia and the metabolic syndrome after an episode of hypertriglyceridemia during 13-cis retinoic acid therapy for acne: A pharmacogenetic study. Ann Intern Med. 2002;136:582–589. 134. Ashley JM, Lowe NJ, Borok ME, Alfin-Slater RB. Fish oil supplementation results in decreased hypertriglyceridemia in patients with psoriasis undergoing etretinate or acitretin therapy. J Am Acad Dermatol. 1988;19:76–82. 135. Chan BC, Reid N, Armour K et al. Hypertriglyceridaemia with acitretin use: A proposal for its management in the context of overall cardiovascular risk. Br J Dermatol. 2014;171:665–667. 136. Lin JC, Massera D, Ghalib M et al. Hyperlipidemia secondary to acitretin therapy for lamellar ichthyosis associated with a NIPAL4 mutation improves on a plant-based diet and relapses on a standard Western diet. Clin Nutr ESPEN. 2018;24:54–57. 137. Zhou X, Zhu W, Shen M, He Y et al. Frizzled-related proteins 4 (SFRP4) rs1802073G allele predicts the elevated serum lipid levels during acitretin treatment in psoriatic patients from Hunan, China. PeerJ. 2018;6:e4637. 138. Standeven AM, Thacher SM, Yuan YD et al. Retinoid X receptor agonist elevation of serum triglycerides in rats by potentiation of retinoic acid receptor agonist induction or by action as single agents. Biochem Pharmacol. 2001;62:1501–1509. 139. Heitel P, Achenbach J, Moser D et al. DrugBank screening revealed alitretinoin and bexarotene as liver X receptor modulators. Bioorg Med Chem Lett. 2017;27:1193–1198. 140. Aktürk AŞ, Güzel S, Bulca S et al. Effects of isotretinoin on serum vitamin E levels in patients with acne. Int J Dermatol. 2013;52:363–366. 141. Cabello I, Servitje O, Corbella X et al. Omega-3 fatty acids as adjunctive treatment for bexarotene-induced hypertriglyceridaemia in patients with cutaneous T-cell lymphoma. Clin Exp Dermatol. 2017;42:276–281. 142. Reichrath J, Saternus R, Vogt T. Endocrine actions of vitamin D in skin: Relevance for photocarcinogenesis of nonmelanoma skin cancer, and beyond. Mol Cell Endocrinol. 2017;453:96–102. Retinoids in Dermatology 143. Vedell PT, Lu Y, Grubbs CJ et al. Effects on gene expression in rat liver after administration of RXR agonists: UAB30, 4-methyl-UAB30, and Targretin (Bexarotene). Mol Pharmacol. 2013;83:698–708. 144. Lalloyer F, Pedersen TA, Gross B et al. Rexinoid bexarotene modulates triglyceride but not cholesterol metabolism via gene-specific permissivity of the RXR/LXR heterodimer in the liver. Arterioscler Thromb Vasc Biol. 2009;29:1488–1495. 145. Vu-Dac N, Gervois P, Torra IP et al. Retinoids increase human apo C-III expression at the transcriptional level via the retinoid X receptor. Contribution to the hypertriglyceridemic action of retinoids. J Clin Invest. 1998;102:625–632. 146. Sundaram M, Zhong S, Khalil MB et al. Expression of apolipoprotein C-III in McA-RH7777 cells enhances VLDL assembly and secretion under lipid-rich conditions. J Lipid Res. 2010;51:150–161. 147. Mendivil CO, Zheng C, Furtado J et al. Metabolism of verylow-density lipoprotein and low-density lipoprotein containing apolipoprotein C-III and not other small apolipoproteins. Arterioscler Thromb Vasc Biol. 2010;30:239–245. 148. Katz RA, Jorgensen H, Nigra TP. Elevation of serum triglyceride levels from oral isotretinoin in disorders of keratinization. Arch Dermatol. 1980;116:1369–1372. 149. Jamshidi M, Obermeyer RJ, Govindaraj S et al. Acute pancreatitis secondary to isotretinoin-induced hyperlipidemia. J Okla State Med Assoc. 2002;95:79–80. 150. Tejedor Tejada J, Torres Yuste R, García Pajares F. Acute pancreatitis secondary to treatment with isotretinoin. Gastroenterol Hepatol. 2019;42:256. 151. Turer AT, Scherer PE. Adiponectin: Mechanistic insights and clinical implications. Diabetologia. 2012;55:2319–2326. 152. Achari AE, Jain SK. Adiponectin, a therapeutic target for obesity, diabetes, and endothelial dysfunction. Int J Mol Sci. 2017;18(6). 153. Mantzoros CS, Magkos F, Brinkoetter M et al. Leptin in human physiology and pathophysiology. Am J Physiol Endocrinol Metab. 2011;301:567–584. 154. Pan H, Guo J, Su Z. Advances in understanding the interrelations between leptin resistance and obesity. Physiol Behav. 2014;130:157–169. 155. Aydin K, Çetinözman F, Elcin G et al. Suppressed adiponectin levels and increased adiponectin response to oral glucose load in lean women with severe acne normalizes after isotretinoin treatment. Dermatology. 2017;233:314–319. 156. Cemil BC, Ayvaz HH, Ozturk G et al. Effects of isotretinoin on body mass index, serum adiponectin, leptin, and ghrelin levels in acne vulgaris patients. Postepy Dermatol Alergol. 2016;33:294–299. 157. Christou GA, Kiortsis DN. Adiponectin and lipoprotein metabolism. Obes Rev. 2013;14:939–949. 158. Krskova-Tybitanclova K, Macejova D, Brtko J et al. Short term 13-cis-retinoic acid treatment at therapeutic doses elevates expression of leptin, GLUT4, PPARgamma and aP2 in rat adipose tissue. J Physiol Pharmacol. 2008;59:731–743. 159. Landrier JF, Kasiri E, Karkeni E et al. Reduced adiponectin expression after high-fat diet is associated with selective upregulation of ALDH1A1 and further retinoic acid receptor signaling in adipose tissue. FASEB J. 2017;31:203–211. 160. Kovács D, Lovászi M, Póliska S et al. Sebocytes differentially express and secrete adipokines. Exp Dermatol. 2016;25:194–199. Endocrine and Metabolic Side Effects 161. Jung YR, Lee JH, Sohn KC et al. Adiponectin signaling regulates lipid production in human sebocytes. PLOS ONE. 2017;12:e0169824. 162. Agra RM, Teijeira-Fernández E, Pascual-Figal D et al. Adiponectin and p53 mRNA in epicardial and subcutaneous fat from heart failure patients. Eur J Clin Invest. 2014;44:29–37. 163. Çölgeçen E, Özyurt K, Ferahbaş Kesikoğlu A. The effect of systemic isotretinoin treatment on skin biophysical parameters among patients with acne vulgaris. Turk J Med Sci. 2016;46:1641–1644. 164. Lee JE, Chang JY, Lee SE et al. Epidermal hyperplasia and elevated HB-EGF are more prominent in retinoid dermatitis compared with irritant contact dermatitis induced by benzalkonium chloride. Ann Dermatol. 2010;22:290–299. 165. Mihály J, Gericke J, Lucas R et al. TSLP expression in the skin is mediated via RARγ-RXR pathways. Immunobiology. 2016;221:161–165. 166. Hatayama T, Segawa R, Mizuno N et al. All-trans retinoic acid enhances antibody production by inducing the expression of thymic stromal lymphopoietin protein. J Immunol. 2018;200:2670–2676. 167. Gericke J, Ittensohn J, Mihály J et al. Regulation of retinoidmediated signaling involved in skin homeostasis by RAR and RXR agonists/antagonists in mouse skin. PLOS ONE. 2013;8:e62643. 168. Bellemère G, Von Stetten O, Oddos T. Retinoic acid increases aquaporin 3 expression in normal human skin. J Invest Dermatol. 2008;128:542–548. 169. Xing F, Liao W, Jiang P et al. Effect of retinoic acid on aquaporin 3 expression in keratinocytes. Genet Mol Res. 2016;15:15016951. 170. Guo L, Chen H, Li Y et al. An aquaporin 3-notch1 axis in keratinocyte differentiation and inflammation. PLOS ONE. 2013;8:e80179. 171. Zheng X, Chen X. Aquaporin 3, a glycerol and water transporter, is regulated by p73 of the p53 family. FEBS Lett. 2001;489:4–7. 172. Pearce DJ, Klinger S, Ziel KK et al. Low-dose acitretin is associated with fewer adverse events than high-dose acitretin in the treatment of psoriasis. Arch Dermatol. 2006;142:1000–1004. 173. Choudhary V, Olala LO, Kagha K et al. Regulation of the glycerol transporter, aquaporin-3, by histone deacetylase-3 and p53 in keratinocytes. J Invest Dermatol. 2017;137:1935–1944. 174. Jiang YJ, Lu B, Kim P et al. Regulation of ABCA1 expression in human keratinocytes and murine epidermis. J Lipid Res. 2006;47:2248–2258. 175. Kuntz M, Candela P, Saint-Pol J et al. Bexarotene promotes cholesterol efflux and restricts apical-to-basolateral transport of amyloid-β peptides in an in vitro model of the human blood-brain barrier. J Alzheimers Dis. 2015;48:849–862. 176. Kumari V, Timm K, Kühl AA et al. Impact of systemic alitretinoin treatment on skin barrier gene and protein expression in patients with chronic hand eczema. Br J Dermatol. 2016;175:1243–1250. 177. Lee HC, Headley MB, Iseki M et al. Cutting edge: Inhibition of NF-kappaB-mediated TSLP expression by retinoid X receptor. J Immunol. 2008;181:5189–5193. 178. Schmuth M, Moosbrugger-Martinz V, Blunder S, Dubrac S. Role of PPAR, LXR, and PXR in epidermal homeostasis and inflammation. Biochim Biophys Acta. 2014;1841:463–473. 103 179. Korkmaz E, Cetinkaya N, Oz M et al. The possibly reversible isotretinoin effect of decreased ovarian reserve in SpragueDawley albinos: Part I, biochemical analyses. Gynecol Obstet Invest. 2017;82:72–77. 180. Abali R, Yuksel MA, Aktas C et al. Decreased ovarian reserve in female Sprague-Dawley rats induced by isotretinoin (retinoic acid) exposure. Reprod Biomed Online. 2013;27:184–191. 181. Yang H, Xie Y, Yang D, Ren D. Oxidative stress-induced apoptosis in granulosa cells involves JNK, p53 and Puma. Oncotarget. 2017; 8:25310–25322. 182. Melnik BC. Apoptosis may explain the pharmacological mode of action and adverse effects of isotretinoin, including teratogenicity. Acta Derm Venereol. 2017;97:173–181. 183. Aksoy H, Cinar L, Acmaz G et al. The effect of isotretinoin on ovarian reserve based on hormonal parameters, ovarian volume, and antral follicle count in women with acne. Gynecol Obstet Invest. 2015;79:78–82. 184. Cinar SL, Kartal D, Aksoy H et al. Long-term effect of systemic isotretinoin on female fertility. Cutan Ocul Toxicol. 2017;36:132–134. 185. Öztürk S, Öztürk T, Ucak H et al. Evaluation of ovarian reserve and function in female patients treated with oral isotretinoin for severe acne: An exploratory study. Cutan Ocul Toxicol. 2015;34:21–24. 186. Sikar Aktürk A, Abalı R, Yüksel MA et al. The effects of isotretinoin on the ovarian reserve of females with acne. Gynecol Endocrinol. 2014;30:30–33. 187. Geiger JM, Walker M. Is there a reproductive safety risk in male patients treated with acitretin (neotigason/soriatane)? Dermatology. 2002;205:105–107. 188. Millsop JW, Heller MM, Eliason MJ, Murase JE. Dermatological medication effects on male fertility. Dermatol Ther. 2013;26:337–346. 189. Ustun I, Rifaioglu EN, Sen BB et al. Gynecomastia: A rare complication of isoretinoin? Cutan Ocul Toxicol. 2013;32:93–94. 190. Gualtieri B, Ingegneri A, Chiricozzi A, Romanelli M. Gynecomastia following isotretinoin treatment: A rare endocrine side effect. G Ital Dermatol Venereol. 2018 Oct 3; doi: 10.23736/S0392-0488.18.06022-4. [Epub ahead of print]. 191. Roodsari MR, Akbari MR, Sarrafi-rad N et al. The effect of isotretinoin treatment on plasma homocysteine levels in acne vulgaris. Clin Exp Dermatol. 2010;35:624–626. 192. Karadag AS, Tutal E, Ertugrul DT, Akin KO. Effect of isotretinoin treatment on plasma holotranscobalamin, vitamin B12, folic acid, and homocysteine levels: Non-controlled study. Int J Dermatol. 2011;50:1564–1569. 193. Zouboulis CC, Seltmann H, Abdel-Naser MB et al. Effects of extracellular calcium and 1,25 dihydroxyvitamin D3 on sebaceous gland cells In vitro and In vivo. Acta Derm Venereol. 2017;97:313–320. 194. Ertugrul DT, Karadag AS, Tutal E, Akin KO. Does isotretinoin have effect on vitamin D physiology and bone metabolism in acne patients? Dermatol Ther. 2011;24:291–295. 195. El-Hamd MA, El Taieb MA, Ibrahim HM, Aly SS. Vitamin D levels in acne vulgaris patients treated with oral isotretinoin. J Cosmet Dermatol. 2019;18:16–20. 196. Reichrath J, Reichrath S, Heyne K et al. Tumor suppression in skin and other tissues via cross-talk between vitamin D- and p53-signaling. Front Physiol. 2014; 5:166.Facimento essenis 18 Other Systemic Side Effects: Cardiovascular, Pulmonary, Otolaryngorhinologic, Genitourinary, Renal, and Immunologic Emin Ozlu, Akif Bilgen, and Ayse Serap Karadag Introduction Vitamin A, also known as retinol, is found in both vegetal and animal diets. Humans can also be exposed to vitamin A and its derivatives (retinoids) pharmacologically, as in the case of treatment for dermatologic and hematologic disorders. The levels of vitamin A in the blood may be exceeded due to both inappropriate use and treatment for diseases. Symptoms of acute vitamin A toxicity include headache, hepatic swelling, vomiting, and diarrhea. Chronic vitamin A toxicity may lead to various symptoms including increased irritability, confusion, anxiety disorders, depression, and suicidal ideation (1). Pseudotumor cerebri may rarely be seen. In addition, impotence can be seen in men (2). The mechanism of these side effects remains unknown (1). Retinoids are a group of compounds derived from natural vitamin A and synthetic analogs. Retinoids can be categorized into three groups based on their molecular structures: first, second, and third generation. Currently, retinoids are used in several fields of dermatology. Although retinoids are very effective agents, unwanted side effects can occur whether used topically or systemically. The most common side effects associated with topical retinoids are skin reactions, with systemic side effects being quite rare. Systemic side effects of oral retinoid therapy are well known. Isotretinoin is the most commonly used agent, and so it is responsible for most of the reported systemic side effects (3). Retinoidrelated cardiovascular, otolaryngologic, pulmonary, and urinary side effects are based on limited studies and case reports. In this chapter, we focus on the side effects of retinoids, primarily in the cardiologic, otolaryngorhinologic, genitourinary, renal, and immunologic systems. Retinoid-related adverse events related to other systems are mentioned in Chapters 11 through 17. Retinoids and Side Effects Associated with the Cardiovascular System Cardiovascular side effects associated with retinoid use are not common. Many studies have suggested that there is no link between oral isotretinoin and cardiovascular side effects (4–6). One study demonstrated that 3-month isotretinoin therapy did not affect heart rate, blood pressure, or P- and QT-wave measurements (4) Another study found that the use of isotretinoin for 6 months at a dose of 0.8 mg/kg/day did not have an arrhythmic effect (5). A previous study found that the use of 0.8 mg/kg/day of isotretinoin for 6 months in acne patients did not prolong the QT interval and did not increase QT dispersion (6). Only a few case reports of cardiovascular side effects associated with usage of isotretinoin have been reported (7–12). Sinus tachycardia associated with isotretinoin use appeared in one patient. Sinus tachycardia, plus a right bundle branch block, developed in an 18-year-old patient after 3 months of receiving isoretinoin (8). There are also instances of atrial tachycardia due to isotretinoin (9–10). In one patient, premature ventricular contractions (11), and a 26-year-old woman developed not only atrial tachycardia but also pericardial effusion while on an isotretinoin regimen (12). Retinoids are involved in the signaling pathways affecting embryonic development. The use of isotretinoin during pregnancy may cause many developmental defects, including defects of the cardiovascular system; however, the cellular and m ­ olecular mechanisms of the developmental toxicity of isotretinoin are unclear. In one study, developmental toxicity induced by isotretinoin ­during early cardiac differentiation was investigated using human-induced pluripotent stem cells and human embryonic stem cells. This study showed that oral isotretinoin affected cardiac differentiation by disrupting mesodermal differentiation (13). Oral isotretinoin has also been suggested to affect the coagulation process, but the mechanism for this is also unknown (14). In a previous study of 30,496 patients who had previously used isotretinoin it was found that its use was not associated with the risk of cardiovascular, cerebrovascular, or thromboembolic events (15). There are only few case reports available in the literature about side effects of isotretinoin on the coagulation system (14,16,17). An acute myocardial infarction developed in a 28-year-old patient taking isotretinoin (16). Two elderly patients taking low-dose isotretinoin had vascular complications (14). Cerebral ischemia in a 30-year-old male patient taking isotretinoin was reported (17). Palpitation and a cerebral vascular accident have occurred in patients treated with oral isotretinoin (18). According to the package insert, capillary leak syndrome, chest pain, cyanosis, increasing bleeding time, intermittent claudication, and peripheral ischemia have all been reported in patients receiving acitretin (19). While the cardiovascular side effects associated with the use of oral isotretinoin are limited to several case reports, such cardiovascular side effects associated with other retinoids have not been reported to date. 105 106 Retinoids and Side Effects Associated with the Respiratory System Systemic Isotretinoin Studies on the effect of systemic isotretinoin on the respiratory system are very limited (20). A study has suggested that nasal mucociliary clearance was elongated in acne patients using isotretinoin. While there was a correlation between drug dose and mucociliary clearance, an isotretinoin regimen did not affect pulmonary function tests (20). Another study found that fetal lung development was accelerated in patients receiving isotretinoin during pregnancy (21). There is only a single report of respiratory side effects associated with usage of isotretinoin, which suggested that there was a significant decrease in forced expiratory flow rate in acne patients taking isotretinoin compared to the control group (22). In addition, two case reports stated that oral isotretinoin triggered bronchospasm (23,24). In another report, allergic pneumonia developed while the subject was taking isotretinoin (25). Other Retinoids The pulmonary side effects associated with retinoids other than oral isotretinoin are quite limited. A previous study on human patients with emphysema suggested that definitive clinical improvement could not be achieved with the administration of retinoids (26). To date, three cases have been reported, where patients developed retinoic acid syndrome due to the use of acitretin for treatment of psoriasis (27–29). Retinoic acid syndrome often develops in patients receiving all-trans-retinoic acid (ATRA) therapy for promyelocytic leukemia. It is characterized by fever, acute renal failure, respiratory distress, hypotension, pleural effusion, and weight gain (30). A 63-year-old patient with significant psoriasis who developed a drug fever attributed to acitretin was reported (31). The package insert also indicates that sinusitis, coughing, increased sputum, and laryngitis may occur (19). In light of the current literature, we believe that retinoids are not associated with respiratory side effects. Large controlled studies of respiratory side effects are essential for a definitive conclusion to be made. Retinoids and Side Effects Associated with the Ear, Nose, and Throat The otorhinolaryngological effects of oral isotretinoin are limited to a very few studies (32–35). Thirty-eight acne patients were evaluated with audiometric tests before treatment and after the first, second, and third weeks of treatment initiation. Oral isotretinoin increased hearing level at all audiometric frequencies (32). Another study with the use of oral isotretinoin for 3 weeks due to acne caused subclinical changes in auditory brainstem response (33). An additional study of 32 patients showed that isotretinoin use caused significant changes in the audiologic and ocular nerve (or retinal) functions (34). Another group has proposed that oral isotretinoin use at a dose of 0.3–0.6 mg/kg/day for acne may cause bilateral hearing threshold changes (35). Retinoids in Dermatology Retinol plays an important role in the normal development of the organ of Corti. In a rat study, retinoic acid was shown to accelerate the regeneration of hair cells in the inner ear (36). Retinoids are known to increase epithelial proliferation, induce mucociliary differentiation, and inhibit squamous cell differentiation in epithelial cells (37). It is also known that oral isotretinoin affects the nose and skin flora (38). In a study investigating the effect of oral isotretinoin on antibiotic-resistant Propionibacterium colonization of the skin and nasal mucosa in acne patients, oral isotretinoin significantly decreased antibioticresistant Propionibacterium levels (38). In another study, the effects of different treatments for acne on oral and nasopharyngeal flora were evaluated. In this study, which was performed with 55 acne patients and 20 healthy controls, four subgroups were formed of patients receiving topical treatment, oral isotretinoin, systemic tetracycline, and the control group. The oral and nasopharyngeal flora did not change after 3 months of treatment in the oral isotretinoin group (39). In another study, the effects of oral isotretinoin and oral antibiotics on the microbial flora in the oropharynx, nose, and feces were evaluated and a significant increase was shown in nasal Staphylococcus aureus carriage after oral isotretinoin treatment (40). Retinoid use after nasal surgery may increase the risk of complications. Nasal deformity developed in three patients receiving oral isotretinoin after rhinoplasty operations (41). In two additional patients, lip and perioral abscesses developed due to isotretinoin use (42,43). The package inserts indicate that both systemic isotretinoin and acitretin may cause tinnitus and hearing impairment (18,19). Isotretinoin-related voice alteration, and acitretinrelated earache and taste loss have also been reported (18,19). The teratogenic effects resulting from oral administration of isotretinoin, known as the retinoic acid syndrome, are characterized by craniofacial dysmorphism and neural tube defects. Isotretinoin directly affects the development of cranial neural crest cells (44). An 8-year-old girl who was exposed to isotretinoin prior to birth reportedly developed a left canal cholesteatoma (45). Malformation of both ears was reported in the child of a woman who became pregnant 1 month after isotretinoin was stopped (46). An asymmetric crying face developed in the newborn child of a mother who was exposed to isotretinoin in the first month of pregnancy (47). Hypoacusia and tinnitus occurred in a 15-yearold boy receiving isotretinoin for acne (48). Two fetuses exposed to isotretinoin were also shown to have developed temporal bone pathology (49). The use of oral isotretinoin during pregnancy is known to cause congenital anomalies in other parts of the otolaryngologic system; however, there are few studies that have investigated the effects of oral isotretinoin on the ears, nose, and throat in adults that revealed contradictory findings, but these are limited to isotretinoin (32–35,44). The Effects of Retinoids on the Genitourinary System and Fertility Systemic Isotretinoin In mammals, retinoic acid regulates testicular activity by affecting retinoic acid receptors (RARs) and retinoid X receptors 107 Other Systemic Side Effects (RXRs) (50). The results of studies on the effects of systemic isotretinoin on spermatogenesis are controversial (51–54); however, it was also stated in one study that spermatogenesis was not affected in rats that had been administered a toxic dose of isotretinoin (55). Human studies investigating the effects of isotretinoin on male fertility have shown that isotretinoin affects fertility (56–58). In another study, a positive effect on spermatogenesis was seen in patients using oral isotretinoin for acne conglobata 6 months after the beginning of treatment; however, it was determined that the values returned to the pretreatment baseline levels 1 year after cessation of treatment (59). The effect of oral isotretinoin on female fertility and ovarian reserve and functions is not clear. In some studies, it has been shown that isotretinoin negatively affects ovarian reserve and functions (60,61). One study found that isotretinoin did not affect ovarian functions (62), while another study reported that ovarian reserve and functions were impaired at the end of 6 months of oral isotretinoin treatment, but returned to the pretreatment baseline level 1 year after cessation of treatment. The authors suggested that the disruptive effect of oral isotretinoin on ovarian reserve was transient (63). Retinoids have antiproliferative, anti-inflammatory, and immunomodulatory effects. As a result, retinoids have been shown to reduce glomerular and tubular damage, plus inflammation in glomerulonephritis and renal interstitial disease (64); however, there are cases where renal side effects have been reported after systemic isotretinoin use (64–66). A 17-year-old girl developed acute renal failure and a 16-year-old boy developed eosinophilic tubulointerstitial nephritis after isotretinoin use (64,65). Perinuclear antineutrophil cytoplasmic antibody-positive vasculitis, oligoarthritis, tendinitis, and myositis developed in a 15-year-old boy 6 weeks after the initiation of oral isotretinoin treatment (66). Isotretinoin-related glomerulonephritis has also been reported (18). Because the number of case reports is limited, it is possible that these side effects are coincidental rather than causal. The available data on the effects of systemic isotretinoin on the urinary system are limited. In a controlled study, there was no statistically significant difference in the prevalence of hematuria between acne patients using isotretinoin and the control group (67). A 16-year-old boy developed terminal hematuria following 1 month of isotretinoin treatment (68). Isotretinoin treatment may also cause urethritis (69) and dermatitis affecting the urinary meatus (70). Although the effects of isotretinoin on uric acid levels were first mentioned 30 years ago, current information on this topic is limited (7,71). Hyperuricemia, hypercalcemia, and nephrolithiasis developed after isotretinoin use in one patient (7). Uric acid levels were measured before treatment and 1 and 2 months after treatment in 51 acne patients taking 0.5 mg/kg/day of oral isotretinoin. The uric acid levels at 1 and 2 months after treatment began were significantly higher than pretreatment levels (71). Other Retinoids Acitretin is believed to have no effect on spermatogenesis; however, the evidence is limited. In one study, acitretin did not affect spermatogenesis in rats at standard and high doses (72). In another study conducted with 10 men receiving acitretin treatment for 3 months, acitretin did not affect spermatogenesis, sperm motility, or sperm morphology (73). The pregnancies of nine women who became pregnant while their partners were receiving acitretin were evaluated. Spontaneous abortions occurred in six women, while two other women had induced abortions; only one woman carried to term and gave birth (74). In light of the current data, it is recommended that partners of men who use acitretin use contraception, but the risk of fetal anomalies is very low when their partners do become pregnant. The literature on the effects of retinoids other than isotretinoin on uric acid levels are limited. In one patient, gouty tophi developed with very high uric acid levels after acitretin use (75). A population-based study showed a positive correlation between retinol levels and uric acid levels (76). The effect of retinoids on the urinary system remains unknown. The limited data available show that large, comprehensive studies of renal side effects are necessary for a definitive conclusion to be made. Retinoids and Hypersensitivity Reactions Allergic reactions, such as urticaria and angiedema related to retinoid use, are extremely rare. Angioedema occurred in three patients treated with acitretin to date: one patient with urticaria and two patients without urticaria (77–79). Angioedema has occurred in four patients treated with isotretinoin: two cases with and two cases without urticaria (77,80–82). The mechanism of the retinoid-induced angioedema or urticaria is unclear. Conclusions Retinoids are essential drugs that are successfully used to treat many skin conditions. The known side effects appear to be quite rare and transient. Because isotretinoin is currently the most commonly used oral retinoid, most reported side effects are associated with isotretinoin. REFERENCES 1. de Oliveira MR. Vitamin A and retinoids as mitochondrial toxicants. Oxid Med Cell Longev. 2015;2015:140267. 2. Boyd AS. An overview of the retinoids. Am J Med. 1989;86:568–574. 3. Khalil S, Bardawil T, Stephan C et al. Retinoids: A journey from the molecular structures and mechanisms of action to clinical uses in dermatology and adverse effects. J Dermatolog Treat. 2017;28:684–696. 4. Karadag AS, Gumrukcuoglu HA, Gunes Bilgili S et al. Does isotretinoin therapy have any effects on electrocardiography, heart rate and blood pressure? J Dermatolog Treat. 2012;23:168–171. 5. Selcoki Y, Gorpelioglu C, Turgut F et al. Isotretinoin: Is there any arrhythmic effect? Int J Dermatol. 2008;47:195–197. 6. Dursun R, Alpaslan M, Caliskan M et al. Isotretinoin does not prolong QT intervals and QT dispersion in patients with severe acne: A surprising finding for a drug with numerous side effects. J Drugs Dermatol. 2011;10:710–714. 7. Bigby M, Stern RS. Adverse reactions to isotretinoin. A report from the Adverse Drug Reaction Reporting System. J Am Acad Dermatol. 1988;18:543–552. 108 8. Charalabopoulos K, Papalimneou V, Charalabopoulos A, Hatzis J. Two new adverse effects of isotretinoin. Br J Dermatol. 2003;148:593. 9. Hasdemir C, Sagcan A, Sekuri C et al. Isotretinoin (13-cisretinoic acid) associated atrial tachycardia. Pacing Clin Electrophysiol. 2005;28:348–349. 10. Dresden G. Atrial tachycardia associated with isotretinoin use. Arch Dermatol. 2007;143:1084–1085. 11. Kiliç E, Sahin M, Sahin S, Ozer S. Isotretinoin (13-cis-retinoic acid)-associated premature ventricular contractions. Turk J Pediatr. 2009;51:387–388. 12. Güler E, Babur Güler G, Yavuz C, Kızılırmak F. An unknown side effect of isotretinoin: Pericardial effusion with atrial tachycardia. Anatol J Cardiol. 2015;15:168–169. 13. Liu Q, Van Bortle K, Zhang Y et al. Disruption of mesoderm formation during cardiac differentiation due to developmental exposure to 13-cis-retinoic acid. Sci Rep. 2018;8:12960. 14. Sambandan DR, Ratner D. Vascular complications after treatment with low-dose isotretinoin in two elderly patients. Dermatol Surg. 2011;37:726–728. 15. Bérard A, Azoulay L, Nakhai-Pour HR, Moussally K. Isotretinoin and the risk of cardiovascular, cerebrovascular and thromboembolic disorders. Dermatology. 2011;223:45–51. 16. Lorenzo N, Antuña P, Dominguez L et al. Acute myocardial infarction in a young woman on isotretinoin treatment. Int J Cardiol. 2015;181:39–41. 17. Laroche ML, Macian-Montoro F, Merle L, Vallat JM. Cerebral ischemia probably related to isotretinoin. Ann Pharmacother. 2007;41:1073–1076. 18. Drugs@FDA: FDA Approved Drug Products—Accutane® (isotretinoin capsules) NDA 018662:1-46. 19. Drugs@FDA: FDA Approved Drug Products—Soriatane® (acitretin) Capsules. NDA 019821/S-024:3-40. 20. Gorpelioglu C, Ozol D, Sarifakioglu E. Influence of isotretinoin on nasal mucociliary clearance and lung function in patients with acne vulgaris. Int J Dermatol. 2010;49:87–90. 21. Fauchère JC, Ersch J, Grant DA et al. Acceleration of lung maturation in a human fetus following maternal isotretinoin intake. Biol Neonate. 2006;90:203–206. 22. Kapur N, Hughes JR, Rustin MH. Exacerbation of asthma by isotretinoin. Br J Dermatol. 2000;142:388–389. 23. Fisher DA. Exercise-induced bronchoconstriction related to isotretinoin therapy. J Am Acad Dermatol. 1985;13:524. 24. Sabroe RA, Staughton RCD, Bunker CB. Bronchospasm induced by isotretinoin. BMJ. 1996;312:886. 25. Oliviero G, Constans P, Caby I et al. Lung disease induced by isotretinoin. Rev Mal Respir. 1995;12:631–633. 26. Roth MD, Connett JE, D’Armiento JM et al. Feasibility of retinoids for the treatment of emphysema study. Chest. 2006;130:1334–1345. 27. Cuhadaroglu C, Korular D, Erelel M et al. Respiratory distress with acitretin, reversal by corticosteroid. Dermatol Online J. 2001;7:5. 28. Liu D, Cao F, Yan X et al. Retinoic acid syndrome in a patient with psoriasis. Eur J Dermatol. 2009;19:632–634. 29. Gu W, Zhao G, Shi F. Acitretin-induced retinoic acid syndrome. J Am Acad Dermatol. 2011;65:e148–e149. 30. De Botton S, Dombret H, Sanz M et al. Incidence, clinical features, and outcome of all-trans-retinoic acid syndrome in 413 cases of newly diagnosed acute promyelocytic leukemia. The European APL Group. Blood. 1998;92:2712–2718. Retinoids in Dermatology 31. Rob F, Fialová J, Brejchová M et al. Drug fever as an adverse effect of acitretin in complicated psoriasis patient. Dermatol Ther. 2015;28:366–368. 32. Karabulut H, Karadag AS, Acar B et al. The effect of oral isotretinoin (13-cis retinoic acid) on hearing systems in patients with acne vulgaris: A prospective study. Int J Dermatol. 2011;50:1139–1143. 33. Nikiforidis G, Tsambaos D, Karamitsos D et al. Effects of oral isotretinoin on human auditory brainstem response. Dermatology. 1994;189:62–64. 34. Aydogan K, Turan OF, Onart S et al. Neurological and neurophysiological effects of oral isotretinoin: A prospective investigation using auditory and visual evoked potentials. Eur J Dermatol. 2008;18:642–646. 35. Akdag M, Akkurt ZM, Gul A et al. The effects of oral isotretinoin (13-cis retinoic acid) on the inner ear: A prospective clinical study. Clin Invest Med. 2014;37:102–107. 36. Hosotani K, Kitagawa M. Improved simultaneous determination method of beta-carotene and retinol with saponification in human serum and rat liver. J Chromatogr B Analyt Technol Biomed Life Sci. 2003;791:305–313. 37. Takci Z, Simsek GG, Karabulut H et al. Effect of systemic isotretinoin therapy on mucociliary clearance and nasal surface mucosa in acne patients. J Drugs Dermatol. 2013;12:124–128. 38. Coates P, Vyakrnam S, Ravenscroft JC et al. Efficacy of oral isotretinoin in the control of skin and nasal colonization by antibiotic-resistant propionibacteria in patients with acne. Br J Dermatol. 2005;153:1126–1136. 39. Ozuguz P, Callioglu EE, Tulaci KG et al. Evaluation of nasal and oropharyngeal flora in patients with acne vulgaris according to treatment options. Int J Dermatol. 2014;53:1404–1408. 40. Başak PY, Cetin ES, Gürses I, Ozseven AG. The effects of systemic isotretinoin and antibiotic therapy on the microbial floras in patients with acne vulgaris. J Eur Acad Dermatol Venereol. 2013;27:332–336. 41. Allen BC, Rhee JS. Complications associated with isotretinoin use after rhinoplasty. Aesthetic Plast Surg. 2005;29:102–106. 42. Huoh KC, Chang KW. Lip abscess associated with isotretinoin treatment of acne vulgaris. JAMA Dermatol. 2013;149:960–961. 43. Beer K, Oakley H, Waibel J. Perioral abscess associated with isotretinoin. J Drugs Dermatol. 2009;8:1034–1036. 44. Webster WS, Johnston MC, Lammer EJ, Sulik KK. Isotretinoin embryopathy and the cranial neural crest: An in vivo and in vitro study. J Craniofac Genet Dev Biol. 1986;6:211–222. 45. Van Abel KM, Nelson ME, Collar RM, Lesperance MM. Development of canal cholesteatoma in a patient with prenatal isotretinoin exposure. Int J Pediatr Otorhinolaryngol. 2010;74:1082–1084. 46. Lee SM, Kim HM, Lee JS et al. A case of suspected isotretinoin-induced malformation in a baby of a mother who became pregnant one month after discontinuation of the drug. Yonsei Med J. 2009;50:445–447. 47. Sarici D, Akin MA, Kurtoglu S et al. Asymmetric crying face in a newborn with isotretinoin embryopathy. Pediatr Dermatol. 2013;30:289–290. 48. Rosende L, Verea-Hernando MM, de Andrés A et al. Hypoacusia in a patient treated by isotretinoin. Case Rep Med. 2011;2011:789143. Other Systemic Side Effects 49. Moerike S, Pantzar JT, De Sa D. Temporal bone pathology in fetuses exposed to isotretinoin. Pediatr Dev Pathol. 2002;5:405–409. 50. Millsop JW, Heller MM, Eliason MJ, Murase JE. Dermatological medication effects on male fertility. Dermatol Ther. 2013;26:337–346. 51. Kamm JJ. Toxicology, carcinogenicity, and teratogenicity of some orally administered retinoids. J Am Acad Dermatol. 1982;6:652–659. 52. Stinson SF, Reznik-Schuller H, Reznik G, Donahoe R. Atrophy induced in the tubules of the testes of Syrian hamsters by two retinoids. Toxicology. 1980;17:343–353. 53. Gencoglan G, Tosun M. Effects of isotretinoin on spermatogenesis of rats. Cutan Ocul Toxicol. 2011;30:55–60. 54. Sadek IA, Abdul-Mohsen MH. Long-term administration of vitamin A and the process of spermatogenesis. East Mediterr Health J. 1999;5:123–129. 55. Kuhlwein A, Schutte B. Light microscopic studies of spermatogenesis in rats following the admisitration of high doses of 13-cis-retinoic acid. Z Hautkr. 1985;60:245–248. 56. Torok L, Kadar L, Kasa M. Spermatological investigations in patients treated with etretinate and isotretinoin. Andrologia. 1987;19:629–633. 57. Vogt HJ, Ewers R. 13-cis-Retinsaure und spermatogenese. Hautarzt. 1985;36:281–286. 58. Çinar L, Kartal D, Ergin C et al. The effect of systemic isotretinoin on male fertility. Cutan Ocul Toxicol. 2016;35:296–299. 59. Hoting VE, Schütte B, Schirren C. [Isotretinoin treatment of acne conglobata. Andrologic follow-up]. Fortschr Med. 1992;110:427–430. 60. Aksoy H, Cinar L, Acmaz G et al. The effect of isotretinoin on ovarian reserve based on hormonal parameters, ovarian volume, and antral follicle count in women with acne. Gynecol Obstet Invest. 2015;79:78–82. 61. Cozzolino M, Domingo J, Soares SR. Ovarian stimulation under the effect of isotretinoin. Gynecol Endocrinol. 2018;34:107–109. 62. Öztürk S, Öztürk T, Ucak H et al. Evaluation of ovarian reserve and function in female patients treated with oral isotretinoin for severe acne: An exploratory study. Cutan Ocul Toxicol. 2015;34:21–24. 63. Cinar SL, Kartal D, Aksoy H et al. Long-term effect of systemic isotretinoin on female fertility. Cutan Ocul Toxicol. 2017;36:132–134. 64. Armaly Z, Haj S, Bowirrat A et al. Acute kidney injury following isotretinoin treatment. Am J Case Rep. 2013;14:554–556. 65. Kaya Aksoy G, Koyun M, Akkaya B et al. Eosinophilic tubulointerstitial nephritis on treatment with isotretinoin. Eur J Pediatr. 2016;175:2005–2006. 109 66. Mangodt TC, Joos R, Siozopoulou V et al. Perinuclear antineutrophil cytoplasmic antibody-positive vasculitis, oligoarthritis, tendinitis, and myositis associated with isotretinoin in a 15-year-old boy: Case report and review of literature. Pediatr Dermatol. 2018;35:173–177. 67. Yesilkaya B, Alli N, Artuz RF et al. The frequency of hematuria in acne vulgaris patients during isotretinoin treatment. Cutan Ocul Toxicol. 2017;36:74–76. 68. Sarifakioglu E, Yilmaz AE, Erpolat S. Terminal hematuria associated with oral isotretinoin treatment in a patient with acne vulgaris. Pediatr Dermatol. 2012;29:668–669. 69. Edwards S, Sonnex C. Urethritis associated with isotretinoin therapy. Acta Derm Venereol. 1997;77:330. 70. Alli N, Yorulmaz A. An unusual side effect of isotretinoin: Retinoid dermatitis affecting external urethral meatus. Cutan Ocul Toxicol. 2015;34:176–177. 71. Solak B, Erdem T, Solak Y. Isotretinoin use for acne vulgaris is associated with increased serum uric acid levels. J Dermatolog Treat. 2017;28:82–85. 72. Sengör B, Bayramgürler D, Müezzinoglu B et al. Effects of acitretin on spermatogenesis of rats. J Eur Acad Dermatol Venereol. 2006;20:689–692. 73. Parsch EM, Ruzicka T, Przybilla B, Schill WB. Andrological investigations in men treated with acitretin (Ro 10–1670). Andrologia. 1990;22:479–482. 74. Geiger JM, Walker M. Is there a reproductive safety risk in male patients treated with acitretin (neotigason/soriatane)? Dermatology. 2002;205:105–107. 75. Vanhooteghem O, Andre J, Pochet JM et al. Occurrence of gouty tophi following acitretin therapy. Clin Exp Dermatol. 1998;23:274–276. 76. Choi WJ, Ford ES, Curhan G Independent association of serum retinol and β-carotene levels with hyperuricemia: A national population study. Arthritis Care Res (Hoboken). 2012;64:389–396. 77. Cunha Filho RR, Almeida HL Jr, Breunig Jde A. Angiodema due to oral acitretin and isotretinoin. An Bras Dermatol. 2011;86:28–30. 78. Pasmatzi E, Monastirli A, Badavanis G, Tsambaos D. Angioedema without urticaria caused by oral acitretin. Acta Dermatovenereol Alp Pannonica Adriat. 2017;26:67–68. 79. Solak B, Metin N, Erdem MT. Angioedema-urticaria due to acitretin. Am J Ther. 2016;23:1116–1117. 80. Saray Y, Seçkin D. Angioedema and urticaria due to isotretinoin therapy. J Eur Acad Dermatol Venereol. 2006;20:118–120. 81. Üstüner P. Angioedema due to systemic isotretinoin therapy. Case Rep Dermatol Med. 2014;2014:595914. 82. Zonunsanga N. Isotretinoin induced rash, urticaria and angioedema: A case report. Our Dermatol Online. 2015;4:460–462. 19 Retinoids in Acne Ruta Ganceviciene and Christos C. Zouboulis Introduction Acne vulgaris is a chronic inflammatory disorder of the pilosebaceous follicles. Being one of the most commonly diagnosed skin diseases worldwide, acne remains a challenging dermatologic disease scientifically, extending into the pathogenetic pathways and therapeutic choices, as well as in daily clinical practice. For patients suffering from acne, this is a disease noticeable to everyone around. The chronic wavy manifestations of acne can lead to dramatic inflammation, rapid scarring, and permanent dyspigmentation if not treated. Acne has adverse emotional consequences and profound negative effects on psychosocial functioning that have been associated with increased rates of depression, anxiety, suicidal ideation, and suicidal attempts (1,2). The prevalence of acne peaks in adolescence, while the number of acne patients outside of the classic age range (>25 years of age) is increasing, especially in adult women (acne tarda, female acne) (3–6). Acne is not a temporary problem, but it shows persistence over years and has been reclassified according to the criteria of the World Health Organization as a chronic inflammatory disease, similar in scope with atopic dermatitis (7). In addition, acne can be an essential component of several systemic diseases or syndromes (8). Both the classic and modern features underlying acne pathogenesis include disturbed sebaceous gland (SG) activity with seborrhea and alterations of the quality of sebum lipids, dysregulation of the hormone microenvironment, and follicular hyperkeratinization. This is accompanied by the homing microbiome, the proliferation of Propionibacterium acnes (P. acnes) within the follicle, and the induction of inflammation primarily through activation of the adaptive immune system. Pro-inflammatory lipids and other inflammatory pathways, neuroendocrine regulatory mechanisms, diet, and exogenous factors all may contribute to this multifactorial process (9–11) (Figure 19.1). Acne is characterized by a polymorphic clinical appearance (Figure 19.2), varying degrees of severity, acute as well chronic forms, and numerous subtypes. Topical therapies are the mainstay of treatment for mild to moderate acne. All forms of severe and scarring acne require systemic treatment (12,13). Role of Retinoids in the Management of Acne Retinoids play a crucial role in the treatment of acne. The multifactorial pathogenesis of acne indicates that combination therapies are more likely to be of increased benefit than singletreatment regimens, with the exception of systemic isotretinoin (14,15). Retinoids act to normalize desquamation by reducing keratinocyte proliferation and promoting differentiation through their immunomodulatory effects. They are also able to block several important inflammatory pathways that activate acne: Tolllike receptors, leukocyte migration, and the AP-1 pathway (16). Topical retinoids have been shown to both reduce visible lesions and inhibit the development of microcomedones and additional new lesions. Those used in a topical form for the treatment of acne include tretinoin (all-trans-retinoic acid, ATRA), isotretinoin (13-cis retinoic acid, 13-cis RA), adapalene, and tazarotene, whereas retinaldehyde, retinol, and retinyl esters are used in cosmetic preparations. Tazarotene is not approved for acne treatment in Europe, and topical isotretinoin is not approved by the US Food and Drug Administration (FDA) (17). Tretinoin, isotretinoin, adapalene, and tazarotene are effective comedolytic agents, while adapalene seems less irritative than tretinoin (18). Consensus guidelines (13) for topical retinoid indications recommend early use to obtain best results in most patients with acne vulgaris. As monotherapy, topical retinoids have been mainly used in apparently noninflammatory comedonal acne. In inflammatory acne, the concomitant use of a topical retinoid with other topical or systemic antibiotics can enhance the beneficial effect (19,20). They also represent an essential part of maintenance therapy (13). In addition to all benefits of local retinoids, systemic isotretinoin decreases sebum production and inhibits P. acnes growth via changes in the follicular milieu. Isotretinoin has revolutionized the management of severe and/ or recalcitrant acne (Figure 19.3), being the only drug available that affects all major pathogenic factors. Since its approval by the FDA in 1982, it still is the only medication available that has been shown to induce long-term remissions of this challenging disease (21,22). Systemic Isotretinoin in the Management of Acne Isotretinoin (13-cis RA), is a natural first-generation monoaromatic retinoid, produced by chemically modifying the polar end group and the polyene side chain of vitamin A (Figure 19.4) (23). Its molecular formula is C2OH28O2. Isotretinoin is related to both ATRA and retinol. 111 112 Retinoids in Dermatology FIGURE 19.1 Current aspects of acne pathogenesis. Androgens, lipid ligands of the peroxisome proliferation-activating receptor (PPAR), regulatory neuropeptides with hormonal, and non-hormonal activity and environmental factors leading to hyperseborrhea, epithelial hyperproliferation in the sebaceous duct, and acroinfundibulum and to expression of pro-inflammatory chemokines/cytokines, which stimulate the development of comedones and inflammatory acne lesions. (Modified from Zouboulis CC et al. Exp Dermatol. 2005;14:143–152 [10].) FIGURE 19.2 The polymorphic clinical appearance of acne from mild comedonal acne to aggressive conglobate and fulminate diseases with deep-seated inflammation, nodules, and scarring. Pharmacodynamic and Pharmacokinetic Profile The liver naturally produces small quantities of 13-cis RA from vitamin A, which is a normal constituent of human serum (24). 13-cis RA is detectable after 30 min in blood, maximum concentrations are reached 2–4 h after oral intake, and steady-state concentrations are achieved in 1 week. 13-cis RA is an interconvertible isomer of ATRA with half-life elimination from 10 to 20 h and bioavailability of 25%. The major metabolites of isotretinoin in blood are 4-oxo- and 4-hydroxy-isotretinoin. The half-life of the metabolites ranges from 11 to 50 h (15,25). Isotretinoin crosses the placenta (26) and is more than 99% bound to plasma proteins, primarily albumin. Serum albumin has a critical function as a retinoidbinding protein in reducing the concentration of active retinoids and restricting the biological effects on sebaceous gland cells (22,27). 113 Retinoids in Acne (a) (b) (c) (d) (e) (f ) FIGURE 19.3 Treatment of severe acne with isotretinoin: (a,b) conglobate acne before and (c,d) after treatment with isotretinoin; (e,f) severe scarring acne before and after treatment with isotretinoin. FIGURE 19.4 Isotretinoin: chemical structure of 3,7-dimethyl-9-(2,6,6trimethyl-1-cyclohexenyl)-nona-2,4,6,8-tetraenoic acid. (See Zouboulis CC, Orfanos CE. Retinoids. In: Millikan LE, editor. Drug Therapy in Dermatology. New York/Basel: Marcel Dekker 2000; pp. 171–233 [16].) Pharmacokinetic studies have shown that absorption can be doubled by taking isotretinoin with or after a meal compared with the fasting state (28). Oral bioavailability can be increased, especially by fatty acids, which prevent the binding of retinoids with albumin and hence improve the clinical effect (29). Isotretinoin undergoes first-pass metabolism in the liver and subsequent enterohepatic recycling. Excretion of the drug is equal both in feces after conjugation and in urine after metabolization to water-soluble glucuronides (30). During long-term therapy it is not significantly displaced by its metabolites. Its epidermal concentrations are rather low, and no progressive accumulation in serum, epidermis, or the subcutis has been found (31). There is low liver or adipose tissue storage, in contrast to vitamin A. After discontinuation of therapy, increased levels of isotretinoin disappear from the serum and skin within 4 weeks (in a few cases within 3 months). Natural concentrations of 13-cis RA and its major metabolites are detected after that time (21). It seems likely that isotretinoin therapy interferes with the endogenous metabolism of vitamin A in the skin because vitamin A levels increased by about 50% and dehydrovitamin A levels decreased by around 80% in some patients (15). Mechanism of Action Among natural and synthetic retinoids administered as a therapy in humans, only oral isotretinoin is characterized by a unique 114 Retinoids in Dermatology sebostatic activity. It suppresses sebum production up to 90% by inhibiting sebaceous lipid synthesis (16,21,32–34). Isotretinoin has been found to be most effective in reducing SG size by decreasing proliferation of basal sebocytes and is able to prohibit the progression of sebocyte differentiation in vivo and in vitro (16,22,35). It is the only drug available that directly suppresses abnormal desquamation of the sebaceous follicle epithelium, decreases hyperkeratinization, and also diminishes the growth of P. acnes and inflammation (33). Unlike other retinoids that exert their effects by modulating gene expression after binding to and/or activating nuclear retinoid receptors (NRRs), 13-cis RA exhibits low binding affinity for both cellular retinoic acid-binding proteins(CRABPs) I and II as well as for NRRs, i.e. retinoic acid receptors (RARs), and retinoid X receptors (RXRs) (36). Isotretinoin has, therefore, been considered as a prodrug which exhibits its activity through isomerization to tretinoin (37) or metabolism to 4-oxo-isotretinoin or 4-hydroxy-isotretinoin (16). Moreover, 13-cis RA induces apoptosis in sebocytes by a RAR-independent mechanism, which contributes to its sebosuppressive effect and the resolution of acne (38). 13-cis RA has been suggested to act in a receptorindependent manner by influencing cellular signaling pathways through direct protein interactions as demonstrated with other retinoids or by enzyme inhibition (39,40). The superior sebostatic effect of isotretinoin has been also attributed to the delayed initiation of retinoid inactivation under incubation of sebocytes with isotretinoin, a fact that leads to high intracellular ATRA concentrations (16). The 4-oxo metabolites of retinoids have been shown to be functionally active in human keratinocytes and fibroblasts by their ability to induce changes in gene expression (41). 13-cis RA also induces the rapid and transient expression of transforming growth factor (TGF)-β1, TGF-β2, and/or TGF-β3, so that the TGFs will inhibit keratinocyte proliferation. TGF-β2 and TGF-β3 may act in the SG as mediators of the effect of 13-cis RA (42). A marked decrease in wax esters, a slight decrease in squalene and triglyceride fraction, and a relative increase in cholesterol level have been detected in skin surface lipids after treatment with isotretinoin (16). Free sterols and total ceramides have been found to be increased in comedonal lipids (43). Like all retinoids, 13-cis RA has also been shown to exert antiinflammatory activity through an inhibition of the migration of granulocytes into the skin (44). It might increase host defense mechanisms and modify monocyte chemotaxis (45). Recent studies indicate that the influence of 13-cis RA on sebocyte inflammatory signaling is likely to be induced by matrix metalloproteinases (MMPs) that have originated from keratinocytes and sebocytes (46). Oral isotretinoin has no direct antimicrobial action, but by modifying the microenvironment within the pilosebaceous duct makes, it is much less favorable to colonization with P. acnes. The result in suppression of proliferation and reduction of P. acnes is significantly greater than that seen with oral and topical antimicrobials (47,48). Isotretinoin has also been shown to competitively inhibit the 3α-hydroxysteroid activity of retinol dehydrogenase, leading to decreased androgen synthesis in vitro (40). Clinical Profile and Benefit After almost four decades of experience with oral isotretinoin, the published data and opinions of many experts, including the authors of the European Acne Guideline, support systemic isotretinoin as the agent of first choice for the treatment of severe papulopustular, moderate nodular, and severe nodular/conglobate acne (13,21,32,49–52). There are certain discrepancies, which create some practical, financial, and clinical difficulties for healthcare professionals, as the opinions of acne experts and the European Directive for systemic isotretinoin prescription may differ (32,53,54) (Table 19.1). There are a number of good reasons why systemic isotretinoin should be considered as the first-line treatment for severe acne “sooner rather than later.” Delaying this effective therapy in certain cases where there is already severe scarring acne in children 12 years old and even younger may be against best and evidencebased practice. Age should not necessarily be a contraindication for the use of isotretinoin (13,32,50,54,55). Isotretinoin up to 0.5 mg/kg/day has been used successfully in a number of neonates or juveniles with acne who have not responded to all appropriate topical or oral therapy (56), and should be considered for pediatric acne patients if there are sufficient clinical indications (57). TABLE 19.1 Comparison of the Recommendations of Pre- and Post-European Directives for Systemic Isotretinoin Prescribing Pre-European Directive (55) Indications for treatment Patient age Dosage of isotretinoin Monitoring of liver function Limitations for peeling and depilation Isotretinoin is recommended as first-line treatment for severe (nodular, congloblata) acne and acne which does not respond to at least 3 months of combined treatment with systemic antimicrobials and local treatment No age limitations 0.5 mg/kg/day – 1.0 mg/kg/day Liver enzymes and lipids should be checked before treatment and 1 month after the maximum dose has been reached Chemical and physical peeling should be avoided during treatment and for 6 months post-treatment; wax depilation should be avoided during and 6 weeks post-treatment Post-European Directive (53) Isotretinoin can only be recommended in severe (nodular, conglobate) acne that has/is not responding to combined antimicrobials and local treatment Not recommended in children <12 years of age Treatment starting at 0.5 mg/kg/day Liver enzymes and lipids should be checked before treatment, 1 month after starting, and every 3 months during treatment All types of peeling, wax depilation, and laser surgery to the face and trunk should be avoided during and up to 6 months post-treatment 115 Retinoids in Acne The reduction of inflammatory acne may prevent the occurrence of clinical and psychologic scarring, improve the quality of life, and in some cases reduce depression. Physical and psychologic severity of acne should play a role in the decision whether or not to prescribe isotretinoin (58–60). According to current recommendations of international experts, oral isotretinoin can be prescribed not only to patients with severe disease but also to patients with less severe disease who failed to respond to topical agents combined with oral antimicrobials, in women under hormonal antiandrogen treatment, and in patients with acne who relapse rapidly on discontinuation of treatment or where acne develops in individuals 25 years old or older (Table 19.2) (55,58,61). Identification of poor prognostic factors should also be taken into account for the early use of isotretinoin (Table 19.3) (54). Although comparative trials are missing, clinical experience confirms that the relapse rates after treatment with isotretinoin remain the lowest among all of the available therapies (13). Dosage, Administration, and Duration of Therapy Evidence on the best dosage, including cumulative dose, is rare and partly conflicting. The individual dose can be adjusted according to several factors: the patient’s body weight, the specific condition being treated, the severity of skin condition and the response to treatment, other treatment used at the same time, TABLE 19.2 Recommendations for the Use of Systemic Isotretinoin in Acne and the severity of side effects. The EMA recommendations to start at the dosage of 0.5 mg/kg daily, and the initial consideration that only a high daily dose (1 mg/kg/day) of isotretinoin can help to achieve optimal benefit has been changed to the more sparing approach (13,21). For severe papulopustular acne/moderate nodular acne, a dosage of systemic isotretinoin of 0.3–0.5 mg/kg can be recommended (13,51). Starting with a personalized low dose (0.1–0.2 mg/kg/day) of isotretinoin and progressively increasing to the highest tolerated dose or even intermittent treatment may reduce the risk and severity of acne flareups, mitigate side effects, and facilitate management (13,51,62–66). In contrast, for severe nodular/conglobate acne, especially for severe involvement of the chest and back, higher doses (≥0.5 mg/kg) of systemic isotretinoin are indicated (51,66,67). Attempts to determine the cumulative dose necessary to obtain an optimal treatment response and low relapse rate have not yet yielded sufficient evidence (13). Studies to derive a cumulative dose for maximum benefit and reduced relapse rate have confirmed that there is a definite effect of both dose and duration of therapy, but there is not any a priori pharmacokinetic reasons to support the concept of accumulation of drug or a cumulative dose effect (150 mg/kg) (68,69). As a rule, a 50% reduction of the pustules can be expected after 2−4 weeks of treatment. A 6-month treatment course is sufficient for the majority of patients. In cases of insufficient response, the treatment period can be prolonged, especially with a continuation of a 0.2–0.5 mg/kg/day dose, to optimize the therapeutic outcome. The duration of therapy should be adjusted to give at least 90% clearance of acne based upon initial clinical acne grade, followed by 4–8 weeks of consolidation (32). Factors contributing to the need for longer treatment include (69): • • • • A low-dose regimen (0.1–0.2 mg/kg/day) Presence of severe acne lesions Extrafacial involvement Prolonged history of the disease There are no reports of cumulative toxicity from using repeat courses. In addition, tachyphylaxis has not been reported (32). Sources: Cunliffe WJ et al. Dermatology. 1997;194:351–357; Layton AM. Am J Clin Dermatol. 2001;2:135–141. (55,58) Contraindications, Major Adverse Events, and Side Effects Absolute contraindications: TABLE 19.3 Prognostic Factors Influencing the Early Use of Isotretinoin Family history Early onset Hyperseborrhea Truncal acne Scarring Psychosocial difficulties Persistent or late onset acne Source: Layton AM et al. J Eur Acad Deratol Venereol. 2006;20:773–776. (54) • • • • Pregnancy or women contemplating becoming pregnant Noncompliance with contraception Breastfeeding Hypersensitivity to preservatives (parabens), dye systems or other components of the capsule • Vitamin A supplements • Blood donation during treatment and at least 1 month after cessation of treatment (FDA Alert for Healthcare Professionals) 116 Retinoids in Dermatology Relative contraindications: • • • • • • • • Leukopenia Moderate to severe hypercholesterolemia Hypertriglyceridemia Significant hepatic or renal dysfunction Hypothyroidism Young children Signs of depression and suicidal ideation Pseudotumor cerebri The major adverse event of isotretinoin is teratogenicity. There is an extremely high risk that severe birth defects will result if pregnancy occurs while taking isotretinoin in any amount, even for short periods of time. A Pregnancy Prevention Program (PPP) for each female patient of childbearing age is required, as proposed by the European Medicines Agency (EMA) and the US FDA (iPledge program) (51,52,70). Women of childbearing potential must use two separate, effective forms of contraception at least 1 month before, during, and 5 weeks post-therapy to make sure the drug is eliminated from the body. The treatment should ideally start on day 3 of the menstrual cycle. Enhanced effectiveness may be expected by the combination of isotretinoin with a contraceptive pill that contains a hormonal antiandrogen. These restrictions are not applicable to males. Despite the fact that all treated patients suffer from some side effects, most of them are predictable and manageable. The range and severity of the side effects depends on the disease being treated, the dose of isotretinoin, and personal issues (34). The side effect profile qualitatively resembles that of toxic effects of vitamin A or hypervitaminosis A syndrome (23). Isotretinoin can initially worsen acne. Usually, the flareup only lasts during the first 2 to 4 weeks (32). There are studies showing that acne patients tend to have comorbid emotional disorders, suicidal ideation as well as depression due to their altered appearance, and psychosocial complications in general, even without any treatment. Rates of depression among isotretinoin users ranges from 1% to 11%, with similar rates found in control groups receiving oral antibiotics. Regardless this data, every patient beginning an isotretinoin regimen should be assessed for a risk of depression, counseled, followed closely during the course of treatment (2,71). Patients treated with high doses of isotretinoin and with repeated cycles have a greater risk of inflammatory colitis but not of Crohn’s disease (72,73). Additionally, mucocutaneous, ophthalmologic, neuromuscular, and gastrointestinal side effects have been documented (74). The mucocutaneous side effects are the earliest and the most frequent ones that affect almost all treated patients (Table 19.4). Xerosis and cheilitis are dose-dependent and mainly reflect a decreased production of sebum, reduced stratum corneum thickness, and altered skin barrier function. These side effects are dose-dependent and become more tolerable by modification of the dose and/or additional symptomatic therapy. Photosensitivity is also frequently observed. Staphylococcus aureus colonization correlates with the isotretinoin-induced reduction in sebum production and may infrequently lead to overt cutaneous infections (32). TABLE 19.4 The Most Common Mucocutaneous Symptoms of Isotretinoin Adverse Effect Cheilitis Facial erythema Dermatitis Xerosis Vestibulitis Epistaxis Conjunctivitis/blepharitis Mucositis Epidermal atrophy Itching Desquamation Fragility of skin Hair loss Incidence (up to) 98% 65% 65% 50% 50% 35% 35% 40% 25% 25% 20% 20% 5% Source: Modified from Orfanos CE, Zouboulis CC. Dermatology. 1998;196:140–147. (15) Systemic side effects (acne fulminans, depression or mood changes, diarrhea or colitis, high-tone deafness, night blindness, Achilles tendonitis, urticaria, vasculitis) are uncommon and if one appears is usually well controlled by reducing the dose. Headaches may uncommonly be an early feature of benign intracranial hypertension, and arthralgia is seen most frequently in those patients participating in regular and heavy exercise (32). The most frequently observed systemic effect—alterations in the lipid plasma levels through increase in triglycerides and cholesterol—is dose-dependent and also related to the duration of treatment. This can be transient, possibly due to the hepatic adaptation of the organ to the drug impact on metabolism that is reflected by transient alterations in transaminase levels (75). Some authorities recommend monitoring lipids at 1 month following initiation of treatment, and every 3 months thereafter. The erythrocyte sedimentation rate (ESR) and blood urea nitrogen (BUN) levels may become above the normal range. Reducing the dosage by 50% may eliminate this abnormality (76). Drug Interactions Concurrent use of isotretinoin with alcohol and some medications may cause significant side effects: • Tetracyclines (77): Development of increased cranial hypertension (pseudotumor cerebri) • Alcohol: Reduced efficacy of isotretinoin (78) • Imidazole fungistatics (ketoconazole): Increased drug levels of isotretinoin • Acidic drugs with a high affinity for albumin (salicylic acid, indomethacin): In the blood, high therapeutic concentrations may displace isotretinoin from protein binding sites, resulting in an increased concentration of the drug (79) • Vitamin A supplements: Additive toxic effects 117 Retinoids in Acne Conclusions Despite some not fully elucidated mechanisms of action and possible accompanying side effects during the treatment period, the systemic retinoid isotretinoin is the only pathogenesis acting drug in acne, and for this reason it still remains the regimen of choice in severe forms of this challenging disease. INFORMATION RESOURCES Websites: • Roaccutane/Accutane (Isotretinoin) www.roche.com • Isotretinoin (marketed as Accutane®) Information: www.fda.gov/cder/drug/infopage/accutane/ Capsule REFERENCES 1. Ghodsi SZ, Orawa H, Zouboulis CC. Prevalence, severity and severity risk factors of acne in high school pupils: A ­ community-based study. J Invest Dermatol. 2009;129:2136–2141. 2. Lukaviciute L, Navickas P, Navickas A et al. Quality of life, anxiety prevalence, depression symptomatology and suicidal ideation among acne patients in Lithuania. J Eur Acad Dermatol Venereol. 2017;31:1900–1906. 3. Goulden V, Stables GI, Cunliffe WJ. Prevalence of facial acne in adults. J Am Acad Dermatol. 1999;41:577–580. 4. Schaefer I, Rustenbach SJ, Zimmer L, Augustin M. Prevalence of skin diseases in a cohort of 48,665 employees in Germany. Dermatology. 2008;217:169–172. 5. Zouboulis CC. Acne vulgaris – rolle der hormone. Hautarzt. 2010;61:107–114. 6. Zouboulis CC. Adulte akne (Acne tarda) der Frau: Eine Herausforderung für den Dermatologen. J Dtsch Dermatol Ges. 2018;16:1177–1179. 7. Gollnick HP, Finlay AY, Shear N. Global alliance to improve outcomes in acne. Can we define acne as a chronic disease? If so, how and when? Am J Clin Dermatol. 2008;9:279–284. 8. Chen W, Obermayer-Pietsch B, Hong J-B et al. Acneassociated syndromes: Models for better understanding of acne p­ athogenesis. J Eur Acad Dermatol Venereol. 2011;25:637–646. 9. Zouboulis CC. Acne and sebaceous gland function. Clin Dermatol. 2004;22:360–6. 10. Zouboulis CC, Eady A, Philpott M et al. What is the pathogenesis of acne? Exp Dermatol. 2005;14:143–152. 11. Kurokawa I, Danby FW, Ju Q et al. New developments in our understanding of acne pathogenesis and treatment. Exp Dermatol. 2009;18:821–832. 12. Gollnick HP, Zouboulis CC. Not all acne is acne vulgaris. Dtsch Arztebl Int. 2014;111:301–312. 13. Nast A, Dréno B, Bettoli V et al. European evidencebased (S3) guidelines for the treatment of acne. JEADV. 2016;30:1261–1268. 14. Gollnick H, Zouboulis CC, Akamatsu H et al. Pathogenesis and pathogenesis related treatment of acne. J Dermatol. 1991;18:489–499. 15. Orfanos CE, Zouboulis CC. Oral retinoids in the treatment of seborrhoea and acne. Dermatology. 1998;196:140–147. 16. Zouboulis CC, Orfanos CE. Retinoids. In: Millikan LE, editor. Drug Therapy in Dermatology. New York/Basel: Marcel Dekker 2000; pp. 171–233. 17. Thielitz A, Abdel-Naser MB, Fluhr JW et al. Topical retinoids in acne-an evidence-based overview. J Dtsch Dermatol Ges. 2008;6:1023–1031. 18. Thielitz A, Krautheim A, Gollnick H. Update in retinoid therapy of acne. Dermatol Ther. 2006;19:272–279. 19. Berson DS, Shalita AR. The treatment of acne: The role of combination therapies. J Am Acad Dermatol. 1995;32:S31–34. 20. Zouboulis CC, Fischer TC, Wohlrab J et al. Study of the efficacy, tolerability, and safety of 2 fixed-dose combination gels in the management of acne vulgaris. Cutis. 2009; 84:223–229. 21. Ganceviciene R., Zouboulis CC. Isotretinoin: State of the art treatment for acne vulgaris. J Dtsch Dermatol Ges. 2010;8:S47–S59. 22. Zouboulis CC. Isotretinoin revisited: Pluripotent effects on human sebaceous gland cells. J Invest Dermatol. 2006;126:2154–2156. 23. Kuenzli S, Saurat J-H. Retinoids. In: Bolognia JL, Jorizzo JL, Rapini RP, editors. Dermatology, vol. 2. St Louis: CV Mosby 2003; pp. 1991–1996. 24. Tang G, Russel RM. 13-cis-Retinoic acid is an endogenous compound in human serum. J Lipid Res. 1990;31:175–182. 25. Orfanos CE, Zouboulis CC, Almond-Roesler B, Geilen CC. Current use and future potential role of retinoids in dermatology. Drugs. 1997;53:358–388. 26. Benifla JL, Ville Y, Imbert MC et al. Fetal tissue dosages of retinoids. Experimental study concerning a case of isotretinoin (Roaccutan) administration and pregnancy. Fetal Diagn Ther. 1995;10:189–191. 27. Tsukada M, Schröder M, Seltmann H et al. High albumin levels restrict the kinetics of 13-cis retinoic acid uptake and intracellular isomerization to all-trans retinoic acid and inhibit its anti-proliferative effect on SZ95 sebocytes. J Invest Dermatol. 2002;119:182–185. 28. Colburn WA, Gibson DM, Wiens RE, Hanigan JJ. Food increases the bioavailability of isotretinoin. J Clin Pharmacol. 1983;23:534–539. 29. Avis I, Mathias A, Unsworth EJ et al. Analysis of small cell lung cancer cell growth inhibition by 13-cis-retinoic acid: Importance of bioavailability. Cell Growth Differ. 1995;6:485–492. 30. Roos TC, Jugert FK, Merk HF, Bickers DR. Retinoid metabolism in the skin. Pharm Rev. 1998;50:315–333. 31. Rollmann O, Vahlquist A. Oral isotretinoin (13-cis-retinoic acid) therapy in severe acne: Drug and vitamin A concentrations in serum and skin. J Invest Dermatol. 1986;86:384–389. 32. Layton A. The use of isotretinoin in acne. Dermatoendocrinol. 2009;1:162–169. 33. Zouboulis CC, Piquero-Martin J. Update and future of systemic acne treatment. Dermatology. 2003;206:37–53. 34. Ganceviciene R, Zouboulis CC. Isotretinoin: state of the art treatment for acne vulgaris. Expert Rev Dermatol. 2007;2:693–706. 35. Zouboulis CC, Korge B, Mischke D, Orfanos CE. Altered proliferation, synthetic activity, and differentiation of cultured human sebocytes in the absence of Vitamin A and their modulation by synthetic retinoids. J Invest Dermatol. 1993;101:628–633. 118 36. Siegenthaler G, Saurat J-H. Binding of isotretinoin to cellular retinoic acid-binding protein: A reappraisal. In: Marks R, Plewig G, editors. Acne and Related Disorders. London: Dunitz 1998; pp. 169–177. 37. Tsukada M, Schröder M, Roos TC et al. 13-cis Retinoic acid exerts its specific activity on human sebocytes through selective intracellular isomerization to all-trans retinoic acid and binding to retinoid acid receptors. J Invest Dermatol. 2000;115:321–327. 38. Nelson AM, Gilliland KL, Cong Z, Thiboutot DM. 13-cis Retinoic acid induces apoptosis and cell cycle arrest in human SEB-1 sebocytes. J Invest Dermatol. 2006;126:2178–2189. 39. Imam A, Hoyos B, Swenson C et al. Retinoids as ligands and coactivators of protein kinase C alpha. FASEB J. 2001;15:28–30. 40. Karlsson T, Vahlquist A, Kedishvili N, Törmä H. 13-cisretinoic acid competitively inhibits 3 alpha-hydroxysteroid oxidation by retinol dehydrogenase RoDH-4: A mechanism for its anti-androgenic effects in sebaceous glands? Biochem Biophys Res Commun. 2003;303:273–278. 41. Baron JM, Heise R, Blaner WS et al. Retinoic acid and its 4-oxo metabolites are functionally active in human skin cells in vitro. J Invest Dermatol. 2005;125:143–153. 42. Downie MMT, Sanders DA, Kealey T. Modelling the remission of individual acne lesions in vitro. Br J Dermatol. 2002;147:869–878. 43. Zouboulis CC, Krieter A, Gollnick H et al. Progressive differentiation of human sebocytes in vitro is characterized by increased cell size and altered antigenic expression and is regulated by culture duration and retinoids. Exp Dermatol. 1994; 3:151–160. 44. Wozel G, Chang A, Zultak M et al. The effect of topical retinoids on the leukotriene-B4-induced migration of polymorphonuclear leukocytes into human skin. Arch Dermatol Res. 1991;283:158–161. 45. Seguin-Devaux C, Hanriot D, Dailloux M et al. Retinoic acid amplifies the host response to LPS through increased T lymphocyte numbers and LPS binding protein expression. Mol Cell Endocrinol. 2005;241:67–76. 46. Papakonstantinou E, Aletras AJ, Glass E et al. Matrix metalloproteinases of epithelial origin in facial sebum of patients with acne and their regulation by isotretinoin. J Invest Dermatol. 2005;125:673–678. 47. Coates P, Adams CA, Cunliffe WJ. Does oral isotretinoin prevent Propionibacterium acnes resistance? Dermatology. 1997;195:4–9. 48. King K, Jones DH, Daltry DC, Cunliffe WJ. A double-blind study of the effects of 13-cis-retinoic acid on acne, sebum excretion rate and microbial population. Br J Dermatol. 1982;107:583–590. 49. Layton AM, Cunliffe WJ. Guidelines for optimal use of isotretinoin in acne. J Am Acad Dermatol. 1992;27:S2–7. 50. Gollnick H, Cunliffe WJ, Berson D et al. Management of acne: A report from a Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2003;49:S1–37. 51. Zouboulis CC, Betolli V. Management of severe acne. Br J Dermatol. 2015;172:S27–S36. 52. Massa AF, Burmeister L, Bass D, Zouboulis CC. Acne fulminans: Treatment experience from 26 patients. Dermatology. 2017;233:136–140. Retinoids in Dermatology 53. EMEA – Committee for Proprietary Medicinal Products (CPMP). European Directive for Systemic Isotretinoin Prescription. London: European Medicines Agency, 2003. 54. Layton AM, Dreno B, Gollnick HPM, Zouboulis CC. A review of the European Directive for prescribing systemic isotretinoin for acne vulgaris. J Eur Acad Deratol Venereol. 2006;20:773–776. 55. Cunliffe WJ, van de Kerkhof PCM, Caputo R et al. Roaccutane treatment guidelines: Results of an international survey. Dermatology. 1997;194:351–357. 56. Horne HL, Carmichael AJ. Juvenile nodulocystic acne responding to systemic isotretinoin. Br J Dermatol. 1997;136:796–797. 57. Clark SM, Cunliffe WJ. The use of isotretinoin in the treatment of acne in children. Br J Dermatol. 1995;133:39. 58. Layton AM. Optimal management of acne to prevent scarring and psychological sequelae. Am J Clin Dermatol. 2001;2:135–141. 59. Rubinow DR, Peck GL, Squillace KM, Gantt GG. Reduced anxiety and depression in cystic acne patients after successful treatment with oral isotretinoin. J Am Acad Dermatol. 1987;17:25–32. 60. Kellet SC, Gawkrodger DJ. The psychological and emotional impact of acne and the effect of treatment with isotretinoin. Br J Dermatol. 1999;140:273–282. 61. Laytom AL. Prescribing oral isotretinoin - The European approach. In: Zouboulis CC, Katsambas AD, Kligman AM, editors. Pathogenesis and Treatment of Acne and Rosacea. Berlin: Springer, 2014, pp. 463–467. 62. Borghi A, Mantovani L, Minghetti S et al. Acute acne flare following isotretinoin administration: potential protective role of low starting dose. Dermatology. 2009;218:178–180. 63. Lee JW, Yoo KH, Park KY et al. Effectiveness of conventional, low dose and intermittent oral isotretinoin in the treatment of acne: a randomized, controlled comparative study. Br J Dermatol. 2011;164:1369–1375. 64. Rademaker M. Isotretinoin: dose, duration and relapse. What does 30 years of usage tell us? Australas J Dermatol. 2013;54:157–162. 65. Borghi A, Mantovani L, Minghetti S et al. Low-cumulative dose isotretinoin treatment in mild-to-moderate acne: Eefficacy in achieving stable remission. J Eur Acad Dermatol Venereol. 2011;25:1094–1098. 66. Zouboulis CC. The truth behind this undeniable efficacy— recurrence rates and relapse risk factors of acne treatment with oral isotretinoin. Dermatology. 2006;212:99–100. 67. Layton AM, Stainforth JM, Cunliffe WJ. Ten years’ experience of oral isotretinoin for the treatment of acne vulgaris. J Dermatolog Treat. 1994;4:S2–5. 68. Harms M, Masooye I, Radeff B. The relapses of cystic acne after isotretinoin treatment are age-related: A long-term follow up study. Dermatologica. 1986;172:148–153. 69. Stainforth JM, Layton AM, Taylor JP, Cunliffe WJ. Isotretinoin for the treatment of acne vulgaris: Which factors may predict the need for more than one course? Br J Dermatol. 1993;129:297–301. 70. Maloney ME, Stone SP. Isotretinoin and iPledge: A view of results. J Am Acad Dermatol. 2011;65:418–419. 71. Marqueling AL, Zane LT. Depression and suicidal behavior in acne patients treated with isotretinoin: a systematic review. Semin Cutan Med Surg. 2007;26:210–220. Retinoids in Acne 72. Bernstein CN, Nugent Z, Longobardi T, Blanchard JF. Isotretinoin is not associated with inflammatory bowel disease: A population based case-control study. Am J Gastroenterol. 2009;104:2774–2778. 73. Crockett SD, Porter CQ, Martin CF et al. Isotretinoin use and the risk of inflammatory bowel disease: a case-control study. Am J Gastroenterol. 2010;105:1986–93. 74. Ellis CN, Krach KJ. Uses and complications of isotretinoin therapy. J Am Acad Dermatol. 2001;45:150–157. 75. De Marchi MA, Maranhao RC, Brandizzi LI, Souza DR. Effects of isotretinoin on the metabolism of triglyceride-rich lipoproteins and on the lipid profile in patients with acne. Arch Dermatol Res. 2006;297:403–408. 119 76. Fex GA, Aronsson A, Andersson A, Larsson K, Nilsson-Ehle P. In vivo effects of 13-cis retinoic acid treatment on the concentration of proteins and lipids in serum. Eur J Clin Chem Clin Biochem. 1996;34:3–7. 77. Lee AG. Pseudotumor cerebri after treatment with tetracycline and isotretinoin for acne. Cutis. 1995;55:165–168. 78. Soria C, Allegue F, Galiana J, Ledo A. Decreased isotretinoin efficacy during acute alcohol intake. Dermatologica. 1991;182:203. 79. Berbis P. Retinoid drug; interactions. Ann Dermatol Venereol. 1991;118:271–272. 20 Retinoids in Hidradenitis Suppurativa/Acne Inversa Uwe Wollina, Piotr Brzezinski, and André Koch Introduction Treatment in General Hidradenitis suppurativa (HS) (also known as acne inversa [AI]) is one of the most severe, debilitating inflammatory dermatoses, with a prevalence of 0.05% to 4.1%. HS is characterized by painful nodules, abscesses, draining sinuses, and hypertrophic scars, localized in the areas with numerous apocrine glands (axillae, submammary folds, groin, perigenital, or perineal) (1). The diagnosis is made clinically (Figures 20.1 and 20.2; Table 20.1) (2). HS is a misnomer, because eccrine glands are not primarily affected. The primary morphological event is the follicular occlusion triad (3). HS pathogenesis is not completely understood. HS is not primarily infectious. The major contributors to the ongoing inflammatory process are a disturbed innate and adaptive immunologic response for bacterial control, a dramatically changed microbiome of skin surface and subcutaneous lesions, activation of Th17 cells, impaired interleukin-22 signaling pathway, and formation of bacterial biofilms (4–7). A minority of patients suffer from syndromic HS (Table 20.2) (8). The disease has been classified according to its severity. Severity of HS is classified in three stages, according to the Hurley Scale, which relies on the subjective extent of the disease (9). Another scoring aid for HS/AI severity includes the Sartorius Scale and its modifications that are used in clinical trials (1,2; Table 20.3). Treatment of HS is dependent on the severity of the disease. Topical treatment is of limited value in mild HS. Systemic medical treatment includes antibiotics, such as clindamycin and rifampicin, and tumor-necrosis factor-alpha inhibitors. Of the latter, only adalimumab has been approved for Hurley grade II and III at a dosage of 40 mg weekly. Infliximab 5 mg/kg was effective, but etanercept 50 mg twice weekly failed (14). Despite efforts in medical treatment, radical surgery remains a cornerstone in the management of severe HS/AI with complete remissions (10,15–17). Trigger Factors and Comorbidities Classic trigger factors of HS are mechanical friction, hyperhidrosis, smoking, and obesity, but the importance of obesity and smoking seems to have decreased in recent years (10,11). Both are no conditio sine qua non. There are a number of important comorbidities that may affect treatment and outcome, with metabolic syndrome and inflammatory bowel diseases being most important (12,13). In an analysis of 117 patients with Hurley grade III anogenital HS, hypertension (14.5%), secondary lymphedema (14.5%), diabetes mellitus type 2 (9.4%), and psychiatric disorders (depression, borderline personality, suicide) (8.5%) were the most frequent (10). Retinoids in Hidradenitis Suppurativa Retinoids have been used for mild to moderate HS for decades (18). No randomized controlled trials have yet been performed. Retinoids influence cellular differentiation and proliferation of keratinocytes as well as normalize abnormal follicular desquamation and follicular occlusion; furthermore, retinoids demonstrate anti-inflammatory activity by downregulating highly expressed Toll-like receptors, such as Toll-like receptor type 2, cytokines, and nitric oxide, as well as modification of monocyte chemotaxis (19,20). In clinical trials, pain reduction has been observed during oral retinoid therapy (see section “Isotretinoin in Hidradenitis Suppurativa”). Etretinate in Hidradenitis Suppurativa There are only limited data available for etretinate (21). In a retrospective study, low-dose etretinate for 4−6 months for mild to moderate HS was investigated in 68 patients. A complete response was observed in 23.5% of patients, with 16.2% maintaining the improvement during follow-up (22). Etretinate is only of historic interest now, because acitretin has taken over its place in drug therapy. Isotretinoin in Hidradenitis Suppurativa The main mechanism of action in HS seems to be that isotretinoin may prevent an affected pilosebaceous unit from being occluded by ductal hyperkeratosis. Oral isotretinoin efficacy 121 122 Retinoids in Dermatology TABLE 20.2 Syndromic HS Syndrome Follicular occlusion tetrad Dowling-Degos disease Down syndrome FIGURE 20.1 Axillary HS with hypertrophic scars in a 32-year-old woman, considered to be Hurley stage IIA (absence of inflammation). KID syndrome PAPASH syndrome PASH syndrome SAPHO syndrome Remarks Genetics HS, acne, dissecting folliculitis, pilonidal sinus Asymmetrical reticular macular hyperpigmentation of the flexures, perioral pitted scars, comedo-like lesions, HS possible Small chin, slanted eyes, poor muscle tone, flat nasal bridge, a single crease of the palm, protruding tongue, and other internal or mental symptoms, probably with HS/AI Keratitis, ichthyosis, and deafness; HS may occur Pyogenic arthritis, pyoderma gangrenosum, acne, HS Pyoderma gangrenosum, acne, HS Synovitis, acne, pustulosis palmoplantaris, hyperostosis and osteitis; HS possible ? Autosomal-dominant loss of function of keratin-5 gene Trisomy 21 Mutations in connexin genes GJB2 and GJB6 PSTPIP1 mutation PSTPIP1 mutation ? TABLE 20.3 Severity Classification of HS According to the Dutch Refined Hurley Classification Grade Hurley I IA (mild) IB (moderate) IC (severe) Hurley II IIA (mild) IIB (moderate) IIC (severe) Hurley III Remarks Absence of sinus tracts ≤2 Body areas AND <5 abscesses/nodules >2 Body areas OR >5 abscesses/nodules, fixed lesions >2 Body areas OR >5 abscesses/nodules, migratory lesions (scarring folliculitis and frictional furuncle phenotype) <1% Body surface of the involved body site with interconnected inflammatory sinus tracts No inflammation ≤2 Body areas with inflammation >2 Body areas with inflammation ≥1% Body surface of the involved body site with interconnected inflammatory sinus tracts Source: Horváth B, Janse IC, Blok JL. Acta Derm Venereol. 2017; 97:412–413. FIGURE 20.2 HS with putrid secretions and fistulas in the groins in a 47-year-old woman (Hurley stage III). TABLE 20.1 Diagnostic Criteria of HS Typical lesions Typical localizations Typical course Deep-seated nodules and/or fibrosis Genitoanal, submammary, and axillary regions, often symmetrical Relapses and chronicity Note: All criteria must be fulfilled for a definite diagnosis. has been evaluated by interviews and examination of 358 consecutive HS patients. Eighty-seven patients had a previous treatment with isotretinoin. Of these, 16.1% of the patients noted an improvement, while 77% had no effect, and 6.9% experienced a worsening of the disease (23). Isotretinoin has a limited therapeutic effect in HS Hurley grade I and is no longer considered as a standard treatment (24). Acitretin in Hidradenitis Suppurativa In an open trial, 17 HS patients not responding to other classic medical treatments received acitretin with an average daily dose of Retinoids in Hidradenitis Suppurativa/Acne Inversa 0.6 mg/kg for up to 9 months. Patients were examined at baseline, after 1 month, and then every 3 months from baseline. Clinical improvement of at least 50% was achieved in 47% of patients. The dropout rate was high, with 47%, either due to side effects or nonresponse. The response was unstable after discontinuation of treatment. Relapse occurred in most patients after 2−8 months (25). A comparative trial investigated 30 patients treated with acitretin 0.5 mg/kg body weight for 12 weeks either given alone or combined with local excision of the sinus tracts with direct primary suturing. The recurrence rate was 20% with combined technique compared to 40% with acitretin alone (26). In another retrospective investigation, 12 patients with severe, recalcitrant HS were treated with acitretin for 9–12 months and followed for 4 years. All 12 patients achieved remission and reported a significant decrease in pain. Eight patients achieved a remission of at least 12 months (27). The cause of variable remission rates and durations remains unclear. Acitretin is a secondline treatment in Hurley grade I and II (24). Alitretinoin in Hidradenitis Suppurativa Alitretinoin has a short half-life of one month. This could be an advantage in women during childbearing years compared to acitretin with a 2-year half-life. Alitretinoin has been used in an open trial with 14 women who persistently failed traditional medical treatments for HS. They were treated with 10 mg alitretinoin per day for 24 weeks. At the end of this trial, 78.5% of patients achieved a significant improvement (28); however, alitretinoin has not been recommended in the European S1 guidelines for HS (24). Conclusions Oral retinoids have some value in milder cases of HS (Hurley I and II with inflammation) with a better response to acitretin and alitretinoin compared to etretinate or isotretinoin. The European guidelines for HS categorize acitretin/etretinate as second-line treatments and isotretinoin as third-line treatment with a level of evidence grade III and IV, respectively (24). Whether retinoids may reduce the relapse rate of surgery needs further investigation. Topical retinoids are useless. Conflicts of Interest U. Wollina and A. Koch have received honoraria for lectures from Abbvie and Novartis. REFERENCES 1. Saunte DML, Jemec GBE. Hidradenitis suppurativa: Advances in diagnosis and treatment. JAMA. 2017;318:2019–2032. 2. Zouboulis CC, Del Marmol V, Mrowietz U et al. Hidradenitis suppurativa/acne inversa: Criteria for diagnosis, severity assessment, classification and disease evaluation. Dermatology. 2015;231:184–190. 3. Sellheyer K, Krahl D. “Hidradenitis suppurativa” is acne inversa! An appeal to (finally) abandon a misnomer. Int J Dermatol. 2005;44:535–540. 123 4. Negus D, Ahn C, Huang W. An update on the pathogenesis of hidradenitis suppurativa: Implications for therapy. Expert Rev Clin Immunol. 2018;14:275–283. 5. Moran B, Sweeney CM, Hughes R et al. Hidradenitis suppurativa is characterized by dysregulation of the Th17:Treg cell axis, which is corrected by anti-TNF therapy. J Invest Dermatol. 2017;137:2389–2395. 6. Jones D, Banerjee A, Berger PZ et al. Inherent differences in keratinocyte function in hidradenitis suppurativa: Evidence for the role of IL-22 in disease pathogenesis. Immunol Invest. 2018;47:57–70. 7. Ring HC, Thorsen J, Saunte DM et al. The follicular skin microbiome in patients with hidradenitis suppurativa and healthy controls. JAMA Dermatol. 2017;153:897–905. 8. Gasparic J, Theut Riis P, Jemec GB. Recognizing syndromic hidradenitis suppurativa: A review of the literature. J Eur Acad Dermatol Venereol. 2017;31:1809–1816. 9. Hurley HJ. Axillary hyperhidrosis, apocrine bromhidrosis, hidradenitis suppurativa and familial benign pemphigus surgical approach. In: Roenigk RK, Roenigk HH, editors. Dermatologic Surgery. New York: Marcel Dekker; 1989. pp. 729–739. 10. Wollina U, Langner D, Heinig B, Nowak A. Comorbidities, treatment, and outcome in severe anogenital inverse acne (hidradenitis suppurativa): A 15-year single center report. Int J Dermatol. 2017;56:109–115. 11. Wollina U, Koch A, Heinig B et al. Acne inversa (Hidradenitis suppurativa): A review with a focus on pathogenesis and treatment. Indian Dermatol Online J. 2013;4:2–11. 12. Stefanadi EC, Dimitrakakis G, Antoniou CK et al. Metabolic syndrome and the skin: A more than superficial association. Reviewing the association between skin diseases and metabolic syndrome and a clinical decision algorithm for high risk patients. Diabetol Metab Syndr. 2018;10:9. 13. Kamal N, Cohen BL, Buche S et al. Features of patients with Crohn’s disease and hidradenitis suppurativa. Clin Gastroenterol Hepatol. 2016;14:71–79. 14. Ingram JR, Woo PN, Chua SL et al. Interventions for hidradenitis suppurativa. Cochrane Database Syst Rev. 2015;(10):CD010081. 15. Wollina U, Tilp M, Meseg A et al. Management of severe anogenital acne inversa (hidradenitis suppurativa). Dermatol Surg. 2012;38:110–117. 16. Kofler L, Schweinzer K, Heister M Surgical treatment of hidradenitis suppurativa: An analysis of postoperative outcome, cosmetic results and quality of life in 255 patients. J Eur Acad Dermatol Venereol. 2018;32:1570–1574. 17. Deckers IE, Dahi Y, van der Zee HH, Prens EP. Hidradenitis suppurativa treated with wide excision and second intention healing: a meaningful local cure rate after 253 procedures. J Eur Acad Dermatol Venereol. 2018;32:459–462. 18. Forbat E, Ali FR, Al-Niaimi F. Dermatological indications for the use of isotretinoin beyond acne. J Dermatolog Treat. 2018;29:698–705. 19. Liu PT, Krutzik SR, Kim J, Modlin RL. Cutting edge: Alltrans retinoic acid down-regulates TLR2 expression and function. J Immunol. 2005;174:2467–2470. 20. Bécherel PA, Mossalayi MD, LeGoff L et al. Mechanism of anti-inflammatory action of retinoids on keratinocytes. Lancet. 1994;344:1570–1571. 21. Chow ET, Mortimer PS. Successful treatment of hidradenitis suppurativa and retroauricular acne with etretinate. Br J Dermatol. 1992;126:415. 124 22. Boer J, van Gemert MJ. Long-term results of isotretinoin in the treatment of 68 patients with hidradenitis suppurativa. J Am Acad Dermatol. 1999;40:73–76. 23. Soria A, Canoui-Poitrine F, Wolkenstein P et al. Absence of efficacy of oral isotretinoin in hidradenitis suppurativa: A retrospective study based on patients’ outcome assessment. Dermatology. 2009;218:134–135. 24. Zouboulis CC, Desai N, Emtestam L et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J Eur Acad Dermatol Venereol. 2015;29:619–644. 25. Matusiak L, Bieniek A, Szepietowski JC. Acitretin treatment for hidradenitis suppurativa: A prospective series of 17 patients. Br J Dermatol. 2014;171:170–174. Retinoids in Dermatology 26. Puri N, Talwar A. A study on the management of hidradenitis suppurativa with retinoids and surgical excision. Indian J Dermatol. 2011;56:650–651. 27. Boer J, Nazary M. Long-term results of acitretin therapy for hidradenitis suppurativa. Is acne inversa also a misnomer? Br J Dermatol. 2011;164:170–175. 28. Verdolini R, Simonacci F, Menon S et al. Alitretinoin: A useful agent in the treatment of hidradenitis suppurativa, especially in women of child-bearing age. G Ital Dermatol Venereol. 2015;150:155–162. 29. Horváth B, Janse IC, Blok JL Hurley staging refined: A ­proposal by the Dutch Hidradenitis Suppurativa expert group. Acta Derm Venereol. 2017;97:412–413. 21 Retinoids in Rosacea Marius Rademaker and Harriet Cheng Introduction Rosacea is a chronic inflammatory skin disease which primarily affects the face and most often presents in adults 30 years and older (1). It is characterized by vascular changes, inflammation, and microbial activity (2). Retinoids have been used in the management of rosacea since the 1980s (3) with therapeutic benefits stemming from their anti-inflammatory and sebum-reducing actions. While there is limited evidence for topical retinoids (4,5), most benefit is seen with the systemic administration of long-term low-dose isotretinoin having an established role in the management of papulopustular rosacea. Systemic retinoids also play a role in management of rosacea subtypes that are traditionally more difficult to treat, including phymatous, ocular, granulomatous, and fulminant disease. Clinical Aspects of Rosacea Rosacea predominantly affects middle-aged and older adults, with women having a higher risk than men (1) and an overall prevalence of approximately 5% (6). Rosacea is more frequently diagnosed in those with lighter skin phototypes, although it is not known whether this is concealment by cutaneous melanin pigment or a reduced risk of rosacea in darker skin types (7,8). Other risk factors for rosacea include family history, past history of smoking, and alcohol consumption (1,9). The pathophysiology of rosacea includes vascular changes, activity of the innate immune system, photodamage, and microbial activity (2). Flushing is an early feature due to neurovascular hyperreactivity, possibly related to dysregulation of thermal mechanisms and trigger factors (10,11). Increased cutaneous blood flow results in accumulation of extracellular fluid, edema, lymphatic failure, and subsequent inflammation (12). Innate immunity is thought to have a central role, with inflammasomemediated cathelicidins leading to chronic inflammation (13) and angiogenesis mediated by interleukin-1 beta following exposure to ultraviolet light (14). Microorganisms augment chronic inflammation in rosacea through particularly heavy infestation with Demodex folliculorum (15). More recently, dietary factors with changes in the gut microbiome have been implicated (16). Rosacea flares can be triggered by extremes of temperatures, hot or spicy foods, and alcohol, which contribute to neurogenic inflammation via activation of receptors on primary sensory ­neurons and keratinocytes (17). The classification of rosacea was updated in 2017 (10). Fixed centrofacial erythema or phymatous changes are diagnostic. In addition, the presence of two of the following major features is also considered diagnostic: flushing, papules and pustules, telangiectasia, and various ocular changes. Secondary features include skin burning or stinging, edema, and dryness. The various clinical features of rosacea can be considered as a spectrum with overlapping features and severities (Table 21.1). Clinical examples of rosacea are shown in Figure 21.1. Treatment of Rosacea Treatment of rosacea begins with education and advice regarding general skin care measures (6). Because rosacea is characterized by a sensitive and irritable skin type, a gentle, soap-free cleanser and a moisturizer are recommended in addition to sun protection and avoidance of other triggers (18). Additional pharmacologic topical and systemic treatments are tailored to the specific rosacea phenotype (18). The use of retinoids in the treatment of rosacea stems from anti-inflammatory, anti-angiogenesis, and sebum suppressing effects. As rosacea is a chronic disease, there is a need to continue treatment for many years. Topical Retinoids for Rosacea Topical retinoids, including tretinoin, adapalene, and tazarotene creams and gels, may have a role in the management of papulopustular rosacea; however, use is limited by their irritant potential which may exacerbate erythema. In a small randomized, double blind trial, 0.025% tretinoin cream was comparable to low dose oral isotretinoin in reducing papules and pustules after 16 weeks of treatment (4). Adapalene 0.1% gel was superior to metronidazole gel in reducing inflammatory lesion count in a head-to-head trial (5). No difference was seen between the two groups in erythema and telangiectasia scores. Topical retinoids are included in some international rosacea management guidelines, primarily for the papulopustular subtype (19,20); however, high quality evidence is limited, and topical retinoids were not included in the 2016 Global Rosacea Consensus Panel recommendations that favor azelaic acid, metronidazole, and ivermectin (18). 125 126 Retinoids in Dermatology TABLE 21.1 Systemic Retinoids for Rosacea Clinical Features and Subtypes of Rosacea Fixed centrofacial erythema (diagnostic feature) Phymatous rosacea (diagnostic feature) Flushing Papules and pustules Skin sensitivity Ocular rosacea Granulomatous rosacea Extrafacial rosacea Morbihan disease Steroid-induced rosacea Rosacea fulminans and conglobata (a) (d) The use of isotretinoin (13-cis retinoic acid) is well established (21). There is also benefit in conditions other than acne; however, many studies lack statistical power or are of low quality (22). The action of isotretinoin in the treatment of rosacea includes atrophy of sebaceous glands, anti-angiogenesis, reduced sebum production, and anti-inflammatory effects. Histologically, there are reduced perivascular inflammation and decreased vascular ectasia (23,24). Isotretinoin has been used to treat rosacea since the 1980s (3,26). Initial dosing schedules (1 mg/kg/day) have been limited by toxicity, including increases in serum triglyceride and cholesterol, along with abnormal liver function tests (26). Highdose regimes have been superseded by lower dose schedules (10–20 mg daily) since the mid 1990s (4,27) that show low dose isotretinoin to be efficacious with improved tolerability (28). One study, using isotretinoin 10 mg daily for 9 weeks, reported less erythema, fewer telangiectasia, and reduction in papules and pustules (28). This has been confirmed in additional trials (29). In 2010, a large German randomized controlled study compared three isotretinoin dosages (0.1, 0.3, or 0.5 mg/kg/day) with doxycycline or placebo over 12 weeks (30). Isotretinoin 0.3 mg/kg/day was found to be the most effective dose, s­ uperior to placebo and non-inferior to doxycycline, but the study was of short duration. Less dermatitis was seen with lower doses of isotretinoin compared with higher-dose groups. A 2016 French study confirmed the value of lower dose isotretinoin (0.24 mg/kg/day) in difficult-to-treat papulopustular rosacea (31). In this double-blind randomized placebo-controlled study of 4 months duration, over half of the isotretinoin patients Characteristic pattern, particularly convex surfaces, telangiectasia may be present May periodically intensify More difficult to detect in darker skin phototypes Hypertrophy of skin and sebaceous glands Inflammatory nodules or plaques Nose as predominant site Men > women Early feature Related to triggers including heat, sunlight, spicy and hot food or drink, alcohol Usually coexist with midface erythema Inflammatory lesions Intolerance to cosmetics, burning, stinging, dryness, and edema Dryness, burning, stinging Gritty or foreign body sensation Photosensitivity Telangiectasia of lid margin and conjunctiva, tear dysfunction, crusting at base of eyelashes Yellow, brown, or red papules Midface distribution Photo-exposed skin Men > women Persistent edema Eyelids as predominant site Precipitated by topical or systemic corticosteroid use Large inflammatory nodules, plaques, and multiple pustules (b) (e) (c) (f ) FIGURE 21.1 Clinical manifestations of rosacea. (a) Facial erythema and scattered papules in early rosacea. (b) Papulopustular rosacea. (c) Papules and pustules on the nose with early rhinophyma. (d) Periorbital edema in Morbihan disease. (e) Periorbital and conjunctival erythema in ocular rosacea. (f) Papules, pustules and erythema in steroid-induced rosacea. ([a–e] Images courtesy of DermNet NZ; [f] Image courtesy of DermNet NZ and Waikato District Health Board.) 127 Retinoids in Rosacea TABLE 21.2 Recommendations for Systemic Retinoid Use in Subtypes of Rosacea Stage or Subtype Use of Isotretinoin Pre or early rosacea Generally not indicated. Use topical therapies, including topical retinoids, but low dose isotretinoin (e.g. 5–10 mg × 2–3/week) can be considered if no response. 10 mg/day (or less) likely to slowly reduce erythema and telangiectasia due to anti-VEGF and anti-inflammatory effects. Consider as second line but continue for several years. Can be used in combination with laser treatment. 10 mg/day, reducing to 10 mg 2–3/week, or 5 mg/day, as long-term maintenance treatment (years). Consider first line, continue for several years. 10–20 mg/day may reduce progression. Reduce dose (e.g., 10 mg × 2–3/week or 5 mg/day), but do not stop, prior to any physical treatments other than deep dermabrasion or full ablative laser. Consider first line. Isotretinoin 10 mg/day. Consider second line after low-dose tetracyclines. Isotretinoin 10–20 mg/day or dapsone. Consider first line. 10–20 mg/day. Consider first line in papulopustular disease. 20–30 mg/day, ± intralesional/systemic steroids. Consider first line. 10 mg/day. Consider first or second line before/after low-dose tetracycline. Isotretinoin 10 mg/day ± systemic corticosteroids. Consider first line. Erythematous telangiectatic rosacea Papulopustular rosacea Phymatous rosacea Ocular rosacea Granulomatous rosacea Extrafacial rosacea Morbihan disease Steroid-induced rosacea Rosacea fulminans/ conglobata achieved the primary endpoint of 90% reduction in lesions, with the numbers needed to treat (NNT) calculated to be 2.1. This was associated with a >50% improvement in quality of life scores (Skindex). In a continuation study, 67% of patients remained completely clear with the remainder significantly improved; however, just over half of the patients relapsed weeks after stopping isotretinoin, with a median course of 15 weeks. Following the observation of recurrences in these studies, a microdose of isotretinoin (20–70 mg weekly) has been proposed for treating recalcitrant rosacea (32). This has been effective in reducing relapse and improving skin-associated quality of life. More recently, an even lower dose of isotretinoin (equivalent to 5 mg/day) used for long courses has been shown to be effective for papulopustular rosacea (33). These very low dose regimes improve the tolerability of isotretinoin; however, controlled, prospective studies are required to confirm safety and efficacy, as long-term treatment may be required for many years. Isotretinoin may be continued with the use of intense pulsed light (IPL) or pulsed dye laser (34). There is minimal evidence to demonstrate the efficacy or superiority of isotretinoin over antimicrobials for treating other rosacea subtypes, including granulomatous (35,36), phymatous (37,38), and extrafacial rosacea (39), Morbihan disease (40,41), and rosacea fulminans (42). Recommendations for the use of isotretinoin in rosacea are summarized in Table 21.2. There are no data on the use of other systemic retinoids, including etretinate, acitretin, alitretinoin, or bexarotene, in the management of rosacea. Conclusions Given the increasing concern over the widespread use of antimicrobials and the need to limit their duration in chronic skin diseases, isotretinoin is likely to play an increasing role in the management of rosacea in the future (25). Level of Evidence (43): 1–5 5 4 1b 4 4 5 4 4 3a 3a REFERENCES 1. Spoendlin J, Voegel JJ, Jick SS, Meier CR. A study on the epidemiology of rosacea in the U.K. Br J Dermatol. 2012;167: 598–605. 2. Del Rosso JQ, Thiboutot D, Gallo R et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 3: A status report on systemic therapies. Cutis. 2014;93:18–28. 3. Nikolowski J, Plewig G. Rosacea. Oral therapy with 13-cis retinoic acid. Hautarzt. 1980;31:660–661. 4. Ertl GA, Levine N, Kligman AM. A comparison of the efficacy of topical tretinoin and low-dose oral isotretinoin in rosacea. Arch Dermatol. 1994;130:319–324. 5. Altinyazar HC, Koca R, Tekin NS, Esturk E. Adapalene vs. metronidazole gel for the treatment of rosacea. Int J Dermatol. 2005;44:252–255. 6. Elewski BE, Draelos Z, Dreno B et al. Rosacea—Global diversity and optimized outcome: Proposed international consensus from the Rosacea International Expert Group. J Eur Acad Dermatol Venereol. 2011;25:188–200. 7. Al-Dabagh A, Davis SA, McMichael AJ, Feldman SR. Rosacea in skin of color: Not a rare diagnosis. Dermatol Online J. 2014;20. 8. Tan J, Steinhoff M, Berg M et al. Shortcomings in rosacea diagnosis and classification. Br J Dermatol. 2017;176:197–199. 9. Abram K, Silm H, Maaroos HI, Oona M. Risk factors associated with rosacea. J Eur Acad Dermatol Venereol. 2010;24:565–571. 10. Gallo R, Granstein R, Kang S et al. Standard classification of rosacea: The 2017 Update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2017;78:148–155. 11. Crawford GH, Pelle MT, James WD. Rosacea: I. Etiology, pathogenesis, and subtype classification. J Am Acad Dermatol. 2004;51:327–341; quiz 42–44. 12. Wilkin JK. Rosacea: Pathophysiology and treatment. Arch Dermatol. 1994;130:359–362. 13. Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci. 2009;55:77–81. 128 14. Salzer S, Kresse S, Hirai Y et al. Cathelicidin peptide LL-37 increases UVB-triggered inflammasome activation: Possible implications for rosacea. J Dermatol Sci. 2014;76:173–179. 15. Zhao YE, Wu LP, Peng Y, Cheng H. Retrospective analysis of the association between Demodex infestation and rosacea. Arch Dermatol. 2010;146:896–902. 16. Maarouf M, Platto JF, Shi VY. The role of nutrition in inflammatory pilosebaceous disorders: Implication of the skin-gut axis. Australas J Dermatol. 2019;60(2):e90–e98. 17. Aubdool AA, Brain SD. Neurovascular aspects of skin neurogenic inflammation. J Invest Dermatol Symp Proc. 2011;15:33–39. 18. Schaller M, Almeida LMC, Bewley A et al. Rosacea treatment update: Recommendations from the global ROSacea COnsensus (ROSCO) panel. Br J Dermatol. 2017;176:465–471. 19. Anzengruber F, Czernielewski J, Conrad C et al. Swiss S1 guideline for the treatment of rosacea. J Eur Acad Dermatol Venereol. 2017;31:1775–1791. 20. Reinholz M, Tietze JK, Kilian K et al. Rosacea – S1 guideline. J Dtsch Dermatol Ges. 2013;11:768–780. 21. Jones H, Blanc D, Cunliffe WJ. 13-cis retinoic acid and acne. Lancet. 1980;2:1048–1049. 22. Forbat E, Ali FR, Al-Niaimi F. Dermatological indications for the use of isotretinoin beyond acne. J Dermatolog Treat. 2018;29:698–705. 23. Park H, Del Rosso JQ. Use of oral isotretinoin in the management of rosacea. J Clin Aesthet Dermatol. 2011;4:54. 24. Plewig G, Nikolowski J, Wolff HH. Action of isotretinoin in acne rosacea and gram-negative folliculitis. J Am Acad Dermatol. 1982;6:766–785. 25. Mobacken H, Berg M, Angesjo E et al. Time to limit the use of antibiotics in rosacea! Lakartidningen. 2018;115. 26. Marsden JR, Shuster S, Neugebauer M. Response of rosacea to isotretinoin. Clin Exp Dermatol. 1984;9:484–488. 27. Hoting E, Paul E, Plewig G. Treatment of rosacea with isotretinoin. Int J Dermatol. 1986;25:660–663. 28. Erdogan FG, Yurtsever P, Aksoy D, Eskioglu F. Efficacy of low-dose isotretinoin in patients with treatment-resistant rosacea. Arch Dermatol. 1998;134:884–885. 29. Uslu M, Savk E, Karaman G, Sendur N. Rosacea treatment with intermediate-dose isotretinoin: Follow-up with erythema and sebum measurements. Acta Derm Venereol. 2012;92:73–77. 30. Gollnick H, Blume-Peytavi U, Szabo EL et al. Systemic isotretinoin in the treatment of rosacea—doxycycline- and placebo-controlled, randomized clinical study. J Dtsch Dermatol Ges. 2010;8:505–515. Retinoids in Dermatology 31. Sbidian E, Vicaut E, Chidiack H et al. A randomized-controlled trial of oral low-dose isotretinoin for difficult-totreat papulopustular rosacea. J Invest Dermatol. 2016;136: 1124–1129. 32. Hofer T. Continuous “microdose” isotretinoin in adult recalcitrant rosacea. Clin Exp Dermatol. 2004;29:204–205. 33. Rademaker M. Very low-dose isotretinoin in mild to moderate papulopustular rosacea: A retrospective review of 52 patients. Australas J Dermatol. 2018;59:26–30. 34. Spring LK, Krakowski AC, Alam M et al. Isotretinoin and timing of procedural interventions: A systematic review with consensus recommendations. JAMA Dermatol. 2017;153:802–809. 35. Rallis E, Korfitis C. Isotretinoin for the treatment of granulomatous rosacea: Case report and review of the literature. J Cutan Med Surg. 2012;16:438–441. 36. Smith KW. Perioral dermatitis with histopathologic features of granulomatous rosacea: Successful treatment with isotretinoin. Cutis. 1990;46:413. 37. Wee JS, Tan KB. Phymatous rosacea presenting with leonine facies and clinical response to isotretinoin. Australas J Dermatol. 2017;58:72–73. 38. Pohl L, Karsai S, Raulin C. [Rhinophyma: Successful treatment with low-dose oral isotretinoin]. Hautarzt. 2018;69:853–856. 39. Bostanci O, Borelli C, Schaller M. Treatment of extrafacial rosacea with low-dose isotretinoin. Acta Derm Venereol. 2010;90:409–410. 40. Mazzatenta C, Giorgino G, Rubegni P et al. Solid persistent facial oedema (Morbihan’s disease) following rosacea, successfully treated with isotretinoin and ketotifen. Br J Dermatol. 1997;137:1020–1021. 41. Smith LA, Cohen DE. Successful long-term use of oral isotretinoin for the management of Morbihan disease: A case series report and review of the literature. Arch Dermatol. 2012;148:1395–1398. 42. Walsh RK, Endicott AA, Shinkai K. Diagnosis and treatment of rosacea fulminans: A comprehensive review. Am J Clin Dermatol. 2018;19:79–86. 43. Oxford Centre for Evidence-based Medicine—Levels of Evidence (March 2009). Available from: https://www.cebm. net/2009/06/oxford-centre-evidence-based-medicine-levelsevidence-march-2009/. 22 Retinoids in Hair Disorders Brent J. Doolan and Rodney Sinclair Introduction Early observations have shown that vitamin A deficiency can induce epidermal hyperkeratosis, squamous metaplasia of mucous membranes, various keratinization disorders, and certain precancerous conditions (1). Conversely, vitamin A has been shown to induce robust immune responses and aids in the differentiation and growth of skin, hair, and other tissues (2). These findings suggest that vitamin A is implicated in both the pathogenesis and treatment of various hair disorders. Retinoids are derivatives of vitamin A, or all-trans retinol, or synthetic compounds that share structural and/or functional similarities with the vitamin. Retinoids function by binding to nuclear receptors, which in turn interact with other transcription factors to coordinate gene expression. The regulation of the retinoid signaling pathway is complex, and retinoids can have numerous effects on multiple tissues in a dose-dependent manner. For decades, dermatologists have used vitamin A and related compounds (retinoids) to treat a wide range of cutaneous disorders, including psoriasis, acne, and cutaneous T-cell lymphoma. More recently, evidence has emerged for the use of retinoids both as a causative agent in some hair disorders as well as a therapeutic option for treatment of specific hair disorders. Retinoids and the Hair Cycle Hair growth involves complex interactions of genes, signaling factors, cell-to-cell interactions, and complex proteins and hormones. Retinoids have a direct impact on these interactions by altering the dynamic hair growth cycle. The cycle of hair growth comprises four main stages, including anagen (growth and differentiation), catagen (regression and apoptosis), telogen (inactivity), and exogen (the shedding of old hair follicles) (Figure 22.1) (3). This cycle results in the replacement of every hair on the scalp every 3–5 years, with individual follicles undergoing 10–30 such cycles in a lifetime (4). On average, a normal scalp has 100,000 hairs, with approximately 86% being in anagen, 1% in catagen, and 13% in telogen (5). The variation in hair cycle length is attributable to the length of the anagen phase, which is unique to the individual (6). As hair is produced solely in anagen, this phase also determines the physical length of the hair. The regeneration of hair is dependent on the recycling of the anagen terminal follicle. The primary follicle stem cells are at the site of contact of the external root sheath and the erector pili muscle, with a secondary site of regeneration located at the anagen bulb (6). Hair follicle induction and growth is also dependent on interactions between the external environment, the epidermis, and underlying mesenchyme. Several pathways, such as the Wnt, sonic hedgehog, bone morphogenetic protein, and fibroblast growth factor intracellular pathways are essential in these reciprocal signaling events necessary for hair follicle morphogenesis and differentiation (7). Studies with transgenic mice support a role for retinoic acid in the hair follicle (8). It was found that blocking of the retinoic acid−signaling pathways resulted in a delay in anagen initiation while increasing retinol and all-trans-retinoic acid (tretinoin) (8). Exogenous tretinoin was also shown to induce catagen in cultured hair follicles (9). In addition, exogenous tretinoin with bone morphogenetic protein directed the differentiation of embryonic and induced pluripotent stem cells into keratinocytes that when grafted into nude mice produced normal epidermis, hair follicles, and sebaceous glands (10). There was upregulation of signaling proteins with the addition of retinoic acid, peaking during mid-anagen through to early catagen (8). The results suggest that retinoic acid can alter differentiation and the hair growth cycle to regulate both the telogen-to-anagen and anagen-to-catagen transitions and assist in lipid metabolism for maintenance of epidermal barrier function. It has also been shown that retinoic acid plays an important role in hair follicle formation and patterning through the homeobox gene proteins Hox C8 and Hox C6 (11). Retinoic acid appears to up- and downregulate the homeobox genes, which consequently influences hair follicle generation, initiation, differentiation, and even inhibition (11). Retinoic acid receptor (RAR) and retinoid X receptor (RXR) genes have been identified in almost every portion of the hair follicle. The RARs and RXRs differ depending on the specific portion of the hair follicle (12). This gene arrangement also provides validation of the complex interaction that exists between protein synthesis, cell turnover, and the activation of cellular retinoic acid-binding protein from retinoic acid within the nucleus (12). The localized components that are involved in the signaling to the hair follicle by retinoic acid have been hypothesized in many reports (13–15). There is still much that is unknown regarding the exact mechanism of retinoic acid’s function within the hair follicle, 129 130 Retinoids in Dermatology FIGURE 22.1 Human hair growth cycle dynamics. and future studies are required to determine the mechanism of retinoic acid differentiation within the hair follicle. Retinoid-Induced Hair Disorders Acute Telogen Effluvium Acute telogen effluvium (ATE) is a self-limiting, non-scarring, diffuse loss of club (telogen) hair in disease states of the follicle that usually occurs 3–4 months after a triggering event (Figure 22.2) (16). The exact prevalence of ATE is not known, but among those seeking treatment, women are overrepresented, probably due to unawareness or underreporting in males. It can occur in people of any age, any gender, and any racial background and can be triggered by metabolic stress, hormonal changes, or medications, including retinoids (17). ATE is usually a reactive and self-limiting condition. FIGURE 22.2 Acute telogen effluvium. The condition can be assessed and monitored using the hair pull test (Figure 22.3), where the clinician applies traction to a bundle of scalp hairs. If more than 10% of the hairs in each bundle are removed from the scalp area, the hair pull test is considered positive. Removal of the inciting factor will usually lead to spontaneous improvement (16). In general, reassurance about the reversibility of the hair loss is sufficient to alleviate the patient’s concern. Dose reduction or cessation of therapy may be necessary in more severe cases. In some cases, telogen effluvium may not spontaneously resolve when the inciting trigger is removed. Chronic telogen effluvium is a diffuse hair loss of the scalp that persists longer than 6 months. It is characterized by abrupt, diffuse shedding of hair that runs a fluctuating course over several years (18). Patients receiving systemic treatment with synthetic retinoids often suffer from substantial retinoid-induced ATE. This is one of the most frequent and psychologically distressing adverse effects of retinoid therapy, which results in premature termination of a clinically desired and often highly effective systemic therapy with retinoids (19). The risk of ATE due to the systemic retinoids has been reported to vary over a range of 10%–75% (20). The risk is greater for acitretin than for etretinate therapy and is much less common with isotretinoin and bexarotene. Hair loss is a dose-related effect and is reversible starting 2 months after either discontinuation of therapy or a significant dose reduction. Hair loss may affect body hair also, with mild hair loss involving the pubic, axillary, and vellus hairs. Increased hair fragility may also be observed. As with telogen effluvium of other causes, women report more noticeable hair loss than men, and the condition may make underlying mild androgenic alopecia more obvious. The administration of systemic retinoids can induce a large number of hair follicles in the growing (anagen) phase to shift to the telogen phase. It is estimated that approximately 7%−35% of the follicles may shift to this state (17). Growth of the telogen hairs ceases for 1−6 months (on average 3 months), though this cessation of growth is not noticed by the patient. When the hairs 131 Retinoids in Hair Disorders FIGURE 22.3 The hair pull test—Around 10–20 hairs are grasped firmly at the scalp between the thumb and index finger, and traction is applied as the hairs are pulled along their length. re-enter the growth phase (anagen), the hairs that had been suspended in the resting phase (telogen) are extruded from the follicle, and hair shedding is observed. A small proportion of ATE cases may experience persistent, episodic shedding, as some follicles may not revert to an asynchronous growth p­ attern (18). The exact mechanism by which systemic retinoids induce ATE has not been established, but it has been hypothesized that it is due to defective anchoring of the hair shaft during telogen (21). It has also been postulated that ATE may in part be due to upregulation of transforming growth factor-beta 2, which is a key inducer of catagen and has been shown to have significant upregulation of transcripts with retinoic acid-treated hair bulbs (9). Alopecia Areata Alopecia areata (AA) is an autoimmune, non-scarring alopecia that is mediated by CD8+ T-cell attack on the lower cycling hair follicle and a loss of immune privilege in the hair follicle (Figure 22.4) (22). Lesions of AA often resolve spontaneously, but the disease may progress to loss of all scalp hair (alopecia totalis) or to total loss of scalp and body hair (alopecia universalis). AA is a common disease, affecting about 0.2% of the population (22). Males and females are affected equally, and the prevalence is almost the same for all ethnic groups. Studies suggest AA is a complex polygenetic disease that also involves exogenous, environmental factors (23). It has been suggested that vitamin A may play a role in the formation of AA, with vitamin A toxicity leading to the establishment of AA (24). It has been reported that the expression of retinoid synthesis enzymes and binding proteins are increased in human patients with AA, as well as in rodent models (25). It was noted that feeding mice high levels of dietary vitamin A combined with increased retinoic acid synthesis accelerated the onset of AA (25). Furthermore, in mice with excess retinol and all-trans-retinoic acid within the basal epidermis and outer root sheath, progressive cyclical alopecia with accelerated telogen to anagen transition was noted. In contrast, a severe reduction in dietary vitamin A intake resulted in a reduction in alopecia-related anagen induction. Vitamin A also directly regulates the immune response, having been shown to increase T-helper 2 and reduce T-helper 1 cytokines (26). Vitamin A also reduces levels of interferon gamma, which has been shown to play a key role in the etiology of AA (26). It has been suggested that vitamin A may promote the FIGURE 22.4 follicles. Alopecia areata with a close-up examination of scalp hair initiation of the anagen hair cycle, which likely increases follicle susceptibility to autoimmune destruction (27). Together, these reports implicate retinoids in the pathogenesis of AA, although the precise mechanism behind these effects remains unclear and requires further investigation. Other Hair Disorders It has been noted that acquired progressive kinking of the hair was present in a case series of three patients who were prescribed 132 Retinoids in Dermatology long-term oral etretinate at 50 mg/day or more (28). Kinking of the hair was noticed 3–12 months after starting treatment and coincides with the normal anagen cycle of hair growth. This finding suggests that systemic retinoid treatment at high doses may have a dynamic effect on the inner root sheath or may represent a pre-alopecia phase of hair loss. There have also been case reports that have documented hair color lightening and darkening while during oral etretinate treatment for psoriasis (29) and pityriasis rubra pilaris (30). Repigmentation of white hair and change of hair texture after 6 months of oral acitretin (25 mg/day) for treatment of psoriasis has also been reported (31). Retinoids for Treatment of Hair Disorders Frontal Fibrosing Alopecia Frontal fibrosing alopecia (FFA) is a primary lymphocytic scarring alopecia with a distinctive clinical pattern of progressive frontotemporal hairline recession and eyebrow loss that mainly affects postmenopausal women (Figure 22.5) (32). Histopathology from affected regions shows an immune-mediated inflammatory infiltrate of lymphocytes surrounding the bulge region of the hair follicle. Inflammation of the bulge area destroys the hair follicle stem cells, preventing hair regeneration (32). Hair follicles are permanently replaced by a scar-like fibrous tissue. It has been hypothesized that loss of the follicular immune privilege and a peroxisome proliferator-activated receptor-γ deficiency may enable the inflammatory process to attack the stem cells in the bulge region and permanently destroy them (33). A recent study assessing the efficacy of oral isotretinoin and acitretin in treatment of FFA showed success with this treatment modality (34). The investigators reported an arrest of disease ­progression in the majority of patients using oral isotretinoin 20 mg/day and in those treated with acitretin 20 mg/day. Furthermore, results were superior to the control group treated with finasteride 5 mg/day. Notably, in contrast to all other drugs used to treat FFA, this study noted no disease progression after discontinuation of treatment. The mechanism of action of retinoids in FFA is not fully understood but may represent an anti-inflammatory effect that contributes to normalizing of the antigen expression of the hair follicle keratinocytes. Androgenetic Alopecia Unlike AA, which is caused by an autoimmune reaction at the hair follicle, androgenetic alopecia (AGA) (commonly referred to as male- or female-pattern baldness) is caused by the heightened sensitivity of scalp follicles to dihydrotestosterone. In men, hair loss typically involves the temporal and vertex region while sparing the occipital region: the characteristic “horseshoe” pattern (35). AGA features a progressive miniaturization of the hair follicle leading to vellus transformation of terminal hair. This results from an alteration in hair cycle dynamics: anagen phase duration gradually decreases and the telogen phase increases. As the anagen phase duration determines hair length, the new anagen hair becomes shorter, eventually leading to bald appearance (35). Data on the use of topical retinoids to treat AGA was first described in 1986, within a cohort of 56 subjects (36). Results showed that after 1 year of combination treatment involving the use of topical tretinoin with 0.5% minoxidil, there was terminal hair regrowth in 66% of the subjects (36). Treatment with tretinoin monotherapy was also shown to stimulate some hair regrowth in approximately 58% of patients. It has been documented that the percutaneous absorption of 2% minoxidil is increased nearly threefold by the addition of 0.05% tretinoin, which increases the permeability of the stratum corneum (37). When minoxidil combined with tretinoin is applied only once daily, the urinary excretion of minoxidil was found to be significantly higher than that of minoxidil alone applied twice daily; moreover, 0.5% minoxidil plus 0.025% tretinoin (95% alcohol plus 5% propylene glycol vehicle) applied twice daily to the affected scalp area was reported to prolong the anagen hair ratio and induce new hair regrowth (37). These findings prompted further studies into the efficacy of combined retinoids. One study assessed the efficacy of 5% topical minoxidil solution with the use of 0.01% tretinoin (38). The efficacy and safety of therapy was compared using a combined solution of 5% minoxidil and 0.01% tretinoin once daily with that of conventional 5% topical minoxidil therapy applied twice daily for treatment of AGA. No statistical differences were found between the two treatment groups, therefore validating the use of daily treatment including the use of 0.01% tretinoin, instead of twice-daily treatment with minoxidil monotherapy. Alopecia Areata FIGURE 22.5 Frontal fibrosing alopecia. Although systemic retinoid therapy has been shown to induce hair loss in some patients, approaches involving the use of topical retinoids have shown promising results as therapeutic options for treatment of AA. This difference in mode of administration most likely represents targeted growth and differentiation from topical retinoid application versus a complete systemic response that may recruit a multitude of other biochemical pathways that possibly result in unwanted side effects such as AA. In a phase I/II randomized, half-head trial reviewing the efficacy of 1% bexarotene gel for management of treatment refractory AA, general improvement in hair regrowth was found 133 Retinoids in Hair Disorders within a cohort of 42 patients over 24 weeks (39). Five of 42 (12%) had 50% or more partial hair regrowth on the treated side, and 6 of 42 (14%) on both sides, including 3 complete responders. Side effects included mild scalp irritation in 31/42 patients, with 4 patients having grade-3 irritation. Topical tretinoin (0.05%) cream was also compared to topical betamethasone dipropionate, dithranol paste (0.25%), and white soft petroleum jelly in a cohort study of 80 patients with AA (40). Medications were applied to the patients twice daily for 3 months. Assessment at the 3-month time interval showed good regrowth in 55% of patients using tretinoin versus 70%, 35%, and 20% of those who used topical steroids, dithranol paste, or white soft petroleum jelly, respectively. In a more recent study, the effectiveness of adapalene in combination with steroids has been assessed for treatment of AA. The researchers compared the efficacy of topical mometasone furoate 0.1% cream monotherapy versus mometasone furoate 0.1% cream plus adapalene 0.1% gel in the treatment of AA (41). Over a 12-week study period, mean regrowth scores were higher in patients who were exposed to combination therapy. Mean percentages of hair regrowth in the combination group were statistically higher than monotherapy group for the fourth (50.2% vs. 23.5%), eighth (78.5% vs. 50.7%), and twelfth week (90.5% vs. 71%). This new approach has potential as a future therapeutic modality in the treatment of AA. Monilethrix Monilethrix presents clinically with hair that tends to be normal at birth but becomes short, fragile, and brittle within months. This results in hypotrichosis, particularly on the occipital scalp (42). It is characterized by regular, periodic thinning of hair shafts, giving them a beaded appearance. Although the occipital scalp is most commonly affected, the eyebrows and eyelashes can be involved, as well as the nails. Three genes have been associated with monilethrix (KRT81, KRT83, and KRT86), which are responsible for the autosomal dominant form of the disease (43). Systemic retinoids have been reported as potential therapeutic options for the treatment of monilethrix. A single case of childhood monilethrix showed increased hair length with loss of beading along the hair shaft with a dose of 0.5 mg/kg of etretinate over 6 months (44). During treatment, the scalp appearance of keratosis pilaris persisted, suggesting that the beading alone was influenced by etretinate. A second case report found cosmetic and clinical improvement with the use of 0.5 mg/kg of acitretin in a 7-year-old girl over a 12-month period, but clinical symptoms recurred within 4 months of therapy discontinuation (45). Conclusions Retinoids are implicated in the pathogenesis and treatment of various hair disorders. Vitamin A and retinoids play an important role in hair follicle transformation and the hair cycle. Therefore, their use may interrupt the normal hair cycle and can cause a diffuse hair loss that presents as a telogen effluvium. They may also be responsible for changes in hair texture and color. Generally, hair loss due to retinoids is reversible with the medication’s withdrawal, and the overall prognosis is favorable. Conversely, there is emerging evidence that retinoids are effective treatments for various hair disorders, including frontal fibrosing alopecia, alopecia areata, androgenetic alopecia, and monilethrix. REFERENCES 1. Rollman O, Vahlquist A. Cutaneous vitamin A levels in seborrheic keratosis, actinic keratosis, and basal cell carcinoma. Arch Dermatol Res. 1981;270:193–196. 2. Oliviera LM, Teixeria LME, Sato MN. Impact of retinoic acid on immune cells and inflammatory diseases. Mediators Inflamm. 2018:3067126. 3. Bergfeld WF. Retinoids and hair growth. J Am Acad Dermatol. 1998;39:S86–S89. 4. Stenn KS, Paus R. Controls of hair follicle cycling. Physiol Rev. 2001;81:449–494. 5. Grover C, Khurana A. Telogen effluvium. Indian J Dermatol Venereol Leprol. 2013;79:591–603. 6. Krause K, Foitzik K. Biology of the hair follicle: The basics. Semin Cutan Med Surg. 2006;25:2–10. 7. Okano J, Levy C, Lichti U et al. Cutaneous retinoic acid levels determine hair follicle development and downgrowth. J Biol Chem. 2012;287:39304–39315. 8. Everts HB. Endogenous retinoids in the hair follicle and sebaceous gland. Biochim Biophys Acta. 2012;1821:222–229. 9. Foitzik K, Spexard T, Nakamura M et al. Towards dissecting the pathogenesis of retinoid-induced hair loss: All-trans retinoic acid induces premature hair follicle regression (catagen) by upregulation of transforming growth factor-beta 2 in the dermal papilla. J Invest Dermatol. 2005;124:1119–1126. 10. Bilousova G, Chen JA, Roop DR. Differentiation of mouse induced pluripotent stem cells into a multipotent keratinocyte lineage. J Invest Dermatol. 2011;131:857–864. 11. Duverger O, Morasso MI. Role of homeobox genes in the patterning, specification and differentiation of ectodermal appendages in mammals. J Cell Physiol. 2008;216:337–346. 12. Persaud SD, Lin YW, Wu CY et al. Cellular retinoic acid binding protein 1 mediates rapid non-canonical activation of ERK1/2 by all-trans retinoic acid. Cell Signal. 2013;25:19–25. 13. Reichrath J, Mittmann M, Kamradt J et al. Expression of retinoid-X receptors (-alpha,-beta,-gamma) and retinoic acid receptors (-alpha,-beta,-gamma) in normal human skin: An immunohistological evaluation. Histochem J. 1997;29:127–133. 14. Billoni N, Gautier B, Mahe YF et al. Expression of retinoid nuclear receptor superfamily members in human hair follicles and its implication in hair growth. Acta Derm Venereol. 1997;77:350–355. 15. Viallet JP, Dhouailly D. Retinoic acid and mouse skin morphogenesis: Expression pattern of retinoic acid receptor genes during hair vibrissa follicle, plantar, and nasal gland development. J Invest Dermatol. 1994;103:116–121. 16. Harrison S, Sinclair R. Telogen effluvium. Clin Exp Dermatol. 2002;27(5):389–395. 17. Bergfeld WF. Telogen effluvium. In: McMichael A, Hordinsky M, editors. Hair and Scalp Diseases: Medical, Surgical and Cosmetic Treatments. Informa Health Care. 2008. p. 119. 18. Messenger AG, de Berker DA, Sinclair RD. Chapter 66: Disorders of hair. In: Burns T, Breathnach S, Cox N, editors. Rook’s Textbook of Dermatology. 8th ed. UK: Blackwell Publishing. 2010. pp. 27–66. 134 19. Katz HI, Waalen J, Leach EE. Acitretin in psoriasis: An ­overview of adverse effects. J Am Acad Dermatol. 1999;41: S7–S12. 20. Murray HE, Anhalt AW, Lessard R et al. A 12-month treatment of severe psoriasis with acitretin: Results of a Canadian open multicenter study. J Am Acad Dermatol. 1991;24: 598–602. 21. Berth-Jones J, Hutchinson PE. Novel cycle changes in scalp hair are caused by etretinate therapy. Br J Dermatol. 1995;132:367–375. 22. Pratt CH, King LE, Messenger AG. Alopecia areata. Nat Rev Dis Primers. 2017;3:17011. 23. Petukhova L, Duvic M, Hordinsky M et al. Genome-wide association study in alopecia areata implicates both innate and adaptive immunity. Nature. 2010;466:113–117. 24. Shih MYS, Kane MA, Zhou P et al. Retinol esterification by DGAT1 is essential for retinoid homeostasis in murine skin. J Biol Chem. 2009;284:4292–4299. 25. Duncan FJ, Silva KA, Johnson CJ et al. Endogenous retinoids in the pathogenesis of alopecia areata. J Invest Dermatol. 2013;133:334–343. 26. Freyschmidt-Paul P, McElwee KJ, Hoffmann R et al. Interferon-gamma-deficient mice are resistant to the development of alopecia areata. Br J Dermatol. 2006;155:515–521. 27. Darwin E, Hirt PA, Fertig R et al. Alopecia areata: Review of epidemiology, clinical features, pathogenesis, and new treatment options. Int J Trichology. 2018;10:51–60. 28. Graham RM, James MP, Ferguson DJ et al. Acquired kinking of the hair associated with etretinate therapy. Clin Exp Dermatol. 1985;10:426–431. 29. Nanda A, Alsaleh QA. Hair discolouration caused by etretinate. Dermatol. 1994;188:172. 30. Vesper JL, Fenske NA. Hair darkening and new growth associated with etretinate therapy. J Am Acad Dermatol. 1996;34:860. 31. Seckin D, Yildiz A. Repigmentation and curling of hair after acitretin therapy. Australas J Dermatol. 2009;50:214–216. 32. Iorizzo M, Tosti A. Frontal fibrosing alopecia: An update on pathogenesis, diagnosis, and treatment. Am J Clin Dermatol. 2019;20:379–390. Retinoids in Dermatology 33. Karnik P, Tekeste Z, McCormick TS et al. Hair follicle stem cell-specific PPAR-γ deletion causes scarring alopecia. J Investig Dermatol. 2009;129:1243–1257. 34. Rakowska A, Gradzinska A, Olszewska M, Rudnika L. Efficacy of isotretinoin and acitretin in treatment of frontal fibrosing alopecia: Retrospective analysis of 54 cases. J Drugs Dermatol. 2017;16:988–992. 35. Lolli F, Pallotti F, Rossi A et al. Androgenetic alopecia: A review. Endocrine. 2017;57:9–17. 36. Bazzano GS, Terezakis N, Galen W. Topical tretinoin for hair growth promotion. J Am Acad Dermatol. 1986;15:880–893. 37. Ferry JJ, Forbes KK, VanderLugt JT, Szpunar GJ. Influence of tretinoin on the percutaneous absorption of minoxidil from an aqueous topical solution. Clin Pharmacol Ther. 1990;47:439–446. 38. Shin HS, Won CH, Lee SH et al. Efficacy of 5% minoxidil versus combined 5% minoxidil and 0.01% tretinoin for male pattern hair loss. Am J Clin Dermatol. 2007;8:285–290. 39. Talpur R, Vu J, Bassett R et al. Phase I/II randomized bilateral half-head comparison of topical bexarotene 1% gel for alopecia areata. J Am Acad Dermatol. 2009;61:592–e1. 40. Das S, Ghorami RC, Chatterjee T, Banerjee G. Comparative assessment of topical steroids, topical tretinoin (0.05%) and dithranol paste in alopecia areata. Indian J Dermatol. 2010;55:148. 41. Unal M. Use of adapalene in alopecia areata: Efficacy and safety of mometasone furoate 0.1% cream versus combination of mometasone furoate 0.1% cream and adapalene 0.1% gel in alopecia areata. Dermatol Ther. 2018;31:e12574. 42. Singh G, Miteva M. Prognosis and management of congenital hair shaft disorders with fragility—part I. Pediatr Dermatol. 2016;33:473–480. 43. Van Steensel M, Vreeburg M, Urbina MT et al. Novel KRT83 and KRT86 mutations associated with monilethrix. Exp Dermatol. 2015;24:222–224. 44. De Berker D, Dawber RP. Monilethrix treated with oral retinoids. Clin Exp Dermatol. 1991;16:226–228. 45. Karincaoglu Y, Coskun BK, Seyhan ME et al. Monilethrix: Improvement with acitretin. Am J Clin Dermatol. 2005;6:407–410. 23 Retinoids in Psoriasis Uwe Wollina, Piotr Brzezinski, and André Koch Introduction Psoriasis is a common, chronic or relapsing, systemic inflammatory disorder mediated by dendritic cells, T-lymphocytes, and neutrophils (1,2). It has been suggested that 2%–4% of the world population is affected by psoriasis (3). Incidence and prevalence of psoriasis show regional and ethnic variability. The incidence varies from 78.9/100,000 personyears (PY) (United States) to 230/100,000 PY (Italy) (4). Psoriasis can affect all ages. The prevalence in children ranged from 0% (Taiwan), 0.71% (Germany), to 2.1% (Italy), and in adults it varied from 0.91% (United States), 8.5% (Norway) (4), 61.5 per 100,000 population in South Korea (5), to 281.5 per 100,000 population in Taiwan (6). In children, the incidence estimate reported (United States) was 40.8/100,000 PY (aged ≤16 years). The prevalence in Germany was 0.71% (4). The incidence and prevalence of psoriatic arthritis, the most common extracutaneous manifestation of psoriasis, has been ­calculated as 83 per every 100,000 PY and 133 per 100,000 ­population (7). Psoriasis can be associated with a negative impact on quality of life independent from the classification as mild, moderate, or severe (1). Genetics may not only affect the clinical presentation and severity of the psoriatic disease but modulate treatment response. A whole exome sequencing analysis in psoriasis patients identified four single nucleotide polymorphisms were found to be significantly associated with acitretin response, i.e., rs1105223T>C in CRB2, rs11086065A>G in ANKLE1, rs3821414T>C in ARHGEF3, and rs1802073T>G in SFRP4. CRB2 rs1105223CC and ANKLE1 rs11086065AG/GG were associated with acitretin failure (8). Oral Retinoids Retinoid’s Mechanism of Action Specific for Psoriasis Treatment The term “retinoid” refers to compounds that have structural or biological activities similar to retinol or vitamin A. In psoriasis, retinoids exert versatile activities. They interact with keratinocytes, fibroblasts, endothelial cells, neutrophils, T cells, and Langerhans cells. Retinoids affect keratinocytes in different mechanisms of action. They stimulate glycosylation, normalize keratin expression, and stimulate DNA-synthesis (9–11). Retinoids reduce desmosomal size and thereby contribute to an improved ­ ­shedding of horny cell layers (12). Tazarotene, a retinoic acid receptor (RAR)-specific retinoid, reduces the expression of keratinocyte markers associated with a hyperproliferative status (13). In psoriasis patients, a significant negative correlation between the severity of the disease as expressed by the Psoriatic Area and Severity Index score (PASI) and the binding of RI regulatory subunit of cAMP-dependent protein kinase (PKA) to the cAMP analog (8-azido [32P] cAMP) in erythrocyte membranes has been observed. Etretinate treatment resulted in a correction of the binding defect (14,15). Retinoids affect vascularization and blood vessel permeability. It was shown that all-trans-retinoic acid (ATRA), 13-cis RA, and all-trans retinol reduced vascular endothelial growth factor (VEGF)/vascular permeability factor (VPF) secretion by epidermal keratinocytes in vitro. The reduction in VEGF/VPF protein was paralleled by a strong downregulation of VEGF/VPF mRNA levels. This can cause a reduction in psoriasis-associated angioproliferation in affected skin (16). Retinoids also have an impact on immunity and inflammation. It was shown that the abnormal distribution of Langerhans cells in affected psoriatic epidermis becomes normalized by retinoids (17). Etretinate reduces increased neutrophil chemotaxis in psoriasis, in particular in pustular psoriasis (18). Acitretin decreases the release of leucotrienes and dihydroeicosatetraenoic acid and inhibits ornithine decarboxylase thus reducing the synthesis of polyamines (19). Etretinate also inhibits keratinocyte production of vascular endothelial growth factor. With molecular techniques such as large DNA microarrays it could be demonstrated that retinoids suppress the protein markers of cornification, the genes responsible for biosynthesis of epidermal lipids, long-chain fatty acids, cholesterol, and sphingolipids. Retinoids stimulate genes associated with the cell cycle and programmed cell death (apoptosis). The response to retinoids is very fast, because 315 genes were regulated after 1 h of more than 500 genes influenced by retinoids (20). Retinoic acid is a regulator of T-helper cell differentiation, ­function, and homing as well as lymphoid organ development (21). 135 136 Retinoids in Dermatology TABLE 23.1 Retinoids in Psoriasis Retinoid Target (s) Psoriasis First-Generation Retinoids All-trans-retinoic acid Tretinoin Isotretinoin Alitretinoin RARs, RXRs, PPAR-β/δ and polymorphic retinoic acid response elements RAR-α, RAR-β, and RAR-γ RAR-γ, RXR RARs and RXR Second-Generation Retinoids Etretinate RARs and CRABP (cellular retinoic acid binding protein) binding Acitretin RARs and CRABP binding Third-Generation Retinoids Tazarotene Selectivity for the beta and gamma RARs Bexarotene RXR-selective Adapalene RAR-β, RAR-γ – – (+) (+) + + + (+) – RAR, Nuclear retinoic acid receptors; RXR, retinoid X receptor. In conclusion, retinoids regulate proliferation, differentiation, inflammation, and immune response (Table 23.1). Oral Retinoids in Adults Historical Background Oral retinoids were introduced into the treatment of psoriasis in the mid-1970s. The first systemic compound was etretinate (Ro 10-9359), a prodrug which becomes hydrolyzed into acitretin (22,23). In the first controlled multicenter trial, 291 patients with psoriasis were treated either by etretinate, topical anthralin, or both. Good results were obtained in 120 patients (61%) treated with oral etretinate; no response was observed in 31 (15.8%). The initial dose was 1.0 mg/kg body-weight/day, subsequently reduced to 25–50 mg/day. In particular, erythrodermic and severe pustular forms responded well. The oral treatment was stopped in 14% of patients due to adverse events (24). Oral retinoids are an option for the treatment of moderate to severe psoriasis; topical retinoids may be used in all types of psoriasis if appropriate. Etretinate Combinations Because etretinate monotherapy had only a moderate effect on psoriasis, combined treatments with topicals and phototherapy had been investigated to improve the outcome of patients. Etretinate combined with topical calcipotriol cream for 3 weeks achieved an improvement of the PASI score by 50.7% compared to 39% with etretinate alone, indicating a faster response of the combination (25). In another trial, 45 psoriasis patients with extensive plaque or guttate psoriasis were treated either with ultraviolet B (UVB) narrow-band (311 nm) phototherapy, etretinate plus UVB, or psoralen plus ultraviolet-A (PUVA). The combined etretinate−phototherapy was superior to UVB alone and reduced the cumulative dosage of irradiation. PUVA plus etretinate had a 100% response rate compared to 93% of etretinate plus UVB. Six months after treatment, 50% of etretinate-PUVA-treated patients remained in remission compared to 33% of etretinate-UVB (26). Long-term therapy with etretinate (up to 4 years) did not increase the risk of cardiovascular disease, diabetes, inflammatory bowel disease, or cancer (27). Acitretin—Monotherapy in Moderate to Severe Plaque Psoriasis Etretinate has been substituted by acitretin. Acitretin is the current principal oral aromatic retinoid. Compared to etretinate it is less hydrophobic, the half-life for elimination is 2 days compared to 120 days for etretinate. For both retinoids, 3-year contraception after stopping the treatment is warranted to avoid teratogenic effects. Patients may not donate blood up to 3 years after discontinuation of treatment (28). The recommended starting dose of acitretin is 20–30 mg/day with a slow dose increment, usually up to 75 mg/day. Because adverse effects are dose-dependent, the maximum dose has to be individualized (28). A PASI is used to quantify the clinical response to antipsoriatic treatment. A PASI75 response (75% improvement) is achieved by 50–75 mg acitretin/day in about 25%–75% of patients (29–31). A randomized, double-blind study investigated three different fixed doses for severe plaque psoriasis, i.e., 25, 35, and 50 mg. After 12 weeks, PASI75 was achieved in 47%, 69%, and 53%, respectively (32). In a double-blind placebo-controlled trial, acitretin at a dosage of 25–75 mg/day reduced erythema, scaling, and induration within 8 weeks but not affected body surface area. A prolonged treatment of at least 20 weeks, however, improved body surface area by 44% (33). Low-dose acitretin with a starting dose of 10 mg/day gradually increased to 25–35 mg/day resulted in a PASI75 response in 47.8% and a PASI50 response in 87% of patients after 10–16 weeks, and a PASI75 after 16 weeks in 67.3%. The benefit of low-dose therapy is the reduction of adverse effects and increased drug adherence. Cheilitis occurs in 100% of traditionally treated psoriasis patients, while only 10.9% experienced this side effect with low-dose treatment. Drug withdrawal was observed in 8.7% (34). For maintenance therapy, a dosage between 25 and 50 mg/day has been recommended (28). Acitretin is not a fast-acting compound and may need 3–4 months for a full response (35). Therefore, drug adherence is of great importance. Acitretin is the major oral retinoid for moderate to severe psoriasis. Moderate or low doses are better tolerated than higher ones. Acitretin in monotherapy needs more time to achieve a significant clinical response than other oral antipsoriatic drugs. Therefore, combinations with other treatment modalities make sense. Acitretin Combined with Phototherapy To increase efficacy and speed of clinical response, acitretin may be combined with narrow-band UVB light (311 nm) or PUVA. Hereby, the number of phototherapy sessions and the dosage of acitretin can be reduced. This increases treatment adherence of patients (36–38). 137 Retinoids in Psoriasis Acitretin Combined with Classical Oral Antipsoriatic Drugs German guidelines do not recommend concomitant use of acitretin with methotrexate, because this can lead to increased hepatotoxicity (28). In an uncontrolled trial with 18 patients, however, the combination has not resulted in an increased hepatotoxicity during an average treatment course of 9 months as long as patients remained abstinent from alcohol. The efficacy, on the other hand, was only moderate. Eight patients did either not respond or experienced adverse events (39). There are not enough data available to recommend a combination in psoriasis treatment with either systemic corticosteroids, cyclosporine A, or fumaric acid esters (28). TABLE 23.2 Systemic Aromatic Retinoids in Psoriasis Daily Dosage (s) Compound Indications (s) Initial Etretinate Acitretin Plaque psoriasis Pustular psoriasis Erythrodermic psoriasis Nail psoriasis Psoriatic arthritis Plaque psoriasis Childhood psoriasis Maximal Maintenance 0.5 mg/kg 1.0 mg/kg 0.5–1.0 mg/kg 0.5 mg/kg 1.0 mg/kg 0.5 mg/kg 0.3 mg/kg 1.0 mg/kg 0.5 mg/kg 0.5 mg/kg 0.5 mg/kg 10–25 mg/kg 0.1 mg/kg 1.0 mg/kg 1.0 mg/kg 75 mg/kg 0.5 mg/kg 0.5 mg/kg 0.5 mg/kg 25–50 mg/kg Acitretin and Biologicals Biologicals are increasingly used to treat patients with moderate to severe psoriasis. Etanercept is a tumor necrosis factor-alpha receptor antagonist approved for psoriasis and psoriatic arthritis. The combination of acitretin with etanercept may increase the efficacy of treatment (28). A multicenter, randomized, open-label trial assessed the efficacy and safety of acitretin 10 mg twice daily, acitretin plus 25 mg etanercept twice weekly, and etanercept 50 mg twice weekly followed by etanercept 25 mg twice weekly. At week 24, acitretin achieved a PASI50 of 44.4% and a PASI75 of 22.2%, while the combination treatment was superior with PASI50 84.2% and PASI75 57.9%. The etanercept-only group achieved PASI50 and PASI75 of 71.4% and 52.4%. Acitretin add on obviously improved the efficacy of etanercept (40). Acitretin has not yet been systematically investigated in combination with other biologicals and related drugs. Acitretin in Pustular Psoriasis Pustular psoriasis is a treatment challenge. The most common subtypes are generalized pustular psoriasis and palmoplantar pustular psoriasis. Generalized pustular psoriasis is a dermatologic emergency. In generalized pustular psoriasis, initiating dosages of acitretin should be higher compared to plaque psoriasis (Table 23.2). Acitretin is considered to be a first-line systemic treatment in this severe psoriasis subtype (35,41). (a) In palmoplantar pustular psoriasis (Figure 23.1), acitretin has some benefit. In a prospective, randomized trial with 111 patients, acitretin 0.5 mg/kg daily achieved a modified palmoplantar PASI (mPPPASI) response of 75% in 8% after 12 weeks of treatment. In this trial, however, methotrexate was more efficacious than acitretin (42). After withdrawal of acitretin, a relapse occurs when no other systemic treatment has been introduced (Figure 23.2). Acitretin combined with PUVA is recommended in particular for palmoplantar pustular psoriasis as second-line therapy after failure of high-potency topical corticosteroids (43). Acitretin in Erythrodermic Psoriasis Erythrodermic psoriasis is a dermatologic emergency. In erythrodermic psoriasis, acitretin should be started at lower dosages (Table 23.2) (44). The disadvantage of acitretin is the slower response compared to cyclosporine A or biologicals (45). Acitretin in Nail Psoriasis In an open trial with 36 patients with nail involvement, acitretin improved the Nail Psoriasis Severity Index (NAPSI) by 41% after 6 months of treatment; 25% achieved a complete clearance (46). Slow improvement of nail psoriasis has also been observed in other trials (47,48). (b) FIGURE 23.1 Palmoplantar psoriasis—an indication for acitretin or RePUVA. (a) Palmar lesion with infiltration, pustules, and scaling. (b) Plantar lesions on typical plantar area with pustulation. 138 Retinoids in Dermatology Isotretinoin in Psoriasis—Combination with Phototherapy Isotretinoin is an oral retinoid approved for the treatment of severe acne. Its use in psoriasis is off-label. A randomized single-blind trial compared isotretinoin 0.5 mg/kg daily with narrow-band UVB versus narrow-band UVB alone. The study was completed by 37 patients with plaque psoriasis. At week 14, complete clearance was reported in 14 patients of the intervention group and 13 in the control group. Isotretinoin reduced the UVB exposure significantly (57). A hospital-based randomized trial compared isotretinoin plus PUVAsol (psoralen + sunlight) with PUVAsol alone in 40 patients with plaque psoriasis. Isotretinoin reduced the mean time to achieve a PASI75, the number of PUVAsol sessions and the mean cumulative dosage of 8-methoxypsoralen to achieve a PASI75 response (58). Wilken et al. reported about two patients with recalcitrant palmoplantar pustular psoriasis who responded to isotretinoin and UVA (59). Bexarotene in Psoriasis FIGURE 23.2 59-year-old patient with relapse of palmar psoriasis after withdrawal of acitretin. Acitretin in Patients with Chronic Infections and/or Immunosuppression Human immunodeficiency virus (HIV) infection is a known trigger factor for psoriasis induction and exacerbation (49). Acitretin is safe in patients with HIV infection and is recommended as second-line treatment after failure of topical treatment (50). Acitretin is a possible aggravating factor in hepatitis A (51). Acitretin is the only drug that could be administered during the active phases of hepatitis B infection; however, the administration of this drug should be reserved only for selected cases ­ without a severe impairment of liver function (52). Considering hepatitis C infection, only very limited data are available on antipsoriatic treatment. Acitretin can be an option in those patients who lack progression to cirrhosis or other forms of severe hepatic impairment in high-need psoriasis patients (52). These patients need intensified monitoring. A well-recognized potential adverse event from acitretin is elevated transaminases, indicating acute hepatocyte damage. But it also bears the risk of possible cholestatic injury, signaled by elevated gamma-glutamyl transferase and alkaline phosphatase. These parameters should be monitored carefully (53). In patients with tuberculosis (TB), a combined deficiency of 13-cis retinoic acid has been reported (54). In vitro studies indicate that ATRA induces mechanistically distinct antimicrobial activities in cells with NPC intracellular cholesterol transporter 2 (55). In rats, retinoic acid attenuates TB severity while improving the host response to the infection (56). Because retinoids are neither immunosuppressive nor cytotoxic, they can also be used in cancer patients. Bexarotene is a retinoid X receptor (RXR)-selective retinoid approved for cutaneous T-cell lymphoma. In a phase II study, safety, tolerability, and effectiveness of bexarotene in psoriasis at doses of 0.5–3.0 mg/kg daily have been evaluated. Fifty patients with moderate to severe plaque-type psoriasis were treated with bexarotene for 12–24 weeks. Bexarotene was well tolerated in most patients without any serious adverse events. Typical laboratory side effects detected were hypertriglyceridemia (56%) and a decrease in free T4 serum levels (54%). Overall response rates (> or =50% improvement) for modified PASI was 22%. No significant dose-response effect was established (60). The use of bexarotene in psoriasis is off-label. Alitretinoin in Psoriasis Alitretinoin is a pan-retinoid-receptor agonist approved for severe chronic hand dermatitis. In a small trial, seven patients with recalcitrant palmoplantar pustular psoriasis were treated with oral alitretinoin 30 mg once daily for 12 weeks. Efficacy was assessed by PPPASI, visual analog scales (VAS) on intensity of pain and pruritus, and an overall patient assessment. At week 12, PPPASI and VAS for pruritus and pain decreased significantly. The overall patient assessment ranged from 60% to 90% clinical improvement. Treatment was well tolerated. Headache was reported in two patients (61). A phase II, randomized, double-blind, placebo-controlled, multicenter study investigated 33 adult patients with palmoplantar psoriasis refractory to topical therapy and standard skin care. Patients were randomized 2:1 to alitretinoin 30 mg once daily or placebo for up to 24 weeks. Thirty-three patients were randomized: 24 patients to alitretinoin 30 mg and 9 to placebo. Overall, there were no significant differences between alitretinoin 30 mg and placebo at week 24 for PPPASI, mPASI, change in pustule count on the palms and sole, and change in the NAPSI. The safety profile was consistent with that seen in patients with chronic severe hand eczema refractory to potent 139 Retinoids in Psoriasis topical corticosteroids. The trial did not encourage further studies (62). The use of alitretinoin in psoriasis is off-label. Oral Retinoids in Children and Adolescents Acitretin is a possible treatment modality in severe childhood and adolescent psoriasis with dramatic responses in selected patients (63). In a retrospective trial with children and adolescents younger than 17 years of age, the median maintenance daily dose was 0.41 mg/kg. A PASI75 response could be achieved in 44.4% of patients at week 16. The authors concluded that acitretin had only a moderate efficacy in their hands (64). In a retrospective study from France collecting data from 2000 to 2014, 154 patients younger than 18 years were analyzed. Acitretin was the most frequently used first-line systemic treatment. The best efficacy with 80.0% improvement was seen with a concurrent PUVA therapy (65). In a study from Chengdu, China, 26 children younger than 14 years of age with generalized pustular psoriasis were investigated. Sixteen patients were treated with acitretin 0.5–1.0 mg/kg daily with a maximum dosage of 40 mg/day and got “satisfactory results” (66). In a Malaysian trial with 27 patients suffering from juvenile pustular psoriasis, acitretin was effective in acute disease in 100% of 16 treated patients (67). The European Medicines Agency has approved acitretin for childhood psoriasis with a grade C recommendation (68). Safety Issues Contraindications of Etretinate and Acitretin Absolute contraindications include pregnancy and breastfeeding due to the high risk of teratogenicity. Severe renal insufficiency or hepatic disorders are contraindications for retinoids. Due to dryness of the eyes, contact lenses are contraindicated. High-dose vitamin A, imidazoles, methotrexate, and tetracyclines are contraindicated during retinoid therapy. Tetracyclines can lead to increased intracranial pressure (pseudotumor cerebri); methotrexate may cause drug-induced hepatitis. Low-dose progesterone contraceptives are not sufficient to protect against contraception during retinoid therapy. Phenytoin levels may become elevated. Another contraindication is excessive alcohol consumption. Alcohol consumption increases the conversion of acitretin to etretinate by transesterification (69). Relative contraindications are diabetes mellitus, a history of pancreatitis, hyperlipidemia, and atherosclerosis (70) (Table 23.3). Common cutaneous side effects are skin fragility, cheilitis, pruritus, alopecia, photosensitivity, and nail changes. Serum lipids can become elevated during treatment and should be monitored. In children, a bone monitoring in liaison with the pediatrician is recommended, to avoid negative effects on growth of the long bones. In adults, calcification of entheses is a rare event that does not justify systemic monitoring (71). Nausea, vomiting, fatigue, irritability and itch are characteristics for an acute overdose. Such patients need immediate TABLE 23.3 Contraindications for Retinoids Absolute Contraindications In women In men and women Pregnancy Nursing Absence of safe contraception for women during childbearing age Severe renal insufficiency Severe hepatic impairment Relative Contraindications Alcohol abuse Diabetes mellitus Use of contact lenses History of pancreatitis Hyperlipidemia Concurrent medication with tetracyclines or methotrexate Childhood Source: Nast AJ et al. Eur Acad Dermatol Venereol. 2015;29:2277–2294. withdrawal from retinoid therapy and close monitoring of renal function, vital parameters, and electrolytes (28). Monitoring (Table 23.4) Triglycerides, high-density lipoprotein, cholesterol, blood count, creatinine, liver enzymes should be controlled initially every month, after 3 months every quarter of a year; for women, pregnancy tests every 4 weeks up to 3 years after withdrawal of retinoids. In cases of coexistent diabetes mellitus, fasting blood sugar should be checked, especially during the induction therapy (28). Hyperlipidemia (trigylcerides, low-density lipoprotein-cholesterol) occurs in about 17% of patients treated with systemic retinoids. The drug binding to RXR leads to increased Apo C-III expression, which contributes to hypertriglyceridemia and atherogenic lipoprotein profile (72). The increased laboratory parameters may need a dose reduction or drug withdrawal. TABLE 23.4 Laboratory Monitoring for Acitretin Therapy Parameter Before Rxe Blood counta Liver enzymesb Lipidsc Pregnancyd x x x x Fasting blood Glucose x After After After 4 Weeks 8 Weeks 12 Weeks x x x x x x x x x x x x Every 3 Months x x x Every month x Source: Nast AJ et al. Eur Acad Dermatol Venereol. 2015;29:2277–2294. a Hemoglobin, hematocrit, leucocytes, thrombocytes. b Aspartate aminotransferase, alanine aminotransferase, gamma-glutamyl transferase, alkaline phosphatase. c Triglycerides, cholesterol, high-density lipoproteins. d Human chorionic gonadotropin in urine. e Rx = treatment. 140 Lipids can be lowered by nutrition, statins, and fibrates (73,74). Partial replacement of casein by fish oil or soy protein isolate have been shown to reduce retinoid-induced hyperlipidemia (75). In children, premature epiphyseal closure would lead to a short stature. Using the lowest doses of retinoids necessary for antipsoriatic activity and for limited time are the best preventive measures. Bone scans once a year are recommended in other chronic disorders like ichthyosis. In psoriasis, treatment is usually limited in time (76). Topical Retinoids Topical treatment is considered first-line treatment in psoriasis affecting <10% body surface or as adjuvant treatment in moderate to severe psoriasis (77). Tazarotene in Plaque Psoriasis Tazarotene 0.05% and 0.1% gel are FDA approved for plaque psoriasis. In two double-blind, placebo-controlled, 12-week trials, tazarotene was superior to placebo, with local irritation as the main adverse effect (78,79). Tazarotene 0.1% gel had a comparable efficacy to fluocinonide at week 12 but was less effective than clobetasol propionate cream 0.05%. Tazarotene, on the other hand, demonstrated a significantly better maintenance of treatment effect after withdrawal of treatment (80,81). Once daily for 12 weeks 0.1% tazarotene gel was comparable to 5% crude coal tar (82) or calcipotriol (83). Tazarotene was demonstrated to be superior to calcipotriol in maintenance (84). Tazarotene in Palmoplantar Pustular Psoriasis In an observer-blinded randomized trial, 30 patients with palmoplantar psoriasis were randomized to either once-daily application of tazarotene 0.1% or once-daily clobetasol propionate cream 0.05% for 12 weeks. Complete clearance was achieved in 52.9% of the patients with tazarotene compared with 61.5% of the patients treated with the topical corticosteroid (p > 0.05) (85). Tazarotene Combined with Topical Corticosteroids A systematic review rated the absolute response rates for trunk and limb psoriasis treated with once-daily tazarotene as 27.3% compared to anthralin (42.8%), vitamin D (43.5%), or very potent corticosteroids (67.9%) (86). To improve the response rates, a fixed combination with corticosteroids seems promising. A multicenter, randomized, double-blind, vehicle-controlled phase 2 study in moderate or severe psoriasis (n = 212) compared a once-daily application of a fixed combination of halobetasol propionate 0.01% and tazarotene 0.045% (HP/TAZ) with the single components and placebo. At week 8, the HP/TAZ lotion was superior in reducing erythema, infiltrations, and scaling at the target lesion. The most frequently reported adverse effects were application site reactions associated with the tazarotene component. Side effects such as skin atrophy were rare (87). Retinoids in Dermatology Tazarotene and Phototherapy Tazarotene can be combined with UVB phototherapy for plaque psoriasis for faster response and reduction of UV exposure (88). Tazarotene in Nail Psoriasis In a small trial, 6 patients diagnosed with nail psoriasis were treated with tazarotene 0.1% ointment under occlusion every night for 6 months in their homes as a monotherapy. Mean NAPSI decreased from 14.3 to 2.3. The percentage improvement at the end of 6 months treatment was 87.9%. No adverse effects were observed (89). A left-to-right controlled trial of 25 patients with recalcitrant bilateral fingernail psoriasis compared tazarotene 0.1% ointment alone with tazarotene 0.1% and 595 nm pulsed dye laser once a month for 6 months. Nineteen patients completed the study. Physician Global Assessment (PGA) showed a significantly higher percentage of patients had ≥75% improvement at 6 months in the combined group than the tazarotene monotherapy group (31.6% vs. 5.3%) (90). Tazarotene—Safety Considerations The potential for systemic adverse effects of tazarotene is minimized by the limited transcutaneous absorption of tazarotene, its rapid metabolism into hydrophilic metabolites, and its rapid elimination from the body. Plasma levels of tazarotene and its main metabolite, tazarotenic acid, are very low (91). Skin irritation has been reported in 40%–50% of patients. Due to the irritation potential of this drug, the body surface treated should be less than 10%. Tazarotene is not recommended for mucous membranes, face, and genitalia. Tazarotene has not been approved for children. The absolute contraindications are the same as for oral retinoids. Other rare adverse effects are periungual granulomas, Koebnerization of vitiligo, and genital painful ulcerations (92–94). Bexarotene in Psoriasis Bexarotene is the only RXR-specific retinoid. It has been approved for cutaneous T-cell lymphoma with an oral formulation. Bexarotene gel has been developed later for the same indication (95). Bexarotene 1% gel has been evaluated in a phase II trial for psoriasis. Twenty-four adults with mild to moderate stable plaque psoriasis involving ≤15% total body surface were enrolled. Patients applied bexarotene gel 1%, starting at once every other day and increasing to four times daily as tolerated and if beneficial for up to 24 weeks. The primary efficacy outcome was evaluated by PGA score evaluating the overall response to treatment. At week 24, 63% of patients achieved at least 50% improvement by PGA score and 24% achieved clearing of ≥90%. The treatment was well tolerated (96). Bexarotene with Phototherapy Bexarotene 1% gel twice daily has been used in combination with narrow-band UVB and compared to UVB 311 nm alone. At week 10, the combination therapy was significantly Retinoids in Psoriasis more effective in a left-right comparison in nine patients (97). Bexarotene use is off-label in psoriasis. Bexarotene Safety Considerations The most frequently observed adverse events related to bexarotene were hypertriglyceridemia (56%) and a decrease in free T4 serum levels (54%), which may need correction by appropriate drug therapy. Characteristic retinoid toxicities, such as cheilitis, headache, and myalgias/arthralgias, were mild or absent (60). Contraindications are the same as listed in Table 23.3. Topical Retinoids with Nanostructured Lipid Carriers New developments include the use of nanostructured lipid carriers (NSLCs) for oral drug therapy. NSLC are made up of physiological, biocompatible, biodegradable, non-sensitizing and non-irritating lipids. They are drug delivery systems composed of both solid and liquid lipids as a core matrix. NSLCs enhance the oral bioavailability of the incorporated drug (98). NSLCs have also been designed as topical penetration enhancers (99). In antiaging medicine, these tools are investigated in detail using retinoids (100). ATRA release from NSLC is significantly greater than the drug released from the ATRA suspension (101). Tolerability can be increased. In case of tretinoin-loaded NSLC, the skin irritation was reduced compared to conventional formulations (102). It could be demonstrated that NSLCs offer enhanced photostability, skin transport, and antipsoriatic activity of tretinoin versus the vesicular carriers like liposomes (103). Topical formulations of acitretin using NSLC are under investigation. The investigations ex vivo detected significantly higher deposition of acitretin in human cadaver skin compared to plain gel. Clinical studies demonstrated significant improvement in therapeutic response and reduction in local side effects with acitretin-loaded NSLCs in the topical treatment of psoriasis (104). Conclusions Retinoids are an established part of topical and oral treatment for psoriasis, especially palmoplantar, pustular, and erythrodermic psoriasis—indications that are not yet covered by biologics. Topical tazarotene, oral etretinate, and acitretin are approved for the treatment of psoriasis but other retinoids have also been investigated. Their efficacy can be further improved by combination with PUVA, known as Re-PUVA. Conflicts of Interest U. Wollina and A. Koch have received consultant fees from Abbvie and Novartis. REFERENCES 1. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386:983–994. 2. Conrad C, Gilliet M. Psoriasis: From pathogenesis to targeted therapies. Clin Rev Allergy Immunol. 2018;54:102–113. 141 3. Wollina U, Hein G, Knopf B. Psoriasis und Gelenker­ krankungen. Pathogenese – Klinik – Diagnostik – Therapie. Jena: Gustav Fischer; 1996. 4. Parisi R, Symmons DP, Griffiths CE, Ashcroft DM. Identification and management of psoriasis and associated comorbidity (IMPACT) project team. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J Invest Dermatol. 2013;133:377–385. 5. Han JH, Lee JH, Han KD et al. Epidemiology and medication trends in patients with psoriasis: A nationwide population-based cohort study from Korea. Acta Derm Venereol. 2018;98:396–400. 6. Wei JC, Shi LH, Huang JY et al. Epidemiology and medication pattern change of psoriatic diseases in Taiwan from 2000 to 2013: A nationwide, population-based cohort study. J Rheumatol. 2018;45:385–392. 7. Scotti L, Franchi M, Marchesoni A, Corrao G. Prevalence and incidence of psoriatic arthritis: A systematic review and metaanalysis. Semin Arthritis Rheum. 2018;48:28–34. 8. Zhou X, He Y, Kuang Y et al. Whole exome sequencing in psoriasis patients contributes to studies of acitretin treatment difference. Int J Mol Sci. 2017;18.pii: E295. 9. Adamo S, De Luca LM, Silverman-Jones CS, Yuspa SH. Mode of action of retinol. Involvement in glycosylation reactions of cultured mouse epidermal cells. J Biol Chem. 1979;254:3279–3287. 10. Staquet MJ, Faure MR, Reano A et al. Keratin polypeptide profile in psoriatic epidermis normalized by treatment with etretinate (aromatic retinoid Ro 10-9359). Arch Dermatol Res. 1983;275:124–129. 11. Christophers E, Braun-Falco O. Stimulation der epidermalen DNS-synthese durch vitamin A-Säure. Arch Klin Exp Dermatol. 1968;232:427–433. 12. Kitajima Y, Mori S. Effects of retinoid (Ro 10-9359) on the plasma membrane of keratinocytes in patients with psoriasis: A freezefracture analysis. J Invest Dermatol. 1983;80:174–180. 13. Nagpal S, Thacher SM, Patel S et al. Negative regulation of two hyperproliferative keratinocyte differentiation markers by a retinoic acid receptor-specific retinoid: Insight into the mechanism of retinoid action in psoriasis. Cell Growth Differ. 1996;7:1783–1791. 14. Raynaud F, Gerbaud P, Enjolras O et al. A cAMP binding abnormality in psoriasis. Lancet. 1989;333:1153–1156. 15. Schopf RE, Langendorf Y, Benz RE et al. A highly decreased binding of cyclic adenosine monophosphate to protein kinase A in erythrocyte membranes is specific for active psoriasis. J Invest Dermatol. 2002;119:160–165. 16. Weninger W, Rendl M, Mildner M, Tschachler E. Retinoids downregulate vascular endothelial growth factor/vascular permeability factor production by normal human keratinocytes. J Invest Dermatol. 1998;111:907–911. 17. Haftek M, Faure M, Schmitt D, Thivolet J. Langerhans cells in skin from patients with psoriasis: Quantitative and qualitative study of T6 and HLA-DR antigen-expressing cells and changes with aromatic retinoid administration. J Invest Dermatol. 1983;81:10–14. 18. Pigatto PD, Riva F, Altomare GF et al. Effect of etretinate on chemotaxis of neutrophils from patients with pustular and vulgar psoriasis. J Invest Dermatol. 1983;81:418–419. 19. Pilkington T, Brogden RN. Acitretin: A review of its pharmacology and therapeutic use. Drugs. 1992;43:597–627. 142 20. Lee DD, Stojadinovic O, Krzyzanowska A et al. Retinoidresponsive transcriptional changes in epidermal keratinocytes. J Cell Physiol. 2009;220:427–439. 21. Bono MR, Tejon G, Flores-Santibañez F et al. Retinoic acid as a modulator of T cell immunity. Nutrients. 2016;8:E349. 22. Ott F, Bollag W. [Treatment of psoriasis with an orally administered effective new vitamin A acid derivative. Preliminary report]. Schweiz Med Wochenschr. 1975;105:439–441. 23. Orfanos CE, Runne U. Systemic use of a new retinoid with and without local dithranol treatment in generalized psoriasis. Br J Dermatol. 1976;95:101–103. 24. Goerz G, Orfanos CE. Systemic treatment of psoriasis with a new aromatic retinoid. Preliminary evaluation of a multicenter controlled study in the Federal Republic of Germany. Dermatologica. 1978;157:38–44. 25. Giannetti A, Coppini M, Bertazzoni MG et al. Clinical trial of the efficacy and safety of oral etretinate with c­alcipotriol cream compared with etretinate alone in moderate-severe psoriasis. J Eur Acad Dermatol Venereol. 1999;13:91–95. 26. Green C, Lakshmipathi T, Johnson BE, Ferguson J. A comparison of the efficacy and relapse rates of narrowband UVB (TL-01) monotherapy vs. etretinate (re-TL-01) vs. etretinatePUVA (re-PUVA) in the treatment of psoriasis patients. Br J Dermatol. 1992;127:5–9. 27. Stern RS, Fitzgerald E, Ellis CN et al. The safety of etretinate as long-term therapy for psoriasis: Results of the etretinate follow-up study. J Am Acad Dermatol. 1995;33:44–52. 28. Nast A, Gisondi P, Ormerod AD et al. European S3-Guidelines on the systemic treatment of psoriasis vulgaris—Update 2015--Short version—EDF in cooperation with EADV and IPC. J Eur Acad Dermatol Venereol. 2015;29:2277–2294. 29. Goldfarb MT, Ellis CN, Gupta AK et al. Acitretin improves psoriasis in a dose-dependent fashion. J Am Acad Dermatol. 1988;18:655–662. 30. Kragballe K, Jansén CT, Geiger JM et al. A double-blind comparison of acitretin and etretinate in the treatment of severe psoriasis. Results of a Nordic multicentre study. Acta Derm Venereol. 1989;69:35–40. 31. Caca-Biljanovska NG, V’lckova-Laskoska MT. Management of guttate and generalized psoriasis vulgaris: Prospective randomized study. Croat Med J. 2002;43:707–712. 32. Dogra S, Jain A, Kanwar AJ. Efficacy and safety of acitretin in three fixed doses of 25, 35 and 50 mg in adult patients with severe plaque type psoriasis: A randomized, double blind, parallel group, dose ranging study. J Eur Acad Dermatol Venereol. 2013;27:e305–e311. 33. Olsen EA, Weed WW, Meyer CJ, Cobo LM. A double-blind, placebo-controlled trial of acitretin for the treatment of psoriasis. J Am Acad Dermatol. 1989;21:681–686. 34. Borghi A, Corazza M, Bertoldi AM et al. Low-dose acitretin in treatment of plaque-type psoriasis: Descriptive study of efficacy and safety. Acta Derm Venereol. 2015;95:332–336. 35. Sbidian E, Maza A, Montaudié H et al. Efficacy and safety of oral retinoids in different psoriasis subtypes: A systematic literature review. J Eur Acad Dermatol Venereol. 2011;25:28–33. 36. Ruzicka T, Sommerburg C, Braun-Falco O et al. Efficiency of acitretin in combination with UV-B in the treatment of severe psoriasis. Arch Dermatol. 1990;126:482–486. 37. Tanew A, Guggenbichler A, Hönigsmann H et al. Photoche­ motherapy for severe psoriasis without or in combination with acitretin: A randomized, double-blind comparison study. J Am Acad Dermatol. 1991;25:682–684. Retinoids in Dermatology 38. Lee CS, Li K. A review of acitretin for the treatment of psoriasis. Expert Opin Drug Saf. 2009;8:769–779. 39. Lowenthal KE, Horn PJ, Kalb RE. Concurrent use of methotrexate and acitretin revisited. J Dermatolog Treat. 2008;19:22–26. 40. Lee JH, Youn JI, Kim TY et al. A multicenter, randomized, open-label pilot trial assessing the efficacy and safety of etanercept 50 mg twice weekly followed by etanercept 25 mg twice weekly, the combination of etanercept 25 mg twice weekly and acitretin, and acitretin alone in patients with moderate to severe psoriasis. BMC Dermatol. 2016;16:11. 41. Robinson A, Van Voorhees AS, Hsu S et al. Treatment of ­pustular psoriasis: From the Medical Board of the National Psoriasis Foundation. J Am Acad Dermatol. 2012;67:279–288. 42. Janagond AB, Kanwar AJ, Handa S. Efficacy and safety of systemic methotrexate vs. acitretin in psoriasis patients with ­ significant palmoplantar involvement: A prospective, randomized study. J Eur Acad Dermatol Venereol. 2013;27: e384–e389. 43. Sevrain M, Richard MA, Barnetche T et al. Treatment for palmoplantar pustular psoriasis: Systematic literature review, evidence-based recommendations and expert opinion. J Eur Acad Dermatol Venereol. 2014;28:13–16. 44. Singh RK, Lee KM, Ucmak D et al. Erythrodermic psoriasis: Pathophysiology and current treatment perspectives. Psoriasis (Auckl). 2016;6:93–104. 45. Rosenbach M, Hsu S, Korman NJ et al. Treatment of erythrodermic psoriasis: From the medical board of the ­ National Psoriasis Foundation. J Am Acad Dermatol. 2010;62: 655–662. 46. Tosti A, Ricotti C, Romanelli P et al. Evaluation of the efficacy of acitretin therapy for nail psoriasis. Arch Dermatol. 2009;145:269–271. 47. Sánchez-Regaña M, Sola-Ortigosa J, Alsina-Gibert M et al. Nail psoriasis: A retrospective study on the effectiveness of systemic treatments (classical and biological therapy). J Eur Acad Dermatol Venereol. 2011;25:579–586. 48. Crowley JJ, Weinberg JM, Wu JJ et al. Treatment of nail psoriasis: Best practice recommendations from the Medical Board of the National Psoriasis Foundation. JAMA Dermatol. 2015;151:87–94. 49. Yen YF, Jen IA, Chen M et al. HIV infection increases the risk of incident psoriasis: A nationwide population-based cohort study in Taiwan. J Acquir Immune Defic Syndr. 2017;75:493–499. 50. Menon K, Van Voorhees AS, Bebo BF Jr et al. Psoriasis in patients with HIV infection: From the medical board of the National Psoriasis Foundation. J Am Acad Dermatol. 2010;62:291–299. 51. Krüger-Krasagakes S, Grabbe J, Czarnetzki BM. Possible aggravation of hepatitis A by acitretin. Acta Derm Venereol. 1995;75:82–83. 52. Bonifati C, Lora V, Graceffa D, Nosotti L. Management of psoriasis patients with hepatitis B or hepatitis C virus infection. World J Gastroenterol. 2016;22:6444–6455. 53. Sauder MB, Cheung L, Beecker J. Acitretin-induced hepatitis: When to monitor cholestatic enzymes. J Cutan Med Surg. 2015;19:115–120. 54. Srinivasan A, Syal K, Banerjee D et al. Low plasma l­evels of cholecalciferol and 13-cis-retinoic acid in tuberculosis: Implications in host-based chemotherapy. Nutrition. 2013;29:1245–1251. Retinoids in Psoriasis 55. Wheelwright M, Kim EW, Inkeles MS et al. All-trans retinoic acid-triggered antimicrobial activity against Mycobacterium tuberculosis is dependent on NPC2. J Immunol. 2014;192:2280–2290. 56. Yamada H, Mizuno S, Ross AC, Sugawara I. Retinoic acid therapy attenuates the severity of tuberculosis while altering lymphocyte and macrophage numbers and cytokine expression in rats infected with Mycobacterium tuberculosis. J Nutr. 2007;137:2696–2700. 57. Mortazavi H, Khezri S, Hosseini H et al. A single blind ­randomized clinical study: The efficacy of isotretinoin plus narrow band ultraviolet B in the treatment of psoriasis vulgaris. Photodermatol Photoimmunol Photomed. 2011;27:159–161. 58. Gahalaut P, Soodan PS, Mishra N et al. Clinical efficacy of psoralen + sunlight vs. combination of isotretinoin and psoralen + sunlight for the treatment of chronic plaquetype psoriasis vulgaris: A randomized hospital-based study. Photodermatol Photoimmunol Photomed. 2014;30: 294–301. 59. Wilken R, Sharma A, Patel F, Maverakis E. Successful treatment of palmoplantar pustulosis with isotretinoin. Dermatol Online J. 2015;21:pii:13030/qt4b4776gb. 60. Smit JV, Franssen ME, de Jong EM et al. A phase II multicenter clinical trial of systemic bexarotene in psoriasis. J Am Acad Dermatol. 2004;51:249–256. 61. Irla N, Navarini AA, Yawalkar N. Alitretinoin abrogates innate inflammation in palmoplantar pustular psoriasis. Br J Dermatol. 2012;167:1170–1174. 62. Reich K, Graff O, Mehta N. Oral alitretinoin treatment in patients with palmoplantar pustulosis inadequately responding to standard topical treatment: A randomized phase II study. Br J Dermatol. 2016;174:1277–1281. 63. Karamfilov T, Wollina U. Juvenile generalized pustular psoriasis. Acta Derm Venereol. 1998;78:220. 64. Di Lernia V, Bonamonte D, Lasagni C et al. Effectiveness and safety of acitretin in children with plaque psoriasis: A multicenter retrospective analysis. Pediatr Dermatol. 2016;33:530–535. 65. Charbit L, Mahé E, Phan A et al. Systemic treatments in childhood psoriasis: A French multicentre study on 154 children. Br J Dermatol. 2016;174:1118–1121. 66. Wang Q, Liu W, Zhang L. Clinical features of von Zumbusch type of generalized pustular psoriasis in children: A retrospective study of 26 patients in southwestern China. An Bras Dermatol. 2017;92:319–322. 67. Lau BW, Lim DZ, Capon F et al. Juvenile generalized pustular psoriasis is a chronic recalcitrant disease: An analysis of 27 patients seen in a tertiary hospital in Johor, Malaysia. Int J Dermatol. 2017;56:392–399. 68. Fortina AB, Bardazzi F, Berti S et al. Treatment of severe psoriasis in children: Recommendations of an Italian expert group. Eur J Pediatr. 2017;176:1339–1354. 69. Sarkar R, Chugh S, Gark VK. Acitretin in dermatology. Indian J Dermatol Venereol Leprol. 2013;79:759–771. 70. Kolios AG, Yawalkar N, Anliker M et al. Swiss S1 guidelines on the systemic treatment of psoriasis vulgaris. Dermatology. 2016;232:385–406. 71. Dubertret L. Retinoids, methotrexate and cyclosporine. Curr Probl Dermatol. 2009;38:79–94. 72. Shenoy C, Shenoy MM, Rao GK. Dyslipidemia in dermatological disorders. N Am J Med Sci. 2015;7:421–428. 143 73. Wang D, Liu B, Tao W et al. Fibrates for secondary prevention of cardiovascular disease and stroke. Cochrane Database Syst Rev. 2015;CD009580. 74. Chou R, Dana T, Blazina I et al. Statin Use for the Prevention of Cardiovascular Disease in Adults: A Systematic Review for the U.S. Preventive Services Task Force [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016. 75. Radcliffe JD, Czajka-Narins DM. A comparison of the effectiveness of soy protein isolate and fish oil for reducing the severity of retinoid-induced hypertriglyceridemia. J Nutr Biochem. 2004;15:163–168. 76. Trüeb RM. Therapies for childhood psoriasis. Curr Probl Dermatol. 2009;38:137–159. 77. Iversen L, Lange MM, Bissonette R et al. Topical treatment of psoriasis: Questionnaire results on topical therapy accessibility and influence of body surface area on usage. J Eur Acad Dermatol Venereol. 2017;31:1188–1195. 78. Weinstein GD, Krueger GG, Lowe NJ et al. Tazarotene gel, a new retinoid, for topical therapy of psoriasis: Vehiclecontrolled study of safety, efficacy, and duration of therapeutic effect. J Am Acad Dermatol. 1997;37:85–92. 79. Weinstein GD, Koo JY, Krueger GG et al. Tazarotene cream in the treatment of psoriasis: Two multicenter, doubleblind, randomized, vehicle-controlled studies of the safety and efficacy of tazarotene creams 0.05% and 0.1% applied once daily for 12 weeks. J Am Acad Dermatol. 2003;48:760–767. 80. Lebwohl M, Ast E, Callen JP et al. Once-daily tazarotene gel versus twice-daily fluocinonide cream in the treatment of plaque psoriasis. J Am Acad Dermatol. 1998;38:705–711. 81. Angelo JS, Kar BR, Thomas J. Comparison of clinical efficacy of topical tazarotene 0.1% cream with topical clobetasol propionate 0.05% cream in chronic plaque psoriasis: A double-blind, randomized, right-left comparison study. Indian J Dermatol Venereol Leprol. 2007;73:65. 82. Kumar U, Kaur I, Dogra S et al. Topical tazarotene vs. coal tar in stable plaque psoriasis. Clin Exp Dermatol. 2010;35:482–486. 83. Kaur I, Dogra S, Jain R, Kumar B. Comparative study of calcipotriol (0.005%) ointment and tazarotene (0.05% and 0.1%) gel in the treatment of stable plaque psoriasis. Indian J Dermatol Venereol Leprol. 2008;74:471–474. 84. Tzung TY, Wu JC, Hsu NJ et al. Comparison of tazarotene 0.1% gel plus petrolatum once daily versus calcipotriol 0.05% ointment twice daily in the treatment of plaque psoriasis. Acta Derm Venereol. 2005;85:236–239. 85. Mehta BH, Amladi ST. Evaluation of topical 0.1% tazarotene cream in the treatment of palmoplantar psoriasis: An observerblinded randomized controlled study. Indian J Dermatol. 2011;56:40–43. 86. Samarasekera EJ, Sawyer L, Wonderling D et al. Topical ­therapies for the treatment of plaque psoriasis: Systematic review and network meta-analyses. Br J Dermatol. 2013;168:954–967. 87. Sugarman JL, Gold LS, Lebwohl MG et al. A phase 2, multicenter, double-blind, randomized, vehicle controlled clinical study to assess the safety and efficacy of a halobetasol/tazarotene fixed combination in the treatment of plaque psoriasis. J Drugs Dermatol. 2017;16:197–204. 88. Koo JY, Lowe NJ, Lew-Kaya DA et al. Tazarotene plus UVB phototherapy in the treatment of psoriasis. J Am Acad Dermatol. 2000;43:821–828. 144 89. Fischer-Levancini C, Sánchez-Regaña M, Llambí F et al. Nail psoriasis: Treatment with tazarotene 0.1% hydrophilic ointment. Actas Dermosifiliogr. 2012;103:725–728. 90. Huang YC, Chou CL, Chiang YY. Efficacy of pulsed dye laser plus topical tazarotene versus topical tazarotene alone in ­psoriatic nail disease: A single-blind, intrapatient ­ left-to-right controlled study. Lasers Surg Med. 2013;45:102–107. 91. Marks R. The role of tazarotene in the treatment of psoriasis. Br J Dermatol. 1999;140:24–28. 92. Piraccini BM, Venturi M, Patrizi A. Periungual pyogenic granulomas due to topical tazarotene for nail psoriasis. G Ital Dermatol Venereol. 2014;149:363–366. 93. Narang T, Dogra S, Kumar U et al. Tazarotene-induced irritation causing vitiligo by Koebnerization. J Eur Acad Dermatol Venereol. 2007;21:988–989. 94. Wollina U. Genital ulcers in a psoriasis patient using topical tazarotene. Br J Dermatol. 1998;138:713–714. 95. Pileri A, Delfino C, Grandi V, Pimpinelli N. Role of bexarotene in the treatment of cutaneous T-cell lymphoma: The clinical and immunological sides. Immunotherapy. 2013;5: 427–433. 96. Breneman D, Sheth P, Berger V et al. Phase II clinical trial of bexarotene gel 1% in psoriasis. J Drugs Dermatol. 2007;6:501–506. 97. Magliocco MA, Pandya K, Dombrovskiy V et al. A randomized, double-blind, vehicle-controlled, bilateral ­ comparison trial of bexarotene gel 1% versus vehicle gel in Retinoids in Dermatology 98. 99. 100. 101. 102. 103. 104. combination with narrowband UVB phototherapy for moderate to severe psoriasis vulgaris. J Am Acad Dermatol. 2006;54:115–118. Gaba B, Fazil M, Ali A, Baboota S, Sahni JK, Ali J. Nanostructured lipid (NLCs) carriers as a bioavailability enhancement tool for oral administration. Drug Deliv. 2015;22: 691–700. Baek JS, Pham CV, Myung CS, Cho CW. Tadalafil-loaded nanostructured lipid carriers using permeation enhancers. Int J Pharm. 2015;495:701–709. Morales JO, Valdés K, Morales J, Oyarzun-Ampuero F. Lipid nanoparticles for the topical delivery of retinoids and derivatives. Nanomedicine (Lond). 2015;10:253–269. Charoenputtakhun P, Opanasopit P, Rojanarata T, Ngawhirunpat T. All-trans retinoic acid-loaded lipid nanoparticles as a transdermal drug delivery carrier. Pharm Dev Technol. 2014;19: 164–172. Ghate VM, Lewis SA, Prabhu P et al. Nanostructured lipid carriers for the topical delivery of tretinoin. Eur J Pharm Biopharm. 2016;108:253–261. Raza K, Singh B, Lohan S et al. Nano-lipoidal carriers of tretinoin with enhanced percutaneous absorption, photostability, biocompatibility and anti-psoriatic activity. Int J Pharm. 2013;456:65–72. Agrawal Y, Petkar KC, Sawant KK. Development, evaluation and clinical studies of acitretin loaded nanostructured lipid carriers for topical treatment of psoriasis. Int J Pharm. 2010;401:93–102. 24 Retinoids in Keratinization Disorders Ümit Türsen and Belma Türsen Introduction In keratinization diseases, the deeper and upper portions of the epidermal keratinocytes adhere together by lipid materials. Desquamation, proliferation, or adherent capacity of the cells are abnormal, and the epidermis may thicken or the skin surface may become xerotic and scaly. Keratinization disorders can be localized or generalized, and various treatment modalities, including topical and systemic retinoids, are used to reduce the clinical symptoms. In this chapter, we describe the use of retinoids in disorders of keratinization (1). The Ichthyoses Ichthyosis disorders are characterized by dryness with marked desquamation. Several types of ichthyosis exist (1). Congenital ichthyosis requires lifelong treatment. Current evidence about ichthyosis treatments with oral retinoids including acitretin, isotretinoin and also oral liarozole as retinoic acid metabolism blocking agent is limited. Topical therapies, such as 5% urea, 5% lactic acid, 20% propylene glycol, calcipotriol, and liarozole 5% cream, have demonstrated some therapeutic efficacy in ­ichthyoses (2–19). Ichthyosis Vulgaris Ichthyosis vulgaris is an autosomal dominant disease with a prevalence of about 1/250. Profilaggrin mutations can cause ichthyosis vulgaris. The dryness is usually mild, and symptoms may be few. The scales and dryness occur mostly on the extensor part of the extremities and palmoplantar creases and less frequently on the flexures. Keratosis pilaris is common on arms and legs. The skin manifestations are usually present in early childhood. Lesions can disappear in adult life, particularly during summer. There is no complete cure for ichthyoses. Various topical emollients and keratolytics, including urea, lactic acid, glycolic acid, glycerol, paraffin, propylene glycol, ammonium lactate, salicylic acid, tazarotene, calcipotriol, N-acetyl-cysteine, and a diversity of fatty creams may be useful (5). Systemic retinoids, such as isotretinoin and acitretin, may also be useful, but regularly monitoring for side effects is mandatory. Patients with severe symptoms may require long-term therapy (6). Liarozole is a new retinoic acid metabolism−blocking agent (5,6). It has a better tolerability and is useful for congenital ichthyosis. Liarozole is not commercially available worldwide (Figure 24.1) (7–9). FIGURE 24.1 Ichthyosis vulgaris. Lamellar Ichthyosis and Non-Bullous Ichthyosiform Erythroderma Lamellar ichthyosis shows genetic heterogeneity. The disease usually appears at birth as the collodion baby. It affects both sexes equally, and prevalence of lamellar ichthyosis is less than 1/300,000. Hyperpyrexia and heat intolerance may be a problem in summertime or during exercise. Young children may have increased nutritional requirements due to their rapid growth and desquamation of their skin. Painful palmar and plantar fissures may be seen. Newborns are at risk for hypernatremic dehydration, secondary infection, and sepsis. The disorder persists throughout life. Newborns require care in the neonatal intensive care unit with a high-humidity chamber, moisturizing, and monitoring of routine biochemistry. Frequent skin infections can be worrisome. Applications of petrolatum and keratolytics are recommended. Family members must be educated about preventing the hyperpyrexia and fever. Regular application of water to lesions may simulate sweating and cool the body. Acitretin (0.4–0.8 mg/kg/day) and, as a second alternative, isotretinoin (0.5–1 mg/kg) may be useful treatment options. Isotretinoin 2 mg/kg/day may be helpful for lamellar ichthyosis and epidermolytic hyperkeratosis with maximum clearing and minimum side effects, according to a multicenter study. Improvement was more prominent in patients with lamellar ichthyosis (10,11). 145 146 Patients with severe ectropion may benefit from acitretin (19). An alternative regimen utilizes apremilast, which was used in a patient with severe ectropion. It effectively controlled the ­ichthyosis and minimized relapse of the ocular lesions (18). X-Linked Recessive Ichthyosis This uncommon X-linked recessive disorder occurs only in boys, although girl carriers can have or show mild desquamation. The lifelong condition affects about 1/2000–6000 boys with steroid sulfatase enzyme deficiency. Accumulation of cholesterol sulfate can result in retention hyperkeratosis. Lesions appear in the first year of life. There are larger and darker scales, particularly in flexural regions and to a lesser extent the extensor areas; however, palmoplantar regions are unaffected. Asymptomatic ocular opacities may appear in half of men and some female carriers. In laboratory analysis, cholesterol sulfate levels are increased, with elevated mobility of β-lipoproteins on electrophoresis. Steroid sulfatase enzyme levels are diminished or absent (14,15). Long-term systemic retinoid therapy is usually avoided to prevent serious side effects. Topical therapy is similar to ichthyosis vulgaris. Generally, oral 0.5–1 mg/kg (10–35 mg/day) acitretin is used until marked improvement is achieved (14). Regular laboratory examination and imaging for calcifications and hyperostosis are mandatory in long-term retinoid therapy (8,14,15). Topical tazarotene 0.05% gel can be a useful and well-tolerated treatment agent in X-linked recessive ichthyosis, for which it may be an alternative to systemic retinoid therapy (15). Collodion Baby This is an interpretation and not a specific disease. Lesions are detected at birth as a collodion-like membrane. Collodion membrane can cause ectropion and feeding difficulties. This membrane is shed within a couple of weeks, leaving behind congenital ichthyosis such as non-bullous ichthyosiform erythroderma or lamellar ichthyosis. The principles of treatment include humidification of the skin, prevention of fluid loss, and use of keratolytic agents. Eye care is also required for extraverted palpebrae. Systemic retinoids (0.5–1 mg/kg/day) treatment provides a dramatic benefit in severe forms of ichthyosis including the colloidon baby and congenital ichthyosiform erythroderma. Long-term use of systemic retinoids has been reported to cause toxic effects in bone tissue. Cheilitis, dryness of mucous membranes, mild hair loss, and pruritus are the other adverse effects of oral retinoids. The use of a high humidity incubator can treat temperature instability and high water loss problems. Emollients also limit fluid loss and make the skin supple. The uncommon form, the “Harlequin fetus,” is characterized by fissured hyperkeratosis and serious ectropion. These children die early. High humidity incubators, monitoring of temperature, nutrient and fluid replacement therapies are recommended. To prevent skin and lung infections, antibiotic therapy should be started (14,17). Erythrokeratoderma Variabilis This condition is characterized by annular erythematous and scaly lesions that vary in size, shape, and distribution within Retinoids in Dermatology hours or days. Predilection sites include the facial region, buttocks, arms, and legs. The mucosal regions, scalp, and nails are not involved. General health is good. Disease may recur periodically. The lesions may become less prominent with age. Topical moisturizer ointments and keratolytic agents, such as salicylic acid and alpha-hydroxy acid in petrolatum, topical calcipotriol, and oral retinoids, have been used with favorable results. Topical retinoids including retinoic acid and tazarotene, and oral retinoids such as vitamin A, etretinate, isotretinoin, and acitretin, have been used with good to excellent results. The use of high-dose 1.3 mg/kg/day isotretinoin resulted in flattening of hyperkeratotic plaques. Isotretinoin can also be administered as a low-dose (0.5 mg/kg/day) regimen (20–23). Symmetric Progressive Erythrokeratoderma (Gottron Syndrome) Gottron syndrome is characterized by symmetric, slowly progressive, erythematous, and hyperkeratotic plaques which appear in infancy. Predilection regions include extremities, buttocks, and head. Pruritus may sometimes be present. The lesions may become less prominent after puberty. The disease is inherited as an autosomal dominant trait. Incomplete penetrance and variable expressivity, and sporadic mutations can also be detected. The life span is unaffected. Moisturizers, topical retinoids, topical steroids, calcipotriol, and keratolytic agents, as well as oral retinoids including acitretin and isotretinoin, have been used with positive results. In adolescents, psoralen and ultraviolet A (PUVA) treatment may be effective (24–27). Epidermolytic Hyperkeratosis (Bullous Ichthyosiform Erythroderma) This autosomal dominant disorder is characterized by redness, bullous lesions. and erosions at birth or shortly after birth. The lesions usually become keratotic and verrucous around flexural regions, and erythematous lesions disappear during childhood. Generally, patients do not respond well to topical moisturizing creams or keratolytic therapy (3). The quality of life of these patients is decreased, and they need lifelong therapy. Treatment is symptomatic and antibiotics may be needed if the blisters become infected. Acitretin and isotretinoin may be useful in severe cases by affecting keratin expression. Topical alpha-hydroxy acids, antimicrobial treatment, and systemic retinoids like acitretin can temporarily cause worsening of the lesions; however, dramatic improvement is expected as a result of normalization of epidermal differentiation. Topical retinoids such as tretinoin and tazaroten may be alternative treatments, but patients generally do not respond well to topical retinoids, with high potential for local irritation. There are no reports on serious side effects with short-term systemic retinoids even at higher doses (28–30). Other Ichthyosiform Disorders Ichthyosiform skin lesions can rarely be seen as a part of a syndrome. Refsum syndrome is an autosomal recessive disorder characterized by elevation of phytanic acid, retinal degeneration, peripheral neuropathy, ataxia, and ichthyosis. A multidisciplinary approach 147 Retinoids in Keratinization Disorders for eye and neurologic findings, along with emollients and keratolytic agents for ichthyosis, are needed. A phytanic acid-free diet (phytanic acid consumption ≤10 mg) and plasmapheresis are recommended. Topical therapy, including moisturizing creams, keratolytic agents, and retinoids, should be considered (31,32). Dorfman-Chanarin syndrome is characterized by collodion baby and ichthyosis. Patients must be evaluated for nystagmus and mental retardation. Oral retinoids, skin-softening creams, and keratolyic agents are recommended. A fat-restricted diet is not effective (31,33). Rud syndrome is characterized by ichthyosis, mental retardation, and epilepsy. Dermatologic treatment includes emollients like soft paraffin, keratolytics, topical retinoids, and vitamin D3 analogs (34). Netherton syndrome is characterized by congenital ichthyosis linearis circumflexa, trichorrhexis invaginata, and atopic predisposition. Water and electrolyte management, emollients such as ammonium lactate lotion, topical tacrolimus, topical steroids, topical retinoids, and keratolytic preparations are recommended. Systemic retinoid treatment is controversial because of its risk of activating the atopic skin lesions during therapy; however, most patients can respond to oral retinoids, narrow-band ultraviolet B, and psoralen plus ultraviolet A therapy (35,36). CHILD (congenital hemidysplasia with ichthyosiform erythroderma and limb defects) syndrome is characterized by congenital hemidysplasia, ichthyosis, and defects in the arms and legs. Different inheritance patterns have been reported including X-linked, recessive, and dominant. There is a unilateral or bilateral ichthyosiform erythroderma. Skin lesions are generally persistent, but may sometimes regress spontaneously. Dystrophic nails and alopecia can also be seen. Skeletal defects include hypoplasia or aplasia of bones of the arms and legs on the side of the skin lesions. Spinal ligament calcifications and osteophyte formations can be seen in veretebral and facial bones. Surgical interventions for skeletal defects, moisturizers such as 10% urea cream, retinoids, methotrexate, nonsteroidal anti-­inflammatory drugs, and keratolytics for skin lesions are recommended. Topical 2% cholesterol and 2% lovastatin cream with or without glycolic acid can improve the treatment (37,38). Conradi-Hunermann disease (Conradi-Hunermann-Happle syndrome; X-linked dominant chondrodysplasia punctata) exhibits X-linked dominant inheritance. It is characterized by whorled-like ichthyosis and atrophoderma vermiculatum lesions, especially on the extremities, alopecia, nail changes, skeletal defects such as hypoplasia, scoliosis, and dysplasia, and eye problems such as cataract, microphthalmia, and optic atrophy. There may be a collodion-like presentation. Skeletal and ophthalmic interventions by an orthopedist and an ophthalmologist, moisturizers and skin-softening creams such as ammonium lactate cream, ceramide-enriched emollients, and petrolatum ointment, PUVA or narrow-band UVB therapies, topical corticosteroids, and retinoids are recommended. The results of systemic retinoid therapy such as acitretin and isotretinoin are unclear (39,40). Extracutaneous Ichthyosiform Disorders Other syndromes have been described by various acronyms. IBIDS (trichothiodystrophy) syndrome is characterized by ichthyosis, brittle hair, impaired intelligence, decreased fertility and short stature. In IBIDS syndrome, application of topical moisturizers and sunscreen creams is recommended. Systemic or topical retinoid therapy and topical keratolytic creams are not effective. Orthopedic and physical therapy interventions should be performed for contracture (31,44,45). KID syndrome is characterized by keratitis, ichthyosis, and deafness. Oral retinoids and ultraviolet light give controversial results in KID syndrome, But studies reported that retinoid (recommended dose of acitretin is 0.5–1 mg/kg/day and recommended dose of etretinate is 0.8–1 mg/kg/day) and UV therapies can be successful. Topical keratolytic and moisturizer creams, cochlear implants and hearing devices for deafness, surgical excision of malignant tumors, antibiotics and antifungal therapy for infections, and ophthalmological interventions for keratitis are recommended for KID syndrome (41–43). IFAP (ichthyosis follicularis, alopecia, photophobia) syndrome includes follicular ichthyosiform lesions with alopecia and photophobia. Photoprotection, prevention of pulmonary infections, application of emollients, keratolytics, and physiotherapy are recommended. Topical urea-containing preparations, emollients and keratolytic creams, and retinoid therapy with acitretin are recommended in IFAP syndrome. Ophthalmologic treatment is also necessary (46,47). Acquired Ichthyosis Acquired ichthyosis is an uncommon condition. Underlying diseases such as Hodgkin lymphoma, other lymphomas, sarcoidosis, leprosy, malabsorption, hypothyroidism, and a poor diet should be investigated if ichthyosis appears suddenly in adulthood period. Primary cutaneous peripheral T-cell lymphoma, present as an acquired ichthyosis, has been treated with oral 300 mg/m2/ day bexarotene monotherapy. Ichthyosis-like scales diminished within 2 months after the administration of bexarotene (48). Topical retinoids may also be beneficial. Topical moisturizers and keratolytics such as lactic, glycolic, and pyruvic acids, lipid-rich lubricants, petrolatum, hydrophilic ointments or heavy creams, salicylic acid, urea, and propylene glycol are recommended (49). Keratoderma of the Palms and Soles Inherited Types Palmoplantar keratodermas can be seen in many genodermatoses as a major manifestation. The types of the lesions and pattern of inheritance change from family to family. Diffuse-type palmoplantar keratodermas can present as epidermolytic keratoderma or nonepidermolytic keratoderma. Nonepidermolytic diffuse palmoplantar keratoderma starts at the first year of life. This genodermatosis has an autosomal dominant inheritance pattern and it is characterized by symmetrical and excessive thickening of the palmoplantar areas with a yellowish discoloration. Lesions may spread to the dorsal regions of hand and foot. Epidermolytic diffuse palmoplantar keratodermas have also an autosomal dominant inheritance pattern. It is characterized by very well-defined, excessive, and symmetrical keratoderma with fine fissuring. Pain with manual work and walking can be seen. 148 Retinoids in Dermatology Different clinical types including punctate palmoplantar keratoderma, striate palmoplantar keratoderma, diffuse palmoplantar keratoderma, and mutilating palmoplantar keratoderma and also association with tyrosinemia have been described. Generally, treatment tends to be unsatisfactory and temporary in palmoplantar keratodermas. In some types, podiatric interventions including debridement, topical moisturizers and baths, topical or systemic antifungal and antibacterial therapy for infections, and topical hyperhydrosis treatment as well as surgical intervention for orthopedic problems have been proposed (50–52). Unna-Thost Palmoplantar Keratoderma This is a diffuse nonepidermolytic palmoplantar keratoderma that starts in infancy as diffuse, very thick yellow-waxy palmoplantar keratoderma with an erythematous halo, hyperhidrosis, nail thickening, and dystrophy. Topical keratolytics including lactic acid, salicylic acid, and urea, topical corticosteroids, moisturizers, and retinoids are recommended. Unna-Thost palmoplantar keratoderma is generally resistant to systemic agents, including retinoids, vitamin D, and 5%-­fluoro-uracil. There are some successful reports on low-dose systemic acitretin therapy and carbon dioxide laser therapy for Unna-Thost palmoplantar keratoderma (52,53). Keratoderma Palmoplantaris Transgrediens (Mal de Meleda) In Mal de Meleda, the skin is markedly very well-defined, thickened, and often has an erythematous tint. The hyperkeratosis tends to spread to the dorsal palmoplantar regions in a “gloveand-sock” pattern with maceration and malodor. The condition may be associated with lingua plicata, mental retardation, knuckle pads, syndactyly, palatal defects, nail changes, and perioral redness. Mal de Meleda palmoplantar keratoderma is a gradually and slowly progressive disease. Patients have a normal life span. Oral retinoids including acitretin, 30 mg/daily alitretinoin, keratolytics, and surgical intervention for pseudoainhum are recommended (54,55). Acitretin and isotretinoin therapies may sometimes lead to activation of palmoplantar keratoderma and may result with painful walking, especially in the epidermolytic types. Recommended starting dose of acitretin is 0.2–0.3 mg/kg/day for Mal de Meleda palmoplantar keratoderma (50–52). FIGURE 24.2 Striate keratoderma. topical steroids, topical retinoids, oral retinoids such as lowdose oral acitretin (10 mg/day) or low-dose etretinate, and biotin administration. Other less utilized therapies include PUVA, retinoid-PUVA combination, intravenous 5-fluoro uracil, and reconstructive surgery (56,57). Striate Palmoplantar Keratoderma (Brunauer-Fuchs Disease) This disease is characterized by longitudinal hyperkeratotic lesions on only part of the palms and soles. Keratolitics such as 10% urea cream, salicylic acid ointments, and topical and oral retinoids are recommended (Figure 24.2) (58–60). Tyrosinemia Type II (Richner-Hanhart Syndrome) Tyrosinemia type II is characterized by well-defined and tender hyperkeratotic plaques on the palmoplantar region commonly located on the hypothenar or thenar regions, fingertips, and the weightbearing areas of the soles, resulting in impaired walking. Elbow and knee involvements with the same lesions, hyperhidrosis, leukokeratosis of the tongue, corneal erosions and ulcerations, and mental retardation can be seen. Systemic retinoids such as etretinate or acitretin, and more importantly tyrosine and a ­phenylamine-free diet, are recommended. The dietary ­regimen must be continued for the patient’s entire life. Urgent dietary restrictions may stop or restrict palmoplantar lesions and eye manifestations, but mental deficiency may continue during the lifetime (61,62). Punctate Palmoplantar Keratoderma (Keratosis Palmaris and Plantaris Punctata, Buschke-Fischer-Brauer Disease) Vohwinkel Syndrome (Keratoderma Hereditaria Mutilans) Punctate palmoplantar keratoderma is characterized by an autosomal dominant palmoplantar keratoderma starting during adolescence. The eruption is located symmetrically on the palmoplantar areas as multiple punctuate keratotic lesions with tenderness and pain. Mental deficiency and skeletal deformities such as acro-osteolysis, clubbing, or clinodactyly may be associated. Keratoderma increases gradually up to the third decade and increases during winter time. Therapy includes topical keratolytics such as salicylic acid, urea, topical calcipotriol, This starts in the infancy period. The syndrome has characteristic palmoplantar keratoderma lesions such as a “honeycomb” appearance and also “star-shaped” hyperkeratotic lesions on the dorsal aspects of the palmoplantar areas, elbows, knees and knuckles, constricting fibrous bands of fingers, occasional scarring alopecia, and an “ichthyotic” presentation. Hearing loss, spastic paraplegia, myopathy, and mental retardation can be seen. Constricting fibrous bands of fingers can cause auto-amputation in the early adulthood period. Oral retinoids (0.6–2 mg/kg/day 149 Retinoids in Keratinization Disorders isotretinoin or etretinate) can stop loss of fingers and function deficiency. Topical keratolytic agents and surgical interventions for constricting fibrous bands of fingers are recommended (63–65). Progressive Palmoplantar Keratoderma (Greither Disease, Keratosis Extremitatum) In progressive palmoplantar keratoderma, extensive keratotic lesions with perilesional erythematous borders occur on palmoplantar surfaces and dorsal regions of the soles and palms, also on knees, elbows, and Achilles tendons, with marked hyperhidrosis. Keratolytics and topical and oral retinoids are recommended. The most commonly used retinoids are acitretin and etretinate in doses varying between 0.5 and 1 mg/kg/day. Phototherapy has shown good results (66,67). Olmsted Syndrome Olmsted syndrome is characterized by well-defined bilateral symmetric palmoplantar keratoderma with painful fissures and erythematous halo. Constricting fibrous bands of digits can lead to auto-amputation and finger loss. Periorificial keratotic plaques, alopecia, nail dystrophy, palmoplantar hyperhidrosis, hyperkeratotic linear streaks, keratosis pilaris, joint laxity, osteoporosis, growth deficiency, ocular involvement, leukokeratosis, immunodeficiency, and lung malignancy have been reported. The lesions are bilateral, yellow-brownish, and well-defined. Squamous cell carcinoma can develop on these slowly progressive palmoplantar keratotic lesions. Therapeutic approaches are unsuccessful. Systemic retinoid therapies including acitretin or isotretinoin are ineffective or only temporarily useful. Topical antibiotics or antiseptics, moisturizers and keratolytic agents, pain killers, and radiation treatment can be useful. Surgical interventions such as autografts are unsuccessful (68–70). Papillon-Lefèvre Syndrome (Palmoplantar Keratoderma with Periodontitis, Diffuse Keratoderma with Periodontopathy) This is a diffuse transgrediens palmoplantar erythrokeratoderma characterized by keratotic knee, elbow, and finger lesions with a perilesional erythematous halo. There may be palmoplantar hyperhidrosis with fetid odor. Severe periodontitis and alveolar bone resorption lead to progressive loss of teeth. Growth and mental deficiencies and brain calcifications have been described. Skin manifestations and periodontitis can diminish with oral retinoids such as acitretin, etretinate, isotretinoin, steroids, or methotrexate. Surgical interventions and grafting for keratotic lesions, topical moisturizing agents such as white petrolatum, keratolytic crams such as urea, salicylic acid, wet dressings, boric acid, tar, topical retinoic acid, shale oil, and topical potent steroids have been also recommended. Low-dose acitretin 25 mg/ twice weekly can be effective (71). Huriez Syndrome (Palmoplantar Keratoderma with Sclerodactyly, Sclerotylosis) Scleroatrophy of the hands with sclerodactyly, and mild palmoplantar keratoderma are the main features of this disease. Huriez syndrome is associated with nail dystrophy, palmoplantar hypohidrosis, and atrophy of the dorsal aspects of the palmoplantar area, scleroderma- and poikiloderma-like changes of the nose and lips, and flexion contractures of hands. There is no tooth involvement. The condition usually persists for the lifetime. There is a high risk for development of squamous cell carcinomas, especially on sun-exposed lesions, after the third decade. Therapy includes oral retinoids such as acitretin and isotretinoin, topical keratolytics, and surgical intervention of premalignant lesions (72,73). Keratosis Palmoplantaris Nummularis (Painful Callosities) Symmetric keratotic lesions generally involve the maximum pressure regions of the palmoplantar surfaces. Patients have severe pain at pressure. There may be nail and finger anomalies. The lesions progress slowly, with worsening of both thickness and pain. Treatment is generally unsatisfactory. Oral retinoids, including acitretin and isotretinoin, may be helpful (74,75). Acrokeratoelastiodosis Ackrokeratoelastiodosis is characterized by small, pearly, firm, smooth, warty, asymptomatic papules along the borders of the hands and wrists and along the sides of the fingers, feet, and ankles. The lesions may become confluent. The condition may be associated with palmoplantar keratoderma, hyperpigmentation, and hyperhidrosis. Keratolytics such as salicylic acid and urea, topical corticosteroids, topical calcipotriol, topical retinoids, oral retinoids like acitretin, ionthophoresis, surgical techniques including liquid nitrogen cryotherapy, and erbium:yttriumaluminum-garnet (YAG) laser may be helpful. Oral retinoids provide the best improvement, but relapse following cessation of therapy and the potential adverse effects of the retinoids for an otherwise benign condition do not support their general use. Treatment is required only for cosmetic reasons (76,77). Naxos Syndrome Woolly hair, palmoplantar keratoderma, and cardiac involvement are the main features of this disease. Painful and linear hyperkeratotic lesions especially involve pressure points and interphalangial regions. Naxos syndrome may be associated with skin dryness, acanthosis nigricans, palmoplantar hyperhidrosis, and follicular hyperkeratosis. Cardiologic treatments and follow-up for rightside cardiac defects, systemic retinoid therapy including acitretin or isotretinoin for keratoderma, and topical keratolytic and moisturizer agents for skin manifestations are recommended (78,79). Acquired Types of Keratoderma Some commonly acquired palmoplantar keratoderma cases occurring late in life in association with internal malignancy include esophageal carcinoma (tylosis), arsenic intoxication, menopause (climacteric palmoplantar keratoderma), and also some inflammatory skin diseases like lichen planus and psoriasis. Punctate or linear palmoplantar keratoderma lesions on palmar creases are quite common as a late development in healthy black patients. 150 Retinoids in Dermatology Regular paring and the use of keratolytic ointments are often more helpful than attempts for hormone replacement, and the condition tends to settle over a few years. Topical treatments such as moisturizers, keratolytics such as 10% urea cream, salicylic acid, and lactic acid, topical retinoids, regular surgical debridement of keratotic lesions, topical corticosteroids, topical selenium sulfide, PUVA, and also acitretin or etretinate in low doses have been recommended (80,81). Knuckle Pads Knuckle pads can be sporadic and rarely familial. Trauma is not an etiologic factor. The condition is characterized by keratotic and fibrotic lesions on the dorsal aspect of the fingers after the late-childhood period. Dupuytren contracture can occur rarely. Treatment is unsatisfactory, but surgery, topical steroids, salicylic acid gel, retinoids, carbon dioxide freezing, intralesional steroid, and 5-fluorouracil injections are recommended (82,83). Callosities and Corns Callus is characterized by thickening of the keratin layer, and it is a protective response to regular trauma. There is also an occupational callus variant. Corns include a central hyperkeratotic area with pain. They appear in the pressure areas, including dorsal joints and prominent bones like metatarsals. “Soft corns” occur in the third or fourth finger clefts on the feet, and they are often macerated. Elimination of the pressure, appropriate shoes, debridement of corns, and sometimes orthopedic interventions are essential treatments. Medical treatment includes silver nitrate, phenol, potassium hydroxide, and callus bands with salicylic acid. Excision, curettage, cryotherapy, erbium-doped yttrium aluminum garnet laser, cantharidin, topical retinoic acid, and if necessary, osteotomies are recommended (84–86). Other Disorders of Keratinization Keratosis Pilaris This autosomal dominant disease is characterized by keratinization of hair follicles, with horny plugs on the extensor surfaces of the proximal parts of extremities. Keratosis pilaris frequently occurs in association with the autosomal dominant ichthyosis vulgaris. Generally, therapy is not necessary. Topical keratolytic agents such as salicylic acid or 10% urea-containing preparations, topical corticosteroids, and topical retinoids can treat the lesions temporarily (87,88). Darier Disease (Keratosis Follicularis) This dominantly inherited disease is characterized by symmetrically distributed firm, red-brown papules and plaques with greasy, crusted, and warty surfaces. It occurs in seborrheic areas including presternal, interscapular regions and behind the ears. The nails may be affected; longitudinal ridges, subungual hyperkeratosis, and V-shaped notches can be seen. Patients with Darier disease usually have punctate keratotic lesions or pits on the palmoplantar regions, psychosocial disturbances, mucosal FIGURE 24.3 Darier disease. manifestations, and also a partial immunodeficiency condition with an increased predisposition for generalized bacterial and viral infections. Sunblock creams are recommended to prevent sunlightrelated exacerbations. Avoiding physical trauma, use of cyclosporine, systemic and topical steroids or vitamin D3 ointment, systemic and topical antibiotic or antifungal therapy to suppress bacterial and fungal infections, topical vitamin A derivatives including tazarotene, isotretinoin, and adapalene or systemic retinoids such as isotretinoin, acitretin, or alitretinoin are also recommended. Alitretinoin should be considered in young women with severe or extensive Darier disease which may be recalcitrant to isotretinoin or other therapies as pan-agonist retinoid. All treatments may be modified according to exacerbations of Darier disease. Severe and complicated patients can be successfully treated by long-term low-dose systemic retinoids like acitretin. Only topical and anti-infective treatments are recommended for patients with localized lesions. For refractory proliferative lesions, botulinum toxin injections, surgical dissection using an yttrium–aluminum–garnet laser are sometimes performed (Figure 24.3) (89,90). Acanthosis Nigricans Acanthosis nigricans (AN) is characterized by hyperkeratosis and hyperpigmentation of the flexural regions of the body such as the antecubital fossa, umblicus, and anogenital and axillary regions. Etiology and pathogenesis depend on underlying disorders. There is usually a subtle onset, as increasing of hyperpigmentation. In every type of AN, there is darkening of pigmentation and the skin appears dirty and velvety; skin lines become accentuated and the surface rugose and papillomatous. Acanthosis nigricans includes five types: malignant AN (type 1), AN related to genetic syndromes (familial; type 2), AN related to obesity (type 3), unilateral nevoid (type 4) AN, and AN induced by drugs (type 5). In type 3 AN, there may be velvety patches on the inner aspect of the legs, along with many acrochordons in the flexural regions of the body. Keratotic and pigmentary changes are more marked in type 5 AN. Palmoplantar hyperkeratosis can cause a “tripe hands” view. Hyperkeratosis and 151 Retinoids in Keratinization Disorders TABLE 24.1 Retinoid Responsive Keratinization Disorders Keratinization Disorders Systemic Retinoids Topical Peeling Agents A. The ichthyoses 1. Ichthyosis vulgaris 2. Lamellar ichthyosis 3. Non-bullous ichthyosiform erythroderma 4. X-linked recessive ichthyosis 5. Collodion baby 6. Erythrokeratoderma variabilis 7. Symmetric progressive erythrokeratoderma (Gottron syndrome) 8. Epidermolytic hyperkeratosis (bullous ichthyosiform erythroderma) 0.5–1 mg/kg/d isotretinoin, 0.4–0.8 mg/ kg/d acitretin, 0.1 g/day liarozole 2%–10% urea, topical isotretinoin, 20% propylene glycol, tazarotene, 0.05% lactic acid, glycolic acid, glycerol, paraffin, propylene glycol (44%–60% in water), ammonium lactate, salicylic acid (6%) B. Other ichthyosiform syndromes 1. Refsum syndrome 2. Dorfman-Chanarin syndrome 3. Rud syndrome 4. Netherton syndrome 5. CHILD syndrome 6. Conradi-Hunermann disease (Conradi-Hunermann-Happle syndrome; X-linked dominant chondrodysplasia punctata) 7. KID syndrome 8. IBIDS syndrome (trichothiodystrophy) 0.2–1 mg/kg/d isotretinoin, 0.4–0.8 mg/ kg/d acitretin, 0.1 g/day liarozole 2%–10% urea, 20% propylene glycol, tazarotene, 0.05% lactic acid, glycolic acid, glycerol, paraffin, propylene glycol (44%–60% in water), ammonium lactate, salicylic acid (6%), topical 2% cholesterol, 2% lovastatin cream, ceramide-enriched emollients C. Acquired ichthyosis 300 mg/m2/day bexarotene Topical isotretinoin, humectants including lactic, glycolic, and pyruvic acids, lipid-rich lubricants, including petrolatum, hydrophilic ointment, or heavy creams, keratolytic agents including salicylic acid, urea, propylene glycol D. Inherited palmoplantar keratodermas 1. Unna-Thost palmoplantar keratoderma 2. Keratoderma palmoplantaris transgrediens (Mal de Meleda) 3. Punctate palmoplantar keratoderma (keratosis palmaris and plantaris punctata, Buschke-Fischer-Brauer disease) 4. Striate palmoplantar keratoderma (Brunauer-Fuchs disease) 5. Tyrosinemia type II (Richner-Hanhart syndrome) 6. Vohwinkel syndrome (keratoderma hereditaria mutilans) 7. Progressive palmoplantar keratoderma (Greither disease, keratosis extremitatum) 8. Olmsted syndrome 9. Papillon-Lefèvre syndrome (palmoplantar keratoderma with periodontitis, diffuse keratoderma with periodontopathy) 10. Huriez syndrome (palmoplantar keratoderma with sclerodactyly, sclerotylosis) 11. Keratosis palmoplantaris nummularis (painful callosities) 12. Acrokeratoelastiodosis 13. Naxos syndrome Lower doses of acitretin (10–25 mg/day; 0.2–0.3 mg/kg/d) and isotretinoin (5–30 mg/kg/d), 30 mg/daily alitretinoin Topical petrolatum, keratolytics such as urea, salicylic acid, wet dressing, boric acid, tar, topical retinoic acid, shale oil, topical corticosteroids E. Acquired palmoplantar keratodermas 1. Keratoderma climactericum, paraneoplastic 2. Arsenic-related 3. Knuckle pads 4. Callosities and corns Acitretin or etretinat in low doses (0.1–0.3 mg/kg/d) Topical keratolytics (urea, salicylic acid, and lactic acid), topical retinoids, topical corticosteroids, topical selenium sulfide, phototherapy (using topical psoralen and ultraviolet A phototherapy) F. Other disorders of keratinization 1. Keratosis pilaris, Darier disease (keratosis follicularis) 2. Akanthosis nigricans 3. Pityriasis rubra pilaris 4. Disseminated superficial actinic porokeratosis 5. Kyrle disease (hyperkeratosis follicularis et parafollicularis in cutem penetrans) Isotretinoin and acitretin (25 mg/day), high-dose vitamin A (100,000 U/daily) Topical keratolytic agents, such as salicylic acid, urea and tretinoin (1–100) 152 hyperpigmentation of mucocutaneous junctions such as perioral and periorbital areas can occur. Treatment is symptomatic. Topical keratolytic agents, such as lactic acid, 5%−10% urea creams, 2%−10% salicylic acid ointments, and 15% trichloroacetic acid peels and/or topical retinoids including adapalene gel and tretinoin or systemic retinoids, topical calcipotriol, fish oil, 20% podophyllin, topical colecalciferol, Kligman’s triple combination formula creams (topical retinoid, topical hydroquinone, and topical steroid) with sunblock creams may diminish acanthosis nigricans (91,92). Grover Disease This is an uncommon, acute papulovesicular eruption of the trunk, accompanied by pruritus, which occurs mainly in middle-aged men accompanied with many inflammatory and neoplastic conditions. Although usually transient, there is a persistent form. Topical corticosteroids, topical vitamin D3 derivatives like calcipotriol, topical zinc oxide cream, emollients, moisturizing agents, or antihistamines are used for topical treatment. Oral steroids, methotrexate, photochemotherapy, and dapsone have been proposed as systemic therapy if topical treatments fail. Isotretinoin, acitretin, and etanercept have been used in refractory cases (93–95). Pityriasis Rubra Pilaris Pityriasis rubra pilaris (PRP) is an uncommon erythematosquamous disorder characterized by scaling, perifollicular redness, and follicular plugging, which may evolve into erythroderma. Follicular hyperkeratotic papules, reddish-orange squamous lesions progressing to generalized erythroderma, and sharply demarcated islands of unaffected skin are typical clinical features. Palmoplantar keratoderma and nail abnormalities have been seen (96). Topical therapies consist of emollients, keratolytic agents, vitamin D3 analogs like calcipotriol, corticosteroids, and vitamin A analogs like tazarotene and isotretinoin. Treatment with systemic agents include etretinate, acitretin, alitretinoin, penicillin, cyclosporin, mycophenolate mofetil, fumaric acid esters, apremilast, intravenous immunoglobulins, and methotrexate. Retinoids (isotretinoin, alitretinoin) have been used with a mean dosage of 0.42–1.55 mg/kg/day. Phototherapy and photochemotherapy, and other retinoids like RO 10–9359, may be successful in some patients. Systemic methotrexate or retinoid therapies are more successful agents. In type 6 PRP, highly active antiretroviral therapy (HAART) is recommended. The anti-TNF agents, such as infliximab, adalimumab, etanercept, and also ustekinumab, secukinumab, alefacept, and p55 receptor immunoadhesion, are effective (95–96). Different systemic agents and/or phototherapy (96,97) can be used together. Disseminated Superficial Actinic Porokeratosis Disseminated superficial actinic porokeratosis is characterized by bilateral atrophic lesions with a raised keratotic margin, occurring particularly on the extensor surfaces of limbs including hands or feet. Generally, the condition spares the palms, soles, and mucous membranes. Characteristic features include xerotic lesions with a central atrophic zone surrounded by a Retinoids in Dermatology well-demarcated hyperkeratotic border. The disease is dominantly inherited in most patients, but sporadic variants do occur. There is a slightly increased risk of malignant skin cancers. Therapy includes topical sunscreens, topical diclofenac, topical 5-fluorouracil, topical steroids, cryotherapy, CO2, Q-switched ruby, neodymium:yttrium-aluminum-garnet (Yag), Er-Yag, pulsed dye, fractional photothermolysis lasers, intensed pulsed light and Grenz ray, photodynamic therapy, vitamin D analogs (tacalcitol, calcipotriol), keratolytics, topical tacrolimus, cantharidin plaster, dermabrasion, topical ingenol mebutate, and imiquimod. Topical and oral retinoids are the first choice of treatment. Relapse is common. Patients should be monitored for skin cancers (98,99). Kyrle Disease (Hyperkeratosis Follicularis et Parafollicularis in Cutem Penetrans) Kyrle disease is characterized by follicular or extrafollicular erythematous papules with central horny plugging particularly located on the extensor legs and forearms. However, there are no lesions on the mucosal or palmoplantar regions. Kyrle disease is chronic and persistent. It has an autosomal dominant inheritance, but there are many sporadic cases. Kyrle disease can respond to topical keratolytic agents, such as salicylic acid, urea, and tretinoin, oral retinoids such as isotretinoin, acitretin (25 mg/day), and high-dose vitamin A, and electrocautery, cryotherapy, and CO2 laser treatments. Emollients, oral clindamycin, combination of oral retinoids and PUVA, surgical curetting, and antihistamines may be helpful (16,100). Conclusions Synthetic retinoids, including isotretinoin and acitretin and topical retinoids such as tazaroten and isotretinoin have been used in the treatment of a variety of keratinization disorders such as ichthyosis and palmoplantar keratoderma (Table 24.1). Relapse following cessation of therapy and the possible side effects of the retinoids for an otherwise benign condition do not support their general use. Topical treatments must be used regularly in keratinization disorders. Low-dose retinoid therapy is recommended as maintenance. Regular biochemistry analysis, strict contraception, and skeletal examination are needed for the safe and successful usage of these drugs. REFERENCES 1. Smack DP, Korge BP, James WD. Keratin and keratinization. J Am Acad Dermatol. 1994;30:85–102. 2. Happle R, van de Kerkhof PC, Traupe H. Retinoids in disorders of keratinization: Their use in adults. Dermatologica. 1987;175:107–124. 3. Hernández-Martin A, Aranegui B, Martin-Santiago A, Garcia-Doval I. A systematic review of clinical trials of ­treatments for the congenital ichthyoses, excluding ichthyosis vulgaris. J Am Acad Dermatol. 2013;69:544–549. 4. Vahlquist A, Ganemo A, Virtanen M. Congenital ichthyosis: An overview of current and emerging therapies. Acta Derm Venereol. 2008;88:4–14. 153 Retinoids in Keratinization Disorders 5. Blanchet-Bardon C, Tadini G, Machado Matos M, Delarue A. Association of glycerol and paraffin in the treatment of ichthyosis in children: An international, multicentric, randomized, controlled, double-blind study. J Eur Acad Dermatol Venereol. 2012;26:1014–1019. 6. Oji V, Tadini G, Akiyama M, Blanchet Bardon C, Bodemer C, Bourrat E et al. Revised nomenclature and classification of inherited ichthyosis: Results of the first ichthyosis consensus conference in Soreze 2009. J Am Acad Dermatol. 2010;63:607–641. 7. Baden HP, Buxman MM, Weinstein GD, Yoder FW. Treatment of ichthyosis with isotretinoin. J Am Acad Dermatol. 1982;6:716–720. 8. Van Wauwe J, Van Nyen G, Coene MC, Stoppie P, Cools W, Goossens J et al. Liarazole, an inhibitor of retinoic acid metabolism, exerts retinoid-mimetic effects in vivo. J Pharmacol Exp Ther. 1992;261:773–779. 9. Lucker GP, Verfaille CJ, Heremans AM, Vanhoutte FP, Boegheim JP, Steijlen PP. Topical liarazole in ichthyosis: A double-blind, left-right comparative study followed by a longterm open maintenance study. Br J Dermatol. 2005;3:566–569. 10. Ganemo A, Virtanen M, Vahlquist A. Improved topical treatment of lamellar ichthyosis: A double-blind study of four different cream formulations. Br J Dermatol. 1999;6:1027–1032. 11. Vahlquist A, Traupe H, Blockhuys S, Shroot B. Liarazole effective in treatment of lamellar ichthyosis. J Invest Dermatol. 2008;128:60. 12. Frenk E. Oral treatment of lamellar ichthyosis (non-bullous congenital ichthyosiform erythroderma) with an aromatic retinoid. Dermatologica. 1981;162:91–103. 13. Fernandes NF, Janniger CK, Schwartz RA. X-linked ichthyosis: An oculocutaneous genodermatosis. J Am Acad Dermatol. 2010;62:480–485. 14. Bruckner-Tuderman L, Sigg C, Geiger JM, Gilardi S. Acitretin in the symptomatic therapy for severe recessive x-linked ­ichthyosis. Arch Dermatol. 1988;124:529–532. 15. Hofmann B, Stege H, Ruzicka T, Lehmann P. Effect of topical tazarotene in the treatment of congenital ichthyoses. Br J Dermatol. 1999;141:642–646. 16. Verma R, Vasudevan B, Kakkar S, Mishra P, Pragasam V, Dabbas D. Kyrle’s disease presenting in an extensive distribution along lines of Blaschko. Indian J Dermatol. 2015;60:423. 17. Özyurt BM, Onay ÖS, Ersoy Ö. Collodion baby case series: The success of oral retinoic acid. Turk Pediatri Ars. 2018;1:51–56. 18. Abboud JJ, Whittington A, Ahmed M, Himebaugh JT, Wiley LA, Haffar A, Nguyen J. Apremilast use in a case of cicatricial ectropion secondary to severe lamellar ichthyosis. Ophthalmic Plast Reconstr Surg. 2018;34:76–77. 19. Singh M, Kaur M, Kaur R, Singh S. Severe ectropion in lamellar ichthyosis managed medically with oral acitretin. Pediatr Dermatol. 2018;35:117–120. 20. Singh N, Thappa DM. Erythrokeratoderma variabilis responding to low-dose isotretinoin. Pediatr Dermatol. 2010;27:111–113. 21. Rappaport IP, Goldes JA, Goltz RW. Erythrokeratodermia variabilis treated with isotretinoin: A clinical, histologic and ultrastructural study. Arch Dermatol. 1986;122:441–445. 22. Tarikci N, Göncü EK, Yüksel T, Singer R, Topal İO, Şahin İM. Progressive symmetrical erythrokeratoderma on the face: 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. A rare condition and successful treatment with calcipotriol. JAAD Case Rep. 2016;2:70–71. Yoo S, Simzar S, Han K, Takahashi S, Cotliar R. Erythrokeratoderma variabilis successfully treated with ­topical tazarotene. Pediatr Dermatol. 2006;23:382–385. Asha GS, Lakshmi DV, Shilpa K, Divya GK. Late onset progressive symmetric erythrokeratoderma with pseudo ainhum. Indian J Dermatol. 2016;61:448–450. Wu F, Chen J, Li ZH, Hu ZL, Deng L, Sang H. Progressive symmetric erythrokeratoderma with dermatophytosis. Indian J Dermatol Venereol Leprol. 2014;80:345–347. Boyden LM, Vincent NG, Zhou J, Hu R, Craiglow BG, Bayliss SJ et al. Mutations in KDSR cause recessive progressive symmetric erythrokeratoderma. Am J Hum Genet. 2017;100:978–984. Shah K, Ansar M, Mughal ZU, Khan FS, Ahmad W, Ferrara TM, Spritz RA. Recessive progressive symmetric erythrokeratoderma results from a homozygous loss-of-function mutation of KRT83 and is allelic with dominant monilethrix. J Med Genet. 2017;54:186–189. Nassif PW, Nakandakari S, Fogagnolo L, Contin LA, Alves CJ. Epidermolytic hyperkeratosis: A follow-up of 23 years of use of systemic retinoids. An Bras Dermatol. 2011;86:72–75. Li H, Törmä H. Retinoids reduce formation of keratin aggregates in heat-stressed immortalized keratinocytes from an epidermolytic ichthyosis patient with a KRT10 mutation. Acta Derm Venereol. 2013;93:44–49. Kwak J, Maverakis E. Epidermolytic hyperkeratosis. Dermatol Online J. 2006;12:6. Yoneda K. Inherited ichthyosis: Syndromic forms. J Dermatol. 2016;43:252–263. Sá MJ, Rocha JC, Almeida MF, Carmona C, Martins E, Miranda V et al. Infantile refsum disease: Influence of dietary treatment on plasma phytanic acid levels. JIMD Rep. 2016;26:53–60. Waheed N, Cheema HA, Suleman H, Mushtaq I, Fayyaz Z. Chanarin-dorfman syndrome. J Coll Physicians Surg Pak. 2016;26:787–789. Rodríguez Sánchez MD, Corral Caramés MJ, Rodríguez Arnao MD, Lorenzo Navarro L, Mancheño Rico E, Pérez Sotelo M. Ichthyosis, epileptic crises and infantilism: 4 cases of Rud syndrome. An Esp Pediatr. 1986;25:201–203. Maatouk I, Moutran R, Tomb R. Narrowband ultraviolet B phototherapy associated with improvement in Netherton ­syndrome. Clin Exp Dermatol. 2012;37:364–366. Ng E, Hale CS, Meehan SA, Cohen DE. Netherton syndrome with ichthyosis linearis circumflexa and trichorrhexis invaginatum. Dermatol Online J. 2014;20:12. Bergqvist C, Abdallah B, Hasbani DJ, Abbas O, Kibbi AG, Hamie L, Kurban M, Rubeiz N. CHILD syndrome: A modified pathogenesis-targeted therapeutic approach. Am J Med Genet A. 2018;176:733–738. König A, Happle R, Bornholdt D. Mutations in the NSDHL gene, encoding a 3β-hydroxysteroid dehydrogenase, cause CHILD syndrome. Am J Med Genet. 2000;90:339–346. Happle R. X-linked dominant chondrodysplasia punctata. Review of literature and report of a case. Hum Genet. 1979;53:65–73. Hartman RD, Molho-Pessach V, Schaffer JV. ConradiHünermann-Happle syndrome. Dermatol Online J. 2010;16:4. 154 41. Wolfe CM, Davis A, Shaath TS, Cohen GF. Visual impairment reversal with oral acitretin therapy in keratitis-ichthyosisdeafness (KID) syndrome. JAAD Case Rep. 2017;3:556–558. 42. Salman A, Gencosmanoglu DS, Yucelten AD, Elcioglu N, Richard G, Demirkesen C. Successful treatment of pityriasis lichenoides chronica with narrow-band ultraviolet B therapy in a patient with keratitis-ichthyosis-deafness syndrome: A case report. Dermatol Online J. 2016;22:5. 43. Patel V, Sun G, Dickman M, Khuu P, Teng JM. Treatment of keratitis-ichthyosis-deafness (KID) syndrome in children: A case report and review of the literature. Dermatol Ther. 2015;28:89–93. 44. Rebora A, Crovato F. PIBI (D) S syndrome-trichothiodystrophy with xeroderma pigmentosum (group D) mutation. J Am Acad Dermatol. 1987;16:940–947. 45. Lambert WC, Gagna CE, Lambert MW. Trichothiodystrophy: Photosensitive, TTD-P, TTD, Tay syndrome. Adv Exp Med Biol. 2010;685:106–110. 46. Mégarbané H, Mégarbané A. Ichthyosis follicularis, alopecia, and photophobia (IFAP) syndrome. Orphanet J Rare Dis. 2011;6:29. 47. Nagakeerthana S, Rangaraj M, Karthikeyan K. Ichthyosis follicularis, alopecia, and photophobia syndrome. Int J Trichology. 2017;9:67–69. 48. Tanita K, Fujimura T, Sato Y, Hidaka T, Furudate S, Kambayashi Y, Tsukada A, Hashimoto A, Aiba S. Successful treatment of primary cutaneous peripheral T-cell lymphoma presenting acquired ichthyosis with oral Bexarotene monotherapy. Case Rep Oncol. 2017;10:328–332. 49. Patel N, Spencer LA, English JC 3rd, Zirwas MJ. Acquired ichthyosis. J Am Acad Dermatol. 2006;55:647–656. 50. Sehgal VN, Kumar S, Narayan S. Hereditary palmoplantar keratoderma (four cases in three generations). Int J Dermatol. 2001;40:130–132. 51. Has C, Technau-Hafsi K. Palmoplantar keratodermas: Clinical and genetic aspects. J Dtsch Dermatol Ges. 2016;14:123–139. 52. O’Connor EA, Dzwierzynski WW. Palmoplantar keratoderma: Treatment with CO2 laser case report and review of the literature. Ann Plast Surg. 2011;67:439–444. 53. Itin PH, Fistarol SK. Palmoplantar keratodermas. Clin Dermatol. 2005;23:15–22. 54. Lestringant GG, Hadi SM, Qayed KI, Blayney BJ. Mal de Meleda: Recessive transgressive palmoplantar keratoderma with three unusual facultative features. Dermatology. 1992;184:78–82. 55. Park HK, Kim EJ, Ko JY. Alitretinoin: Treatment for refractory palmoplantar keratoderma. Br J Dermatol. 2016;174:1143–1144. 56. Jo JW, Jeong DS, Kim CY. Case of punctate palmoplantar keratoderma type I treated with combination of low-dose oral acitretin and topical salicylic acid and steroid. J Dermatol. 2018;45:609–612. 57. Asemota E, Markova A, Ho J, Lichtman MK. Disseminated punctate keratoderma: A rare case report and review of the literature. Dermatol Online J. 2017;23:3. 58. Bragg J, Rizzo C, Mengden S. Striate palmoplantar keratoderma (Brunauer-Fohs-Siemens syndrome). Dermatol Online J. 2008;14:26. 59. Tursen U, Ustunsoy D, Api H, Polat A, Ikizoglu G. Concordance of striate palmoplantar keratoderma and brachyphalangia in monozygous twins. J Eur Acad Dermatol Venereol. 2006;20:1343–1345. Retinoids in Dermatology 60. White KL. Striate palmoplantar keratoderma. Dermatol Online J. 2002;8:16. 61. Fraser NG, MacDonald J, Griffiths WA, McPhie JL. Tyrosinaemia type II (Richner-Hanhart syndrome)-report of two cases treated with etretinate. Clin Exp Dermatol. 1987;12:440–443. 62. Locatelli F, Puzenat E, Arnoux JB, Blanc D, Aubin F. Richner-Hanhart syndrome (tyrosinemia type II). Cutis. 2017;100:20–22. 63. Goldfarb MT, Woo TY, Rasmussen JE. Keratoderma hereditaria mutilans (Vohwinkel’s syndrome): A trial of isotretinoin. Pediatr Dermatol. 1985;2:216–218. 64. Camisa C, Rossana C. Variant of keratoderma hereditaria mutilans (Vohwinkel’s syndrome). Treatment with orally administered isotretinoin. Arch Dermatol. 1984;120:1323–1328. 65. Wereide K. Mutilating palmoplantar keratoderma successfully treated with etretinate. Acta Derm Venereol. 1984;64:566–569. 66. Guaraldi Bde M, Jaime TJ, Guaraldi Rde M, Melo DF, Nogueira OM, Rodrigues N. Progressive symmetrical erythrokeratodermia – case report. An Bras Dermatol. 2013;88:109–112. 67. Ott H, Lehmann S, Poblete-Gutiérrez P, Frank J. Progressive symmetric erythrokeratodermia of Darier-Gottron. Hautarzt. 2004;55:994–996. 68. Armstrong AP, Percival N. Olmsted’s syndrome. J R Soc Med. 1997;90:81–82. 69. Nishina K, Mikawa K, Maekawa N, Yaku H, Obara H. Anesthetic management of a child with Olmsted’s syndrome. J Anesth. 1994;8:101–103. 70. Duchatelet S, Hovnanian A. Olmsted syndrome: Clinical, molecular and therapeutic aspects. Orphanet J Rare Dis. 2015;10:33. 71. Sarma N, Ghosh C, Kar S, Bazmi BA. Low-dose acitretin in Papillon-Lefèvre syndrome: Treatment and 1-year follow-up. Dermatol Ther. 2015;28:28–31. 72. Riggio E, Spano A, Bonomi S, Nava M. Huriez syndrome: Association with squamous cell carcinoma and a surgical approach. Plast Reconstr Surg. 2005;116:689–691. 73. Surana T, Padhiar B, Karia U, Pandya P. Huriez syndrome with superadded dermatophyte infection. Indian Dermatol Online J. 2016;7:288–289. 74. Wachters DH, Frensdorf EL, Hausman R, van Dijk E. Keratosis palmoplantaris nummularis (“hereditary painful callosities”). Clinical and histopathologic aspects. J Am Acad Dermatol. 1983;9:204–209. 75. Nogita T, Furue M, Nakagawa H, Ishibashi Y. Keratosis palmoplantaris nummularis. J Am Acad Dermatol. 1991;25:113–114. 76. Xu CC, Fu LY, Lin D, Li H, Du WH, Wang PG. A case of acrokeratoelastoidosis. Clin Exp Dermatol. 2018;43:819–820. 77. Shiiya C, Hata H, Inamura Y, Imafuku K, Kitamura S, Yanagi T, Fujita Y, Shimizu H. Acrokeratoelastoidosis successfully treated with 10% salicylic acid ointment. J Dermatol. 2017;44:46–47. 78. Protonotarios N, Tsatsopoulou A, Fontaine G. Naxos disease: Keratoderma, scalp modifications, and cardiomyopathy. J Am Acad Dermatol. 2001;44:309–311. 79. Islam AM, Rahman MT, Chowdhury AH. Cardiocutaneous syndrome (Naxos disease) in a Bangladeshi boy. Cardiovasc Diagn Ther. 2016;6:462–465. 80. Cohen PR, Anderson CA. Topical selenium sulfide for the treatment of hyperkeratosis. Dermatol Ther (Heidelb). 2018;8:639–646. Retinoids in Keratinization Disorders 81. Patel S, Zirwas M, English JC 3rd. Acquired palmoplantar keratoderma. Am J Clin Dermatol. 2007;8:1–11. 82. Hyman CH, Cohen PR. Report of a family with idiopathic knuckle pads and review of idiopathic and disease-associated knuckle pads. Dermatol Online J. 2013;19:18177. 83. Knobloch K. Knuckle pads and therapeutic options. MMW Fortschr Med. 2012;154:41–2. 84. Balevi A, Engin Uysal S, Doga Ustuner P, Ozdemir M. How I do it: Treatment of plantar calluses and corns with an erbium-doped yttrium aluminum garnet laser. Dermatol Surg. 2016;42:1304–1307. 85. Akdemir O, Bilkay U, Tiftikcioglu YO, Ozek C, Yan H, Zhang F, Akin Y. New alternative in treatment of callus. J Dermatol. 2011;38:146–150. 86. Günther S. Topical administration of vitamin A acid (retinoic acid) in palmar keratoses: Callosities, hyperkeratotic eczema, hypertrophic lichen planus, pityriasis rubra pilaris. Dermatologica. 1972;145:344–7. 87. Baden HP, Byers HR. Clinical findings, cutaneous pathology, and response to therapy in 21 patients with keratosis pilaris atrophicans. Arch Dermatol. 1994;130:469–75. 88. Siegenthaler G, Saurat JH, Salomon D, Mérot Y. Skin cellular retinoid-binding proteins and retinoid-responsive dermatoses. Dermatologica. 1986;173:163–173. 89. Shreberk-Hassidim R, Sheffer S, Horev L, Zlotogorski A, Ramot Y. Successful treatment of refractory Darier disease with alitretinoin with a follow up of over a year: A case report. Dermatol Ther. 2016;29:222–223. 155 90. Takagi A, Kamijo M, Ikeda S. Darier disease. J Dermatol. 2016;43:275–279. 91. Schwartz RA. Efficacy of topical 0.1% adapalene gel for use in the treatment of childhood acanthosis nigricans: A pilot study. Dermatol Ther. 2015;28:266. 92. Phiske MM. An approach to acanthosis nigricans. Indian Dermatol Online J. 2014;5:239–49. 93. Miljković J, Marko PB. Grover’s disease: Successful treatment with acitretin and calcipotriol. Wien Klin Wochenschr. 2004;116:81–83. 94. Helfman RJ. Grover’s disease treated with isotretinoin. Report of four cases. J Am Acad Dermatol. 1985;12:981–984. 95. Norman R, Chau V. Use of etanercept in treating pruritus and preventing new lesions in Grover disease. J Am Acad Dermatol. 2011;64:796–798. 96. Wang D, Chong VC, Chong WS, Oon HH. A review on pityriasis rubra pilaris. Am J Clin Dermatol. 2018;19:377–390. 97. Kromer C, Sabat R, Celis D, Mössner R. Systemic therapies of pityriasis rubra pilaris: A systematic review. J Dtsch Dermatol Ges. 2019;17:243–259. 98. Weidner T, Illing T, Miguel D, Elsner P. Treatment of porokeratosis: A systematic review. Am J Clin Dermatol. 2017;18:435–449. 99. Uusküla A, Erm T. Disseminated giant hyperkeratotic porokeratosis and treatment with acitretin: A case report. Acta Derm Venereol. 2015;95:241–242. 100. Nair PA, Jivani NB, Diwan NG. Kyrle’s disease in a patient of diabetes mellitus and chronic renal failure on dialysis. J Family Med Prim Care. 2015;4:284–286. 25 Retinoids in Antiaging Therapy Zehra Aşiran Serdar and Ezgi Aktaş Karabay Introduction Skin aging represents a complex biologic process that is influenced by endogenous and exogenous factors. Skin aging may present with various signs, including wrinkles, uneven pigmentation, skin roughness, and laxity. Topical retinoids, in the form of topical tretinoin, have been used in the treatment of skin aging since the 1980s, becoming the gold standard in the treatment of photoaged skin (1,2). The adverse effects of tretinoin, even when minimal, have limited its use. To prevent or minimize such side effects as pruritus, burning sensation, erythema, and desquamation in antiaging treatment, studies evaluating the efficacy of tretinoin, tazarotene, isotretinoin, adapalene, retinol, and retinaldehyde have been performed (3). Skin Aging Skin aging is a complex biologic process involving cytokines and mediators. Several factors, including genetic features, cellular metabolism, hormone and metabolic processes, chronic ultraviolet (UV) light exposure, pollution, ionizing radiation, chemicals, toxins (smoking), and mechanical stress, contribute to alterations in skin structure, function, and appearance, each of which may contribute to cutaneous aging. UV radiation, nevertheless, is the main factor in the development of skin aging (4–6). Aged skin is atrophic, leading to a vascular appearance and loss of elasticity. In addition, there is thinning of the epidermis with flattening of the dermoepidermal junction, resulting in fragile skin. The decrease in dermal thickness, vascularity, and fibroblast functions leads to delayed wound healing (7,8). Decreased immune cells reduce immune responsiveness and vitamin D synthesis in aged skin (7,9). Skin damage occurs due to chronic exposure to UV light, presenting as atrophy, laxity, wrinkles, irregular hyperpigmentation, lentigines, and telangiectasias. The processes of collagen degeneration and deposition of abnormal elastotic material manifest as wrinkles, furrows, and discoloration of the skin, which are the characteristics of photodamaged skin (10). Benign neoplasms, premalignant lesions, and malignant lesions of the skin also increase in photodamaged skin (11,12). The response of human skin cells to UV radiation is the activation of multiple cytokine and growth factor receptors, including epidermal growth factor receptor, interleukin (IL)-1 receptor, insulin receptor, and platelet-derived growth factor (PAF) receptor (1). UV irradiation causes both collagen degradation via matrix metalloproteinases (MMPs) and downregulation of type I collagen through downregulation of the transcription of genes that encode for type I procollagen. UV irradiation downregulates transforming growth factor-beta (TGF-β) in human skin, which also causes the breakdown of collagens and impairment in cellular functions of the skin (4,14). UV light exposure of the skin may result in an increase in reactive oxygen species, leading to alterations in the genes and the protein structure and functions. As a result, skin damage occurs (1,4). Retinoids have been used for at least 30 years to diminish the aging process (15). Retinoids The retinoids are composed of vitamin A and its natural (retinaldehyde, retinoic acid, and retinyl esters) and synthetic derivates (16). Retinoids play roles in several cellular processes, including cellular growth and differentiation, cell surface alterations, and immune modulation. Retinoids show their effects by binding to their specific cellular and nucleic acid receptors. The cellular or cytoplasmic receptors include cellular retinoic acid-binding protein (CRABP) types I and II and cellular retinol binding protein (17,18). Tretinoin and its analogs show their effects through nucleic acid receptors. Three forms of the nuclear retinoic acid receptor (RAR) family have been described: RAR-α, RAR-β, and RAR-γ. These receptors are activated by RAR-specific all-transretinoic acid (tretinoin). In the human skin, RARs partner with retinoid X receptors (RXRs) to form heterodimers (19–22). The RXRs are the second family of nuclear receptors, and they interact with 9-cis retinoic acid. Both RARs and RXRs, which are found in normal skin, maintain the retinoid repair process of photodamaged skin. In the human epidermis, RARs are mostly composed of the RAR-γ subtype, while RXRs are mostly composed of RXR-α. As a result, the heterodimer complex of RAR-γ and RXR-α is the major regulator in normal human skin. This heterodimer complex binds to DNA—specifically, to retinoic acid response elements (RARE)—in the promoter region of the genes that are regulated by that specific retinoid. RAR-specific retinoid (tretinoin) provides binding to RARE and initiates transcriptional activity. RXR protein has to associate with RAR protein to initiate the heterodimer function. Retinoids are lipophilic molecules. Through their ability to diffuse through the cellular membranes, they improve photoaging 157 158 by interacting with epithelial cell growth and differentiation. Once they are inside the cells, they bind to specific nuclear receptors and modulate the expression of the genes involved in cellular proliferation and differentiation (10). Topical retinoids affect cellular differentiation by increasing epidermal proliferation, thereby leading to epidermal thickening, stratum corneum compacting, and biosynthesis and deposition of the glycosaminoglycans (23). Tretinoin Tretinoin is the oxidized form of all-trans retinol and the biologically active form of vitamin A. It is distributed predominantly in keratinocytes, with minimal uptake by the dermis. Tretinoin binds all subtypes of RARs and can isomerize to 9-cis retinoic acid, which binds to RXRs (24,25). Tretinoin improves aged skin by inhibiting interstitial collagenase and gelatinase synthesis, which results in collagen repair in the papillary dermis and reduction in wrinkles (13,25). Topical 0.1% tretinoin blocks the UV-induced activation of the nuclear transcription factors activator protein (AP) 1 and nuclear factor (NF) kappa B (13). Tretinoin’s efficacy in antiaging was first described in 1984 (26). Since then, it has become the most widely studied retinoid in the treatment of skin aging (27). Several studies have been performed to evaluate the efficacy and tolerability of tretinoin in the treatment of photoaging. Short-term and long-term studies have shown that the clinical signs of photoaging significantly diminish with the use of tretinoin (1,28–32), and this may continue even after the treatment course has been completed (1). Tretinoin 0.05% cream has been shown to have long-term efficacy and safety in the treatment of photoaging (1,30). In addition, there are studies reporting a similar efficacy of 0.025% tretinoin and 0.1% tretinoin treatment in the improvement of the histologic and clinical signs of skin aging. Treatment with 0.025% or 0.02% tretinoin (known as low-strength tretinoin) has been shown to be safe and well tolerated in most patients for reducing the changes of skin aging (1,33,34). Tretinoin cream 0.02% has also been approved by the Food and Drug Administration (FDA) for photoaging. In addition, treatment with tretinoin at 0.025, 0.05, and 0.1% for aging with regimens of applications on alternate days, twice a week, or three times a week has been shown to be effective in skin aging (28,36–41). The duration of tretinoin treatment varied between 6 and 12 months before a satisfactory improvement was reached. For a significant improvement in dermal changes, more than 6 months of tretinoin therapy may be required (42). In studies performed with high-strength tretinoin solutions/creams, the patients’ skin adjusted to retinoid’s side effects in just 2 weeks of treatment, and the typical side effects of retinoids rapidly disappeared (41). Since the 1980s, tretinoin has become the gold standard in the treatment of photoaged skin (1). Its clinical efficacy as a remedy for photoaging has been investigated and proven more than that of any other treatment, including any other retinoid (1); however, the use of high-strength tretinoin has some limitations. Because it takes a long time to see the effects of tretinoin and the progress is slow, patient adherence to the treatment may be deficient. Retinoid-induced adverse effects are also more common in Retinoids in Dermatology high-strength retinoids (1). Its use may be associated with pruritus, a burning sensation, erythema, and desquamation (43). Isotretinoin The antiaging effects of topical isotretinoin (13-cis retinoic acid) have been evaluated in several studies. Patients treated with topical isotretinoin cream showed dimunition of aging, including fine wrinkles, hyperpigmentation, and swelling. Both 0.1% and 0.05% isotretinoin preparations and a combination of the two were found to be effective antiaging agents. The treatment periods in the various studies ranged between 24 and 36 weeks (44–46). Histologic examination has shown a significant increase in epidermal thickness, while no significant changes were observed in other histologic parameters, including dermal elastosis, thickness of the dermis, epidermal melanin content, number of fibroblasts, and melanocyte dysplasia or keratinocyte atypia (46). Severe irritation due to isotretinoin therapy has been reported in a small number of patients (5%–10%), while mild irritation was common, mostly on the face. In addition, no increase was reported in the plasma levels of isotretinoin over a period of 36 weeks of treatment (1,46). The efficacy of oral isotretinoin in antiaging has also been evaluated. Patients receiving oral isotretinoin 10–20 mg three times a week for 2 months in addition to facial rejuvenation procedures such as peels, botox and collagen injections, blepharoplasty, liposuction, fat transfer, and facelift and patients who received only facial rejuvenation procedures were compared. The isotretinoin-treated group showed a statistically significant lessening of the signs of aging, such as wrinkles, skin thickness, tone, elasticity, and mottled hyperpigmentation (47). The efficacy of low-dose oral isotretinoin was compared with that of 0.05% tretinoin for the treatment of photoaging, and no significant difference was found (48). In another study, both clinical and histologic improvements in skin quality were found after treatment with 20 mg of oral isotretinoin 3 days a week for 12 weeks (49). Retinol Vitamin A alcohol, or all-trans retinol, is a member of the endogenous natural retinoid family, and it is a precursor in the synthesis of endogenous retinal and retinoic acid. Although all-trans retinol has been used in some cosmetic products since 1984 (50), its effect on antiaging was first described in 1995 (51). All-trans retinol induces epidermal thickening and enhances the expression of CRABP II and CRABP I, II mRNAs, and proteins, with fewer side effects than tretinoin (51). Retinol was shown to inhibit UV-induced MMP activation and stimulate collagen synthesis in photoaged skin (13,43,52,53). Effects of retinol are clinically and histologically comparable to tretinoin (54,55), although it is 10 times less potent than ­tretinoin. It must be converted to retinoic acid (in vivo) to be active (43,56–58). Retinol is a highly unstable agent, and through exposure to light and air, it may easily degrade to biologically inactive forms; thus, the vehicle for retinol is critical (1). 159 Retinoids in Antiaging Therapy Studies comparing retinol and tretinoin have shown similar clinical results in photodamaged skin (43,56–58). At high doses, ranging from 0.4% to 1.6% (51,59), retinol produces unwanted side effects, such as skin dryness, irritation, and itching (60). In addition, at high concentrations, retinol is expected to show dermal effects, while at lower, more tolerable doses, it may primarily exert biologic activities in the epidermis (61). At the same time, many studies have established that retinol can reduce signs of chronologic aging—significant lessening of suborbital wrinkles under the eyes, fine lines, and uneven tone—without any significant adverse skin reaction (61). Retinol Derivates In the attempt to stabilize retinol, retinol derivates, including retinyl acetate, retinyl propionate, and retinyl palmitate have been developed. They have been widely used in cosmetic products (1). In contrast to topical retinol, retinyl propionate cream does not demonstrate any statistically significant improvements in photoaging (62). Among several retinol derivates, the n-formyl aspartame derivative of retinol was reported to be a promising antiaging agent, with good photostability and a tolerable profile (63). The efficacy of retinol derivatives in reducing skin aging is still unclear. Retinol Combinations There is a rise in developing combination therapies in order to obtain a greater improvement in antiaging results. Retinol is commonly used in combination with other antiaging agents. In the studies of evaluating the effects of retinol and vitamin C combinations on aging skin, repeated application of retinol and vitamin C in combination was shown to reverse skin changes due to chronologic aging and photoaging (64). A combination of retinol (0.3%) and hydroquinone (4%) proved to be more effective than 0.05% tretinoin emollient cream at 16 weeks, when considering dyspigmentation, fine wrinkles, and tactile roughness (65). A combination of retinol and glycolic acid may induce more significant improvement in the treatment of photoaged skin when compared with glycolic acid or retinol alone (66). In a study conducted among postmenopausal women, daily treatment with a retinol–dimethylenolamine combination was reported to improve signs of skin aging (67). Retinaldehyde Retinaldehyde is an intermediate metabolite formed in the transformation of retinol to retinoic acid in human keratinocytes (68). Its biologic activity results from its enzymatic transformation into retinoic acid via the activity of epidermal keratinocytes, and it is qualitatively similar to that of retinoic acid. Treatment with topical retinaldehyde was demonstrated to induce CRABP II mRNA and protein, increase epidermal t­hickness, increase keratin-14 expression, and enhance keratinocyte proliferation (69). Retinaldehyde 0.05% and 0.05% retinoic acid treatments are equally effective in reducing wrinkles and skin roughness, whereas retinaldehyde causes minimal irritation, leading patients to be compliant with the therapy (70,71). In another study, retinaldehyde creams at 0.1% and 0.05% doses were well tolerated and effectively improved photoaged skin (72). Daily application of topical 0.05% retinaldehyde after laser therapy was found to be associated with better results, suggesting that retinaldehyde can be used as an adjuvant therapy in antiaging procedures (73). Tazarotene Tazarotene, an acetylenic retinoid, is used mainly in the treatment of psoriasis and acne. Tazarotene is a prodrug that is rapidly metabolized to its active form, tazarotenic acid. Although tazarotene is a member of the retinoid family, it presents a different receptor selectivity pattern from tretinoin. Tretinoin directly activates all RAR subtypes, while it indirectly stimulates RXRs; tazarotenic acid selectively binds to RAR-β and RAR-γ but not RXRs (1). Tazarotenic acid modulates the expression of retinoid-­responsive genes, including the ones that regulate cell proliferation, cell differentiation, and inflammation. Tazarotene also downregulates the abnormal expression of keratinocytes, epidermal growth factor receptor, and hyperproliferative keratins (74–76). Clinical trials have shown that topical tazarotene application was effective in the treatment of aged skin. Both 0.05% and 0.1% concentrations of tazarotene showed the same efficacy in antiaging treatment; however, in lower concentrations, side effects, including irritation, were milder, possibly contributing to better compliance. Tazarotene elicits more rapid progress in the treatment of antiaging when compared with tretinoin, but ultimately, both showed a similar degree of improvement in epidermal thickness, fine wrinkling, lentigines, elastosis, and mottled hyperpigmentation. Local adverse events were mild to moderate with a burning sensation occurring with higher tazarotene concentrations (31,32,77,78). Bexarotene Bexarotene is a synthetic topical retinoid that is mainly used in the treatment of cutaneous T-cell lymphoma stages IA and IB, as well as alopecia, chronic hand dermatitis, lymphomatoid papulosis, and psoriasis (25,79). No studies evaluating the efficacy of bexarotene in the treatment of photoaging are available. Adapalene Adapalene is a third-generation synthetic retinoid, which shows selectivity to the nuclear retinoic acid receptor (RAR-β/γ) and does not bind to RXRs. The receptor selectivity of adapalene provides less irritation (1,25,80). It targets abnormal desquamation, modulates cellular differentiation, and shows anti-inflammatory effects (81). Adapalene 0.1% and 0.3% have also been shown to be effective in the treatment of actinic keratoses and solar lentigines (1). Adapalene may reduce wrinkles and hyperpigmentation, as well as improve cutaneous hydration (29,83). It is well tolerated by patients (84) and may be preferred in the treatment of mild or moderate skin aging or in patients who show intolerance to conventional retinoids. 160 Alitretinoin Alitretinoin, or 9-cis retinoic acid, is a natural, endogenous retinoid that binds to and activates all known intracellular RAR and RXR subtypes (85). It has been used in the topical treatment of AIDS-associated Kaposi sarcoma (86) and chronic hand dermatitis (87). In a study evaluating the antiaging effects of 0.1% topical alitretinoin improvement in seborrheic keratoses, actinic keratoses and other signs of photoaging were noted. It is well tolerated (82). Seletinoid G Seletinoid G is a fourth-generation retinoid with receptor selectivity for RAR-γ. It is predominantly expressed in the epidermis compared with other RARs (1). In a recent study, topical treatment with seletinoid G improved aged skin similarly to tretinoin by increasing expressions of type I procollagen, tropoelastin, and fibrillin-1, while reducing MMP-1. It may cause minimal irritation, but under occlusion and in contrast to tretinoin it does not lead to severe erythema (35). Seletinoid G may be considered as an effective agent in the treatment of skin aging, with the advantage of an absence of skin irritation. Conclusions Skin aging is a complex biological process influencing individuals’ feelings of wellbeing. Topical retinoids remain the gold standard therapy. Their effects emerge in interactions with different cellular pathways, from keratinocyte and melanocyte differentiation to collagen type I synthesis. In contrast, the adverse effects of retinoids, such as erythema, burning, sensitivity, and irritation occasionally reduce compliance and subsequent usage. REFERENCES 1. Mukherjee S, Date A, Patravale V et al. Retinoids in the treatment of skin aging: An overview of clinical efficacy and safety. J Clin Interv Aging. 2006;1:327–348. 2. Kligman AM, Grove GL, Hirose R, Leyden JJ. Topical tretinoin for photoaged skin. J Am Acad Dermatol. 1986;15:836–859. 3. Babamiri K, Nassab R. Cosmeceuticals: The evidence behind the retinoids. Aesthet Surg J. 2010;30:74–77. 4. Rittié L, Fisher G. UV-light-induced signal cascades and skin aging. Aging Res Rev. 2002;1:705–720. 5. Cevenini E, Invidia L, Lescai F et al. Human models of aging and longevity. Expert Opin Biol Ther. 2008;8:1393–1405. 6. Uitto J. Understanding premature skin aging. N Engl J Med. 1997;337:1463–1465. 7. Yaar M, Gilchrest BA. Skin Aging: Postulated mechanisms and consequent changes in structure and function. Clin Ger Med. 2001;17:617–630. 8. Rheinwald JG, Hahn WC, Ramsey MR et al. A two-stage p16 (INK4A) and p53–dependent keratinocyte senescence mechanism that limits replicative potential independent telomere status. Mol Cell Bio. 2002;22:5157–5172. 9. Baumann L. Skin ageing and its treatment. J Pathol. 2007;211:241–251. 10. Gilchrest BA. A review of skin aging and its medical therapy. Br J Dermatol. 1996;135:867–875. Retinoids in Dermatology 11. Torras H. Retinoids in aging. Clin Dermatol. 1996;74:207–215. 12. Oppel T, Korting HC. Actinic keratosis: The key event in the evolution from photoaged skin to squamous cell carcinoma. Therapy based on pathogenetic and clinical aspects. Skin Pharmacol Physiol. 2004;17:67–76. 13. Fisher GJ, Datta SC, Talwar HS et al. The molecular basis of sun induced premature ageing and retinoid antagonism. Nature 1996;379:335–338. 14. Massague J. TGF-beta signal transduction. Ann Rev Biochem. 1998;67:753–791. 15. Ramos-e-Silva M, Hexsel DM et al. Hydroxy acids and retinoids in cosmetics. Clin Dermatol. 2001;19:460–466. 16. Antille C, Tran C, Sorg O, Saurat JH. Penetration and metabolism of topical retinoids in ex-vivo organ-cultured fullthickness human skin explants. Skin Pharmacol Physiol. 2004;17:124–128. 17. Roos TC, Jugert FK, Merk HF, Bickers DR. Retinoid metabolism in the skin. Pharmacol Rev. 1998;50:315–333. 18. Astrom A, Tavakkol A, Pettersson U et al. Molecular cloning of two human cellular retinoic acid-binding proteins (CRABP). J Biol Chem. 1991;266:17662–17666. 19. Giguère V, Ong ES, Segui P, Evans RM. Identification of a receptor for the morphogen retinoic acid. Nature 1987;330: 624–629. 20. Brand MJ, Petkovich M, Krust A et al. Identification of a second human retinoic acid receptor. Nature 1988;332:850–853. 21. Fisher GJ, Talwar HS, Xiao JH et al. Immunological identification and functional quantification of retinoic acid and retinoic X receptor proteins in the human skin. J Biol Chem. 1994;269:20629–20635. 22. Xiao JH, Durand B, Chambon P, Voorhees JJ. Endogenous retinoic acid receptor-retinoid X receptor heterodimers are the major functional forms regulating retinoid-responsive elements in adult human keratinocytes. J Biol Chem. 1995;270:3001–3011. 23. Griffiths CEM, Finkel IJ, Tranfaglia MG et al. An in-vivo experimental model for topical retinoid effects on human skin. Br J Dermatol. 1993;29:389–399. 24. Robinson DM, Aasi SZ. Cosmetic concerns and management strategies to combat aging. Maturitas. 2011;70:256–260. 25. Wolverton SE, editor. Comprehensive Dermatologic Drug Therapy. 3rd ed. Philadelphia: Saunders, 2012; pp. 252–268. 26. Kligman LH, Chen HD, Kligman AM. Topical retinoic acid enhances the repair of ultraviolet damaged dermal connective tissue. Connect Tissue Res. 1984;12:139–150. 27. Riahi RR, Bush AE, Cohen PR. Topical retinoids: Therapeutic mechanisms in the treatment of photodamaged skin. Am J Clin Dermatol 2016;17:265–276. 28. Darlenski R, Surber C, Fluhr JW. Topical retinoids in the management of photodamaged skin: From theory to evidencebased practical approach. Br J Dermatol. 2010;163:1157–1165. 29. Farris PK, Rendon MI. The mechanism of action of the topical retinoids for the treatment of nonmalignant photodamage. J Cosmet Dermatol. 2010;23:108–109. 30. Kang S, Bergfeld W, Gottlieb AB et al. Long-term efficacy and safety of tretinoin emollient cream 0.05% in the treatment of photodamaged facial skin: A two-year, randomized, ­placebo-controlled trial. Am J Clin Dermatol. 2005;6:245–253. 31. Lowe N, Gifford M, Tanghetti E et al. Tazarotene 0.1% cream versus tretinoin 0.05% emollient cream in the treatment of photodamaged facial skin: A multicenter, double-blind, randomized, parallel-group study. J Cosmet Laser Ther. 2004;6:79–85. Retinoids in Antiaging Therapy 32. Kang S, Leyden JJ, Lowe NJ et al. Tazarotene cream for the treatment of facial photodamage: A multicenter, investigator masked, randomized, vehicle-controlled, parallel comparison of 0.01%, 0.025%, 0.05%, and 0.1% tazarotene creams with 0.05% tretinoin emollient cream applied once daily for 24 weeks. Arch Dermatol. 2001;137:1597–1604. 33. Griffiths CEM, Kang S, Ellis CN et al. Two concentrations of topical tretinoin (retinoic acid) cause similar improvement but different degrees of irritation. Arch Dermatol. 1995;131:1037–1044. 34. Nyirady J, Bergfeld W, Ellis C et al. Tretinoin cream 0.02% for the treatment of photodamaged facial skin: A review of 2 double-blind clinical trials. Cutis. 2001;68:135–142. 35. Kim MS, Lee SR, Rho HS et al. The effects of a novel synthetic retinoid, seletinoid G, on the expression of extracellular matrix proteins in aged human skin in vivo. Clinica Chimica Acta. 2005;362:161–169. 36. Raghu P, Sivakumar B. Interactions amongst plasma retinolbinding protein, transthyretin and their ligands: Implications in topical retinoids: Therapeutic mechanisms in the treatment of photodamaged skin 275 vitamin A homeostasis and transthyretin amyloidosis. Biochimicaet Biophysica Acta. 2004;1703:1–9. 37. Ellis CN, Weiss JJ, Hamilton TA et al. Sustained improvement with prolonged topical tretinoin (retinoic acid) for photoaged skin. J Am Acad Dermatol. 1990;23:629–637. 38. Green LJ, McCormick A, Weinstein GD. Photoaging and the skin: The effects of tretinoin. Dermatol Clin. 1993;11: 97–105. 39. Olsen EA, Katz HI, Levine N et al. Tretinoin emollient cream for photodamaged skin: Results of 48-week, multicenter, double-blind studies. J Am Acad Dermatol. 1997;37: 217–226. 40. Cuce LC, Bertino MC, Scattone L, Birkenhauer MC. Tretinoin peeling. Dermatol Surg. 2001;27:12–14. 41. Kligman DE, Draelos ZD. High-strength tretinoin for rapid retinization of photoaged skin. Dermatol Surg. 2004;30:864–866. 42. Bhawan J, Olsen E, Lufrano L et al. Histologic evaluation of the long-term effects of tretinoin on photodamaged skin. J Dermatol Sci. 1996;11:177–182. 43. Bouloc A, Vergnanini AL, Issa MC. A double-blind randomized study comparing the association of retinol and LR2412 with tretinoin 0.025% in photoaged skin. J Cosmet Dermatol. 2015;14:40–46. 44. Cunningham WJ. Topical isotretinoin and photodamage. Dermatologica. 1990;181:350–351. 45. Armstrong RB, Lesiewicz J, Harvey G et al. Clinical panel assessment of photodamaged skin treated with isotretinoin using photographs. Arch Dermatol. 1992;128:352–356. 46. Maddin S, Lauharanta J, Agache P et al. Isotretinoin improves the appearance of photodamaged skin: Results of a 36-week, multicenter, double-blind, placebo-controlled trial. J Am Acad Dermatol. 2000;42:56–63. 47. Hernandez-Perez E, Khawaja H, Alvarez T. Oral isotretinoin as part of the treatment of cutaneous aging. Dermatol Surg. 2000;26:649–652. 48. Bagatin E, Guadanhim LR, Enokihara MM et al. Low-dose oral isotretinoin versus topical retinoic acid for photoaging: A randomized, comparative study. Int J Dermatol. 2014;53:114–122. 161 49. Bravo BS, Azulay DR, Luiz RR et al. Oral isotretinoin in photoaging: Objective histological evidence of efficacy and durability. Ana Bras Dermatol. 2015;90:479–486. 50. Rolewski SL. Clinical review: Topical retinoids. Dermatol Nurs. 2003;15:447–465. 51. Kang S, Duell EA, Fisher GJ et al. Application of retinol to human skin in vivo induces epidermal hyperplasia and cellular retinoid binding proteins characteristic of retinoic acid but without measurable retinoic acid levels or irritation. J Invest Dermatol. 1995;105:549–556. 52. Sorg O, Antille C, Kaya G, Saurat JH. Retinoids in cosmeceuticals. Dermatol Ther. 2006;19:289–296. 53. Kafi R, Kwak HS, Schumacher WE et al. Improvement of naturally aged skin with vitamin A (retinol). Arch Dermatol. 2007;143:606–612. 54. Wójcik A, Bartnicka E, Namieciński P, Rotsztejn H. Influence of the complex of retinol-vitamin C on skin surface lipids. J Cosmet Dermatol. 2015;14:92–99. 55. Bubna AK. Alitretinoin in dermatology—an update. Indian J Dermatol. 2015;60:520. 56. Randhawa M, Rossetti D, Leyden JJ et al. One-year topical stabilized retinol treatment improves photodamaged skin in a double-blind, vehicle-controlled trial. J Drugs Dermatol. 2015;14:271–280. 57. Babcock M, Mehta RC, Makino ET. A randomized, doubleblind, split-face study comparing the efficacy and tolerability of three retinol-based products vs. three tretinoin-based products in subjects with moderate to severe facial photodamage. J Drugs Dermatol. 2015;14:24–30. 58. Ho ET, Trookman NS, Sperber BR et al. A randomized, ­doubleblind, controlled comparative trial of the antiaging properties of non-prescription tri-retinol 1.1% vs. prescription tretinoin 0.025%. J Drugs Dermatol. 2012;11: 64–69. 59. Varani J, Warner RL, Gharaee-Kermani M et al. Vitamin A antagonizes decreased cell growth and elevated collagendegrading matrix metalloproteinases and stimulates collagen accumulation in naturally aged human skin. J Invest Dermatol. 2000;114:480–486. 60. Kim BH, Lee YS, Kang KS. The mechanism of retinolinduced irritation and its application to anti-irritant development. Toxicol Lett. 2003;146:65–73. 61. Bellemère G, Stamatas GN, Bruère V et al. Antiaging action of retinol: From molecular to clinical. Skin Pharmacol Physiol. 2009;22:200–209. 62. Green C, Orchard G, Cerio R, Hawk JL. A clinicopathological study of the effects of topical retinyl propionate cream in skin photoageing. Clin Exp Dermatol. 1998;23:162–167. 63. Han HS, Kwon YJ, Park MS et al. Efficacy validation of synthesized retinol derivatives in vitro: Stability, toxicity, and activity. Bioorg Med Chem. 2003;11:3839–3845. 64. Seité S, Bredoux C, Compan D et al. Histological evaluation of a topically applied retinol-vitamin C combination. Skin Pharmacol Physiol. 2005;18:81–87. 65. Draelos S. Novel approach to the treatment of hyperpigmented photodamaged skin: 4% hydroquinone/0.3% retinol versus tretinoin 0.05% emollient cream. Dermatol Surg. 2005;31:799–804. 66. Feinberg C, Hawkins S, Battaglia A, Weinkauf R. Comparison of anti-aging efficacy from cosmetic ingredients on photoaged skin. J Am Acad Dermatol. 2004;50:P27. 162 67. Barkovic S, Leyden JJ, Wu IT et al. Clinical evaluation of topical retinol-dimethylenolamine (DEMA) treatments for aging skin. J Am Acad Dermatol. 2005;52:P27. 68. Sass J, Didierjean I, Carraux P et al. Metabolism of topical retinaldehyde and retinol by mouse skin in vivo: Predominant formation of retinyl esters and identifi cation of 14-hydroxy-4, 14-retro-retinol. Exp Dermatol. 1996;5:267–271. 69. Saurat JH, Didierjean L, Masgrau E et al. Topical retinaldehyde on human skin: Biological effects and tolerance. J Invest Dermatol. 1994;103:770–774. 70. Creidi P, Vienne MP, Ochonisky S et al. Profilometric evaluation of photodamage after topical retinalde­ hyde and r­etinoic acid treatment. J Am Acad Dermatol. 1998;39:960–965. 71. Diridollou S, Vienne MP, Alibert M et al. Efficacy of topical 0.05% retinaldehyde in skin aging by ultrasound and rheological techniques. Dermatology. 1999;199:37–41. 72. Kwon HS, Lee JH, Kim GM, Bae JM. Efficacy and safety of retinaldehyde 0.1% and 0.05% creams used to treat photoaged skin: A randomized double-blind controlled trial. J Cosmet Dermatol. 2018;17:471–476. 73. Mordon S, Lagarde JM, Vienne MP et al. Ultrasound imaging demonstration of the improvement of non-ablative laser remodeling by concomitant daily topical application of 0.05% retinaldehyde. J Cosmet Laser Ther. 2004;6:5–9. 74. Roeder A, Schaller M, Schäfer-Korting M, Korting HC. Tazarotene: Therapeutic strategies in the treatment of psoriasis, acne and photoaging. Skin Pharmacol Physiol. 2004;17:111–118. 75. DiSepio D, Ghosn C, Eckert RL et al. Identification and characterization of a retinoid-induced class II tumor suppressor/ growth regulatory gene. Proc Natl Acad Sci USA. 1998;95:14811–14815. 76. Chandraratna RA. Tazarotene-first of a new generation of receptor-selective retinoids. Br J Dermatol. 1996;135:18–25. Retinoids in Dermatology 77. Machtinger LA, Kaidbey K, Lim J et al. Histological effects of tazarotene 0.1% cream vs. vehicle on photodamaged skin: A 6-month, multicentre, double-blind, randomized, vehiclecontrolled study in patients with photodamaged facial skin. Br J Dermatol. 2004;151:1245–1252. 78. Kang S, Krueger GG, Tanghetti EA et al. Tazarotene cream in photodamage study group. A multicenter, randomized, double-blind trial of tazarotene 0.1% cream in the treatment of photodamage. J Am Acad Dermatol. 2005;52:268–274. 79. Rajiv M, Singh N. Bexarotene gel: A new topical therapy for alopecia areata. 2010;2:66–67. 80. Bagatin E, Goncalves HdS, Sato M et al. Comparable efficacy of adapalene 0.3% gel and tretinoin 0.05% cream as treatment for cutaneous photoaging. Eur J Dermatol. 2018;28:343–350. 81. Leyden J. Adapalene in clincal practice. Cutis. 2001;68:7–9. 82. Baumann L, Vujevich J, Halem M et al. Open-label pilot study of 0.1% alitretinoin gel in the treatment of photoaging. Cutis. 2005;76:69–73. 83. Herane MI, Orlandi C, Zegpi E et al. Clinical efficacy of adapalene (Differin(®)) 0.3% gel in Chilean women with cutaneous photoaging. J Dermatolog Treat. 2012;23:57–64. 84. Kang S, Goldfarb M, Weiss J et al. Assessment of adapalene gel for the treatment of actinic keratoses and lentigines: A randomized trial. J Am Acad Dermatol. 2003;49:83–90. 85. Cheer SM, Foster RH. Alitretinoin. Am J Clin Dermatol. 2000;1:307–316. 86. Bodsworth NJ, Bloch M, Bower M et al. Phase III vehiclecontrolled, multi-centered study of topical alitretinoin gel 0.1% in cutaneous AIDS related Kaposi’s sarcoma. Am J Clin Dermatol. 2001;2:77–87. 87. Ruzicka T, Larsen FG, Galewicz D et al. Oral alitretinoin (9-cis-retinoic acid) therapy for chronic hand dermatitis in patients refractory to standard therapy: Results of a randomized, doubleblind, placebo-controlled, multicenter trial. Arch Dermatol. 2004;140:1453–1459. 26 Retinoids in Other Skin Diseases Uwe Wollina, Piotr Brzezinski, and André Koch TABLE 26.1 Introduction Retinoids were introduced into dermatology four decades ago. There is an ongoing interest to use these compounds in recalcitrant skin diseases not found in the list of approved retinoid indications. These off-label indications include inflammatory diseases, metabolic and storage disorders, autoimmune and bullous diseases, pigmentary and infectious disorders, nail diseases, and selected genodermatoses. This chapter will provide a review of this field. Because larger trials are often missing, the references are mainly small series and case reports, with the level of evidence often being low. Inflammatory Disorders Lichen Planus Lichen planus (LP) is a noncontagious papular inflammatory lichenoid skin disease. The disease is characterized by small papules often accompanied by severe itching. LP affects both mucous membranes and skin. In 20% of the cases, LP is found both on skin and mucous membranes, and in about 10% only skin is affected. Some cases occur on the mucous membranes alone. Typically, one can see a whitish network, known as Whickham’s striae, that is caused by hypergranulation in the affected epithelium (1). The retinoid of first choice for mucocutaneous LP is oral acitretin, but there are case reports on isotretinoin, etretinate, and alitretinoin as well (1–3). For topical treatment retinaldehyde 0.1% gel, retinoic acid 0.05% gel, tretinoin 0.1% gel, isotretinoin 0.05% gel, and tazarotene 0.1% gel have been used in treating oral LP (Tables 26.1 and 26.2). Systemic retinoids are effective in cutaneous LP but sometimes have a limited efficacy in mucous membrane and adnexal types of LP (4). Acitretin continues to be as effective in oral LP (5) and esophageal LP (6) as corticosteroids. A dosage of 30 mg alitretinoin/day for 6 months was effective in inducing a remission in recalcitrant cutaneous and esophageal LP. In cases of relapse, alitretinoin remained effective without tachyphylaxis (6). Palmoplantar LP is a rare type which can lead to painful ulcerations. A 50-year-old man was treated with acitretin 0.5 mg/ kg body weight (35 mg), resulting in complete clearance after only 2 months (7). A patient with LP pemphigoides has been Improvement and Clearance Rates of Oral Lichen Planus by Topical Retinoids (Rx−Treatment) Retinoid Concentration Retinaldehyde Retinoic acid 0.1% 0.1% Tretinoin 0.05% Fenretinide Isotretinoin ? 0.1% Tazarotene 0.1% Duration of Rx 2 months 3 weeks to 2 months 1–2 months 2 months 2–4 months 2 months Result (% of Patients [P] or Lesions [L]) 88% improvement P 90%–100% improvement L 46%–87% improvement P 100% L 90%–100% L 100% L successfully treated with acitretin 0.5 mg/kg body weight for 4 months (8). Oral alitretinoin 30 mg/day has been suggested for LP of the nails (9). Disseminated hypertrophic LP was treated successfully with acitretin, administered for 9 months. The initial dosage of oral acitretin 40 mg/day was reduced to 30 mg/day after 3 months and 25 mg/day thereafter (10). A recent prospective open-label single arm pilot study investigated the efficacy and safety of oral alitretinoin 30 mg/day for up to 24 weeks in severe oral LP refractory to standard therapy (n = 10). A >50% reduction in LP severity measured by the Escudier severity score, a scoring system for mucosal disease severity with special reference to oral lichen planus, was observed in 40% of patients. The drug dropout rate was 20% (11). There are two case reports of alitretinoin 30 mg/d for cutaneous LP. The lesions completely disappeared after administration for 5 and 6 months, respectively (12). In summation, more than 500 patients have been treated with either topical or oral retinoids. Granuloma Annulare Granuloma annulare (GA) is a benign, chronic inflammatory skin disease with characteristic annular smooth discolored plaques. Histologically, palisading granulomas can be found (13). Systemic retinoids alone or in combination with psoralen and ultraviolet-A irradiation (RePUVA) have been used for disseminated GA in particular. Best evidence is available for isotretinoin used in dosages of 0.5–1.0 mg/kg/day (14). 163 164 Retinoids in Dermatology TABLE 26.2 Possible Indications of Retinoids in Various Dermatoses Disorder Lichen planus Granuloma annulare Pityriasis rubra pilaris Lichen niditus Prurigo nodularis Acquired perforating dermatosis Lichen sclerosus Elephantiasis nostras Behçet’s disease Dissecting cellulitis Lichen amyloidosis Milia en plaque Lupus erythematosus Morphea IgA-pemphigus Idiopathic guttate hypomelanosis Progressive macular hypomelanosis Melasma and related dyschromias Verrucae vulgaris Facial plane warts Condylomata acuminata Onychomycosis Trachyonychia Brittle nails Hailey-Hailey disease Chanarin-Dorfman syndrome Retinoid(s) Level of Evidence Acitretin Alitretinoin Topical tazarotene or isotretinoin for oral lichen planus Isotretinoin Etretinate, acitretin Acitretin, etretinate, isotretinoin Alitretinoin, topical tazarotene Isotretinoin Alitretinoin Topical tretinoin III IV III Isotretinoin Acitretin Etretinate Acitretin Isotretinoin Isotretinoin Acitretin Acitretin Alitretinoin Topical tretinoin Acitretin Isotretinoin Acitretin Acitretin Topical tretinoin IV II IV IV III IV IV IV IV IV IV IV IV IV IV Isotretinoin IV Topical tretinoin III Isotretinoin Acitretin Topical adapalene Acitretin Isotretinoin Topical tazarotene Acitretin Topical tazarotene Etretinate, acitretin, alitretinoin Acitretin (for ichthyosis) III IV III IV IV IV IV III IV IV III IV III IV IV IV IV suspected clinically, the histopathology does not demonstrate a significant inflammatory infiltrate (15). For juvenile circumscribed PRP, topical tazarotene 0.1% twice a day has been used successfully, leading to postinflammatory hyperpigmentation but total clearance of PRP lesions after 6 weeks of treatment (16,17). Cases resistant to topical treatment may respond to oral alitretinoin 30 mg/day for 7 months combined with moisturizers (18). For moderate to advanced disease, systemic treatment is recommended. Systemic retinoids (etretinate, acitretin, isotretinoin) are considered as first-line therapy for adults and children (19–23). The clinical response is delayed, usually for 3 to 6 months. The recommended daily dosages are 25–75 mg for etretinate, 25–50 mg for acitretin, and 1 mg/kg/day for isotretinoin (Figure 26.1). In cases of limited response, low-dose methotrexate had been added (22). In one prospective study with 45 PRP patients, isotretinoin 2 mg/kg/day was used. After 4 weeks of treatment, 62% of patients achieved a significant improvement (19). In another, but retrospective trial with 75 PRP patients, isotretinoin was used in a dose of 40 mg twice a day in 15 patients. After 16−44 weeks, 67% of patients had a complete clearance, while three patients remained refractory to treatment (24). The author suggested initiating early treatment with retinoids (24). For isotretinoin, the response was independent from the duration of disease in one trial (19). In another study including 50 patients with PRP, 32 received oral retinoids (not further specified). Of these, 59% of patients found the use of retinoids to be “helpful” in treating the disease (23). A retrospective study investigated alitretinoin for type I PRP. Four of five patients responded well to the standard dose of 30 mg/day within 6 months (25). A 19-year-old man with PRP type IV was treated with oral acitretin, 25 mg every other day, with a complete response after 6 months (26). Lichen Nitidus Lichen nitidus is a chronic pruritic inflammatory disease characterized by multiple tiny papules. The generalized type is a rare variant of the disease, and no standardized treatment is available. In a single report, a 15-year-old girl resistant to topical corticosteroids was treated with a starting dose of 0.8 mg/kg body weight isotretinoin, resulting in a complete and stable clearance after 4 months. There was no relapse during the 10-month follow-up period (27). Prurigo Nodularis Pityriasis Rubra Pilaris Pityriasis rubra pilaris (PRP) is a rare chronic papulosquamous disorder of keratinization, with an incidence of between 1 in 5000 and 1 in 50,000 in the population, and no gender predilection. Five major types can be differentiated, with the classic adult type being the most common. PRP is characterized by small follicular papules, coalescing scaly yellow pink patches, and palmoplantar keratoderma. Lesions are symmetrical and diffuse with islands of sparing. Although massive inflammation can be Prurigo nodularis is a chronic pruritic disorder where the lesions follow the cleavage lines. It can be considered as traumatic chronic papulosis with cutaneous neural hyperplasia of xerodermal skin (28). The disease can occur as solitary disease or in association with other dermatoses, such as xerosis cutis, psoriasis, and atopic dermatitis. Treatment is difficult. Alitretinoin 30 mg/day achieved a complete clearance of all lesions in a 46-year-old woman with psoriasis after 5 months of treatment. A maintenance dosage of 30 mg alitretinoin every other day was used for 18 months (29). 165 Retinoids in Other Skin Diseases (a) (b) FIGURE 26.1 Pityriasis rubra pilaris type I in a 69-year-old male patient. (a) Before treatment with massive erythema and infiltrations; note the islands of sparing. (b) After 1 week with 30 mg acitretin/day, significant improvement. Acquired Perforating Dermatosis Acquired perforating dermatosis is a chronic dermatosis with umblicated papules and plaques covered by crusts. It belongs to the heterogeneous group of transepidermal eliminating disorders and may be associated with metabolic or neoplastic diseases (30). Oral retinoids (acitretin 10–20 mg/day or isotretinoin 40 mg/d) can be used as second-line therapy in corticosteroid-refractory cases. Topically, tretinoin 0.02%–0.025% has been employed for limited lesions (31). Lichen Sclerosus Lichen sclerosus (LS) is a chronic inflammatory disorder affecting predominantly genital skin and mucous membranes, with only 6% of all LS cases occurring on extragenital skin. Topical and systemic retinoids are effective: topical tretinoin 0.025% applied once a day, 5 days a week, lessened vulval LS after 12 months of treatment. Oral etretinate 1 mg/kg ameliorated vulval LS recalcitrant to corticosteroids (32). A double-blind, placebocontrolled, multicenter trial investigated acitretin 20 to 30 mg/ day in severe vulvar LS in 78 women of whom 46 were eligible for efficacy analysis. At week 16, 14 of 22 patients had at least a partial response. Pruritus and burning could be stopped in 100% (33). A randomized, double-blind, placebo-controlled study was performed in 52 men with severe, long-standing LS receiving either acitretin 35 mg/day or placebo for 20 consecutive weeks. Of the 49 patients who completed the study, 36.4% achieved a complete response, while 36.4% achieved partial response (34). Elephantiasis Nostras Elephantiasis nostras is an end-stage lymphatic disorder characterized by chronic inflammation and disturbed lymphatic flow leading to fibrosis, papillomatosis, and sometimes verrucous skin lesions. A nearly complete resolution of verrucous elephantiasis nostras has been reported in a 64-year-old man during acitretin therapy (35). Behçet’s Disease Behçet’s disease is a multisystemic neutrophilic disorder with endemic hot-spots in the Mediterranean region, along the Silk Road, and on the Korean peninsula. It is characterized by recurrent oral and genital ulcerations, uveitis, and central nervous system vasculitis (36). Tretinoin has demonstrated ex vivo an inhibitory activity in peripheral mononuclear blood cells from patients with active Behçet’s disease by the nuclear factor-kappa pathway in a dose-dependent manner with 0.01 µmol as the lowest dosage investigated (37). A single-blinded, controlled study investigated safety and efficacy of isotretinoin in 30 patients with Behçet’s disease. Isotretinoin was used at a daily dosage of 20 mg for 3 months. The regimen reduced oral and cutaneous ulcers and other features of the Clinical Manifestation Index and minimized C-reactive protein and pathergy tests (38). Perifolliculitis Capitis Abscedens et Suffodiens (Dissecting Cellulitis) Perifolliculitis capitis abscedens et suffodiens (Hoffman), or dissecting cellulitis (DC), is a severe chronic scalp disorder with destructive folliculitis, perifollicular pustules, nodules, abscesses, and sinus formation. Untreated, the disease causes scarring alopecia. It has a predominance in African-American men and can occur in children, adolescents, and adults. It may be a single disease, or it can be associated with hidradenitis suppurativa/acne inversa or Crohn’s disease (39,40). The etiology is not well understood, with a follicular occlusion and an aberrant cutaneous immune response to commensal bacteria being considered (41). Antimicrobials, dapsone, and tumor necrosis 166 Retinoids in Dermatology (a) (b) FIGURE 26.2 Folliculitis decalvans with patchy alopecia, crusts, and bundle hairs. (a) Before treatment and (b) after 2 weeks a combination of initially 40 mg isotretinoin, 300 mg clindamycin and 20 mg prednisolone per day. factor-alpha (TNF-α) (adalimumab) have been used sometimes in conjunction with surgery (39,41). Isotretinoin 1 mg/kg/day or acitretin 10 mg/day is helpful in controlling the disease, but a regimen of a minimum of 3−5 months is required (42–44). Oral isotretinoin 40 mg/day has been successfully used in a single patient with generalized LA. Complete clearance was achieved by 3 months (50). Milia en Plaque Folliculitis Decalvans Folliculitis decalvans (FD) is another neutrophilic chronic relapsing disorder of the scalp. An abnormal host response to Staphylococcus aureus has been considered as a pathogenetic factor. In a subset of patients with FD, tufted hair folliculitis was the major presentation. A 27-year-old Caucasian man was treated successfully with an initial combination of isotretinoin 40 mg, clindamycin 300 mg, and prednisolone 20 mg per day. By 3 weeks, there was an excellent response (Figure 26.2) (45). Metabolic and Storage Disorders Lichen Amyloidosis Lichen amyloidosis (LA) is characterized by the deposition of amyloid originating from epidermal keratin. LA is seen in association with other dermatoses such as atopic dermatitis (AD), stasis dermatitis, or interface dermatitis. There are three major subtypes: papular, macular, and nodular (46). A 49-year-old woman with AD developed localized brownish papules on the left forearm and right elbow, which could be identified as LA. Because LA was unresponsive to various other systemic treatments, alitretinoin therapy was initiated. After a 6-month course of alitretinoin 30 mg/day, there was a marked improvement with dimunition of the hyperkeratotic papules without worsening of AD. Histologically, there was clearance of amyloid deposition (47). The observation is supported by another patient, where a daily dose of 30 mg alitretinoin led to a complete response (48). There is an additional case report of a 22-year-old woman from China who was afflicted for 20 years with multiple papular and poikiloderma-like, mildly pruritic, LA skin lesions on her face, outer ear, neck, and upper aspect of the back. LA was confirmed by histopathology, and she was treated with a daily regimen of oral acitretin 0.5 mg/kg. There was a partial response after 6 months that continued for another 18 months (49). Milia en plaque (MEP) is a benign disorder with multiple tiny cysts on a limited area. A 7-year-old boy with MEP on the tip of his nose applied tretinoin cream 0.025% nightly. A complete clearance could be achieved by the eighth week (51). Autoimmune Diseases Lupus Erythematosus Lupus erythematosus (LE) is considered the most frequent type of autoimmune connective tissue disorder. Chronic discoid LE (CDLE) is a subtype with chronic inflammatory discoid lesions in the sun-exposed areas. Untreated CDLE usually results in scarring. Acitretin is an option for corticosteroid-resistant CDLE as underlined by a recent systematic Cochrane Review (52). The current S2k European Guideline for Cutaneous Lupus Erythematosus considers retinoids as second-line treatment of disseminated CDLE (53). Acitretin is also effective in LE/LP overlap syndrome (54). Low-dose isotretinoin (20 mg/day) has also been used occasionally in women of childbearing age due to the shorter half-life of the drug. The initial dosage is 40 mg/d, while maintenance therapy may be either 20 mg/day or 40 mg every other day for 6 months (55). Morphea and Systemic Sclerosis Morphea and systemic sclerosis (SS) are connective tissue diseases characterized by tightening, thickening, and hardening of the skin, leading to significant morbidity. SS may affect internal organs, resulting in mortality. Because a major pathogenetic pathway is the excessive production of collagen, systemic retinoids have been investigated to control this aspect of the disease (56). Retinoic acid leads to increased expression of cyclooxygenase-2 (COX-2), which by induction of prostaglandin E2 inhibits fibroblast proliferation. Retinoic acid suppresses expression of 5-lipooxygenase (5-LOX) that subsequently leads to an inhibition of 167 Retinoids in Other Skin Diseases both connective tissue growth factor and transforming growth factor-beta. These result in reduction of the level of type I and type III collagen mRNA with reduced synthesis of collagen (56). In an analysis of eight studies with oral etretinate 0.5–0.8 mg/ kg/day administered for up to 12 months, acitretin 1 mg/kg/day, followed by PUVA therapy for at least 12 months, and topical tretinoin 0.05% or tocoretinate 0.25% for up to 3 years, there was clearance of morphea lesions and lessening of skin tightness in SS (56). Acitretin 10 mg/day combined with narrow-band UVB for 2 months was successful in a woman with morphea that developed after radiotherapy for breast cancer (57). Bullous Disorders Linear IgA Bullous Dermatosis Linear IgA bullous dermatosis is a very rare bullous disease that can be further differentiated into intra-epidermal neutrophilic IgA dermatosis and subcorneal pustular dermatosis-type. There are two case reports on successful treatment with 35 mg acitretin/day either alone or in combination with 100 mg dapsone/day (58,59). Pigmentary Disorders Idiopathic Guttate Hypomelanosis Idiopathic guttate hypomelanosis is a common acquired leukoderma of heterogeneous and largely unknown pathogenesis. Clinically, it is characterized by multiple, discrete round or oval, porcelain-white macules on sun-exposed areas of the forearms or pretibial aspects of the legs. It affects mostly middle-aged patients (60). Among other medical treatments, tretinoin 0.025% cream has been used for several weeks with variable results (61). Progressive Macular Hypomelanosis Progressive macular hypomelanosis (PMH) is a rare dyschromic disorder characterized by asymptomatic, hypopigmented macules located predominantly on the trunk. Oral isotretinoin 40 mg/day was successful in a single case of PMH within 1 year (62) but failed in another patient (63). Melasma and Post-Inflammatory Hyperpigmentation Melasma and post-inflammatory hyperpigmentation are the most common dyschromias. Tretinoin 0.05% in combination with fluocinolone acetonide 0.01% and hydroquinone 4% (Kligman formula) is FDA approved for skin bleaching (64). The combination has also been effective in mild to moderate melasma in Chinese patients, as shown in a randomized, double-blind, placebo-­ controlled, multicenter, parallel-group study with a clinical efficacy of 74.3% after 8 weeks of treatment versus 6.6% response in the placebo group (65). Mild to moderate melasma was treated in 39 women with Fitzpatrick skin type III−VI in a single-center, investigator-blinded study employing a combination of 4% hydroquinone skin care system plus tretinoin 0.02% cream for 24 weeks. Melasma severity, pigmentation intensity, and Melasma Area and Severity Index (MASI) scores were reduced markedly following 1 month of treatment, and subsequently at week 24, 87.9% of patients were “satisfied” or “very satisfied” (66). Infectious Disorders Currently, the mechanism by which retinoids cure HPV-virus lesions remains obscure. Verrucae Vulgaris Verrucae vulgaris (VV) (common warts) are caused by the human papilloma virus (HPV), mainly HPV-1 and -2, less common HPV-4 to -7. Although VV are common, the ideal treatment has yet to be developed. Widespread warts are a particular challenge. In such cases, oral acitretin is a therapeutic option (67–69). A dosage of 25 mg to 30 mg/day achieved a complete response of widespread recalcitrant common warts within 3−6 months of treatment (68,69). In two adult patients with multiple plane warts of skin and mucosa, 0.3−0.4 mg/kg isotretinoin achieved a complete remission after 1 month (70). There is one randomized comparative open trial for plantar warts with either topical adapalene or cryotherapy. This study enrolled 50 patients with 424 plantar warts. Adapalene gel 0.1% was used twice daily under occlusion. All warts cleared on average within 36.1 days with adapalene compared to 52.2 days with cryotherapy (71). Facial Plane Warts A double-blind, randomized, placebo-controlled trial was conducted for recalcitrant facial plane warts treated for at least 3 years without success (n = 31). Patients received either isotretinoin 30 mg/day or placebo for 12 weeks. All warts cleared in the isotretinoin group, although some patients had not previously responded to acitretin. The most common adverse events included cheilitis, xerosis, dry eyes, and photosensitivity seen in all of the patients (72). Condylomata Acuminata Condylomata acuminata are anogenital warts, often caused by HPV subtypes 6 and 11. They are highly contagious. Giant condylomas are called Buschke-Löwenstein tumors (73). A 15-year-old boy with recalcitrant giant condylomas was treated with a combination of 25 mg acitretin/day and Mycobacterium indicus pranii vaccination immunotherapy. Complete clearance was obtained after 6 months of acitretin with no recurrence within the next 2 years of follow-up (74). A 16-year-old girl with HPV-6-positive giant condyloma acuminatum was cured by a combination of intramuscular interferon-gamma 1 MIU/day and oral acitretin 30 mg/day after 3 months of treatment (75). Genital warts can be a treatment challenge in immunosuppressed patients. A woman with systemic lupus erythematosus (SLE) not responding to topical imiquimod and regular 168 cryotherapy achieved complete remission of the warts with a combination of surgical debulking and oral isotretinoin with an initial dose of 20 mg/day and a gradual tapering over 8 months. At a 2-year follow-up, there had been no recurrence (76). Retinoids in Dermatology 5 (ABHD5), a highly conserved regulator of adipose triglyceride lipase (ATGL)-mediated lipolysis. The disease belongs to the family of neutral lipid storage disorders with ichthyosis. A classical feature is the presence of Jordan’s anomaly in leucocytes (87). Acitretin 20–30 mg/day was useful in the treatment of nonbullous ichthyosis of this rare disease (88,89). Nail Disorders Onychomycosis Conclusions Onychomycosis is a common fungal infection caused by both dermatophytes and yeast. Topical tazarotene 0.1% gel was investigated in a pilot trial of 15 patients with distal and lateral subungual onychomycosis of the toenails. Tazarotene gel was applied once a day for 12 weeks. Complete clinical and mycologic healing was obtained in all patients at week 12. In addition, in vitro disk diffusion assay with tazarotene solution showed a central area of inhibition in all examined fungal cultures 48 h after incubation (77). The list of possible indications for the therapeutic use of retinoids, in particular the oral retinoids, is still growing (Table 26.2). The versatile effects of retinoids encourage their application for inflammatory and autoimmune disorders, cutaneous infections, and adnexal disorders. Patients with common and orphan diseases may profit from their use. The major drawback of the retinoids is their teratogenicity. This limits their use during childbearing age in women. The drugs need some kind of laboratory monitoring, which increases treatment costs. Finally, systemic retinoids have other unwanted side effects such as dry skin and mucous membranes, increased hair loss, and nail changes. In several indications retinoids compete with other possible treatments and may be cheaper, more convenient, or more efficacious. At least in the Western world, retinoids are currently used less commonly than at the end of the twentieth century. Trachyonychia Trachyonychia (rough nails) is characterized by brittle, thin nails, with excessive longitudinal ridging. On histology, spongiosis becomes evident (78). Case reports have been published on the use of daily oral acitretin 0.3 to 0.5 mg/kg alone or in combination with clobetasol or other topical corticosteroids with partial improvements after 2 months and further improvement during the following 10 months of treatment (79,80). Brittle Nails Brittle nails are a common disorder with surface roughness, raggedness, and peeling. Exposure to wet work is a known trigger. In an open trial, patients with brittle nails applied 0.1% tazarotene gel twice daily for 24 weeks. After 36 weeks, 89.5% agreed that their nails had improved overall (81). Genodermatoses Hailey-Hailey Disease (Familial Benign Chronic Pemphigus) Hailey-Hailey (HH) disease, or familial benign chronic pemphigus, is a rare autosomal dominant acantholytic disorder localized in areas of repeated friction. The gene defect affects the ATPase calcium-transporting type 2C member 1 gene (ATP2C1) located on chromosome 3q21-q24. Its function is to maintain normal intracellular concentrations of Ca2+/Mn2+ by transporting Ca2+/Mn2+ into the Golgi apparatus (82). Oral etretinate 25 mg/day, acitretin 25 mg/day or alitretinoin 30 mg/day have been used in refractory HH disease with success. In some patients, a complete response could be achieved within 1−3 months, even in the vesiculobullous subtype (83–86). Chanarin-Dorfman Syndrome Chanarin-Dorfman syndrome is an autosomal-recessive disease caused by mutations of alpha-beta hydrolase domain-containing REFERENCES 1. Schilling L, Vogt T. Lichen ruber planus: Better understanding, better treatment! Hautarzt. 2018;69:100–108. 2. Petruzzi M, Lucchese A, Lajolo C et al. Topical retinoids in oral lichen planus treatment: An overview. Dermatology. 2013;226:61–67. 3. Miyagaki T, Sugaya M, Miyamoto A et al. Oral erosive lichen planus associated with thymoma treated with etretinate. Australas J Dermatol. 2013;54:e25–e27. 4. Schenkel JS, Lübbers HT, Rostetter C, Metzler P. Traitement médicamenteux du lichen plan buccal. Swiss Dent J. 2017;127:538–539. 5. Singh AR, Rai A, Aftab M et al. Efficacy of steroidal vs nonsteroidal agents in oral lichen planus: A randomised, openlabel study. J Laryngol Otol. 2017;131:69–76. 6. Kolios AG, Marques Maggio E, Gubler C et al. Oral, esophageal and cutaneous lichen ruber planus controlled with alitretinoin: Case report and review of the literature. Dermatology. 2013;226:302–310. 7. Solak B, Kara RO, Kosem M. Palmoplantar lichen planus s­uccessfully treated with acitretin. BMJ Case Rep. 2015;2015:pii: bcr2015211115. 8. Hackländer K, Lehmann P, Hofmann SC. Successful treatment of lichen planus pemphigoides using acitretin as monotherapy. J Dtsch Dermatol Ges. 2014;12:818–819. 9. Iorizzo M. Nail lichen planus—a possible new indication for oral alitretinoin. J Eur Acad Dermatol Venereol. 2016;30:509–510. 10. Jaime TJ, Jaime TJ, Guaraldi Bde M et al. Disseminated hypertrophic lichen planus: Relevant response to acitretin. An Bras Dermatol. 2011;86:S96–S99. 11. Kunz M, Urosevic-Maiwald M, Goldinger SM et al. Efficacy 169 Retinoids in Other Skin Diseases 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. and safety of oral alitretinoin in severe oral lichen planus– results of a prospective pilot study. J Eur Acad Dermatol Venereol. 2016;30:293–298. Molin S, Ruzicka T. Oral alitretinoin in lichen planus: Two case reports. Acta Derm Venereol. 2010;90:523–524. Goucha S, Khaled A, Kharfi M et al. Granuloma annulare. G Ital Dermatol Venereol. 2008;143:359–363. Butsch F, Weidenthaler-Barth B, von Stebut E. Granuloma annulare. Hautarzt. 2015;66:867–875. Wollina U. Pityriasis rubra pilaris. Hautarzt. 2012;63:655–661. Caldarola G, Zampetti A, De Simone C et al. Circumscribed pityriasis rubra pilaris type IV. Clin Exp Dermatol. 2007;32:471–472. Karimian-Teherani D, Parissa M, Tanew A. Response of juvenile circumscribed pityriasis rubra pilaris to topical tazarotene treatment. Pediatr Dermatol. 2008;25:125–126. Yun CH, Kim JS, Ryu HR et al. Circumscribed juvenile ­pityriasis rubra pilaris responsive to alitretinoin. Dermatol Ther. 2016;29:81–83. Goldsmith LA, Weinrich AE, Shupack J. Pityriasis rubra pilaris response to 13-cis-retinoic acid (isotretinoin). J Am Acad Dermatol. 1982;6:710–715. Clayton BD, Jorizzo JL, Hitchcock MG et al. Adult pityriasis rubra pilaris: A 10-year case series. J Am Acad Dermatol. 1997;36:959–964. Gemmeke A, Schönlebe J, Koch A, Wollina U. Pityriasis rubra pilaris – a retrospective single center analysis over eight years. J Dtsch Dermatol Ges. 2010;8:439–444. Eastham AB, Femia AN, Qureshi A, Vleugels RA. Treatment options for pityriasis rubra pilaris including biologic agents: A retrospective analysis from an academic medical center. JAMA Dermatol. 2014;150:92–94. Ross NA, Chung HJ, Li Q et al. Epidemiologic, clinicopathologic, diagnostic, and management challenges of pityriasis rubra pilaris: A case series of 100 patients. JAMA Dermatol. 2016;152:670–675. Dicken CH. Treatment of classic pityriasis rubra pilaris. J Am Acad Dermatol. 1994;31:997–999. Amann PM, Susic M, Glüder F et al. Alitretinoin (9-cis ­retinoic acid) is effective against pityriasis rubra pilaris: A retrospective clinical study. Acta Derm Venereol. 2015;95:329–331. Mota F, Carvalho S, Sanches M, Selores M. Late onset pityriasis rubra pilaris type IV treated with low-dose acitretin. Acta Dermatovenerol Alp Pannonica Adriat. 2016;25:15–17. Topal IO, Gokdemir G, Sahin IM. Generalized lichen nitidus: Successful treatment with systemic isotretinoin. Indian J Dermatol Venereol Leprol. 2013;79:554. Wollina U, Simon D, Knopf B. Hyde’s nodular prurigo– preference for creases of the skin. Dermatol Monatsschr. 1990;176:469–473. Gadaldi K, Erdemoğlu Y, Yawalkar N. Successful treatment of recalcitrant prurigo with alitretinoin. Dermatology. 2015;231:330–333. Wollina U. Transepidermal elimination. Dermatol Monatsschr. 1989;175:321–325. Wagner G, Sachse MM. Acquired reactive perforating dermatosis. J Dtsch Dermatol Ges. 2013;11:723–730. Fistarol SK, Itin PH. Diagnosis and treatment of lichen sclerosus. An update. Am J Clin Dermatol. 2013;14:27–47. Bousema MT, Romppanen U, Geiger JM et al. Acitretin in the treatment of severe lichen sclerosus et atrophicus of the 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. vulva: A double-blind, placebo-controlled study. J Am Acad Dermatol. 1994;30:225–231. Ioannides D, Lazaridou E, Apalla Z et al. Acitretin for severe lichen sclerosus of male genitalia: A randomized, placebo controlled study. J Urol. 2010;183:1395–1399. Polat M, Sereflican B. A case of elephantiasis nostras verrucosa treated by acitretin. J Drugs Dermatol. 2012;11:402–405. Zouboulis CC, Kötter I, Djawari D et al. Current epidemiological data from the German Registry of AdamantiadesBehçet’s disease. Adv Exp Med Biol. 2003;528:43–48. Djeraba Z, Boumedine K, Arroul-Lammali A et al. Ex vivo immunomodulatory effect of all-trans-retinoic acid during Behçet’s disease: A study in Algerian patients. Immunopharmacol Immunotoxicol. 2014;36:78–86. Sharquie KE, Helmi RM, Noiami AA et al. The therapeutic role of isotretinoin in the management of Behçet’s disease: A single-blinded, controlled therapeutic study. J Drugs Dermatol. 2013;12:e68–e73. Wollina U, Gemmeke A, Koch A. Dissecting cellulitis of the scalp responding to intravenous tumor necrosis factor-alpha antagonist. J Clin Aesthet Dermatol. 2012;5:36–39. Syed TA, Ul Abideen Asad Z, Salem G et al. Dissecting ­cellulitis of the scalp: A rare dermatological manifestation of Crohn’s disease. ACG Case Rep J. 2018;5:e8. Scheinfeld N. Dissecting cellulitis. Skinmed. 2015;13:236–238. Tchernev G. Folliculitis et perifolliculitis capitis abscedens et suffodiens controlled with a combination therapy: Systemic antibiosis (metronidazole plus clindamycin), dermatosurgical approach, and high-dose isotretinoin. Indian J Dermatol. 2011;56:318–320. Mihić LL, Tomas D, Situm M et al. Perifolliculitis capitis abscedens et suffodiens in a caucasian: Diagnostic and therapeutic challenge. Acta Dermatovenerol Croat. 2011;19:98–102. Jacobs F, Metzler G, Kubiak J et al. New approach in combined therapy of perifolliculitis capitis abscedens et suffodiens. Acta Derm Venereol. 2011;91:726–727. Gemmeke A, Wollina U. Folliculitis decalvans of the scalp: Response to triple therapy with isotretinoin, clindamycin, and prednisolone. Acta Dermatovenerol Alp Pannonica Adriat. 2006;15:184–186. Sipe JD, Benson MD, Buxbaum JN et al. Amyloid fibril protein nomenclature: 2012 recommendations from the Nomenclature Committee of the International Society of Amyloidosis. Amyloid. 2012;19:167–170. Koh WS, Oh EH, Kim JE, Ro YS. Alitretinoin treatment of lichen amyloidosis. Dermatol Ther. 2017;30(6). doi: 10.1111/ dth.12537. Tietze JK, Heppt MV, Flaig MJ, Thomas P. Successful treatment of lichen amyloidosus with oral alitretinoin. J Eur Acad Dermatol Venereol. 2016;30:884–885. Ma H, Su X, Zhu G et al. Primary localized cutaneous amyloidosis with lichen and poikiloderma-like lesions and an excellent response to systemic acitretin. An Bras Dermatol. 2016;91:661–663. Atacan D, Ergin C, Çelik G et al. Oral isotretinoin: A new treatment alternative for generalized lichen amyloidosis. Australas J Dermatol. 2016;57:246–247. Nambudiri VE, Habib N, Arndt KA, Kane KS. Milia en plaque of the nose: Report of a case and successful treatment with topical tretinoin. Pediatrics. 2014;133:e1373–e1376. 170 52. Jessop S, Whitelaw DA, Grainge MJ, Jayasekera P. Drugs for discoid lupus erythematosus. Cochrane Database Syst Rev. 2017;5:CD002954. 53. Kuhn A, Aberer E, Bata-Csörgő Z et al. S2k guideline for treatment of cutaneous lupus erythematosus – guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol. 2017;31:389–404. 54. Lospinoso DJ, Fernelius C, Edhegard KD et al. Lupus erythematosus/lichen planus overlap syndrome: Successful treatment with acitretin. Lupus. 2013;22:851–854. 55. Pérez-Crespo M, Bañuls J, Mataix J, Lucas A. Lowdose isotretinoin for treatment of chronic discoid lupus in women of childbearing age. Actas Dermosifiliogr. 2008;99: 489–498. 56. Thomas RM, Worswick S, Aleshin M. Retinoic acid for treatment of systemic sclerosis and morphea: A literature review. Dermatol Ther. 2017;30(2). doi: 10.1111/dth.12455. 57. Newland K, Marshman G. Success treatment of post-irradiation morphoea with acitretin and narrowband UVB. Australas J Dermatol. 2012;53:136–138. 58. Bellissen A, Lebas D, Wantz M et al. Efficacy of acitretin in IgA pemphigus. Ann Dermatol Venereol. 2013;140:793–796. 59. Monshi B, Richter L, Hashimoto T et al. IgA pemphigus of the subcorneal pustular dermatosis type. Successful therapy with a combination of dapsone and acitretin. Hautarzt. 2012;63:482–486. 60. Kim SK, Kim EH, Kang HY et al. Comprehensive understanding of idiopathic guttate hypomelanosis: clinical and histopathological correlation. Int J Dermatol. 2010;49:162–166. 61. Juntongjin P, Laosakul K. Idiopathic guttate hypomelanosis: A review of its etiology, pathogenesis, findings, and treatments. Am J Clin Dermatol. 2016;17:403–411. 62. Kim YJ, Lee DY, Lee JY, Yoon TY. Progressive macular hypomelanosis showing excellent response to oral isotretinoin. J Dermatol. 2012;39:937–938. 63. Damevska K, Pollozhani N, Neloska L, Duma S. Unsuccessful treatment of progressive macular hypomelanosis with oral isotretinoin. Dermatol Ther. 2017;30(5). doi: 10.1111/ dth.12514. 64. Sofen B, Prado G, Emer J. Melasma and post inflammatory hyperpigmentation: Management update and expert opinion. Skin Therapy Lett. 2016;21:1–7. 65. Gong Z, Lai W, Zhao G et al. Efficacy and safety of fluocinolone acetonide, hydroquinone, and tretinoin cream in Chinese patients with melasma: A randomized, double-blind, placebo-controlled, multicenter, parallel-group study. Clin Drug Investig. 2015;35:385–395. 66. Rendon M, Dryer L. Investigator-blinded, single-center study to evaluate the efficacy and tolerability of a 4% hydroquinone skin care system plus 0.02% tretinoin cream in mildto-moderate melasma and photodamage. J Drugs Dermatol. 2016;15:466–475. 67. Choi YL, Lee KJ, Kim WS et al. Treatment of extensive and recalcitrant viral warts with acitretin. Int J Dermatol. 2006;45:480–482. 68. Proietti I, Skroza N, Bernardini N et al. Acitretin in management of diffuse common warts: A case report. Dermatol Ther. 2011;24:581–583. 69. El-Khayat RH, Hague JS. Use of acitretin in the treatment of resistant viral warts. J Dermatolog Treat. 2011;22:194–196. Retinoids in Dermatology 70. Miljkovic J. A novel therapeutic approach to plane warts: A report on two cases. Acta Dermatovenerol Alp Pannonica Adriat. 2012;21:63–64. 71. Gupta R, Gupta S. Topical adapalene in the treatment of plantar warts; randomized comparative open trial in comparison with cryo-therapy. Indian J Dermatol. 2015;60:102. 72. Olguin-García MG, Jurado-Santa Cruz F, Peralta-Pedrero ML, Morales-Sánchez MA. A double-blind, randomized, placebocontrolled trial of oral isotretinoin in the treatment of recalcitrant facial flat warts. J Dermatolog Treat. 2015;26:78–82. 73. Wollina U, Steinbach F, Verma S, Tchernev G. Penile tumours: A review. J Eur Acad Dermatol Venereol. 2014;28:1267–1276. 74. Khullar G, Narang T, De D et al. Recalcitrant giant condyloma acuminatum treated successfully with a novel combination of Mycobacterium indicus pranii immunotherapy and acitretin. Int J STD AIDS. 2017;28:1155–1157. 75. Tian YP, Yao L, Malla P et al. Successful treatment of giant condyloma acuminatum with combination retinoid and interferon-γ therapy. Int J STD AIDS. 2012;23:445–447. 76. Yew YW, Pan JY. Complete remission of recalcitrant genital warts with a combination approach of surgical debulking and oral isotretinoin in a patient with systemic lupus erythematosus. Dermatol Ther. 2014;27:79–82. 77. Wollina U, Nenoff P, Haroske G, Haenssle HA. The diagnosis and treatment of nail disorders. Dtsch Arztebl Int. 2016;113:509–518. 78. Campione E, Paternò EJ, Costanza G et al. Tazarotene as alternative topical treatment for onychomycosis. Drug Des Devel Ther. 2015;9:879–886. 79. Gordon KA, Vega JM, Tosti A. Trachyonychia: A comprehensive review. Indian J Dermatol Venereol Leprol. 2011;77:640–645. 80. Kolbach-Rengifo M, Navajas-Galimany L, AranedaCastiglioni D, Reyes-Vivanco C. Efficacy of acitretin and topical clobetasol in trachyonychia involving all twenty nails. Indian J Dermatol Venereol Leprol. 2016;82:732–734. 81. Sherber NS, Hoch AM, Coppola CA et al. Efficacy and safety study of tazarotene cream 0.1% for the treatment of brittle nail syndrome. Cutis. 2011;87:96–103. 82. Deng H, Xiao H. The role of the ATP2C1 gene in HaileyHailey disease. Cell Mol Life Sci. 2017;74:3687–3696. 83. Berger EM, Galadari HI, Gottlieb AB. Successful treatment of Hailey-Hailey disease with acitretin. J Drugs Dermatol. 2007;6:734–736. 84. Hunt MJ, Salisbury EL, Painter DM, Lee S. Vesiculobullous Hailey-Hailey disease: Successful treatment with oral retinoids. Australas J Dermatol. 1996;37:196–198. 85. Sárdy M, Ruzicka T. Successful therapy of refractory Hailey-Hailey disease with oral alitretinoin. Br J Dermatol. 2014;170:209–211. 86. Vasudevan B, Verma R, Badwal S et al. Hailey-Hailey disease with skin lesions at unusual sites and a good response to acitretin. Indian J Dermatol Venereol Leprol. 2015;81:88–91. 87. Verma SB, Mittal A, Wollina U et al. Chanarin-Dorfman syndrome with rare renal involvement. Br J Dermatol. 2017;176:545–548. 88. Israeli S, Pessach Y, Sarig O et al. Beneficial effect of acitretin in Chanarin-Dorfman syndrome. Clin Exp Dermatol. 2012;37:31–33. 89. Srinivasaraghavan R, Krishnamurthy S, Chandar R et al. Acitretin-responsive ichthyosis in Chanarin-Dorfman syndrome with a novel mutation in the ABHD5/CGI-58 gene. Pediatr Dermatol. 2014;31:612–614. 27 Retinoids in Lymphoma Robert Duffy and Joya Sahu Introduction A rare disease entity, mycosis fungoides (MF) is the most common subtype of cutaneous T-cell lymphoma (CTCL) (1). Often misdiagnosed for years, MF is impossible to cure, short of a stem cell transplant. Therefore, treatment is palliative, aimed at ameliorating symptoms while achieving clinical remission. As common dermatologic staples used in acne and psoriasis, retinoids are the workhorse of cutaneous lymphoma physicians worldwide (2). Generally well tolerated with a manageable side effect profile, they activate apoptosis, incite cell cycle arrest, and change the cytokine profile in malignant T cells (3–6). Though the onset of action is delayed due to the nature of activation via nuclear ­transcription factors, the effects of retinoids are long lasting. Types of Cutaneous Lymphomas Primary cutaneous lymphomas can be divided into two broad groups based on the cell of origin: cutaneous T-cell lymphomas (CTCL) and cutaneous B-cell lymphomas (CBCL). From this division, many subtypes of CTCL and CBCL exist. The differences of each subtype of CTCL are based on clinical or histologic features, location of the neoplasm, type of T cell involved, or immunohistochemical staining profile. Folliculotropic MF, pagetoid reticulosis, and granulomatous slack skin are all examples of MF variants that present with a unique histology and ­clinical picture. Sézary syndrome is characterized by the presence of Sézary cells within the blood. Aggressive epidermotropic CD8+ cytotoxic T-cell lymphoma is characterized by a predominance of CD8+ T cells instead of the more common CD4+ T cells in MF. Lymphomatoid papulosis and cutaneous anaplastic large cell lymphoma are characterized by the presence of CD30 positivity. The types of CBCL are determined by various stains and cellular morphologies. Examples of these subtypes include cutaneous marginal zone lymphoma, cutaneous follicle center lymphoma, and cutaneous large B-cell lymphoma, leg type. The most recent classification of the major subtypes can be found in the 2018 update of the World Health OrganizationEuropean Organization for Research and Treatment of Cancer (WHO-EORTC) classification (7). CTCL represents 75%–80% of cutaneous lymphomas, while CBCL represents 20%–25%. The most common subtype of CTCL is MF, representing 50% of all CTCL cases (1). MF is a lymphoma that usually presents as scaling, erythematous patches and plaques on the hip-girdle region or in a bathing suit distribution, and is commonly associated with pruritus (8). Histologically, MF is characterized by a lymphocytic infiltrate normally present in a superficial perivascular pattern associated with varying degrees of epidermal involvement (none, interface, spongiotic, or psoriasiform). A classic finding is tagging at the dermalepidermal junction (DEJ) with varying degrees of lymphocytic epidermotropism. Although pathognomonic for MF, formation of Pautrier’s microabscesses is a relatively uncommon occurrence. The lymphocytes themselves are atypical, often increased in size, with irregularly contoured, hyperchromatic nuclei (9). Immunohistochemically, the lymphocytes are predominantly CD4+ T cells, with a high CD4 to CD8 ratio (10). As the disease progresses, loss of CD7-positivity with variable amounts of CD30-positivity can be seen (11). Although not imperative for a diagnosis, adjunctive molecular studies can show positivity of T-cell gene rearrangements (12). MF, often misdiagnosed initially due to lack of clear histopathological findings, is diagnosed following a clinicopathologic correlation (13). The severity of MF is determined through staging via the tumor-node-metastasis-blood (TNMB) classification system. The National Comprehensive Cancer Network (NCCN) guidelines lay out a comprehensive formula to determine a patient’s TNMB classification and staging. Tumor burden dominates staging early in the disease course. If a patient only has patch/plaque disease less than 10% of their body surface area (BSA), they have at least stage IA disease. If a patient only has patch/plaque disease greater than 10% of their BSA, they have at least stage IB disease. Presence of tumoral lesions automatically places them at least at IIB, and generalized erythroderma of greater than 80% BSA places a patient at least at IIIA. Stage IV is differentiated by whether the patient has high blood involvement (IVA1) or whether they have late lymph node involvement (IVA2). Finally, IVB is characterized by metastases. The nuances of this algorithm and more details on disease management can be found in the NCCN guidelines (13). Proposed Mechanism of Action The mechanism of action for retinoids and their therapeutic application in MF is incompletely understood. Some of the confusion stems from the enigma that surrounds key aspects of the pathogenesis of the disease entity itself, i.e., is MF a cancer of uncontrolled, enhanced mitosis or is it a cancer of impaired apoptosis? 171 172 CTCL cells express survivin, a protein that allows for evasion of apoptosis. It has been shown that bexarotene exposure reduces survivin levels, allowing for mediated apoptosis via activation of caspase-3 and the cleavage of poly-(ADP-ribose) polymerase (PARP). At bexarotene concentrations of 1 µM and 10 µM, apoptosis of CTCL cells is experimentally induced. With approved bexarotene dosages, plasma levels fall within the experimental concentration range needed for apoptosis to be stimulated, furthering this study’s clinical utility. Also, despite CTCL cells normally missing Fas/FasL, a common mediator of cell-induced apoptosis, retinoids activated this programmed cell death, revealing an alternative mechanism (3). In contrast, another view considers cell cycle arrest as the most likely mechanism behind bexarotene’s efficacy, where bexarotene exposure reduced the amount of intracellular cdc2(p34)-cyclin B1 complex. The repercussions of this decrease are widespread. Bexarotene stabilizes survivin, thus allowing for the decrease in this protein (potentially the mechanism behind the previous proposed mechanism of action). It also decreases the amount of active cdc2 kinase, which is involved in the progression of G2 phase (4). The same study also exhibited an increase in p21 with a decrease in cyclin D1, instrumental in the progression through G1. Thus, two major checkpoints are affected, S phase and M phase entry. This theory was then expanded to p53, a known cell-cycle regulator, which is an upstream signaling molecule to many of the proteins (p21, Bax, cdc2, and survivin) whose levels are affected by bexarotene. Finally, bexarotene was also shown to upregulate p73, a protein that shares many of the same functions as p53. This protein is also fairly stable in structure in CTCL, making it able to suppress tumor pathways despite possible mutations in p53. The ATM gene, upstream of these two molecules, is most likely the main molecule affected by bexarotene, because it is phosphorylated and activated by the drug (4). When these concepts are summarized, the two key mechanisms of action for bexarotene in MF may be activation of apoptosis and/or cell cycle arrest. Other mechanisms have been proposed regarding the role of retinoids and MF pertaining to the interplay between cytokines in the treatment of CTCL. For example, retinoid-exposed Langerhans cells are unable to activate T-cell populations, despite an elevated capacity, due to changes in class II major histocompatibility factors and CD11c expression. These changes are thought to potentially increase keratinocyte-derived immunosuppressive signaling (5). Another study demonstrated that retinoid exposure in doses from 1 to 10 ng/mLl induced production of interferon (IFN)-γ. It is known that CTCL has a Th2 cytokine profile and a depressed Th1 profile. The production of IFN-γ, a Th1 cytokine, suggests a shift in T-cell profile, with either a subsequent cytotoxic effect against CTCL cells or through activation of other cell death mechanisms (6). As more research is performed, the answer regarding the mechanisms behind the therapeutic effects of retinoids will be further elucidated. Treatment Non-Retinoid Treatment Options There are many therapy options that can be utilized in the treatment of CTCL, and they may be classified as either skin directed or systemic. The decision to start a skin-directed medication Retinoids in Dermatology TABLE 27.1 Medications Used in the Treatment of CTCL Skin-Directed Medications Topical steroids Topical retinoids Mechlorethamine gel Calcineurin inhibitors Imiquimod Phototherapy Total skin electron beam therapy Local radiation therapy Systemic Medications Retinoids Interferons (α and γ) Brentuximab Histone deacetylase inhibitors Methotrexate Pralatrexate Extracorporeal photopheresis Alemtuzumab Bortezomib Gemcitabine Mogamulizumab Pembrolizumab Pentostatin Temozolomide (13) versus a systemic medication is complicated by multiple variables. Clinical disease presentation is important in this decision, because most topical therapies will only affect the upper layers of the skin. If a patient presents with tumoral lesions, a systemic approach may be more suitable. Body surface area is also a consideration because with a higher percentage of body affected, difficulty applying topical medication increases, overall decreasing compliance. Finally, the inherent features of the tumor, such as histologic variants and associated prognosis, will affect how aggressive the treatment should be. Most patients begin treatment with skin-directed therapy. This can reduce disease burden, but more importantly, will reduce overall symptomatology, increasing the patient’s overall quality of life. The skin-directed and systemic medications that can be used for CTCL have been listed in Table 27.1. Retinoid Treatment Options Topical Retinoids Three topical retinoids that have been studied for treating CTCL include: • Bexarotene • Tazarotene • Alitretinoin Table 27.2 lists the treatment modalities used for each of these topicals in the literature. Of the three retinoids, only topical bexarotene 1.0% is currently FDA approved for the treatment of CTCL. 173 Retinoids in Lymphoma TABLE 27.2 Topical Treatment Modalities Medication Name Author (Year of Publication) Type of Article (Number of Patients) Bexarotene Breneman D et al. (2002) (14) Prospective, phase I and II trials (67) Heald P et al. (2003) (15) Walling HW et al. (2008) (16) Prospective, phase III trial (50) Case study (1) Tazarotene Apisarnthanarax N et al. (2004) (17) Prospective pilot study (20) Alitretinoin Bassiri-Tehrani S et al. (2002) (18) Case study (1) Dosage Used Patient Response (Change in BSA) Escalated dose q2wks: 0.1% BID, 0.5% QD, 0.5% BID, 1.0% BID, then optionally TID and QID 1% gel applied every day weekly increasing applications/day to QID max, as tolerated 1% gel applied every other day for 2 weeks, followed by twice daily on weekdays for 12 weeks 0.1% gel QD for 24 weeks, with topical steroids 63% of patients had 50% or better response, 21% complete response and 42% partial response Median BSA at baseline was 9%, by week 44, it is 4.5% Less plaque induration and improvement in follicular plugging 0.1% gel BID to tumor, in addition to acitretin 35 mg QD and PUVA twice weekly Topical bexarotene has the most data supporting its efficacy and has been shown in multiple clinical trials to be a reliable and effective treatment modality for early stage MF. Patients can be given bexarotene gel 1.0% one to four times daily for treatment of patch and plaque CTCL. In the phase 1 and 2 trials of bexarotene, 67 adults with early stage CTCL were given incrementally increasing doses of bexarotene to test for tolerance. Most patients tolerated 1.0% gel twice daily, with an overall response rate of 63% and a clinical complete response of 21%. One striking feature was that patients who had never been treated prior to starting bexarotene had a better response rate than those who had previously been treated (14). In another study, patients with this medication regimen had responses to bexarotene gel recorded using various metrics. Only patients with stage IA or IB disease responded at 64% and 50%, respectively. Although the patients with stage II disease no longer held response to intervention, with only 3 patients in stage IIA and IIB compared to 27 patients in IA and IB, comparison between the two stages is difficult. When analyzing overall response, attention should be given to the length of time until response, measured from the initiation of medication usage until the patient obtained 50% clearance. This ranged from 28 to 504 days, with a projected median time to response being 142 days (15). A positive response was also shown in folliculotropic MF (FMF). In one case study, this disease entity, which has the potential to be more aggressive, developed in a 73-year-old man. He had developed erythematous comedonal plaques and follicular plugging on indurated lesions and was determined to be stage IA. After 12 weeks of treatment, there was significant reduction in lesion severity. The patient obtained partial remission with continued medication usage over the next 4 months (16). FMF shares clinical and histological features with acne, so it is not surprising that retinoids have been shown to be beneficial. In our experience, topical retinoids can be superior to other commercially available topical therapies for challenging, refractory cases of FMF. Tazarotene has been shown in a prospective study to have good efficacy in patients with stable or treatment refractory disease with a body surface area of less than 20%. Tazarotene gel 0.1% was applied to 20 patients once daily for 24 weeks. Of their patient 58% achieved at least moderate improvement in BSA, 35% of 99 index lesions cleared completely Complete remission population, 19 patients received treatment and 16 completed at least 12 weeks of treatment. One patient withdrew from the study at 8 weeks, one developed progressive disease on his body while treating just his hands and feet, and one patient developed allergic contact dermatitis to the gel. Of the 19 treated patients, 11 patients (58%) had at least moderate (>50%) improvement in their BSAs, and 35% of the 99 index lesions cleared. There were statistically significant changes in all categories of Composite Assessment of Index Lesion Severity (CAILS) for index lesions and an overall statistical difference in BSA of 22% (17). Alitretinoin 0.1% has been used for treatment of a tumor lesion in combination with systemic acitretin 35 mg daily and psoralen-ultraviolet A (PUVA) twice weekly. When this topical treatment was applied to the tumor twice daily, after 6 weeks, a 6-centimeter plaque with a 1-centimeter black eschar appeared where the tumor had been. Other tumoral lesions without treatment remained. As the eschar re-epithelialized, resolution of the ulcer was noted. Although this is a single case report, resolution of the solitary treated lesion in a background of residual, stable tumoral lesions shows potential therapeutic application as a topical therapy for tumors (18). Topical retinoids are well known for generating irritant contact dermatitis, most commonly presenting as localized erythema, an eczematous eruption, and minor burning and irritation. Clinicians can use the findings of slight irritation and erythema as indicators of patient compliance. Patients will note that often bexarotene-associated irritant contact dermatitis is dose or application dependent. Patients may opt to apply medication at less than the recommended dosing of four times a day to decrease irritation, i.e., twice-a-day application, with acceptable clinical results. Another method to reduce irritation is to apply the retinoid in combination with a topical, usually mid- to high-potency, steroid. Rarely, off-label usage of either topical adapalene (over-the-counter) or tretinoin is recommended if the patient finds topical bexarotene too irritating, is concerned about the potential side effects, or finds the regimen cost prohibitive. We also use topical bexarotene gel not only to treat MF, but also to treat FMF and lymphomatoid papulosis. Treatment should be titrated for patient comfort and to maximize compliance. Once the eruption is cleared, topical bexarotene can 174 slowly be tapered to a maintenance regimen, i.e., biweekly or weekly application. Although considered to be off-label usage, topical bexarotene gel also can be used as a maintenance therapy, following consolidation treatment with total skin electron beam therapy (TSEBT), and in elderly patients with numerous comorbidities unable to tolerate systemic medications. This regimen has the potential to increase disease-free survival after obtaining clinical remission from TSEBT prior to recurrence of disease. Retinoids in Dermatology Systemic retinoids were first used in the treatment of CTCL in 1983, when isotretinoin was given to four patients with doses ranging from 1 to 3 mg/kg/day that produced 50%–100% lesion reduction (19). Although a small case series, this finding introduced retinoids as a modality for treating CTCL and subsequently stimulated the use of additional retinoids. side effects may be peripheral edema and nausea, with pancreatitis rarely occurring but also being avoidable by monitoring triglyceride levels. Bexarotene is usually dosed at 300 mg/m2 with initial dosing starting at 150 mg/m2 po daily for 3–4 weeks, then increasing to 300 mg/m2 po daily. Levothyroxine, fenofibrate, and atorvastatin (if indicated) should be concomitantly initiated. Providing detailed take-home instructions and adequate in-visit counseling greatly increases patient compliance. Patients are instructed that the course of bexarotene will continue for 1 year prior to being eligible for tapering, with periodic clinical assessments every 3–4 months. Should the patient flare up during this time frame, we recommend increasing the dosage to 450 mg/m2 po daily as tolerated. If the patient achieves partial remission/clinical remission following the 1-year period, the bexarotene dose is decreased to 75 mg/m2 po daily as maintenance therapy. Other skin-directed therapies can be applied simultaneously for a synergistic effect while taking bexarotene. Bexarotene Isotretinoin Multiple randomized controlled trials have demonstrated bexarotene’s efficacy as a first-line therapy for MF with response rates similar to those of other stand-alone agents used to treat MF but with more tolerable side effects (20–22). In addition, bexarotene can be utilized in combination with multiple therapeutic options for MF, i.e., PUVA, narrow-band ultraviolet B (nb-UVB), and extracorporeal photopheresis (ECP), often with higher response rates than bexarotene alone (23–26). Combining multiple therapies with different mechanisms of action can have an overall better response due to synergistic effects (27). Our initial choice of retinoids is oral bexarotene for patients with a moderate to high burden of disease, B0 to B1 blood involvement, difficult to treat locations, or FMF. We also use bexarotene as a maintenance therapy following disease consolidation with TSEBT. We have found that starting a systemic treatment after clearance from TSEBT allows for a longer time prior to disease recurrence. The side effects are generally limited and tolerable when compared to other systemic therapies. Central hypothyroidism occurs in approximately 29%−53% of patients (28). Before initiating treatment, a baseline thyroid-­ stimulating hormone (TSH) and a free T4 (thyroxine) level should be obtained; however, only T4 levels should be monitored as treatment progresses. Because bexarotene causes central hypothyroidism, TSH levels will always be low due to the druginduced decrease in production of thyroid-releasing hormone. To combat this hypothyroidism, we recommend starting all patients on levothyroxine 50 µg daily at the beginning of therapy and titrating upward as necessary depending on dosage adjustments and T4 levels. Bexarotene can also cause hyperlipidemia and hypercholesterolemia (28). Prior to initiating oral bexarotene, baseline lipid levels should be established. If there are abnormalities, they should be corrected prior to initiation. Once oral bexarotene has begun, close monitoring should occur. The most common lipid abnormality is hypertriglyceridemia at 79% (28). To combat this, patients are started on fenofibrate. If LDL cholesterol levels also rise, atorvastatin can be initiated; however, we preemptively initiate atorvastatin 40 mg at baseline. Finally, with the possibility of hepatotoxicity, liver enzymes should be monitored. Additional Isotretinoin has been established as a therapeutic option for the treatment of MF in various stages and presentations, either as a sole agent or combined with an adjuvant therapy, such as PUVA (29–34). Unfortunately, increasing data demonstrate reduced activity (33) and commonly pronounced mucocutaneous side effects. This leads to many patients discontinuing this retinoid or decreasing the dosage below therapeutic levels (35). While treating acne, a usual regimen for isotretinoin is 120– 150 mg/kg in divided doses over several months, often initially dosed at 40 mg/day for 30 days. In the treatment of MF, isotretinoin can commonly be initiated at lower doses, starting at 20 mg/ day. Isotretinoin dosing can be uptitrated per each individual patient’s side effect tolerance and laboratory testing levels. If the patient sustains partial remission or obtains near or complete clinical remission, then the dosing can remain stable for a period of 6–12 months prior to tapering. Isotretinoin is not considered first-line therapy due to its efficacy in only select patients, rigorous enrollment process, and the multitude of side effects. We only prescribe isotretinoin for compliant patients in certain circumstances, i.e., in challenging cases of FMF, in patients wishing to conceive in the near future, or in patients who fail to tolerate oral bexarotene. Systemic Retinoids Acitretin Acitretin is generally a well-tolerated medication, most commonly prescribed for severe psoriasis. Acitretin is available in 10 mg or 25 mg capsules and is usually dosed at 0.25–1 mg/kg/ day after a meal for the treatment of psoriasis. Dosed similarly to isotretinoin, it is usually initiated at lower levels for MF patients and likewise clinically titrated. The scant evidence that is available to support acitretin use as a sole oral agent in MF suggests that acitretin be used in conjunction with adjuvant skin-directed therapies including topical corticosteroids, topical nitrogen mustard, and phototherapy in patients with early-stage disease (36). Because acitretin has yet to become an approved treatment for MF, it is not a commonly used first line agent. We occasionally resort to this agent in recalcitrant cases of FMF, in erythrodermic patients, or as an alternative systemic agent to bexarotene, either alone or in conjunction with isotretinoin due to its limited efficacy. 175 Retinoids in Lymphoma TABLE 27.3 Dosages of Topical Medications Retinoid Bexarotene Tazarotenea Alitretinoina a Dose Apply to lesions in increasing increments weekly: every other day, every day, twice daily, three times daily, four times daily Apply to lesions daily Apply to lesions twice daily Case studies. REFERENCES TABLE 27.4 Dosages of Systemic Medications Retinoid Bexarotene Isotretinoin Acitretin Alitretinoina a studied. Other retinoid options will be utilized if a patient cannot tolerate bexarotene or as adjuvant therapy in specific clinical scenarios, such as FMF. Topical retinoids are usually utilized for patients with low disease burden. Oral retinoids are usually used for patients with greater disease burden. Both can be used as maintenance methods following consolidation therapy. Finally, retinoids can often be combined with other treatment modalities for a synergistic effect. Dose 150–300 mg daily, can be increased to 400 mg daily for refractory cases 1–2 mg/kg daily 10–50 mg (mode: 25 mg) daily, titrated to 10 mg daily or 25 mg three times weekly for maintenance 30 mg daily Case study. Alitretinoin Because alitretinoin is an agonist of both the RARs and the RXRs, there may be an additional benefit to this medication’s use. No prospective randomized-controlled clinical trials exist to support the use of alitretinoin; however, limited case reports and case series suggest that alitretinoin may be beneficial in select patients (37–39). Prospective studies with less confounding variables will be needed to further prove the efficacy of using alitretinoin for CTCL. Generalized Retinoid Dosing Information Based on the information provided in this chapter, dosing can be extrapolated for the various retinoid treatments. The level of confidence in the dosing from the literature should be based upon the overall validity of the studies. Dosing from a prospective study is more valid and thus more clinically relevant than that from a case study (which will be noted by an “a”). Table 27.3 shows the dosing for topical retinoids in the treatment of MF; Table 27.4 shows the dosing for systemic retinoids in the treatment of MF. Prevention No data currently exist regarding the use of retinoids as chemoprophylactics in the prevention of lymphoma. Conclusions Retinoids are an available and effective treatment modality for MF. Because of the relatively low side effect profile in addition to the overall effectiveness, the authors often utilize them as a first-line treatment. Bexarotene is typically the first choice because it is FDA approved and has been the most extensively 1. Willemze R, Jaffe ES, Burg G et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3768–3785. 2. Zaenglein AL, Pathy AL, Schlosser BJ et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74:945–973.e33. 3. Zhang C, Hazarika P, Ni X et al. Induction of apoptosis by bexarotene in cutaneous T-cell lymphoma cells: Relevance to mechanism of therapeutic action. Clin Cancer Res. 2002;8:1234–1240. 4. Nieto-Rementería N, Pérez-Yarza G, Boyano MD et al. Bexarotene activates the p53/p73 pathway in human cutaneous T-cell lymphoma. Br J Dermatol. 2009;160:519–526. 5. Meunier L, Bohjanen K, Voorhees JJ et al. Retinoic acid upregulates human langerhans cell antigen presentation and surface expression of HLA-DR and CD11c, a β2 integrin critically involved in T-cell activation. J Invest Dermatol. 1994;103:775–779. 6. Rook AH, Kubin M, Fox FE et al. The potential therapeutic role of interleukin-12 in cutaneous T-cell lymphoma. Ann N Y Acad Sci. 1996;795:310–318. 7. Willemze R, Cerroni L, Kempf W et al. The 2018 update of the WHO-EORTC classification for primary cutaneous ­lymphomas. Blood. 2019;133:1703–1714. 8. Willemze R. Cutaneous T-cell lymphoma. In: Jean L. Bolognia, Julie V. Schaffer, and Lorenzo Cerroni, editors. Dermatology. 4th ed. Philadelphia, PA: Elsevier Saunders, 2018; pp. 2131–2132. 9. Shapiro PE, Pinto FJ. The histologic spectrum of mycosis fungoides/Sézary syndrome (cutaneous T-cell lymphoma): A review of 222 biopsies, including newly described patterns and the earliest pathologic changes. Am J Surg Pathol. 1994;18:645–667. 10. Massone C, Crisman G, Kerl H et al. The prognosis of early mycosis fungoides is not influenced by phenotype and T-cell clonality. Br J Dermatol. 2008;159:881–886. 11. Duvic M, Tetzlaff MT, Gangar P et al. Results of a phase II trial of brentuximab vedotin for CD30+ cutaneous T-cell lymphoma and lymphomatoid papulosis. J Clin Oncol. 2015;33:3759–3765. 12. Bignon YJ, Roger H, Souteyrand P et al. Study of T-cell antigen receptor gene rearrangement: A useful tool for early diagnosis of mycosis fungoides. Acta Derm Venereol. 1989;69:217–222. 13. Mycosis Fungoides/Sèzary Syndrome (Version 2.2019) [Internet]. 2019 [cited May 1, 2019]: https://www.nccn.org/ professionals/physician_gls/pdf/primary_cutaneous.pdf. 14. Breneman D, Duvic M, Kuzel T et al. Phase 1 and 2 trial of bexarotene gel for skin-directed treatment of patients with cutaneous T-cell lymphoma. Arch Dermatol. 2002;138:325–332. 176 15. Heald P, Mehlmauer M, Martin AG et al. Topical bexarotene therapy for patients with refractory or persistent early-stage cutaneous T-cell lymphoma: Results of the phase III clinical trial. J Am Acad Dermatol. 2003;49:801–815. 16. Walling HW, Swick BL, Gerami P et al. Folliculotropic mycosis fungoides responding to bexarotene gel. J Drugs Dermatol. 2008;7:169–171. 17. Apisarnthanarax N, Talpur R, Ward S et al. Tazarotene 0.1% gel for refractory mycosis fungoides lesions: An open-label pilot study. J Am Acad Dermatol. 2004;50:600–607. 18. Bassiri-Tehrani S, Cohen DE. Treatment of cutaneous T-cell lymphoma with alitretinoin gel. Int J Dermatol. 2002;41:104–106. 19. Kessler JF, Meyskens FL, Levine N et al. Treatment of cutaneous T-cell lymphoma (mycosis fungoides) with 13-cis-retinoic acid. Lancet. 1983;1:1345–1347. 20. Duvic M, Martin AG, Kim Y et al. Phase 2 and 3 clinical trial of oral bexarotene (Targretin capsules) for the treatment of refractory or persistent early-stage cutaneous T-cell lymphoma. Arch Dermatol. 2001;137:581–593. 21. Duvic M, Hymes K, Heald P et al. Bexarotene is effective and safe for treatment of refractory advanced-stage cutaneous T-cell lymphoma: Multinational phase II-III trial results. J Clin Oncol. 2001;19:2456–2471. 22. Abbott RA, Whittaker SJ, Morris SL et al. Bexarotene therapy for mycosis fungoides and Sézary syndrome. Br J Dermatol. 2009;160:1299–1307. 23. Whittaker S, Ortiz P, Dummer R et al. Efficacy and safety of bexarotene combined with psoralen-ultraviolet A (PUVA) compared with PUVA treatment alone in stage IB-IIA mycosis fungoides: Final results from the EORTC cutaneous lymphoma task force phase III randomized clinical trial (NCT00056056). Br J Dermatol. 2012;167:678–687. 24. Lokitz ML, Wong HK. Bexarotene and narrowband ultraviolet B phototherapy combination treatment for mycosis fungoides. Photodermatol Photoimmunol Photomed. 2007;23:255–257. 25. D’Acunto C, Gurioli C, Neri I. Plaque stage mycosis fungoides treated with bexarotene at low dosage and UVB-NB. J Dermatolog Treat. 2010;21:45–48. 26. Tsirigotis P, Pappa V, Papageorgiou S et al. Extracorporeal photopheresis in combination with bexarotene in the treatment of mycosis fungoides and Sézary syndrome. Br J Dermatol. 2007;156:1379–1381. 27. Talpur R, Ward S, Apisarnthanarax N et al. Optimizing bexarotene therapy for cutaneous T-cell lymphoma. J Am Acad Dermatol. 2002;47:672–684. Retinoids in Dermatology 28. Bexarotene. In: Lexi-Drugs Online Database [database on the internet]. Riverwoods, (IL): Lexicomp. Wolters Kluwer Health, Inc., 2019 (updated February 22, 2019; cited February 22, 2019). Available from: http://online.lexi.com. Subscription required to view. 29. Warrell RP, Coonley CJ, Kempin SJ et al. Isotretinoin in cutaneous T-cell lymphoma. Lancet. 1983;2:629. 30. Thomsen K, Molin L, Volden G et al. 13-cis-retinoic acid effective in mycosis fungoides. A report from the Scandinavian mycosis fungoides group. Acta Derm Venereol. 1984;64:563–566. 31. Kessler JF, Jones SE, Levine N et al. Isotretinoin and cutaneous helper T-cell lymphoma (mycosis fungoides). Arch Dermatol. 1987;123:201–204. 32. Neely SM, Mehlmauer M, Feinstein DI. The effect of isotretinoin in six patients with cutaneous T-cell lymphoma. Arch Intern Med. 1987;147:529–531. 33. Molin L, Thomsen K, Volden G et al. Oral retinoids in mycosis fungoides and Sézary syndrome: A comparison of isotretinoin and etretinate. Acta Derm Venereol. 1987;67:232–236. 34. Thomsen K, Hammar H, Molin L et al. Retinoids plus PUVA (RePUVA) and PUVA in mycosis fungoides, plaque stage. A report from the Scandinavian Mycosis Fungoides Group. Acta Derm Venereol. 1989;69:536–538. 35. Olsen EA, Hodak E, Anderson T et al. Guidelines for phototherapy of mycosis fungoides and Sezary syndrome: A consensus statement of the United States Cutaneous Lymphoma Consortium. J Am Acad Dermatol. 2016;74:27–58. 36. Cheeley J, Sahn RE, DeLong LK et al. Acitretin for the treatment of cutaneous T-cell lymphoma. J Am Acad Dermatol. 2013;68:247–254. 37. Molin S, Ruzicka T. Possible benefit of oral alitretinoin in T-lymphoproliferative diseases: A report of two patients with palmoplantar hyperkeratotic-rhagadiform skin changes and mycosis fungoides or Sézary syndrome. Br J Dermatol. 2009;161:1420–1422. 38. Coors EA, von den Driesch P. Treatment of 2 patients with mycosis fungoides with alitretinoin. J Am Acad Dermatol. 2012;67:e265–e267. 39. Kapser C, Herzinger T, Ruzicka T et al. Treatment of cutaneous T-cell lymphoma with oral alitretinoin. J Eur Acad Dermatol Venereol. 2015;29:783–788. 28 Retinoids in Cutaneous Chemoprophylaxis Robert Duffy and Joya Sahu Introduction Retinoids were first linked to cancer in 1926, when mice fed vitamin A-deficient diets developed gastric carcinomas (1). Since then, retinoids have been found to affect the development of many types of cancers, including those of the skin. Although early studies looking at retinoids for the treatment of pre-existing cancers were relatively unfruitful, one study found a relationship between isotretinoin usage and a reduction in new skin cancer development (2–4). This finding has motivated many to quantify further the effectiveness of retinoids in the prevention of skin cancers. This chapter highlights the proposed mechanism of retinoid action in chemoprophylaxis and gives health-care providers practical information from the literature regarding successful retinoid chemoprophylactic dosages, time frames used within the studies, and the side effects experienced by patients. against tumor development (8). Numerous other studies have also shown that vitamin A derivatives are potent agents against cancer development (7,9). Finally, retinoids can potentially damage subclinical squamous cell carcinoma (SCC) cells. Studies found that N-(4-hydroxy­ phenyl)retinamide (4HPR), an artificial retinoid, promotes apoptosis through the creation of reactive oxygen species (ROS) (10). This was shown to be in part due to the ability of 4HPR to promote mitochondrial permeability transition, the process of mitochondrial change that initiates the cascade of apoptosis through caspase activation, producing superoxide, an ROS, and disrupts mitochondrial membrane potentials, reducing organelle function (11,12). One study found that in SCC cells, 4HPR was able to induce cell death by enzymatically producing hydroperoxide, most likely in either Complex I or III of the e­ lectron transport chain (13). Non-Melanoma Skin Cancer Proposed Mechanism of Action Topical Retinoids Scant data exists on how retinoids express their effects as chemoprophylactic agents for cutaneous cancers. Early studies using isotretinoin as chemoprophylaxis in patients with xeroderma pigmentosum showed antitumor effects quickly upon starting and stopping treatment. This may be due to the rapidity of action and inaction when the medicine began and ended; it can be assumed the retinoid is affecting a late stage of cancer development, not preventing or repairing DNA damage (5). This theory involving retinoids protecting cells from the later stages of carcinogenesis was then furthered by studies exhibiting a reduction in malignant transformation induced by UV radiation (6). Other mechanisms for the potential protective abilities of retinoids show activity at multiple stages of tumor development. Retinoids have previously been shown to alter carcinogen metabolism, inhibiting DNA damage and thus quelling the earliest stages of carcinogenesis (7). A large study demonstrated that retinoic acid can also act as a potent antioxidant. Pretreatment with retinoic acid was shown to recover levels of glutathione and its metabolites, both potent antioxidants, highlighting its own antioxidant abilities. This was further underscored by its ability to elevate levels of glutathione-S-transferase, quinone reductase, and xanthine oxidase, all detoxifying enzymes. Finally, the study showed retinoic acid’s ability to inhibit ornithine decarboxylase and incorporate (3H) ­thymidine in DNA, which both protect It is a well-established fact that UV radiation exposure has been associated with the damage and aging of skin and the development of skin cancers. As a result, many medications have been investigated to prevent these natural consequences of exposure. Retinoids have been utilized for this purpose with great success, with the first report of photodamage reversal in 1986 and the FDA approving tretinoin (Renova) 0.02% emollient cream in 2004 for the same purpose (14,15). Due to the intimate relationship between actinic damage and skin cancer development, it is no surprise that long-term (mean: 2.3 years) tretinoin 0.05% treatment was shown to reduce histologic epidermal cellular atypia (16). For basal cell carcinomas (BCCs), long term tazarotene 0.1% gel was found to be effective at treating 30%–50% of sporadic BCCs (17). This is a promising finding that reiterates previous studies showing 16 of 30 sporadic BCCs treated after 8 months of tazarotene treatment (18). A mouse model using Ptch1+/− mice (predisposed to develop BCCs) also supports this by showing an overall reduction in the concentration of microscopic BCCs per centimeter of skin on tazarotene-treated mice in comparison to vehicle-control treated ones (19). Variable response to treatment is hypothesized to be due to the degree of partial or total loss of RAR-γ expression, a main receptor of a­ ctivity for tazarotene (20). 177 178 Despite these promising findings, results for retinoids have been mixed regarding the clinical reduction of clinically apparent atypia, with some studies even showing increased carcinogenesis. One study analyzing long-term topical application of retinaldehyde (0.05%) found that there was no difference in the development of actinic keratoses between the treatment and control groups (21). This was a disappointing result considering the low risk of irritant contact dermatitis that accompanies this weaker retinoid, but it is also unsurprising when one considers the dose-dependent effect of retinoids for chemoprophylaxis that has already been discussed. In another hairless mouse study, it was found that the topical application of retinoic acid increased the number of tumors and decreased the length of time for tumor emergence following UV exposure (22). Although there is controversial evidence when discussing all retinoids, the literature regarding tretinoin and tazarotene as topical chemoprophylaxis against non-melanoma skin cancers (NMSCs) seems promising As more data become available, subtle differences between the various retinoids may shed more light as to why some are more effective than others in this pursuit. Systemic Retinoids Although topical retinoids have a more tolerable side effect profile, as one study reports, “local irritation and the lack of patient motivation” limit the effectiveness in usage (23). Due to this, many studies exploring the potential for chemoprophylaxis have analyzed systemic retinoid therapy. Psoralen ultraviolet-A (PUVA)-treated patients have developed many skin cancers due to the increased level of UV radiation to which they are exposed. In one study, 135 patients treated with PUVA and concurrent systemic retinoids were found to have a 20% reduction of SCC incidence in long-term follow-up after adjusting for other significant predictors of SCC occurrence. The cohort was administered either etretinate or acitretin, with 95% and 90% of each group, respectively, receiving dosages of 25 mg/ day or more. Upon discontinuation of the retinoid, levels of SCC incidence quickly rose to levels above those preceding the retinoid use. The authors conclude that the chemoprophylactic usage of retinoids is only present while actively taking the medication as directed and not after discontinuation or sporadic usage. One particularly striking finding from this study concerns retinoid use causing no statistically significant reduction in the incidence of BCCs (24). The previous study analyzed patients at high risk for cancer development due to their carcinogenic exposures from psoriasis treatments. Another study analyzed patients on BRAF inhibitors (vemurafenib or dabrafenib) given acitretin (10–50 mg/day) therapy to see if the rate of verrucal keratoses and SCC would decline. Prior to starting therapy, eight patients had 24 SCCs removed. Upon starting therapy, two of the eight patients had five lesions removed (25). This reduction, despite being a small sample size, exhibits the recurring theme of the effectiveness of retinoid chemoprophylaxis in patients at high risk for developing NMSCs. When the level of risk diminishes, so too do the benefits of retinoid chemoprophylaxis. Patients with moderate risk for NMSC given low-dose isotretinoin for chemoprophylaxis did not exhibit significant reduction in cancer risk (26,27). One of these two studies concluded that currently, the risk of side effects from Retinoids in Dermatology isotretinoin far outweighed any theoretical benefit for moderaterisk patients (26). The dichotomy between the results in patients at high risk versus those with low risk for NMSC sheds light on the clinical decision-making dilemma that a dermatologist or oncologist will encounter. At present, no treatment algorithm exists. The treating physician must first establish the level of risk of developing NMSC (low, moderate, and high) and identify evidence in the literature supporting use of a chemoprophylactic retinoid. Next, one must determine whether the risk of side effects outweighs the risk of developing skin cancer. In summary, physicians must use their clinical judgment on a case-by-case basis to determine what is best for individual patients when retinoid chemoprophylaxis is being considered. High-Risk Patient Populations Xeroderma Pigmentosum Some of the earliest studies analyzing the efficacy of retinoids in the prevention of NMSC were in patients with xeroderma pigmentosum (XP). XP is an autosomal-recessive condition in which patients are unable to repair UV-induced DNA damage (28), predisposing them to developing large amounts of actinic skin damage with subsequent exuberant carcinogenesis. Patients with XP are at extremely high risk of developing aggressive and early skin cancers, so developing a prophylactic medication is a high priority for patient safety. An initial study of five XP patients analyzed the amount of NMSCs that developed 2 years prior to starting isotretinoin and for 2 years while taking isotretinoin. The authors observed that before the intervention, the patients had 121 cancers and while taking isotretinoin, developed 25 (a 63% reduction in cancers). The reduction could be attributed to the high dose of isotretinoin (2 mg/kg/day) (29). This study was furthered by many of the same authors who followed it with a low-dose regimen (0.5 mg/kg/day) for patients after completion of the first high-dose portion. Two additional patients were included in the low-dose portion of the study who were initially in the high-dose patient group but were unable to tolerate the therapy. From this study, the authors found that response was dose-dependent (5). This study shows that the chemoprophylactic dose of isotretinoin in XP patients must be titrated up from a low-dose regimen, ensuring that patients will receive the maximal prophylactic benefits with the least likelihood of developing side effects. Transplant Population Because transplant patients receive immunosuppressive therapy to prevent organ rejection, they are also at an increased risk for developing NMSCs. A meta-analysis of nine studies (111 transplant patients) found that oral retinoids could be used to decrease the incidence of NMSC. Unfortunately, they were unable to draw conclusions as to the dosages or which retinoid was best, but more recent studies are able to make suggestions as to an ­appropriate algorithm for treatment (30). One review concluded that acitretin should be initiated for patients at high risk for the development of NMSC considering it has been shown in previous studies to reduce lesions and is 179 Retinoids in Cutaneous Chemoprophylaxis FDA approved for overlapping application (psoriasis treatment in patients receiving concurrent PUVA) (31). Potential dosing regimens to administer based on reported studies include 30 mg/ day for 6 months, 0.3 mg/kg/day or an escalation approach of 0.25 mg/kg every other day for 1 month, followed then by 0.25 mg/kg/day for 1 month, with the dosage plateauing in the third month at 0.5 mg/kg/day (as long as it does not exceed 175 mg/week) (32–34). The authors then suggest the use of bexarotene as a second-line agent for this population. They argue that bexarotene is better for patients who are unable to tolerate acitretin (RXR receptor binding leads to less xerosis and desquamation), who want to become pregnant within 2 years (must be off medication for 1 month prior to contraception), or who have impaired kidney function (minimal renal excretion). The decision to endorse bexarotene is based on anecdotal evidence of efficacy in a patient with keratoacanthoma-type SCC post treatment with sorafenib. The dosage the authors use in this case is 150 mg/day, increased to 225 mg/day after 3 months, resulting in total treatment of all lesions present (31). Melanoma Because malignant melanoma is such a devastating and deadly cancer with an estimated 7320 deaths in 2019, efforts have been made to find potential chemoprophylactic agents to prevent its development (35). Topical Retinoids There have been a few trials evaluating the efficacy of topical retinoids in the prevention of malignant melanoma (MM). In one study, topical tretinoin was used for three patients with dysplastic nevus syndrome (potential MM precursor). Upon histologic examination post-treatment, regression to benign compound nevi occurred in some subjects (36). A clinical trial using tretinoin 0.05% once daily under occlusion or twice daily for 4 months caused dysplastic nevi to either disappear or be significantly reduced/develop benign characteristics in 21 patients (37). Another smaller study of five men with tretinoin 0.05% once daily titrated, as tolerated, up to 0.1% twice daily, found that when applied to half of each participant’s backs, the side treated had clinically significant resolution. The treated side had 4 out of 16 nevi meet histologic criteria for dysplasia, while 13 of the 16 untreated met the criteria (38). In contrast, one study identified no difference in histologic atypia between tretinoin 0.1%, tretinoin 0.1% with 1% hydrocortisone, and placebo under occlusion (39). Due to the irritation caused, there was difficulty for patients treating large portions of their bodies or nevi and potentially low compliance. As a result, the feasibility of topical chemoprophylaxis is limited. Systemic Retinoids There are many studies that look at dietary retinol intake or supplementation to determine whether they can be used as easy and affordable ways to prevent melanoma with a low side effect profile. One study showed that retinol supplementation was inversely associated with melanoma risk. Although not statistically significant, there was an observed increased risk reduction in women, although it was not able to be determined if this was due to sampling, known better outcomes in women, or differences in gender use and storage of retinol (40). One large study with a population of 162,000 women who took vitamin A supplementation in addition to normal dietary intake found a reduction in melanoma risk for low-risk individuals (41). This information differs from the information about NMSCs, which found benefit in high-risk populations. Previous studies have shown similar results for the intake of vitamin A or derivatives, such as carotenes, in the reduction of melanoma incidence. One study using retrospective data collection via food survey found patients with dietary intake of alpha- and beta-carotenes at a decreased risk of developing melanoma (42). The data are directly contradicted when comparing these results to other population studies looking at the risk of melanoma and vitamin A consumption. Many studies found there to be no difference between the two groups on consumption of vitamin A and melanoma risk (43–47). As more information is collected, the medical community will further understand if dietary supplementation with vitamin A prevents melanoma or not. There is little literature supporting the use of pharmacologic retinoids (acitretin, isotretinoin, bexarotene, alitretinoin) for prophylaxis against malignant melanoma. This is in comparison to the relatively large amount of research on the use of systemic retinoids in the prevention of NMSC. The reason lies within the risk-versus-benefit analysis. Although MM can be a more serious and life-threatening diagnosis, in general, than SCC or BCC, its incidence is extremely low in comparison. As of 2019, MM was the fifth most common cancer to be diagnosed, representing 5.5% of new cancer diagnoses. Despite the number of new diagnoses increasing, the trend in mortality is decreasing (35). This is due to better screening based on population studies determining risk factors, prompt diagnosis using technologies that aid in diagnosis (i.e., dermatoscopy), and effective treatment modalities. Because melanoma has such a low incidence in comparison to NMSC, which represents the highest number of new cancer diagnoses and can be associated with high levels of morbidity with each diagnosis, the risks of starting a retinoid to prevent melanoma systemically far outweigh the potential benefits (35). Conclusions Retinoids have been studied for at least 30 years in an effort to determine if they can be used, either topically or systemically, in the prevention of cutaneous cancers (NMSC or MM). Unfortunately, conflicting data exists from similarly designed studies showing either a decrease in cancer incidence or no difference. As the incidence of all skin cancers continues to increase, more research will be devoted to finding chemoprophylactic agents that are effective and have low side effect profiles. Acitretin has been shown to be potentially effective at reducing incidence of SCCs in high-risk individuals. Topical therapies have shown better efficacy for the treatment of BCCs rather than systemic therapies. Tretinoin has been shown to decrease the atypia associated with dysplastic nevi, and some population studies have shown that dietary or supplemental retinol and derivatives can potentially reduce the risk of melanoma. These studies all have contradictory studies associated with them. 180 Finally, little research has been performed on systemic pharmacologic intervention for melanoma prophylaxis due to the risks of side effects outweighing the potential benefit of chemoprophylaxis. REFERENCES 1. Peck GL, DiGiovanna JJ. Retinoids. In: Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg IM, Austen KF, editors. Dermatology in General Medicine, 3rd ed. New York, McGraw-Hill, 1987; pp. 2582–2906. 2. Peck GL, Yoder FW, Olsen TG, Pandya MD, Butkus D. Treatment of Darier’s disease, lamellar ichthyosis, pityriasis rubra pilaris, cystic acne, and basal cell carcinoma with oral 13-cis-retinoic acid. Dermatologica. 1978;157:11–12. 3. Peck GL et al. Treatment of basal cell carcinomas with 13-cis-retinoic acid. Proc Am Assoc Cancer Res. 1979;20:56 (abstract). 4. Peck GL, Gross EG, Butkus D, DiGiovanna JJ. Chemoprevention of basal cell carcinoma with isotretinoin. J Am Acad Dermatol. 1982;6:815–823. 5. Kraemer KH, DiGiovanna JJ, Peck GL. Chemoprevention of skin cancer in xeroderma pigmentosum. J Dermatol. 1992;19:715–718. 6. Harisiadis L, Miller RC, Hall EJ, Borek C. A vitamin A analogue inhibits radiation-induced oncogenic transformation. Nature. 1978;274:486–487. 7. McCarthy DJ, Lindamood III C, Hill DL. Effect of retinoids on metabolizing enzymes and on binding of benzo (a) pyrene to rate tissue DNA. Cancer Res. 1987;47:5014–5020. 8. Sultana S, Alam A, Sharma S, Khan N. 13-cis Retinoic acid ameliorates benzoyl peroxide-induced oxidative stress and hyperproliferative response in murine skin: A chemopreventive study. Cancer Detect Prev. 2004;28:200–207. 9. Samokyszyn VM, Marnett LJ. Inhibition of liver microsomal lipid peroxidation by 13-cis-retinoic acid. Free Radic Biol Med. 1990;8:491–496. 10. Delia D, Aiello A, Meroni L, Nicolini M, Reed JC, Pierotti MA. Role of antioxidants and intracellular free radicals in retinamide-induced cell death. Carcinogenesis. 1997;18:943–948. 11. Kroemer G, Zamzami N, Susan SA. Mitochondrial control of apoptosis. Immunol Today. 1997;18:44–51. 12. Kroemer G, Petit P, Zamzami N, Vayssière JL, Mignotte B. The biochemistry of programmed cell death. FASEB J. 1995;9:1277–1287. 13. Hail N Jr, Lotan R. Mitochondrial respiration is uniquely associated with the prooxidant and apoptotic effects of N-(4-hydroxyphenyl)retinamide. J Biol. Chem. 2001;276: 45614–45621. 14. Kligman AM, Grove GL, Hirose R, Leyden JJ. Topical tretinoin for photoaged skin. J Am Acad Dermatol. 1986;15:836–859. 15. US Food and Drug Administration (FDA). FDA Talk Paper: FDA Approves Renova to Assist in Reducing Skin Damage. Washington, DC, 2004. 16. Cho S, Lowe L, Hamilton TA, Fischer GJ, Voorhees JJ, Kang S. Long-term treatment of photoaged human skin with topical retinoic acid improves epidermal cell atypia and thickens the collagen band in papillary dermis. J Am Acad Dermatol. 2005;53:769–774. Retinoids in Dermatology 17. Bianchi L, Orlandi A, Campione E, Angeloni C, Costanzo A, Spagnoli LG, Chimenti S. Topical treatment of basal cell carcinoma with tazarotene: A clinicopathological study on a large series of cases. Br J Dermatol. 2004;151:148–156. 18. Peris K, Fargnoli MC, Chimenti S. Preliminary observations on the use of topical tazarotene to treat basal-cell carcinoma. N Eng J Med. 1999;341:1767–1768. 19. So P-L et al. Topical tazarotene chemoprevention reduces basal cell carcinoma number and size in Ptch1+/− mice exposed to ultraviolet or ionizing radiation. Cancer Res. 2004;64:4385–4389. 20. So P-L, Wang GY, Wang K, Chuang M, Chiueh VC, Kenny PA, Epstein EH Jr. PI3K-AKT signaling is a downstream effector of retinoid prevention of murine basal cell carcinogenesis. Cancer Prev Res. 2014;7:407–417. 21. Campanelli A, Naldi L. A retrospective study of the effect of long-term topical application of retinaldehyde (0.05%) on the development of actinic keratosis. Dermatol. 2002;205:146–152. 22. Forbes PD, Urbach F, Davies RE. Enhancement of experimental photocarcinogenesis by topical retinoic acid. Cancer Lett. 1979;7:85–90. 23. Ting W. Tretinoin for the treatment of photodamaged skin. Cutis. 2010;86:47–51. 24. Nijsten TEC, Stern RS. Oral retinoid use reduces cutaneous squamous cell carcinoma risk in patients with psoriasis treated with psoralen-UVA: A nested cohort study. J Am Acad Dermatol. 2003;49:644–650. 25. Anforth R, Blumetti TCMP, Clements A, Kefford R, Long GV, Fernandez-Peñas P. Systemic retinoids for the chemoprevention of cutaneous squamous cell carcinoma and verrucal keratosis in a cohort of patients on BRAF inhibitors. Br J Dermatol. 2013;169:1310–1313. 26. Tangrea JA et al. Long-term therapy with low-dose isotretinoin for prevention of basal cell carcinoma: A multicenter clinical trial. J Natl Cancer Inst. 1992;84:328–332. 27. Levine N, Moon TE, Cartmel B, Bangert JL, Rodney S, Dong Q, Peng YM, Alberts DS. Trial of retinol and isotretinoin in skin cancer prevention: A randomized, double blind, controlled trial. Southwest Skin Cancer Prevention Study Group. Cancer Epidemiol Biomarkers Prev. 1997;6:957–961. 28. Kraemer KH, Lee MM, Scotto J. Xeroderma pigmentosum: Cutaneous, ocular, and neurologic abnormalities in 830 published cases. Arch Dermatol. 1987;123:241–250. 29. Kraemer KH, DiGiovanna JJ, Moshell AN, Tarone RE, Peck GL. Prevention of skin cancer in xeroderma pigmentosum with the use of oral isotretinoin. N Engl J Med. 1988;318:1633–1637. 30. Kovach BT, Sams HH, Stasko T. Systemic strategies for chemoprevention of skin cancers in transplant recipients. Clin Transplant. 2005;19:726–734. 31. Lien MH, Fenske NA, Glass LF. Advances in the chemoprevention of non-melanoma skin cancer in high-risk organ transplant recipients. Semin Oncol. 2012;39:134–138. 32. Bavinck J, Tieben L, Van der Woude F, Tegzess AM, Hermans J, ter Schegget J, Vermeer BJ. Prevention of skin cancer and reduction of keratotic skin lesions during acitretin therapy in renal transplant recipients: A double-blind, placebo-controlled study. J Clin Oncol. 1995;13:1933–1938. 33. McKenna DB, Murphy GM. Skin cancer chemoprophylaxis in renal transplant recipients: 5 years of experience using lowdose acitretin. Br J Dermatol. 1999;140:656–660. Retinoids in Cutaneous Chemoprophylaxis 34. Otley C, Staska T, Tope W, Lebwohl M. Chemoprevention of nonmelanoma skin cancer with systemic retinoids: Practical dosing and management of adverse effects. Dermatol Surg. 2006;32:562–568. 35. Howlader N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA, editors. SEER Cancer Statistics Review, 1975–2016, National Cancer Institute. Bethesda, MD, https://seer.cancer.gov/csr/1975_2016/, based on November 2018 SEER data submission, posted to the SEER web site, April 2019. 36. Meyskens FL Jr, Edwards L, Levine NS. Role of topical tretinoin in melanoma and dysplastic nevi. J Am Acad Dermatol. 1986;15:822–825. 37. Edwards L, Jaffe P. The effect of topical tretinoin on dys­ plastic nevi. A preliminary trial. Arch Dermatol. 1990;126:494–499. 38. Halpern AC, Schuchter LM, Elder DE, Guerry D IV, Elenitsas R, Trock B, Matozzo I. Effects of topical tretinoin on dysplastic nevi. J Clin Oncol. 1994;12:1028–1035. 39. Stam-Posthuma JJ, Vink J, le Cessie S, Bruijn JA, Bergman W, Pavel S. Effect of topical tretinoin under occlusion on ­atypical naevi. Melanoma Res. 1998;8:539–548. 40. Asgari MM, Brasky TM, White E. Association of vitamin A and carotenoid intake with melanoma risk in a large prospective cohort. J Invest Dermatol. 2012;132:1573–1582. 181 41. Feskanich D, Willett WC, Hunter DJ, Colditz GA. Dietary intakes of vitamin A, C, and E and risk of melanoma in two cohorts of women. Br J Cancer. 2003;88:1381–1387. 42. Millen AE, Tucker MA, Hartge P, Halpern A, Elder DE, Guerry D IV, Holly EA, Sagebiel RW, Potischman N. Diet and melanoma in a case-control study. Cancer Epidemiol Biomarkers Prev. 2004;13:1042–1051. 43. Osterlind A, Tucker MA, Stone BJ, Jensen OM. The Danish case-control study of cutaneous malignant melanoma. IV. No association with nutritional factors, alcohol, smoking or hair dyes. Int J Cancer. 1988;42:825–828. 44. Vinceti M, Pellacani G, Malagoli C, Bassissi S, Sieri S, Bonvicini F, Krogh V, Seidenari S. A population-based casecontrol study of diet and melanoma risk in northern Italy. Public Health Nutr. 2005;8:1307–1314. 45. Kirkpatrick CS, White E, Lee JA. Case-control study of malignant melanoma in Washington state. II. Diet, alcohol, and obesity. Am J Epidemiol. 1994;139:869–880. 46. Stryker WS, Stampfer MJ, Stein EA, Kaplan L, Louis TA, Sober A, Willett WC. Diet, plasma-levels of beta carotene and alpha-tocopherol, and risk of malignant melanoma. Am J Epidemiol. 1990;131:597–611. 47. Le Marchand L, Saltzman BS, Hankin JH, Wilkens LR, Franke AA, Morris SJ, Kolonel LN. Sun exposure, diet, and melanoma in Hawaii Caucasians. Am J Epidemiol. 2006;164:232–245. 29 Guide to Good Clinical Practice for Vulnerable Populations (Infancy, Childhood, Fertile Period, Elderly) Elif Yildirim and Berna Aksoy Introduction Infancy Retinoids are most frequently indicated for keratinization disorders and psoriasis during the infantile period. Children need retinoid treatment for these same indications and additionally acne treatment. Fertile women need retinoids especially for acne and psoriasis. Special precautions are needed for the use of retinoids during pregnancy and breastfeeding. The elderly population has additional indications of antiaging and prevention of skin carcinogenesis for the use of topical and systemic retinoids. Retinoids require special attention when used in these vulnerable populations that include infants, children, fertile women, and the elderly. The major concern for use in infants and children is the skeletal toxicity, while teratogenicity is the major concern in fertile women. Tolerability is the main limiting factor for the elderly. Various precautions are needed when retinoids are used in these populations. Nonetheless, retinoids can be used safely and effectively in these vulnerable populations with strict follow-up and obedience of the established rules. Table 29.1 summarizes the use of retinoids in these vulnerable populations. Topical Retinoids Although none of the available retinoids have been approved by the United States Food and Drug Administration (FDA) for use in children, topical retinoids may also be used in infants, when required (1). There are few studies about use of topical retinoids in pediatric patients. The known side effects include a mild irritant dermatitis, which can be controlled by decreasing the frequency of application (2). In a 16-week study of 12 infants with infantile acne (mean age, 12.6 months), 0.1% adapalene cleared both comedonal and inflammatory lesions in a median of 3.4 months. The mild side effects did not require discontinuation, underscoring the reported high tolerability of adapalene (3). Tazarotene has been used less often as a first-line agent for acne, as it is more irritating (4). Systemic Retinoids Oral synthetic retinoids are effective especially against keratinization disorders, psoriasis, and severe acne developing in infants. TABLE 29.1 Isotretinoin Use of Retinoids in Vulnerable Populations Infancy Childhood Topical Retinoids Systemic Retinoids Use adapalene as first line and tazarotene as second line Skin irritation is the major concern Can be safely used Skin irritation is the major concern Can be safely used for keratinization disorders, acne, and psoriasis Fertile women Should be avoided during pregnancy and breastfeeding Elderly Risk of significant skin irritation Adherence is lower than other patient populations Skeletal toxicity is the major concern Can be safely used for limited time periods Avoid during pregnancy and breastfeeding Should use two different contraceptive methods during and following systemic retinoid usage Mucocutaneous side effects are increased Can be safely used for short-term treatment Oral isotretinoin has been used with success to treat resistant occurrences of infantile acne causing severe scarring and cosmetic sequelae (5). It has been safely used with doses of 0.2–2 mg/kg/day divided into two daily doses and given with food or milk to enhance oral absorption for 4–14 months of therapy (6,7). The ideal cumulative isotretinoin dose for infantile acne is not known. Isotretinoin is available in 10-, 20-, and 40-mg soft gelatin capsules. In order to administer dosages in the 0.2–2 mg/kg/day range, it may be necessary to puncture capsules with an 18-gauge needle to squeeze the contents of the capsule into soft food like cottage cheese, ice cream, pudding, oatmeal, or butter. Because isotretinoin is extremely sensitive to light and oxygen, it requires immediate usage. Another approach for administration of isotretinoin to infants is freezing the capsule, cutting it to the desired dose, and concealing it in a palatable food, or even a candy bar or cookie. This method minimizes exposure of the active ingredient to light and oxygen and masks the poor taste of the vehicle (8). 183 184 Acitretin and Etretinate Acitretin and etretinate are mainly effective against disorders of keratinization via promoting keratinocyte differentiation. Most ichthyoses, except for Netherton syndrome, respond well to ­systemic retinoids within a few weeks. Autosomal recessive congenital ichthyosis (ARCI), including lamellar ichthyosis (LI), congenital ichthyosiform erythroderma (CIE), and harlequin ichthyosis (HI), have been treated effectively with oral retinoids, but continued treatment is necessary (9). In neonates with HI, the early induction of systemic retinoids promotes accelerated shedding of the hyperkeratotic plates, and continued use reduces scaling and diminishes the formation of an ectropion or eclabium. Use of systemic retinoid and neonatal intensive care unit admission appear to lead to better prognosis in the HI fetus (10). A multicenter retrospective questionnaire–based survey among referring physicians conducted in the United Kingdom, Sweden, the United States, Iran, Turkey, and New Zealand found an overall survival rate of 56% (25/45 patients) among HI. A total of 83% of HI neonates treated with systemic retinoids survived, whereas the long-term survival was only 24% for those who were not given oral retinoids (11). Etretinate has been administered with a dosage of 1–3 mg/kg/day and acitretin with a dosage of 0.5–1 mg/kg/day (12). Among several types of retinoid derivatives, acitretin may be preferred because its shorter half-life ­provides a better safety profile (13). The treatment of ichthyoses using acitretin is mainly described in open series with small numbers of patients primarily with LI and nonbullous ichthyosiform erythroderma who were treated for up to 25 years (13) with oral retinoids. Significant improvements were noted with a mean (standard deviation [SD]) optimal dosage for acitretin of 0.47 (0.17) mg/kg per day. Adverse but reversible effects included frequent mild to moderate mucocutaneous dryness with minor abnormalities of liver function tests (four patients) and triglycerides (one patient). Recommendations for acitretin therapy for children include beginning with 0.5 mg/ kg per day, with careful monitoring of mucocutaneous side effects and laboratory tests (13). Although retinoids have been used widely in inherited disorders of keratinization, there are few case reports and case series about the administration of acitretin for the treatment of infantile psoriasis. Retinoids have been recommended for short-term treatment in pustular or erythrodermic psoriasis in infants (14). Data suggest that acitretin may be considered as a treatment option in the first 3 months of therapy in children, as it is used in adults. Although potential systemic toxicity of acitretin is a concern in long-term use, close monitoring of adverse effects may help minimize complications (15,16). A 2.5-month-old girl with infantile pustular psoriasis was treated with acitretin 0.7 mg/kg/day, which led to remission of the skin lesions in 4 months. She was maintained on a dose of 0.3 mg/kg/ day for another 3 months. A short course of steroids was also given during the initial phase (17). A 6-week-old infant with generalized pustular psoriasis was given acitretin at 1 mg/kg/day with resolution of the lesions in 6 weeks, after which the acitretin was tapered to 0.4 mg/kg/day for maintenance for 6 additional months (18). Skeletal toxicity has been a major concern in children treated with systemic retinoids, as there are reports of premature Retinoids in Dermatology epiphyseal closure. Studies have shown no significant skeletal toxicity in children aged 6 months to 16 years (19). The current approach is to monitor patients treated with systemic ­retinoids every 6 months with serial skeletal surveys (19). Childhood Topical Retinoids Tretinoin gel 0.05% is FDA approved for use in children ≥10 years of age (20), and adapalene gel 0.1%–2.5% is indicated for ages 9 and older. Adapalene gel, tretinoin gel, and tretinoin microsphere gel have been investigated in both open-label and blinded studies in children less than 12 years of age (3,21,22). Tazarotene is an effective topical retinoid, but it is used less often as a first-line agent due to irritation (23). Continuous daily dosing of tretinoin 0.1% cream, tazarotene 0.1% gel, or adapalene 0.1% gel has been shown to only slightly increase the mean maximum plasma levels of circulating retinoids in most patients. Serum retinoid levels may be influenced more by dietary retinoid intake than by topical application of tretinoin in children (24). In the absence of significant systemic absorption of the topically applied active retinoid ingredients, the possibility of topical irritation remains the primary safety issue with topical retinoid usage in children. The most common adverse effects of topical retinoids include burning, stinging, dryness, and scaling (25). These effects may be reduced by initiating treatment with the lowest strength, typically sufficient to treat mild acne, or by recommending regular use of a moisturizer with topical retinoid usage in children. Patients should be instructed not to spot-treat but rather to use a pea-sized amount to cover the entire face. In patients with sensitive skin, therapy can be initiated with thriceweekly application, increasing to daily use as tolerated (21). Systemic Retinoids During childhood and adolescence, the main safety concern in the use of retinoids is their effects on bone development. Acute mucocutaneous toxicities and mild laboratory abnormalities are common and reversible and rarely a cause for cessation of therapy in this age group (16,24). The interaction between retinoids and skeletal homeostasis is complex, and there is limited and conflicting evidence concerning retinoid-related bone changes. The duration of therapy is important for the safe use of oral retinoids for dermatologic conditions in children and adolescents. While short-term therapy such as a single-course acne therapy possesses low risk of skeletal toxicity, this risk increases as the duration of therapy increases such as for keratinization disorders (16,24). Isotretinoin has been shown to have no effect on bone density in a recent double-blind randomized study, which followed 358 teenagers for 5.5 months (26). Skeletal toxicities are more common in children on long-term retinoid therapy (i.e., etretinate and acitretin for keratinization disorders); within this group, risk can be stratified according to low-dose (0.3–0.5 mg/ kg/d) and high-dose (>1.0 mg/kg/d) treatment (16). Case reports and case series have identified patients who developed depressive symptoms while receiving or after isotretinoin therapy (27), and one study has documented changes in Guide to Good Clinical Practice for Vulnerable Populations (Infancy, Childhood, Fertile Period, Elderly) cerebral metabolism in patients receiving isotretinoin therapy (28). Epidemiologic studies, however, do not support a causative association between isotretinoin and depression (29). Fertile Period Topical Retinoids Tretinoin (Pregnancy Category C, which means there is proven risk to the fetus in animal studies but no such data is available for humans) has low percutaneous absorption that does not change endogenous levels but can cross the human placenta (30). There have been reports of congenital malformations associated with first-trimester use (31). Some studies found no difference in minor malformations between patients exposed to tretinoin in the first trimester and controls (32–34). A recent meta-analysis ruled out a major increase in the rates of major congenital malformations, spontaneous abortions, low birthweight, and prematurity (35); however, topical retinoid use in pregnancy is not recommended, because their risk/benefit ratio is questionable. Tretinoin has not been studied during breastfeeding. Breastfeeding should probably be avoided during topical retinoid use. Because it is poorly absorbed after topical application, it is considered to be a low risk to the nursing infant (36–38), but the infant’s skin should not come into direct contact with the areas of skin that have been treated. Adapalene (Category C) has been poorly studied. The drug has negligible percutaneous systemic absorption, and it remains unknown whether it crosses the placenta. There is a case report of maternal exposure to adapalene in early pregnancy with fetal anophthalmia and agenesis of the optic chiasma (39). A study including 24 pregnant patients exposed to adapalene in the first trimester did not find any fetal risks from adapalene (32). Tazarotene (Category X) is a prodrug that is converted to tazarotenic acid, its active metabolite. Animal studies have shown retinoid-like anomalies with topical tazarotene, so it is contraindicated during pregnancy (36). Plasma levels of tazarotene and tazarotenic acid after topical application are similar to those of endogenous retinoids (30). It is possible that limited use of tazarotene may be safe because the systemic exposure is even lower. Healthy infants were born to women enrolled in registries for topical tazarotene use; however, knowledge about the timing and extent of the usage is inadequate (40). Systemic Retinoids Oral retinoids, such as isotretinoin and acitretin, are well-known category X teratogens and are absolutely contraindicated during pregnancy (41). The adverse effects of therapeutically used systemic retinoids in embryonic development are similar. Vitamin A derivatives play a crucial role in embryonic development, and systemic retinoids are highly teratogenic especially early in pregnancy. Exposure during pregnancy is associated with a high risk of fetal malformation. These include the following structures (42–44): • Craniofacial • Cardiac • Thymic 185 • Parathyroid • Central nervous system Fertile women can receive the systemic retinoids mainly for the indication of acne and rarely for psoriasis or cutaneous T-cell lymphoma (CTCL) treatment. Women of childbearing potential should be followed carefully with strict guidelines. There are various programs to prevent pregnancy during systemic retinoid usage, such as iPLEDGE in the United States and PPP in Europe. Teaching effective contraception, periodical pregnancy tests, and prohibition for blood donation even after the end of therapy is very important. This is necessary because bleeding at the time of implantation may simulate the menstrual period, and human chorionic gonadotropin levels may not increase until 7–9 days after fertilization. There is evidence that retinoids such as bexarotene and acitretin decrease the efficacy of oral contraceptives, especially progesterone-only compounds like the minipill, by inducing CYP450 (e.g., CYP3A4). For this reason two different contraceptive methods are required during systemic isotretinoin usage in fertile women. Retinoid levels can be elevated for months to years, depending on the compound used, due to the bioavailability and storage in adipose tissue as fat-soluble derivatives of vitamin A. The highly lipophilic etretinate has a very long half-life and may be detected in the body 2 years after the end of therapy (45). The elimination half-life of acitretin is 33–96 h; however, acitretin has the potential to re-esterify to etretinate after alcohol consumption, which has a much longer elimination half-life and which requires the use of contraception for 2–3 years after cessation of acitretin (46). For this reason, women with childbearing potential should avoid the consumption of alcohol until 2 months after the end of acitretin therapy. During systemic use of alitretinoin, isotretinoin and bexarotene, contraception should be continued for at least 1 month after the end of therapy. Elderly Topical Retinoids Tretinoin and isotretinoin, as well as adapalene and tazarotene preparations, may cause significant irritation in the elderly. Significantly greater adverse effects are associated with the higher strength formulations. Older skin seems to be more sensitive to the topical retinoids than more youthful skin (47). Adherence to topical treatments seems to be lower in older patients (48). Systemic Retinoids Retinoids act by inducing cell differentiation and maturation and may help reverse the pathogenesis of malignancies (49). Unfortunately, most common side effects include dryness of the skin and mucosal membranes that can further exacerbate already present xerosis, common in the older population (50). To alleviate these side effects, frequent application of emollients may be recommended as well as limiting soap to the critical areas or reducing the dosage (51). 186 Retinoids are known to increase serum lipids and triglycerides, but they have not been found to significantly increase cardiovascular risk (52). Because the cardiovascular risk of hypertriglyceridemia usually takes many years to develop, the short-term use is likely to be safe in the geriatric population (53). Although there are no studies evaluating retinoids specifically in the elderly population, this therapy has not been associated with life-threatening toxicity and is a reasonable therapeutic option (48). Conclusions Topical and systemic retinoids can be used safely and effectively in infants, children, and the elderly when clinically indicated, regardless of age. Women of childbearing age should only be given oral retinoids under controlled circumstances, as there are some reports of embryotoxicity even caused by topical retinoid usage during early gestational periods. Systemic retinoids should not be used during pregnancy, and women of childbearing age require the use of two different contraceptive methods during systemic retinoid treatment. REFERENCES 1. Lucky AW. A review of infantile and pediatric acne. Dermatology 1998;196:95–97. 2. Cunliffe WJ, Baron SE, Coulson IH. A clinical and therapeutic study of 29 patients with infantile acne. Br J Dermatol. 2001;145:463–466. 3. Kose O, Koç E, Arca E. Adapalene gel 0.1% in the treatment of infantile acne: An open clinical study. Pediatr Dermatol. 2008;25:383–386. 4. Bershad S, Kranjac Singer G, Parente JE et al. Successful treatment of acne vulgaris using a new method: Results of arandomized vehicle-controlled trial of short contact therapy with 0.1% tazarotene gel. Arch Dermatol. 2002;138:481–489. 5. Arbegast KD, Braddock SW, Lamberty Sawka AR. Treatment of infantile cystic acne with oral isotretinoin: A case report. Pediatr Dermatol. 1991;8:166–168. 6. Antoniou C, Dessinioti C, Stratigos AJ, Katsambas AD. Clinical and therapeutic approach to childhood acne: An update. Pediatr Dermatol. 2009;26:373–380. 7. Admani S, Barrio VR. Evaluation and treatment of acne from infancy to preadolescence. Dermatol Ther. 2013;26:462–466. 8. Barnes CJ, Eichenfield LF, Lee J, Cunningham BB. A practical approach for the use of oral isotretinoin for infantile acne. Pediatr Dermatol. 2005;22:166–169. 9. Khalil S, Bardawil T, Stephan C et al. Retinoids: A journey from the molecular structures and mechanisms of action to clinical uses in dermatology and adverse effects. J Dermatolog Treat. 2017;28:684–696. 10. Shibata A, Akiyama M. Epidemiology, medical genetics, diagnosis and treatment of harlequin ichthyosis in Japan. Pediatr Int. 2015;57:516–522. 11. Rajpopat S, Moss C, Mellerio J et al. Harlequin ichthyosis: A review of clinical and molecular findings in 45 cases. Arch Dermatol. 2011;147:681–686. 12. Harvey HB, Shaw MG, Morrell DS. Perinatal management of harlequin ichthyosis: A case report and literature review. J Perinatol. 2010;30:66–72. Retinoids in Dermatology 13. Lacour M, Mehta-Nikhar B, Atherton DJ et al. An appraisal of acitretin therapy in children with inherited disorders of keratinization. Br J Dermatol. 1996;134:1023–1029. 14. de Jager ME, de Jong EM, van de Kerkhof PC et al. Efficacy and safety of treatments for childhood psoriasis: A systematic literature review. J Am Acad Dermatol. 2010;62:1013–1030. 15. Katugampola RP, Finlay AY. Oral retinoid therapy for disorders of keratinization: Single-center retrospective 25 years’ experience on 23 patients. Br J Dermatol. 2006;154:267–276. 16. Brecher AR, Orlow SJ. Oral retinoid therapy for dermatologic conditions in children and adolescents. J Am Acad Dermatol. 2003;49:171–182. 17. Ergin S, Ersoy-Evans S, Sahin S, Ozkaya O. Acitretin is a safe treatment option for infantile pustular psoriasis. J Dermatolog Treat. 2008;19:341–343. 18. Chao PH, Cheng YW, Chung MY. Generalized pustular psoriasis in a 6-week-old infant. Pediatr Dermatol. 2009;26:352–354. 19. Dogra S, Yadav S. Acitretin in psoriasis: An evolving s­ cenario. Int J Dermatol. 2014;53:525–538. 20. Atralin (tretinoin) Gel, 0.05% [package insert]. Fort Worth, TX: Coria Laboratories; 2007. 21. Eichenfield LF, Matiz C, Funk A, Dill SW. Study of the efficacy and tolerability of 0.04% tretinoin microsphere gel for preadolescent acne. Pediatrics. 2010;125:e1316–23. 22. Eichenfield LF, Hebert AA, Schachner L et al. Tretinoin microsphere gel 0.04% pump for treating acne vulgaris in preadolescents: A randomized, controlled study. Pediatr Dermatol. 2012;29:598–604. 23. Bershad S, Kranjac Singer G, Parente JE et al. Successful treatment of acne vulgaris using a new method: Results of a randomized vehicle-controlled trial of short contact therapy with 0.1% tazarotene gel. Arch Dermatol. 2002;138:481–489. 24. Eichenfield LF, Krakowski AC, Piggott C et al. American Acne and Rosacea Society. Evidence-based recommendations for the diagnosis and treatment of pediatric acne. Pediatrics. 2013;131:163–186. 25. Gollnick H, Cunliffe W, Berson D et al. Global Alliance to Improve Outcomes in Acne. Management of acne: A report from a Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2003;49:1–37. 26. Hoover KB, Miller CG, Galante NC, Langman CB. A double-blind, randomized, Phase III, multicenter study in 358 pediatric subjects receiving isotretinoin therapy demonstrates no effect on pediatric bone mineral density. Osteoporos Int. 2015;26:2441–2447. 27. Magin P, Pond D, Smith W. Isotretinoin, depression and suicide: A review of the evidence. Br J Gen Pract. 2005;55:134–138. 28. Bremner JD, Fani N, Ashraf A et al. Functional brain imaging alterations in acne patients treated with isotretinoin. Am J Psychiatry. 2005;162:983–991. 29. Bauer LB, Ornelas JN, Elston DM, Alikhan A. Isotretinoin: Controversies, facts, and recommendations. Expert Rev Clin Pharmacol. 2016; 91435–1442. 30. Kroumpouzos G, Draelos Z. Skin care products, cosmetics and cosmeceuticals. In: Kroumpouzos G, editor. Text Atlas of Obstetric Dermatology. Philadelphia, PA: Lippincott Williams & Wilkins, 2013; pp. 251–257. 31. Mutyambizi K, Mackool BT. Drug safety. In: Kroumpouzos G, editor. Text Atlas of Obstetric Dermatology. Philadelphia, PA: Lippincott Williams & Wilkins, 2013; pp. 217–250. Guide to Good Clinical Practice for Vulnerable Populations (Infancy, Childhood, Fertile Period, Elderly) 32. Panchaud A, Csajka C, Merlob P et al. Pregnancy outcome following exposure to topical retinoids: A multicenter ­prospective study. J Clin Pharmacol. 2012;52:1844–1851. 33. Loureiro KD, Kao KK, Jones KL et al. Minor malformations characteristic of the retinoic acid embryopathy and other birth outcomes in children of women exposed to topical tretinoin during early pregnancy. Am J Med Genet A. 2005;136:117–121. 34. Shapiro L, Pastuszak A, Curto G et al. Safety of first-trimester exposure to topical tretinoin. Lancet. 1997;350:1143–1144. 35. Kaplan YC, Ozsarfati J, Etwel F et al. Pregnancy outcomes following first-trimester exposure to topical retinoids: A systematic review and meta-analysis. Br J Dermatol. 2015;173:1132–1141. 36. Leachman SA, Reed BR. The use of dermatologic drugs in pregnancy and lactation. Dermatol Clin. 2006;24:167–197. 37. Zip C. Common sense dermatological drug suggestions for women who are breast-feeding. Skin Therapy Lett. 2002;7:5–7. 38. Butler DC, Heller MM, Murase JE. Safety of dermatologic medications in pregnancy and lactation: Part II Lactation. J Am Acad Dermatol. 2014;70:417.e1–417.e10. 39. Autret E, Berjot M, Jonville-Bera AP et al. Anophthalmia and agenesis of optic chiasma associated with adapalene gel in early pregnancy. Lancet. 1977;350:339. 40. Wilmer E, Chai S, Kroumpouzos G. Drug safety: Pregnancy rating classifications and controversies. Clin Dermatol. 2016;34:401–409. 41. Cunningham FG, Leveno KJ, Bloom SL et al. Maternal ­physiology. In: Williams Obstetrics. 22nd ed. New York: McGraw-Hill, 2005; pp 121–150. 42. Lammer EJ, Chen DT, Hoar RM et al. Retinoic acid embryopathy. N Engl J Med. 1985;313:837–841. 43. Barbero P, Lotersztein V, Bronberg R et al. Acitretin embryopathy: A case report. Birth Defects Res A Clin Mol Teratol. 2004;70:831–833. 187 44. de Die-Smulders CE, Sturkenboom MC, Veraart J et al. Severe limb defects and craniofacial anomalies in a fetus conceived during acitretin therapy. Teratology. 1995;52:215–219. 45. Baron JM. Retinoid pharmacology. In: Krieg T, Bickers DR, Miyachi Y, editors. Therapy of Skin Diseases. Berlin Heidelberg: Springer-Verlag, 2010; pp. 77–85. 46. Larsen FG, Jakobsen P, Knudsen J et al. Conversion of acitretin to etretinate in psoriatic patients is influenced by ethanol. J Invest Dermatol. 1993;100:623–627. 47. Marks R. Acne and its management beyond the age of 35 years. Am J Clin Dermatol. 2004;5:459–462. 48. Kostović K, Žužul K, Čeović R, Bukvić Mokos Z. Psoriasis in the mature patient: Therapeutic approach in the era of biologics. Clin Dermatol. 2018;36:222–230. 49. Bhutani T, Koo J. A review of the chemopreventative effects of oral retinoids for internal neoplasms. J Drugs Dermatol. 2011;10:1292–1298. 50. Wong JW, Koo JYM. The safety of systemic treatments that can be used for geriatric psoriasis patients: A review. Dermatol Res Pract. 2012;367475. 51. Seukeran DC, Cunliffe WJ. Acne vulgaris in the elderly: The response to low dose isotretinoin. Br J Dermatol. 1998;139:99–101. 52. Hugh J, Van Voorhees AS, Nijhawan RI et al. From the Medical Board of the National Psoriasis Foundation: The risk of cardiovascular disease in individuals with psoriasis and the potential impact of current therapies. J Am Acad Dermatol. 2014;70:168–177. 53. Butler DC, Koo JYM. Psoriasis therapy in the geriatric population. In: Chang ALS, editor. Advances in Geriatric Dermatology. New York: Springer, 2015; pp. 65–69. 30 Retinoids and Concomitant Surgery H. Mete Aksoy Introduction Oral retinoids, especially isotretinoin and acitretin, are used to treat acne and other dermatologic conditions. Accordingly, the number of patients who take systemic retinoid therapy and wish for or need surgical treatment has also increased. Isotretinoin (its isomer 13-cis retinoic acid) is a non-aromatic, first-generation systemic retinoid that was first introduced in 1982 for the treatment of acne and is currently used to treat a variety of dermatologic disorders. Acitretin is a mono-aromatic, second-generation systemic retinoid (a metabolite of etretinate). Acitretin is used to treat psoriasis and several other dermatologic diseases, as well as in the chemoprevention of skin cancer. Retinoids and Wound Healing Wound healing is a complex process, and the role of retinoids in wound healing is confusing and controversial (1). Isotretinoin and other retinoids exhibit anti-inflammatory actions on human keratinocytes, enhance epithelialization, and stimulate epidermal cell migration (2). Retinoids have been observed to inhibit collagen synthesis and fibroblast proliferation in human normal skin fibroblast cell culture studies. An experimental study reported that 13-cis retinoic acid and etretinate inhibited collagen synthesis in human skin fibroblast cell cultures, although 13-cis retinoic acid did so to a greater degree. Etretinate inhibits DNA synthesis, and so this compound may inhibit fibroblast proliferation; however, 13-cis retinoic acid does not inhibit DNA synthesis or fibroblast proliferation (3). All-trans-retinoic acid (vitamin A acid) and 13-cis retinoic acid have been shown to inhibit collagen and non-collagenous protein synthesis through decreasing procollagen gene expression (4). Retinoids reduce collagen production and collagenase synthesis in human keloid fibroblast cell cultures. Isotretinoin suppresses the size and activity of sebaceous glands, and induces apoptosis in sebocytes (2). Experimental animal models have contributed to investigating the systemic influence of isotretinoin on skin wound healing. The results of an experimental study using the rabbit ear model of wound healing indicated that systemic administration of isotretinoin did not affect collagen synthesis. The dose of isotretinoin was 4 mg/kg/day in this study (5). The results of an experimental study using dogs indicated that there was no difference regarding healing of partial- and full-thickness wounds between the 13-cis retinoic acid-administered group and control group. The dose of isotretinoin was 2.5 mg/kg/day in this study (6). The results of an experimental study using a porcine model of wound healing indicated that there was no difference regarding healing of partial- and full-thickness wounds between the isotretinoin-administered group and control group. The dose of isotretinoin was 2 mg/kg/day in this study (7). In an experimental study using rats, isotretinoin administration permanently accelerated mast cell accumulation in the wound area. This study showed that retinoids increase mast cell content in the skin during wound healing. The histologic features of wound healing in isotretinoin-administered rats were better than those of the control group, and healing was faster in rats receiving the retinoid (8). An animal study using guinea pigs receiving isotretinoin 10 mg/kg/day found that animals on systemic isotretinoin had a delay in wound contraction compared to control animals, and this difference was statistically significant. This dose seems to be higher than doses used for the treatment of acne. When isotretinoin was discontinued, all wounds healed completely within a week in the same study (9). Therapeutic isotretinoin doses are usually not greater than 2 mg/kg/day in clinical practice, so experimental studies that have supplemented test animals with drug doses close to 2 mg/kg/ day are expected to correlate more with the clinical situations (2). Acitretin has been reported to prolong secondary wound healing in rats with a dose of oral acitretin 2.5 mg/kg/day. Oral acitretin delayed secondary wound healing, epithelization, and angiogenesis (10). The authors concluded that acitretin can adversely affect wound healing even when the dose of the drug is low, in contrast to isotretinoin. Cartilage tissue healing under the influence of isotretinoin has not been investigated, and direct cartilage healing problems related to retinoid use have not been reported (2). In an animal study using rats, daily isotretinoin in a dose corresponding to the dose employed for the treatment of cystic acne (7.5 mg/kg/day) accelerated alveolar repair following tooth extraction (11). In another experimental study involving rats, isotretinoin promoted acceleration of new bone formation in rat calvarial bone. The dose of the drug was also 7.5 mg/kg/day in this study; however, this increase in new bone formation was not statistically significant (12). Studies indicate that isotretinoin does not appear to cause bone healing problems; however, studies consistently show that isotretinoin can damage skeletal muscle tissue and affect muscle healing following surgery (2). Corticosteroids significantly impair wound healing, and steroid retardation of healing is a significant clinical problem. They cause dehiscence of surgical incisions, increase risk of wound 189 190 infection, and delay healing of open wounds. Corticosteroids bring about these effects by interfering with inflammation, fibroblast proliferation, collagen synthesis and degradation, deposition of connective tissue ground substances, angiogenesis, wound contraction, and re-epithelialization. These effects are mediated by the antagonism of various growth factors and cytokines (13). Retinoids have the unique ability to reverse certain inhibitory effects of corticosteroids on wound healing (13,14). Impairment of the inflammatory response, tensile strength, and collagen accumulation in cutaneous wounds following corticosteroid treatment are partially, but significantly, reversed by retinoids. Retinoids do not reverse the adverse effects of glucocorticoids on wound contraction and infection. Retinoids restore the inflammatory response and promote epithelialization and the synthesis of collagen and ground substances (13); however, little is known about the mechanism of retinoid reversal. Certain actions of retinoids on cells are now known to be mediated via regulation of the levels of expression of growth factors and/or their receptors. Two of the peptides that regulate retinoids include the transforming growth factor β (TGF-β) isoforms, TGF-β1, -2, and -3, and insulin-like growth factor I (IGF-I). These growth factors regulate important phases of wound healing upon their release from platelet α granules. In an animal study, methylprednisolone treatment significantly reduced TGF-β and IGF-I levels in wound fluid and hydroxyproline content in tissue. Oral all-trans- and 9-cis retinoic acid partially reversed the TGF-β and IGF-I decrease and significantly increased hydroxyproline content toward normal levels in experimental animals given these agents. Oral all-trans-retinoic acid increased collagen deposition, TGF-β, and IGF-I levels over normal in control animals fed with chow. The authors postulated that corticosteroids reduce TGF-β and IGF-I levels and collagen deposition in wounds and that retinoids stimulate corticosteroidimpaired TGF-β and IGF-I release and collagen production (15). Retinoids and Surgical Procedures For many years, there has been intense debate on whether the use of systemic isotretinoin therapy in the perioperative period is safe. It has been suggested that in some circumstances a combination of isotretinoin therapy with surgery may be potentially more efficient than either therapy alone. The present established standard preoperative surgical care recommends the discontinuation of systemic isotretinoin therapy for 6–12 months prior to elective surgical procedures due to previous reports of delayed wound healing and keloid formation (16). The current standard recommendation appears to be to avoid surgical procedures in patients using oral isotretinoin. This recommendation places restrictions on physicians performing surgical procedures in patients with a history of retinoid use. As a result of medicolegal implications, physicians often delay the appropriate treatment for their patients (17). As a safeguard, performing surgical interventions in patients with a history of retinoid use is recommended only after obtaining a written informed consent containing information on possible adverse effects of retinoids on healing; however, this recommendation has been questioned in several studies (17). Consequently, it is doubtful that isotretinoin affects cutaneous Retinoids in Dermatology wound healing following surgery adversely, but there could be a small risk. Larger studies are needed. A clinical study aimed to evaluate the prevalence of abnormal scarring and postoperative complications in patients with or without exposure to isotretinoin in the perioperative period. One thousand six patients with isotretinoin and its brand names mentioned in their medical records were identified from the hospital clinical database, and medical records were searched for procedures involving a skin incision. Presence of surgical adverse effects was investigated in patients with or without a history of retinoid use in the perioperative period. Following medical record review, this study concluded that wound healing did not appear to be affected, and abnormal scar formation did not appear to be evident in patients undergoing isotretinoin therapy in comparison with those patients who were not exposed to the medication in the perioperative period. Surgical outcome in patients taking isotretinoin during the perioperative period was no different than in those not taking isotretinoin in this study. The findings of this study challenge the current practice of waiting 6–12 months to undergo elective surgery following isotretinoin exposure, despite the fact that this study was limited by an overall low level of surgical adverse effects and its retrospective nature. The same study states that a re-evaluation of the practice of recommending discontinuation of isotretinoin therapy in the perioperative period should be considered (18). Timing of Surgery Avoidance of use of systemic isotretinoin therapy in the perioperative period was accepted as a medical-legal standard in the 1980s following reports of cases of possible retinoid-related surgical complications. Isotretinoin discontinuation should range from 6−24 months prior to any elective cutaneous surgical procedure (2); however, the optimal timing for surgery in patients taking systemic isotretinoin remains unclear. Reaching definite conclusions concerning the effects of systemic use of isotretinoin on healing of surgical patients appears to require more clinical data. Recent clinical studies are challenging the belief that cutaneous incisional surgery in patients who have used isotretinoin in the perioperative period has an unacceptable risk of abnormal ­healing (2). There may be exceptions. A consensus report recommends that cutaneous incisional surgery involving muscle flaps should be delayed in patients who are on systemic isotretinoin therapy or have recently completed such therapy. The currently recommended time interval between discontinuation of systemic isotretinoin therapy and execution of surgery should be reviewed. One study states that considering oral isotretinoin pharmacokinetics may be a more logical approach to this issue, and this approach appears to be an objective treatment guide. This study suggests that discontinuation of isotretinoin for 30–35 days prior to surgical procedures is a justifiable delay when isotretinoin pharmacokinetics are considered (2). Anesthesia and Isotretinoin No study has verified how isotretinoin influences anesthesia. Studies on the interference of isotretinoin in hepatic drug metabolism, kidney damage, and arrhythmias can be combined to give 191 Retinoids and Concomitant Surgery an idea of how isotretinoin may influence anesthesia. Fifteen percent of patients who are on therapy with systemic isotretinoin displayed altered liver function. These alterations in liver function are generally mild. Seldom is discontinuation of isotretinoin necessary due to development of hepatitis or significantly ­elevated liver enzymes, although isotretinoin induces hepatic cytochrome P-450 action. This action of isotretinoin may reduce the therapeutic activity of warfarin (2). Only one case report on the association of systemic isotretinoin use with acute interstitial nephritis exists. Renal toxicity is not characteristic of isotretinoin use. This drug can alleviate kidney damage in animal models. Patients with end-stage kidney disease can safely take this drug (2). Systemic isotretinoin use is rarely associated with cardiac arrhythmias. Reported cases suffered from benign arrhythmias that resolved without development of complications. A study specifically designed to investigate retinoid-associated arrhythmias failed to report any occurrence of such arrhythmias (2). Risk of altered liver, renal, or cardiac function and risk of ­disturbances in the metabolism and excretion of drugs used during anesthesia are possibly not significant in patients who are on ­systemic isotretinoin therapy. There is a lack of reports of adverse interactions between anesthesia and systemic retinoid therapy, whose use is quite common (2). It may be concluded that it is safe to administer anesthesia to patients taking isotretinoin therapy as long as they are healthy and their preoperative blood test results fall within normal limits (19). Isotretinoin Use and Risk of Abnormal Bleeding during or after Surgery Systemic isotretinoin use has been found to be associated with thrombocytopenia; however, association of thrombocytopenia and systemic isotretinoin use is a rare occurrence, and only five cases have been reported up to 2016. Rapid recovery of platelet counts was observed 7–9 days after cessation of systemic isotretinoin in four of these cases. In one case, thrombocytopenia lasted 2 months but other clinical conditions apart from isotretinoin use may have contributed to the prolonged thrombocytopenia. It can be concluded that the risk of bleeding due to retinoid-related thrombocytopenia is very low (2). A clinical study reported that isotretinoin lowered platelet counts in 110 patients treated for acne. Platelet counts for all the patients in this study were at least 200,000/microliter, and this is a value which is normal by any standard. According to the results of this study, there is no increased risk of bleeding as a result of thrombocytopenia in patients who are on systemic retinoid therapy (2). Thrombocytosis is an uncommon finding during systemic isotretinoin use. Data about the incidence of this finding are controversial, and no clinical complications of isotretinoin-induced thrombocytosis have been reported in the literature. Platelet counts should drop to normal values 3 weeks following discontinuation of systemic isotretinoin therapy. A clinical study has shown that acne treatment with systemic isotretinoin therapy for a duration of 1 month does not lead to an increase in prothrombin time (PT) or the international normalized ratio (INR); h­ owever, the same study showed that systemic retinoid use prolongs ­activated partial thromboplastin time (APTT) in these patients. APTT alteration was within normal time standards and had no impact on blood coagulation in patients in this study (2). In summary, systemic isotretinoin therapy rarely affects coagulation and creates a very low risk of bleeding during or after a surgical intervention. Retinoids and Risk of Surgical Infection Retinoids inhibit mycobacteria growth in laboratory culture media. Systemic isotretinoin use leads to dryness in mucosal membranes and skin. This effect is associated with changes in the bacterial flora of specific sites of the body. A clinical study found that systemic isotretinoin therapy eliminated gram-negative bacteria from the anterior nares, face, and axilla with simultaneous increase of the Staphylococcus aureus population in the nose; however, this finding was not related to increased infections. In conclusion, studies do not provide any evidence that isotretinoin interferes with infection (2). Retinoids and Surgical Dermabrasion Surgical dermabrasion is usually performed by the use of a power-driven rotating diamond rasp. The depth of dermabrasion is determined by the operator and can range from the superficial epidermal level to the deep reticular dermal level. This technique is not frequently used because there is a serious health risk concerning operative personnel as a result of aerosolization of skin and blood during this procedure. Unlike other resurfacing procedures, it is possible to perform dermabrasion on all skin types. Photodamage, superficial rhytids, hyperpigmentation, and scarring can all be treated by using dermabrasion (20). Nine patients with severe nodulocystic acne vulgaris who were treated with oral 13-cis retinoic acid were reported in 1985. Their acne cleared, and these patients underwent full-face dermabrasion during or after retinoid therapy. Postoperative healing was normal, and no significant complication was observed in this report (21). Dermabrasion might have been performed superficially in these cases, but this issue is not clear in the study. In a study performed in 1986, keloid development was observed in six patients who underwent dermabrasion while they were on systemic isotretinoin therapy or after they had recently completed such therapy. All patients in this study developed keloids in atypical locations. The authors concluded that dermabrasion should be delayed in those patients who are taking or recently have been on isotretinoin therapy. Dermabrasion might have been performed on deeper layers of dermis in this case series study and it is accepted that this practice can increase the risk of proliferative scar formation, but this issue is not clear in the study. It is known that retinoids display modulatory effects on the metabolism of connective tissue, including suppression of collagenase. Authors have suggested that this effect may enhance keloid formation secondary to mechanical dermabrasion (22). A 70-year-old man treated for rhinophyma using dermabrasion was reported in 1988. Immediately after dermabrasion, he was given isotretinoin daily for the treatment of rosacea. Healing took 4 weeks, and a keloid was detected on his nose 8 weeks after the operation. A normal healing time period after surgical dermabrasion is approximately 10 days, in contrast to the prolonged 192 healing time (4 weeks) seen in this male patient. Because dermabrasion was used to treat rhinophyma, it must have been deeply performed, and this may have contributed to occurrence of delayed healing and keloid formation in this patient (23). A 27-year-old woman with acne who underwent dermabrasion for a large traumatic scar on her left cheek while she was on isotretinoin daily for the treatment of acne was also reported. Complete healing took about 3 months. Keloid formation in the treated area was observed 6 months later. A normal healing time after surgical dermabrasion is approximately 10 days, in contrast to the prolonged healing time (3 months) seen in this patient. The same patient had undergone dermabrasion for the correction of the same problem with uneventful healing 1 year prior to the second procedure (23). The second procedure must have involved deeper layers of dermis, which may have contributed to delayed healing and keloid formation in this patient. In 1994, a case of atypical scarring was reported in a patient who began using systemic isotretinoin therapy 2 months following dermabrasion. This scarring was accepted as atypical, because it developed outside the typical danger zones such as mandible and malar eminences (24). Retinoids have been shown to modulate the metabolism of connective tissue in human keloid fibroblast cell cultures (23). Oral retinoids have been found to be associated with suppression of collagenase. This effect of retinoids may potentially cause accumulation of excessive collagen and lead to keloid formation (18,23). Suppression of production of collagenase by retinoids may be responsible for the development of keloids observed in patients with a history of systemic retinoid use following s­urgical interventions like mechanical dermabrasion (22,23); however, the problem of abnormal scarring related to retinoid use is ­complex and controversial, because isotretinoin has been shown to selectively inhibit normal skin fibroblasts, and under certain conditions isotretinoin reduces collagen formation in vitro. Topical retinoids have been used for the treatment of hypertrophic scars and keloids (23). Consequently, development of abnormal ­scarring following mechanical dermabrasion observed in patients with a history of retinoid use may not be related to effects of this drug on connective tissue metabolism. Another important factor affecting abnormal scar formation following mechanical dermabrasion may be delayed epithelialization. Growth of epidermal cells has been shown to be decreased in most in vitro studies (23). Oral retinoids have also been associated with possible atrophy of the pilosebaceous unit, and this unit is where re-epithelialization for wound healing originates (18). Split-thickness skin damage heals by proliferation of epidermal cells from the edges of the wound and skin adnexa like sweat and sebaceous glands. Prolonged wound healing secondary to delayed epithelialization may subsequently result in development of scar hypertrophy following mechanical dermabrasion (23). The risk of abnormal scarring following mechanical dermabrasion may also be related to skin dryness, as isotretinoin impairs sebaceous glands physiologically. A patient who is on systemic therapy with isotretinoin may be at increased risk of poor healing of partial-thickness wounds such as mechanical dermabrasion if skin dryness is detected on clinical examination. Systemic retinoids lead to skin thinning physiologically. It is also known that as dermal injury becomes deeper, the scar will be worse. Consequently, transient skin thinning brought about by Retinoids in Dermatology isotretinoin use may lead to poor epithelialization because skin thinning can increase the risk of inadvertent skin damage deeper than usual during execution of mechanical dermabrasion (2). It can be concluded that mechanical dermabrasion is not advised in the setting of systemic isotretinoin treatment. There is insufficient evidence to support delaying manual dermabrasion for patients currently receiving or having recently completed isotretinoin therapy (19). Seven patients taking oral isotretinoin to treat acne and with atrophic acne scars on the face were reported in a prospective study. In all patients, manual dermabrasion was performed in a facial skin area of approximately 1 cm2, and a 6-month follow-up by clinical evaluation to assess epithelialization was performed. All patients in the study displayed normal scarring evolution, and hypertrophic scarring or keloid development was not observed as a result of localized manual dermabrasion. This study suggests that abrasion of a small test area may be a useful predictor of wound healing, and this approach makes earlier acne scar treatment possible with the use of manual d­ ermabrasion (25). Cutaneous Surgery and Retinoids Patients using systemic isotretinoin therapy were treated with a variety of surgical procedures involving the skin, and they were reported to heal without development of complications. Twelve blepharoplasties, nine liposuctions, nine fat transfers, nine facelifts, eight skin biopsies, seven subcisions, two excisions, and twelve punch elevations of scars healed without any problem (17,19). A patient who underwent pilonidal sinus excision during isotretinoin treatment for acne was reported. There were no complications related to wound healing in this case. Two patients undergoing otolaryngologic surgery were reported. They had their isotretinoin treatment stopped for 2 days prior to surgery and for 1 week postoperatively. They healed normally following surgical interventions. A separate patient undergoing surgery involving skin incision was reported. This patient experienced slow healing while on systemic isotretinoin therapy (26). A young patient with a 130-day-old incision scar located on his right cheek experienced dehiscence of incision scar of a previous cyst excision after hitting his right cheek 29 days after initiation of retinoid therapy to treat acne lesions involving his face (27). Isotretinoin is known to decrease collagen synthesis during wound healing so the authors have postulated that the scar located on the cheek of the patient contained less collagen than a scar developed in the absence of retinoid therapy, and retinoid-induced decrease in collagen synthesis was accepted as the cause of scar dehiscence which occurred as a result of minor trauma (27). Two squamous cell carcinomas (SCCs), one located on the helical rim of the ear and the other located on the forehead, were removed from an elderly patient. Oral acitretin therapy was initiated for chemoprevention of development of new SCCs and to treat widespread actinic keratoses. On day 8 of acitretin treatment, the 25-day-old surgical scar on the forehead dehisced spontaneously, and the left helical scar became wider in time. It is known that acitretin inhibits both fibroblast proliferation and collagen synthesis. The authors concluded that the healed surgical wound of the patient contained less collagen, and wound tensile strength of the scar of the patient was less in comparison with 193 Retinoids and Concomitant Surgery a scar formed in the absence of retinoid therapy, and these caused spontaneous dehiscence of the patient’s scar following initiation of systemic acitretin therapy (27). The widened auricular scar in case 2 was older than the dehisced forehead scar. Dehisced scars present in both cases healed with secondary wound healing, which lasted longer than expected, and treatment with systemic retinoids continued in the presence of dehisced wounds. The authors have suggested that isotretinoin and acitretin seem to impair the remodeling phase of wound healing. The authors of this study recommended postponing systemic retinoid treatment for 6 months to 1 year following cutaneous incisional surgery, especially involving the face and ears (27). There appears to be insufficient evidence to postpone cutaneous surgery involving incisions for patients who are currently taking or have recently completed systemic isotretinoin therapy. A careful approach seems to be necessary when systemic ­retinoid therapy is planned in patients with a recent history of cutaneous incisional surgery involving the face or ears, considering the possibility of late wound dehiscence. Testing preoperative serum creatine phosphokinase (CPK) level appears to be warranted when cutaneous surgery is associated with a musclecontaining flap. Clinical reports indicate that retinoids probably do not adversely affect concurrent wound healing following incisional surgery, but the effects of systemic use of retinoids on cutaneous wound healing are still debated and controversial. In conclusion, well-controlled clinical trials are needed to clarify this subject (19). Skin Cancer Surgery and Retinoids A clinical study involving patients taking a second-generation retinoid, acitretin, contributes to evaluation of effects of retinoids on healing after surgical procedures (19). Twenty-nine immunosuppressed organ transplant recipients underwent Mohs micrographic or excisional surgery for the treatment of basal cell or squamous cell carcinoma. Surgical wounds were assessed postoperatively after an average of 12.9 days (early) and an average of 75.8 days (late). Presence of infection, hypertrophic granulation tissue, and hypertrophic scarring were recorded for all wounds. Reconstructed wounds were also assessed for the presence of dehiscence. Eleven patients were taking oral acitretin, and they had 41 wounds. In this group of patients, 33 wounds were reconstructed and 8 healed by secondary intention. Eighteen patients with 44 wounds were not taking systemic acitretin and they constituted the control group. In this group of patients, 33 wounds were reconstructed and 11 healed by secondary intention. Wounds resulting from excisions were reconstructed by using layered linear closure, full-thickness skin graft, or flap. No statistically significant differences between the acitretin group and the control group were found regarding incidences of infection, dehiscence, hypertrophic granulation tissue, or hypertrophic scarring at both early and late evaluation points. Systemic acitretin chemoprophylaxis does not seem to increase the risk of complications of wound healing in immunosuppressed organ transplant recipients (28). Immunosuppressed transplant recipients represent an older patient population in comparison with the adolescent acne population so they may be less likely to develop hypertrophic scars (19). Retinoids and Muscle-Containing Flaps Systemic isotretinoin use may increase CPK levels in 15%–50% of patients. Acute severe rhabdomyolysis may occur, but it is a rare event. Muscle alterations which develop during systemic isotretinoin use are usually benign and it is possible to treat them by reducing the level of the patient’s physical activity; however, an elevated CPK level indicates muscle injury, and serum CPK level greater than fivefold of normal may indicate presence of rhabdomyolysis. Patients taking isotretinoin with serum CPK blood levels above twofold of normal in the absence of a history of recent vigorous exercise may carry a risk for muscle flap failure. This risk factor is associated with the possibility of ­retinoid-induced rhabdomyolysis in these patients. Because systemic isotretinoin may affect any muscle in the body, it is not possible to identify which muscles have been damaged by the effect of this drug. A muscle flap may be inadvertently designed on a muscle that has already been injured by the effect of retinoids, so the risk of necrosis will be higher for this flap. Major reconstructive surgery involving muscle-containing flaps especially requires ­caution when the patient is receiving systemic isotretinoin therapy. If possible, flap surgery should be delayed until the patient displays CPK blood levels below twofold of normal value (2). Another study suggests that this recommendation about muscle flap use in patients using retinoid therapy lacks literature support. The same study reported that a thorough review performed by authors failed to find literature specifically addressing this warning. It appears that additional prospective, well-controlled clinical trials are needed to make definitive conclusions concerning this subject (19). Nose Surgery and Retinoids A patient developed osteophytes involving nasal bones following retinoid therapy. Bilateral 2.5- and 3.0-mm nasal bone osteophytes occurred 5 weeks following the initiation of systemic isotretinoin therapy in a healthy 30-year-old woman with a history of uneventful rhinoplasty 12 years earlier. Mature bone fragments were removed surgically. The authors concluded that development of clinically significant nasal bone osteophytes may be accepted as another adverse reaction to systemic isotretinoin therapy, given the fact that vitamin A and its analogs have been associated with hyperostosis of the vertebrae and long bones (29). Three cases were described in which postoperative use of isotretinoin was associated with development of nasal tip deformities following primary rhinoplasty. Isotretinoin was prescribed for acne within 2 years following a primary rhinoplasty procedure in all three cases. The nasal tip deformities were observed within 6 months after initiation of isotretinoin therapy. All three patients required subsequent surgical correction of these deformities. The authors concluded that further studies are necessary to investigate a possible causative relationship between systemic retinoid therapy and development of nasal tip deformities and they also stated that isotretinoin use may have been only coincidentally associated with development of nasal tip deformities. The authors recommended postponing isotretinoin treatment 194 for a minimum of 2 years following rhinoplasty (30). All three patients were from the same surgeon’s logbook (26). A study has reported that combining retinoid therapy with surgery appears to be safe, and this approach may also provide excellent cosmetic outcomes in thick-skinned patients undergoing facial plastic surgery including rhinoplasty. The same study also reported that low-dose regimens of isotretinoin may provide advantages over standard dosage therapies due to better tolerability and safety in long-term use as an adjunct to surgical procedures (16). Thicker nasal skin blunts the definition of the underlying osseocartilaginous frame of the nose, and this is especially important for the nasal tip region. Presence of thick skin poses additional challenges in producing desirable tip definition following rhinoplasty (31). Despite the use of a proper structural approach where grafts and sutures are used to give definition to the nasal tip, frequently the results of surgery are suboptimal in the presence of thick nasal skin (32). Although difficulty of management of patients with thick nasal skin has been recognized, there is a paucity of literature data on how to handle this problem. The skin thickness secondary to sebaceous overactivity can be decreased with the use of retinoids, and this is commonly accomplished under the advice of a dermatologist prior to nasal surgery (31). The use of systemic isotretinoin therapy as an adjunct to rhinoplasty can adequately suppress the sebaceous glands and reduce the thickness of skin− subcutaneous tissue envelope in a uniform fashion. In a clinical study performed in 2016, comparison of pre- and postoperative pictures of the nose showed improved definition of the nasal tip and dramatic improvement on sebaceous gland activity after 2 years of follow-up. The authors concluded that initiation of isotretinoin treatment in combination with rhinoplasty helped to define the nasal tip and improved the surgical outcome in patients with thick nasal skin (32). In a double-blind placebo-controlled clinical study, 48 rhinoplasty cases with thick skin were divided into two groups randomly. Oral isotretinoin (0.5 mg/kg/day) was started on the 31st day following surgery. Isotretinoin was given every other day for 1 month, and after 1 month the drug was given daily for 2 additional months in the first group. The second study group received a placebo in the same form, sequence, and time interval as the first group. The aesthetic results based on satisfaction of patients and ranking by an expert surgeon in the field of rhinoplasty were compared between the two study groups at 3 months, 6 months, and 1 year following aesthetic nose surgery in this study. Both patient satisfaction and ranking by an expert surgeon in the isotretinoin group at 3 months and 6 months after surgery were significantly better than those in the placebo group in this study; however, 12 months after surgery, there was no statistically significant difference between the two groups in this study (33). Although postoperative use of oral isotretinoin in patients with thick nasal skin accelerates improvement in aesthetic results during the early months after surgery, it does not significantly affect the final aesthetic result 1 year after surgery (33). Therapy durations longer than 4 months, and daily isotretinoin doses higher than 0.5 mg/kg/day such as 1 mg/kg/day (total isotretinoin dose of 120 mg/kg), may have produced different results because a significant sebosuppressive effect of isotretinoin requires longer therapy duration and higher doses (34). Retinoids in Dermatology Tooth Extraction and Retinoids A clinical study reported a higher rate of alveolar osteitis (11.4%) than the average cited rates (3%–5%) among 26 patients who underwent wisdom tooth extraction while they were concomitantly taking isotretinoin or had completed treatment 1 month prior to the procedure. A causal relationship between isotretinoin use and complications of wisdom tooth removal could not be concluded due to the limited sample size. All patients with dry sockets healed without further complications. The results obtained from this study on the effects of systemic isotretinoin use on wisdom tooth removal suggest that patients do not need to refrain from third molar tooth removal during treatment with isotretinoin (35). It can be concluded that wisdom tooth extraction is a safe procedure in patients who are on systemic retinoid therapy. In a clinical study on the relationship between interventional therapies and systemic retinoid use, a case of wisdom tooth extraction was reported. Healing was satisfactory after wisdom tooth extraction in this patient, despite the fact that the patient was on systemic isotretinoin therapy (17). In a clinical study on the relationship between systemic retinoid use and surgical outcome, two cases were reported where problematic healing after dental procedures occurred. Poor, edematous, and erythematous healing at the incision site was observed following wisdom tooth extraction in a patient who had discontinued systemic retinoid therapy 2 months prior to surgical intervention. Alveolar osteitis developed following tooth extraction in a patient who was using systemic retinoids at the time of surgical procedure. These cases were detected retrospectively out of 76 patients who underwent surgery following recent (less than or equal to 2 years) use of systemic retinoids (18). Ophthalmic Surgery and Systemic Retinoid Use The most widely performed type of refractive surgery is LASIK (laser-assisted in situ keratomileusis), where a laser is used to reshape the cornea. Laser refractive surgery, or LASIK, is one of the most common elective surgical procedures performed in the United States today. LASIK is a revolutionary procedure, and vision correction is achieved by the use of an excimer laser, which ablates corneal stroma. There are certain systemic conditions that may represent contraindications to the LASIK procedure. This procedure should be avoided in uncontrolled diabetes, collagen vascular disease and pregnancy, and in patients taking amiodarone or isotretinoin (36). It is known that systemic isotretinoin use leads to corneal xerosis, or dry eye, and LASIK surgery also causes this condition. LASIK surgery is contraindicated during systemic isotretinoin therapy for this reason (17,37). The complications of severe acute and chronic dry eye can be quite serious, and these include structural corneal damage and ulceration, infection, decreased vision, and even loss of vision (37). Subconjunctival hemorrhage following LASIK procedure has been reported in a patient who was on systemic retinoid therapy in a clinical study. Hemorrhage resolved without permanent sequelae in this patient (17). The average age of patients undergoing LASIK procedure is 40 years, but many patients are between Retinoids and Concomitant Surgery the ages of 18 and 30. This age range overlaps with the age profile of patients with acne, because the average age of acne patients is 24 years (37). Ophthalmologists should screen their patients for isotretinoin use before approving LASIK operations. The general consensus is that patients should wait for 6 months after a systemic isotretinoin course before they become candidates for LASIK procedure. Isotretinoin should not be prescribed for a duration of 6 months after LASIK procedure. This recommendation is based on the healing time of the cornea following refractive operation (17,37). There is a critical period of healing after a LASIK procedure, and corneal healing would be compromised by the initiation of a medication like isotretinoin. Dermatologists should ask their patients whether they have recently had LASIK surgery. The numbers of LASIK procedures and isotretinoin prescriptions are increasing rapidly, and it would be critical for dermatologists to be aware of the danger of prescribing systemic isotretinoin to patients who have had a LASIK procedure within the previous 6 months (37). Beneficial effects of use of systemic retinoid treatment on postoperative clinical outcome of eyes with proliferative vitreoretinopathy (PVR) have been reported (38). Postoperative administration of oral 13-cis retinoic acid seems to reduce PVR and increase the rate of retinal adherence following surgical therapy (39). Postoperative use of systemic 13-cis retinoic acid therapy for 8 weeks seems to maintain retinal attachment, reduce macular pucker, and improve vision following surgical treatment of eyes with PVR (38). The role of retinoic acid therapy as an adjunct to surgical therapy has also been investigated in an animal model of PVR. Retinoic acid can reduce the rate of tractional retinal detachment in a rabbit model of PVR when this agent is injected into the vitreous cavity in the form of retinoic acid−loaded microspheres. The use of oral 13-cis retinoic acid as an adjunct to surgery in PVR has shown promising results, but further studies on the efficacy of this agent are needed to support its use (40). Conclusions The preoperative surgical recommendation advising discontinuation of systemic isotretinoin therapy for 6–12 months prior to elective surgical procedures has been questioned in several studies. It is doubtful that isotretinoin adversely effects cutaneous wound healing following surgery, but there could be a small risk. Larger studies are needed. Mechanical dermabrasion, laser refractive surgery or LASIK, and reconstructive surgery using muscle-containing flaps are risky in patients with a history of retinoid therapy. Initiation of systemic retinoid therapy may negatively affect results of aesthetic nose surgery or cause dehiscence of healed surgical wounds located in the facial region, including the ears. REFERENCES 1. Abdelmalek M, Spencer J. Retinoids and wound healing. Dermatol Surg. 2006;32:1219–1230. 2. Ungarelli LF, Hetem CM, Farina Junior JA. Is it safe to operate on patients taking isotretinoin? Aesthetic Plast Surg. 2016;40:139–148. 195 3. Shigematsu T, Tajima S. Modulation of collagen synthesis and cell proliferation by retinoids in human skin fibroblasts. J Dermatol Sci. 1995;9:142–145. 4. Oikarinen H, Oikarinen AI, Tan EM et al. Modulation of procollagen gene expression by retinoids. Inhibition of collagen production by retinoic acid accompanied by reduced type I procollagen messenger ribonucleic acid levels in human skin fibroblast cultures. J Clin Invest. 1985;75:1545–1553. 5. Moy RL, Moy LS, Bennett RG et al. Systemic isotretinoin: Effects on dermal wound healing in a rabbit ear model in vivo. J Dermatol Surg Oncol. 1990;16:1142–1146. 6. Dzubow LM, Miller WH Jr. The effect of 13-cis-retinoic acid on wound healing in dogs. J Dermatol Surg Oncol. 1987;13:265–268. 7. Larson DL, Flugstad NA, O’Connor E et al. Does systemic isotretinoin inhibit healing in a porcine wound model? Aesthet Surg J. 2012;32:989–998. 8. Gencoglan G, Tosun M, Gencoglan O. Isotretinoin-induced effects of mast cells on wound healing. J Drugs Dermatol. 2010;9:1207–1210. 9. Arboleda B, Cruz NI. The effect of systemic isotretinoin on wound contraction in guinea pigs. Plast Reconstr Surg. 1989;83:118–121. 10. Gunes Bilgili S, Calka O, Akdeniz N et al. The effects of retinoids on secondary wound healing: Biometrical and histopathological study in rats. J Dermatolog Treat. 2013;24:283–289. 11. Bergoli RD, Chagas Junior OL, de Souza CE et al. Isotretinoin effect on alveolar repair after exodontia—a study in rats. Oral Maxillofac Surg. 2011;15:85–92. 12. de Oliveira HT, Bergoli RD, Hirsch WD et al. Isotretinoin effect on the repair of bone defects—a study in rat calvaria. J Craniomaxillofac Surg. 2013;41:581–585. 13. Anstead GM. Steroids, retinoids, and wound healing. Adv Wound Care. 1998;11:277–285. 14. Paquette D, Badiavas E, Falanga V. Short-contact topical tretinoin therapy to stimulate granulation tissue in chronic wounds. J Am Acad Dermatol. 2001;45:382–386. 15. Wicke C, Halliday B, Allen D et al. Effects of steroids and retinoids on wound healing. Arch Surg. 2000;135:1265–1270. 16. Heppt MV, Kirchberger MC, Ruzicka T et al. Indications and use of isotretinoin in facial plastic surgery. Facial Plast Surg. 2018;34:75–81. 17. Mahadevappa OH, Mysore V, Viswanath V et al. Surgical outcome in patients taking concomitant or recent intake of oral isotretinoin: A multicentric study-ISO-AIMS study. J Cutan Aesthet Surg. 2016;9:106–114. 18. Tolkachjov SN, Sahoo A, Patel NG et al. Surgical outcomes of patients on isotretinoin in the perioperative period: A single-center, retrospective analysis. J Am Acad Dermatol. 2017;77:159–161. 19. Spring LK, Krakowski AC, Alam M et al. Isotretinoin and timing of procedural interventions: A systematic review with consensus recommendations. JAMA Dermatol. 2017;153:802–809. 20. Buchanan PJ, Gilman RH. Retinoids: Literature review and suggested algorithm for use prior to facial resurfacing procedures. J Cutan Aesthet Surg. 2016;9:139–144. 21. Roenigk HH Jr, Pinski JB, Robinson JK, Hanke CW. Acne, retinoids, and dermabrasion. J Dermatol Surg Oncol. 1985;11:396–398. 22. Rubenstein R, Roenigk HH Jr, Stegman SJ, Hanke CW. Atypical keloids after dermabrasion of patients taking isotretinoin. J Am Acad Dermatol. 1986;15:280–285. 196 23. Zachariae H. Delayed wound healing and keloid formation following argon laser treatment or dermabrasion during isotretinoin treatment. Br J Dermatol. 1988;118:703–706. 24. Katz BE, Mac Farlane DF. Atypical facial scarring after isotretinoin therapy in a patient with previous dermabrasion. J Am Acad Dermatol. 1994;30:852–853. 25. Bagatin E, dos Santos Guadanhim LR, Yarak S et al. Dermabrasion for acne scars during treatment with oral isotretinoin. Dermatol Surg. 2010;36:483–489. 26. Wootton CI, Cartwright RP, Manning P, Williams HC. Should isotretinoin be stopped prior to surgery? A critically appraised topic. Br J Dermatol. 2014;170:239–244. 27. Aksoy HM, Aksoy B, Çalikoglu E. Systemic retinoids and scar dehiscence. Indian J Dermatol. 2019;64:68–70. 28. Tan SR, Tope WD. Effect of acitretin on wound healing in organ transplant recipients. Dermatol Surg. 2004;30:667–673. 29. Novick NL, Lawson W, Schwartz IS. Bilateral nasal bone osteophytosis associated with short-term oral isotretinoin therapy for cystic acne vulgaris. Am J Med. 1984;77:736–739. 30. Allen BC, Rhee JS. Complications associated with isotretinoin use after rhinoplasty. Aesthetic Plast Surg. 2005;29:102–106. 31. Guyuron B, Lee M. An effective algorithm for management of noses with thick skin. Aesthetic Plast Surg. 2017;41:381–387. 32. Cobo R, Vitery L. Isotretinoin use in thick-skinned rhinoplasty patients. Facial Plast Surg. 2016;32:656–661. 33. Sazgar AA, Majlesi A, Shooshtari S et al. Oral isotretinoin in the treatment of postoperative edema in thick-skinned Retinoids in Dermatology 34. 35. 36. 37. 38. 39. 40. rhinoplasty: A randomized placebo-controlled clinical trial. Aesthetic Plast Surg. 2019;43:189–195. Hughes BR, Cunliffe WJ. A prospective study of the effect of isotretinoin on the follicular reservoir and sustainable sebum excretion rate in patients with acne. Arch Dermatol. 1994;130:315–318. Sharma J, Thiboutot DM, Zaenglein AL. The effects of isotretinoin on wisdom tooth extraction. J Am Acad Dermatol. 2012;67:794–795. Bower KS, Woreta F. Update on contraindications for laserassisted in situ keratomileusis and photorefractive keratectomy. Curr Opin Ophthalmol. 2014;25:251–257. Miles S, McGlathery W, Abernathie B. The importance of screening for laser-assisted in situ keratomileusis operation (LASIK) before prescribing isotretinoin. J Am Acad Dermatol. 2006;54:180–181. Chang YC, Hu DN, Wu WC. Effect of oral 13-cis-retinoic acid treatment on postoperative clinical outcome of eyes with proliferative vitreoretinopathy. Am J Ophthalmol. 2008;146:440–446. Fekrat S, de Juan E Jr, Campochiaro PA. The effect of oral 13-cis-retinoic acid on retinal redetachment after surgical repair in eyes with proliferative vitreoretinopathy. Ophthalmology. 1995;102:412–418. Charteris DG. Proliferative vitreoretinopathy: Pathobiology, surgical management, and adjunctive treatment. Br J Ophthalmol. 1995;79:953–960. 31 Retinoids and Concomitant Aesthetic Procedures Zekayi Kutlubay, Ayşegül Sevim Keçici, and Yalçın Tüzün Introduction Dermabrasion Retinoids are structural and functional analogs of vitamin A. They regulate gene transcription via intracellular nuclear receptors and have many effects on cell differentiation and proliferation, together with the immune system and embryonic developments. Retinoids may show their effects on wound healing by binding with two nuclear receptors (RAR and RXR, steroid receptor superfamily) that cause transactivation of gene expression, providing mRNA and protein synthesis and inducing epithelial proliferation and differentiation (1). Retinoids can also affect wound healing via regulating synthesis and the release of the growth factors TGF-β and IGF-1. TGF-β affects all phases of wound healing and contributes to fibroblast proliferation, chemotaxis, angiogenesis, and other growth factor−related effects. IGF-1 can increase proteoglycan and collagen synthesis, as well as fibroblast proliferation. 13-cis retinoic acid and etretinate have inhibited collagen and non-collagenous protein synthesis in fibroblast cell cultures. Etretinate is known to inhibit DNA synthesis and therefore inhibit fibroblast proliferation (2,3). Isotretinoin, a retinol derivative of vitamin A widely used in the treatment of acne, has many pharmacologic actions that affect the epidermis, sebaceous gland, and collagen formation. The drug has long been thought to have potential effects on poor wound healing, keloid development, and hypertrophic scarring, particularly in patients who undergo dermatosurgical procedures while on this agent. It is the only drug that acts on all the stages of acne formation and hence is indicated in moderate to severe acne, which otherwise could result in permanent scarring. For a long period of time, delaying cutaneous interventions for 6–12 months after systemic isotretinoin (13-cis retinoic acid) therapy has been advised, as the drug can cause hypertrophic scarring and delayed wound healing (4). This knowledge is based on three case series published in the mid-1980s describing a total of eleven patients with delayed healing and keloid development following mechanical dermabrasion and argon laser treatment (5–7); however, recent case series and clinical trials report many favorable outcomes in cases of aesthetic procedures during or after systemic retinoid use. The goals of this chapter are to establish the level of evidence for delaying procedural interventions in the setting of concurrent or recent systemic retinoid therapy and to make evidencebased recommendations for delaying or not delaying therapeutic interventions in this setting, as well as to create a comprehensive source of evidence about the underlying risks. The concern about mechanical dermabrasion in the setting of isotretinoin use arose from a series of case reports from 1985−1994, where the first published paper on the subject suggested an association of isotretinoin use with possible wound healing complications in patients undergoing full-face mechanical dermabrasion (5). Nine patients treated concomitantly with, or having recently completed, isotretinoin therapy healed at a normal rate with no postoperative complications. Other case series published in 1986 and 1988 reported a total of eight patients concomitantly receiving or having completed isotretinoin treatment 2–6 months prior, with delayed healing and keloid development following mechanical dermabrasion (6,7). A single case report published in 1994 noted delayed-onset hypertrophic scarring of the cheeks when mechanical dermabrasion was followed with a course of isotretinoin therapy (8). According to more recent studies, manual dermabrasion procedures (a minimal- to medium-depth resurfacing modality performed without connection to a rotation engine) or trichloroacetic acid (TCA) chemical peelings are considered safe during or after isotretinoin therapy, even in patients with Fitzpatrick skin types IV−V and patients with a previous history of hypertrophic acne scars (9,10). In 2016, a multicenter, prospective interventional study of microdermabrasion evaluated 504 procedural interventions performed on 183 patients with Fitzpatrick skin types IV and V. Sixty-six percent of those patients were concomitantly taking isotretinoin, the rest of them having recently completed therapy (11). Of the 504 dermatosurgical and laser procedures, only two cases of keloid were documented. On the basis of existing literature, abnormal scarring may be associated with mechanical dermabrasion in the setting of recent or concomitant isotretinoin use and is not recommended; however, delaying manual or microdermabrasion may not be necessary as there is not enough evidence for those procedures on patients who are concurrently on isotretinoin therapy or who have recently completed their therapy. Chemical Peel Many trials in the literature report favorable outcomes for patients taking systemic isotretinoin while undergoing chemical peeling. TCA and salicylic acid peelings are well tolerated, and favorable 197 198 cosmetic outcomes can be obtained in the setting of isotretinoin use without adverse effects on healing (10,12). Systemic isotretinoin can even enhance the cosmetic outcome in cases of rejuvenation. Surgical modalities of rejuvenation such as resorcinol peels and ablation have been shown to be more effective when combined with low-dose systemic isotretinoin (10–20 mg three times a week), such as noted improvement in wrinkles, thickness and color of the skin, size of pores, skin elasticity, tone, and reduction in pigmented lesions and mottled hyperpigmentation with negligible side effects (13); however, reports of some serious side effects do exist in cases of low-dose oral isotretinoin and α-hydroxy acid chemical peeling combinations, such as persistent postlesional hyperpigmentation, erosions, and scarring. Severe painful erythema and erosions that lead to permanent hyperpigmentation, scarring, and keloid formation on the face and neck can be seen with glycolic acid peeling, even after the discontinuation of systemic isotretinoin (14). Another common but benign sequela of chemical peelings during isotretinoin therapy is transient erythema (11). There is reasonable evidence to suggest that superficial chemical peels in the setting of low-dose isotretinoin treatment may not be associated with increased scarring or poor wound healing, contrary to popular belief. However, additional prospective clinical trials investigating all depths of peels in the setting of a wide dose range of isotretinoin treatment are recommended. Cutaneous Surgery The present established standard preoperative surgical care so far advises the stoppage of oral isotretinoin 6–12 months before any surgical procedure (15). This was based on the early reports of keloids or delayed wound healing in patients on isotretinoin during surgery documented in the 1980s; however, according to many multicentered studies, patients treated with a variety of cutaneous surgical procedures, such as blepharoplasties, liposuctions, fat transfers, facelifts, skin biopsies, and excisions or subcisions of scars while receiving systemic isotretinoin mostly healed without sequelae (11,13). A 2016 systematic review of oral isotretinoin use and surgical procedures concluded that the current data on coagulation disorders, liver toxic effects, kidney toxic effects, arrhythmia, and infection associated with isotretinoin use indicate that it is safe to operate on patients taking isotretinoin on the condition that preoperative blood test results fall within normal limits (16). While muscle flaps may be endangered in patients taking isotretinoin, healing of other tissues and systemic effects that could compromise surgery safety are rare. Regarding the specific setting of major reconstructive surgery requiring the mobilization of muscle flaps, patients taking isotretinoin and presenting with creatine phosphokinase (CPK) levels higher than twofold of normal may present an unusual risk factor for muscle flap failure and rhabdomyolysis. Postponing surgery until the patient displays normal CPK levels, or at least CPK levels below twofold of normal, should be recommended. Overall, there is insufficient evidence to delay cutaneous surgery for patients currently taking or having recently completed isotretinoin therapy. Testing preoperative CPK level is not warranted, particularly for cutaneous surgery not involving a muscle Retinoids in Dermatology flap or pedicle, because elevated creatine kinase level is usually a common finding in patients taking isotretinoin (17). Laser Laser interventions represent the most studied procedural category in patients taking isotretinoin. The previous literature mentions development of keloids following argon laser therapy and pulsed dye laser therapy (7,18); however, during the past two decades, laser treatments for hair removal, acne scarring, and removal of superficial benign cutaneous lesions have been used on many patients without major complications. Selective photothermolysis is the principle on which laser hair removal is based, where the target chromophore is the melanin in the hair follicle (4). By this principle, the collagen is untouched and the epidermis is not affected. Theoretically, the procedure should be safe even among patients on isotretinoin. According to a number of studies, use of diode, long-pulse flash lamp, and neodymium-doped yttrium aluminum garnet (Nd:YAG) lasers for hair removal are reported to be safe on patients concomitantly taking isotretinoin (19–22). There are also numerous case series and randomized clinical trials showing normal wound healing after treatment with ablative and nonablative fractional laser procedures in patients receiving systemic isotretinoin. Use of the 1550-nm nonablative fractionated erbium laser for acne scarring on patients has reported to be safe with respect to the recovery process and final cosmetic results (23). The 10,600-nm carbon dioxide (CO2) laser has also been found safe for the use of facial resurfacing with an ablation during or immediately after systemic isotretinoin treatment (24). Even for patients with Fitzpatrick skin types III and IV, normal postprocedural re-epithelialization without scar formation can be observed after full-face fractional ablative CO2 laser resurfacing treatments during isotretinoin use (25). Hypertrophic scarring or keloid formation is also reported to be similar after fractionated laser procedures, in cases of concomitant isotretinoin use (24). In cases of laser hair removal and other acne scar treatment options during isotretinoin use, like CO2 laser, dermaroller, and microneedling radiofrequency, only mild transient erythema may be observed but abnormal wound healing or atypical scarring is unlikely to occur (26). In one report, there were no incidences of keloid formation, hypertrophic scarring, or delayed healing in 140 procedures, including fractional erbium:yttrium-aluminumgarnet (Er:YAG) laser resurfacing, fractional CO2 laser resurfacing, and full-face CO2 laser resurfacing in patients concomitantly taking isotretinoin or who had recently completed therapy (11). Transient postinflammatory pigmentation or erythema may be observed after these types of procedures. It is possible that ablative and abrasive treatment of acne scars may give better results during oral isotretinoin therapy, as skin is primed for quicker healing. When histologically evaluated, nonablative fractional laser may induce mild epidermal hyperplasia with orthokeratosis, whereas ablative fractional laser treatment may cause papillary dermal fibrosis in addition to epidermal hyperplasia. A normal healing process has been shown even at a high dose of isotretinoin in cases of both ablative and nonablative fractional lasers, whereas fully ablative Er:YAG laser implementation may cause scarring in cases of isotretinoin use, with flattened 199 Retinoids and Concomitant Aesthetic Procedures epidermis and fully evolved dermal scar on histopathological basis (27). This finding may be explained by the different wound healing response seen with use of a fully ablative laser compared with the fractionated modalities; the fully ablative laser is nearly analogous to mechanical dermabrasion and is rarely preferred nowadays, with the frequent use of fractional ablative and nonablative lasers. There is not enough evidence to delay fractional ablative and nonablative laser treatment for patients who are currently taking or have recently completed isotretinoin treatment. Moderate to severe inflammatory acne may cause prominent scarring and should be treated as soon as possible in order to prevent permanent damage. The current practice of avoiding procedural interventions for 6–12 months in patients treated with systemic isotretinoin is in direct conflict with the approaches of early intervention of scars and delays in treatment; however, based on limited evidence, fully ablative laser procedures are not recommended in the setting of recent isotretinoin use. Other Procedures Radiofrequency devices are used in dermatology practice to either cut or coagulate exophytic lesions or for collagen stimulation in scars and rejuvenation. The limited data show both ablative radiofrequency and fractional microneedling radiofrequency to be safe (11). Similarly, skin biopsies that involve collagen damage are not expected to cause keloid formation in patients using systemic isotretinoin. Septorhinoplasty procedure in patients concomitantly using systemic isotretinoin may also cause development of nasal tip complications due to soft tissue deformities (28). The use of isotretinoin in the postoperative period after rhinoplasty may predispose to the thinning of the nasal tip skin through its interactions with collagen in the dermis. Such interactions with fibroblasts in the healing dermis may lead to increased contracture; however, there are also contrary approaches supporting the use of isotretinoin after performing rhinoplasty in order to control the overabundance of the sebaceous glands and thin the skin−subcutaneous tissue and eventually to improve the definition of the nasal tip in thick-skinned rhinoplasty patients (29). Although a direct association is not proven, postoperative alveolar osteitis after tooth extraction may be observed in patients concomitantly taking isotretinoin or who had completed treatment 1 month prior to the procedure (30). Although the molecular structure and mechanism of action are similar, there have been limited studies about the effects of acitretin on wound healing in the literature. There are contradictory results on animal studies. While some studies (31,32) are showing delayed wound healing, decrease in angiogenesis, and slowdown of the epithelization process in animal models, and scar dehiscence, others (33) demonstrate no significant intense granulation or hypertrophic scar formation. Acitretin also possesses significant benefits in cutaneous malignancy chemoprevention. Studies among organ transplant recipients taking acitretin did not demonstrate any increased rates of infection, dehiscence, hypertrophic granulation tissue, or hypertrophic scarring, for cases of both primary closure or full-thickness skin grafts and flaps after Mohs microscopic or open surgery for various skin malignancies (34). Conclusions There is not enough evidence to support the current recommendation to delay microdermabrasion, superficial chemical peels, cutaneous surgery, radiofrequency, microneedling, laser hair removal, fractional ablative, and fractional nonablative laser resurfacing for patients who are concomitantly taking or during the 6–12 months following isotretinoin therapy. These procedures can be performed safely (35,36). Aggressive procedures such as mechanical dermabrasion, fully ablative laser resurfacing, and deep peels, where there are small reports of adverse effects, are rarely performed in current practice, particularly in darker skin types, and are not recommended in the setting of isotretinoin use. These procedures may be performed with caution, most preferably after a period of 6 months of stopping the therapy. Appropriate informed consent needs to be taken in such cases, and the physician should follow all the applicable protocols. When all the studies in the literature are taken into account, there is a major need for additional well-controlled, prospective studies that can better elucidate the effect of retinoid use on scarring and wound healing. Physicians may evaluate the benefits and risks of cutaneous aesthetic procedures in the setting of retinoid treatment, and for some patients and some conditions, an informed decision may lead to earlier and potentially more effective interventions. REFERENCES 1. Talas DU, Nayci A, Atis S et al. The effects of corticosteroids and vitamin A on the healing of tracheal anastomoses. Int J Pediatr Otorhinolaryngol. 2003;67:109–116. 2. Shigematsu T, Tajima S. Modulation of collagen synthesis and cell proliferation by retinoids in human skin fibroblasts. J Dermatol Sci. 1995;9:142–145. 3. Ohta A, Louie JS, Uitto J. Retinoid modulation of collagenase production by adherent human mononuclear cells in culture. Ann Rheum Dis. 1987;46:357–362. 4. Zaenglein AL, Thiboutot DM. Acne vulgaris. In: Bolognia JL, Jorizzo JL, Schaffer JV, editors. Dermatology. 3rd ed. Philadelphia, PA: Elsevier, 2012; p. 558. 5. Roenigk HH Jr, Pinski JB, Robinson JK et al. Acne, retinoids, and dermabrasion. J Dermatol Surg Oncol. 1985;11:396–398. 6. Rubenstein R, Roenigk HH Jr, Stegman SJ et al. Atypical keloids after dermabrasion of patients taking isotretinoin. J Am Acad Dermatol. 1986;15:280–285. 7. Zachariae H. Delayed wound healing and keloid formation following argon laser treatment or dermabrasion during isotretinoin treatment. Br J Dermatol. 1988;118:703–706. 8. Katz BE, MacFarlane DF. Atypical facial scarring after isotretinoin therapy in a patient with previous dermabrasion. J Am Acad Dermatol. 1994;30:852–853. 9. Bagatin E, dos Santos Guadanhim LR, Yarak S et al. Dermabrasion for acne scars during treatment with oral isotretinoin. Dermatol Surg. 2010;36:483–489. 10. Picosse FR, Yarak S, Cabral NC et al. Early chemabrasion for acne scars after treatment with oral isotretinoin. Dermatol Surg. 2012;38:1521–1526. 200 11. Mahadevappa OH, Mysore V, Viswanath V et al. Surgical outcome in patients taking concomitant or recent intake of oral isotretinoin: A multicentric study-ISO-AIMS study. J Cutan Aesthet Surg. 2016;9:106–114. 12. Kar BR, Tripathy S, Panda M. Comparative study of oral isotretinoin versus oral isotretinoin + 20% salicylic acid peel in the treatment of active acne. J Cutan Aesthet Surg. 2013;6:204–208. 13. Hernandez-Perez E, Khawaja HA, Alvarez TY. Oral isotretinoin as part of the treatment of cutaneous aging. Dermatol Surg. 2000;26:649–652. 14. Gerber PA, Kukova G, Bölke E et al. Severe hyperpigmentation and scarring following glycolic acid peel treatment in combination with low-dose isotretinoin. Eur J Med Res. 2014;19:60. 15. Abdelmalek M, Spencer J. Retinoids and wound healing. Dermatol Surg. 2006;32:1219–1230. 16. Ungarelli LF, Hetem CM, Farina Junior JA. Is it safe to operate on patients taking isotretinoin? Aesthetic Plast Surg. 2016;40:139–148. 17. Landau M, Mesterman R, Ophir J et al. Clinical significance of markedly elevated serum creatine kinase levels in patients with acne on isotretinoin. Acta Derm Venereol. 2001;81:350–352. 18. Bernestein LJ, Geronemus RG. Keloid formation with the 585-nm pulsed dye laser during isotretinoin treatment. Arch Dermatol. 1997;133:111–112. 19. Khatri KA. Diode laser hair removal in patients undergoing isotretinoin therapy. Dermatol Surg. 2004;30:1205–1207. 20. Cassano N, Arpaia N, Vena GA. Diode laser hair removal and isotretinoin therapy. Dermatol Surg. 2005;31:380–381. 21. Khatri KA, Garcia V. Light-assisted hair removal in patients undergoing isotretinoin therapy. Dermatol Surg. 2006;32:875–877. 22. Khatri KA. The safety of long-pulsed Nd:YAG laser hair removal in skin types III-V patients during concomitant isotretinoin therapy. J Cosmet Laser Ther. 2009;11:56–60. 23. Leal H, Cantu P. Fractional erbium laser during oral isotretinoin treatment. J Am Acad Dermatol. 2011;62:AB18. Retinoids in Dermatology 24. Yoon JH, Park EJ, Kwon IH et al. Concomitant use of an infrared fractional laser with low-dose isotretinoin for the treatment of acne and acne scars. J Dermatolog Treat. 2014;25:142–146. 25. Kim HW, Chang SE, Kim JE et al. The safe delivery of fractional ablative carbon dioxide laser treatment for acne scars in Asian patients receiving oral isotretinoin. Dermatol Surg. 2014;40:1361–1366. 26. Chandrashekar BS, Varsha DV, Vasanth V et al. Safety of performing invasive acne scar treatment and laser hair removal in patients on oral isotretinoin: A retrospective study of 110 patients. Int J Dermatol. 2014;53:1281–1285. 27. Khatri KA, Iqbal N, Bhawan J. Laser skin resurfacing during isotretinoin therapy. Dermatol Surg. 2015;41:758–759. 28. Allen BC, Rhee JS. Complications associated with isotretinoin use after rhinoplasty. Aesthetic Plast Surg. 2005;29:102–106. 29. Cobo R, Vitery L. Isotretinoin use in thick-skinned rhinoplasty patients. Facial Plast Surg. 2016;32:656–661. 30. Sharma J, Thiboutot DM, Zaenglein AL. The effects of isotretinoin on wisdom tooth extraction. J Am Acad Dermatol. 2012;67:794–795. 31. Gunes Bilgili S, Calka O, Akdeniz N et al. The effects of retinoids on secondary wound healing: Biometrical and histopathological study in rats. J Dermatolog Treat. 2013;24:283–289. 32. Aksoy HM, Aksoy B, Çalikoglu E. Systemic retinoids and scar dehiscence. Indian J Dermatol. 2019;64:68–70. 33. Frosch PJ, Czarnetzki BM. Effect of retinoids on wound healing in diabetic rats. Arch Dermatol Res. 1989;281:424–426. 34. Tan SR, Tope WD. Effect of acitretin on wound healing in organ transplant recipients. Dermatol Surg. 2004;30:667–673. 35. Mysore V, Mahadevappa OH, Barua S et al. Standard guidelines of care: Performing procedures in patients on or recently administered with isotretinoin. J Cutan Aesthet Surg. 2017;10:186–194. 36. Spring LK, Krakowski AC, Alam M et al. Isotretinoin and timing of procedural interventions: A systematic review ­ with consensus recommendations. JAMA Dermatol. 2017;153:802–809. 32 Laboratory and Clinical Follow-Up Nadide Burcu Öztürk and Berna Aksoy Introduction Retinoids are metabolites and synthetic analogs of vitamin A (retinol) that are not only commonly used in dermatologic practice, but are also irreplaceable in the treatment of many diseases, including acne and psoriasis. The primary drugs in this group include isotretinoin, acitretin, bexarotene, and alitretinoin. Isotretinoin, acitretin, and bexarotene have been approved by the United States Food and Drug Administration (FDA) for the treatment of acne, psoriasis, and cutaneous T-cell lymphoma, respectively, but they have been used in the treatment of many other diseases with success. Alitretinoin is used for chronic hand dermatitis. In general, their efficacy improves with increased dosage, although the frequency of common mucocutaneous and metabolic side effects also increases. In general, most side effects are dose-dependent and reversible; however, by definition, teratogenicity is the most significant problem associated with retinoids. All retinoids are in the X class in pregnancy, indicating that no pregnant woman or someone intending to become pregnant would have these agents prescribed. Isotretinoin Isotretinoin (13-cis retinoic acid) is a natural physiologic compound that is produced by the metabolism of vitamin A. It was approved by the FDA in 1982 for the treatment of severe and resistant nodular acne. Isotretinoin has important mucocutaneous, metabolic, and teratogenic side effects. When considering the use of isotretinoin and other retinoids, the physician should evaluate the prospective candidate for liver disease, lipid abnormalities, and psychiatric disorders prior to treatment. In addition, tetracyclines should not be used during retinoid therapy. Isotretinoin is teratogenic, as with all other systemic retinoids, and leads to characteristic congenital defects known as retinoic acid embryopathy, encompassing a wide spectrum of birth defects including craniofacial, heart, and nervous system malformations. It has no long-term effect on fertility, and any risk of fetal malformation returns to normal 1 month after treatment. Because isotretinoin can no longer be found in the body 1 month after completion of a course of treatment, there would not be any further prohibition against pregnancy (1). In addition, there are no clear data regarding the necessity and duration of contraception for men; however, there is no evidence of retinoid embryopathy or fetal malformations following conception by men taking isotretinoin, acitretin, bexarotene, or alitretinoin (2). Many risk management programs have been produced to prevent the teratogenic effects of isotretinoin and to control the use of the drug among women. The iPLEDGE program, initiated in 2006 by the FDA, is the most well known. Patients are informed of teratogenicity, and a written record is obtained. As a precaution, women of childbearing potential are required to use two complementary contraceptive methods, have a monthly pregnancy evaluation after starting treatment with isotretinoin, perform at least two pregnancy tests prior to beginning the drug and obtain two negative results, and to start the drug on the second or third day of the next menstrual period (3). Many of the side effects associated with the drug resemble those of the hypervitaminosis A, as might be expected from an analog of vitamin A. Several side effects, including mucocutaneous and gastrointestinal side effects, are lessened when the drug is administered twice daily (4). Patients should be informed about common side effects, particularly mucocutaneous toxicity, prior to the start of treatment, and signs and symptoms should be monitored at each clinical visit (4–6). The most common mucocutaneous side effect is cheilitis, which can approach 100% of acne patients being treated (7–9). Other less common mucocutaneous side effects include mucosal dryness, dry eyes, xerosis, pruritus, retinoid dermatitis, epistaxis, ingrown nail, and periungual granulation tissue (10). Isotretinoin may also result in numerous ophthalmic side effects, including dry eyes and night blindness. Because it may cause impaired night vision and difficulty in adapting to darkness (2,11), pilots, train engineers, bus drivers, and those in other occupations requiring night vision should be warned. Many case reports and case series have been presented on the psychiatric side effects of isotretinoin, although the results of the performed studies are controversial (4,12–14). Several reports suggest that predisposed individuals may be at risk for worsening of psychiatric symptoms when starting systemic isotretinoin treatment. Patients should be evaluated before the start of treatment for signs of any psychiatric disorder and re-evaluated at each visit for signs of depression or suicidal ideation. In general, patients should be informed about the possible risk of depression and suicidal tendencies, and patients should be referred for psychiatric appraisal when necessary. Some patients may also experience headaches and fatigue. These patients should be examined for pseudotumor cerebri if the headache is continuous and unresponsive to medication, 201 202 because benign intracranial hypertension (pseudotumor cerebri) may occur on rare occasions during treatment (4,5). Bone pain may be seen during isotretinoin treatment (15). Myalgia is seen in 15% of patients (7,16) and is more prominent after exercise in general. Patients should be questioned about presence of any pain at each clinical visit and advised to avoid excessive exercise. Some gastrointestinal symptoms, such as nausea, diarrhea, and abdominal pain, may occur. The symptoms of inflammatory bowel disease may increase or develop for the first time, although this topic is controversial (17–19). Patients should also be questioned about the presence of any gastrointestinal symptoms at each clinical visit. The most common and significant laboratory side effect of isotretinoin is its effect on lipid levels. Reversible hypertriglyceridemia is seen in the first month in 25% of patients, accompanied by elevated total cholesterol and low-density lipoprotein (LDL) levels and decreased high-density lipoprotein (HDL) concentrations. Acute pancreatitis may be seen in cases of severe hypertriglyceridemia (5), and dose reduction and/or additional antihyperlipidemic agents are recommended when triglyceride levels reach 500 mg/dL. Treatment cessation is recommended when no improvement is seen despite administration of antihyperlipidemic agents (4,20). Liver function tests may be mildly or moderately elevated in 15% of patients (20), but these are reversible. The elevation of transaminases has been reported as mild in general, while severe lipid and transaminase elevations have been observed as transient and reversible in general in a study of 13,772 patients with acne undergoing isotretinoin treatment (21). Baseline fasting triglyceride levels, cholesterol levels, and liver function tests (aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, lactate dehydrogenase) should be evaluated prior to the start of therapy. Repeat laboratory studies now appear to be optional (22). Previously it has been suggested that liver function tests, cholesterol, triglyceride, and LDL cholesterol levels be checked monthly if they are initially in the upper limits, and at 2- to 3-month intervals in the remaining conditions in order to decrease costs (23). A recent study suggests that in healthy patients with normal baseline lipid panel and liver function test results, repeated studies may be performed at the second month of isotretinoin therapy. If findings are normal, no further testing may be required (24). Dose reductions are recommended when the results of liver function tests are found to be elevated two- to threefold above normal levels, and treatment should be stopped when no improvement is seen with dose reduction. When the results of liver function tests are elevated more than threefold above normal levels, the treatment should be stopped (4,20). Other dose-dependent changes are a decreased number of leukocytes and neutrophils, thrombocytopenia, and agranulocytosis (20), although no impairment in the hematological parameters was seen in general in previous studies. It was thus concluded that no routine follow-up of hemoglobin, leukocyte, and platelet levels is required unless there is a clinical suspicion during systemic retinoid treatment (24,25). Acitretin Acitretin has significant metabolic, skeletal, and teratogenic side effects (26). Accordingly, patients should be questioned in Retinoids in Dermatology detail and tests should be made prior to the start of treatment and regularly during treatment to prevent or lessen the possible side effects that may develop. Patients should be evaluated in particular for the presence of liver and kidney disease prior to treatment, and for the use of any drugs that may interact with acitretin. Acitretin use by women of reproductive age should be avoided due to its teratogenic effect. Because the possibility of teratogenicity can exist for up to 3 years following treatment, contraceptive precautions should be continued after completion of the acitretin regimen. This includes two negative pregnancy tests prior to initiation of treatment, and monthly thereafter (26). It has been recommended that a pregnancy test should be performed in the final 2 weeks prior to the start of the treatment, and that treatment should be started on the second or third day of the following menstrual cycle. The Association of the British Pharmaceutical Industry recommends contraception starting at least 4 weeks prior to treatment, during treatment, and for 3 years after treatment, and similarly, in the United States, contraception is recommended for 3 years after the cessation of treatment (26). There is as yet no definitive data about male patients for this period (27). The FDA specifies that the drug not be used during lactation, although the amount of drug passing to the breast milk is minimal (28). The skeletal toxicity of retinoids is a debatable issue. The effects of acitretin defined in previous reports have been heterogeneous, containing no information on pretreatment conditions (29–31). In addition, no radiologic follow-up has been recommended in any report, as skeletal toxicity during acitretin treatment has yet to be proven (32). That said, the possible effects on the skeletal system include hyperostosis and/or osteoporosis (26,33). There is no consensus on the pretreatment evaluation, and treatment should be continued while pediatric patients are being followed up closely for growth parameters and any abnormalities in bone development during treatment. The drug may also cause mucocutaneous side effects requiring dose reductions, with the most commonly seen effects being a result of dryness of the skin and mucosae. Cheilitis is a doserelated, preventable, and transient condition, and the treatment may be associated with other well-known retinoid-related mucocutaneous adverse effects including epistaxis, xerosis, and hair loss (25,33–35). Severe mucocutaneous side effects have been reported to be dose-dependent, with an increased risk reported in some publications at high doses such as 50–75 mg daily (35–37). Patients should be informed about the most common mucocutaneous side effects before the start of treatment and monitored at each clinical visit. Cases of idiopathic intracranial hypertension have been reported with the use of acitretin (38), and a fundoscopic examination of the eye should be performed in the presence of such complaints as severe headache, nausea, vomiting, and problems with vision (34). Visual impairments may include decreased color image, blurred vision, and decreased night vision (26,33,35), although dry eyes and irritation are among the most common ophthalmological side effects in this regard. Drivers and pilots should be warned about these side effects, and use of contact lenses may also be limited (39). An increase in liver enzymes may occur due to hepatotoxicity (26,33,35), with transient and reversible increases in liver 203 Laboratory and Clinical Follow-Up enzymes having been reported in more than 15% of patients using acitretin in studies (34,40), although severe hepatotoxic reactions such as cholestatic hepatitis and cirrhosis are rare (41). There were no liver toxicities in liver biopsies taken before and after treatment in patients receiving 25–50 mg acitretin daily for 2 years (40), although chemical hepatitis was reported in a small number of patients in a study evaluating 1877 patients receiving acitretin (34). A gastroenterology consultation should be requested when bilirubin levels reach >50 µmol/L (3 mg/dL) or ALT is >200 IU/L, and acitretin dose should be reduced when the levels of the transaminases are more than twofold the normal levels. In cases where treatment is stopped, transaminase levels should be checked at 1- to 2-week intervals until they decline to normal levels. Restarting at lower doses is recommended under such circumstances (25). Acitretin may also cause hyperlipidemia (25,26,33), which is directly proportional to the acitretin dose and ameliorates in general 4–8 weeks after the cessation of treatment (41). Increased triglyceride and cholesterol levels are seen in 20%–40% and 10%–30% of patients, respectively. The lipid levels of patients undergoing acitretin treatment should be tested regularly, since decreased HDL levels in addition to an increase in very low-density lipoproteins and LDL can lead to an increased risk of cardiovascular diseases (42–44). One case has been reported with pancreatitis due to high serum triglyceride levels (41), while those with diabetes, obesity, and excessive alcohol use and those with a family history of hypertriglyceridemia are in the high-risk group for development of pancreatitis. If the therapeutic response is good but the serum lipid levels are continuously elevated, dietary precautions should be taken prior to the start of a lipid-lowering drug. A triglyceride level of >5 mmol/L (442.48 mg/dL) necessitates evaluation by a lipidologist, while other causes of hypertriglyceridemia are also required to be evaluated. A triglyceride level higher than 10 mmol/L (884.96 mg/dL) requires cessation of treatment and evaluation of the patient by a lipidologist, since this condition may be a risk factor for acute pancreatitis (19). Incidences of vulvovaginitis caused by Candida albicans have also been reported during acitretin treatment (45). Acitretin use with antidiabetic drugs may cause hypoglycemia due to increased insulin sensitivity (46). Such patients are advised to check their glucose levels regularly and even more often than normal during the early phases of the treatment. In a study evaluating the effects of acitretin on wound healing, 44 complex wounds in transplant recipients were followed up, and no significant effect of the drug during the treatment period was observed in wound infection, dehiscence, hypertrophic scarring, or hypergranulation, meaning that there was no need to cease treatment during routine operative procedures (47). The risk of side effects is reported to increase with high daily doses of acitretin of 50–75 mg, resulting in the cessation of treatment due to decreased patient tolerance. Accordingly, it is recommended that the administered dosages be adjusted in order to optimize the effect and compliance and to reduce side effects. Clinical evaluation for the response to treatment should be made after the 12th week of treatment (33). There are some drugs that should be used with caution during acitretin treatment due to the potential for drug interactions and common side effects, as summarized in Table 32.1. TABLE 32.1 Drug Interactions of Acitretin Drug Tetracycline-group antibiotics Methotrexate Etretinate Antidiabetic drugs Oral contraceptives Vitamin A Phenytoin Rifampin, phenobarbital, carbamazepine Imidazole-group antifungals Lipid-lowering drugs (gemfibrozil and statins) Comment Risk of development of pseudotumor cerebri (34) Increased risk of liver toxicity (48) Attacks of sporadic toxic hepatitis (48) Potential for hypoglycemia (46) Acitretin decreases the anti-ovulatory effects only when it is used with progestin-only pills. It has no effect on combined preparations (49) Dietary intake should not exceed the daily dose recommended (2400–3000 IU daily) Acitretin increases free phenytoin levels due to the decreasing effect of it on the phenytoinbinding protein (33,50) Lowered serum acitretin level (2) Increased risk of liver toxicity (51) Increased risk of myotoxicity (51) In general, a complete blood count, liver function studies, serum creatinine, urea, fasting blood sugar, triglycerides, cholesterol, and HDL levels should be measured prior to treatment, after which measurements should be taken monthly at the beginning for 1–2 months, every 3 months thereafter, and following each dose increase. Laboratory tests should be carried out more often if the patient has diabetes, obesity, alcoholism, cardiovascular risk factors, lipid metabolism disorders, or a family history of any such conditions (26). Pregnancy tests should be repeated every month. Daily treatment doses should be reduced in the event of a more than twofold increase in the results of liver function tests and should be stopped when they increase threefold. Weekly tests are recommended when an abnormality in the results is detected (26). Treatment may be stopped for some time as necessary and then started again at a lower dose. Diet and lifestyle changes should be applied before starting a course of lipid-lowering drugs in the event of increased lipid levels. Patients who have been administered acitretin should not donate blood during treatment and for 3 years after the cessation of treatment due to the possibility of acitretin being metabolically converted to etretinate. Patients should refrain from alcohol during treatment, and female patients should not consume alcohol for 2 months following the cessation of treatment. Bexarotene Bexarotene was approved by the FDA in 1999 for patients with cutaneous T-cell lymphoma (CTCL) in all stages who have previously received at least one systemic treatment. It was licensed as a 75-mg soft gelatin capsule in 2002. The manufacturer’s recommended dosage of bexarotene is 300 mg/m2, which is effective in all stages of CTCL (52,53). The rate of response to treatment increases with an increased dose of bexarotene. The drug should be administered at least 8 weeks prior to evaluation of the efficacy of treatment, with 204 Retinoids in Dermatology the highest response rate observed to occur after a mean of 3 months of treatment. The period of response was reported to be 8 months. Treatment dose can be increased to 400 mg/m2 when no response is achieved in the eighth week of treatment, although the patient should be closely followed up for side effects (52–54). Hyperlipidemia and hypothyroidism develop in the majority of patients being treated with bexarotene. In a study involving 66 patients, all were reported to develop hyperlipidemia and hypothyroidism during oral bexarotene treatment for mycosis fungoides (MF) (54). Hyperlipidemia is frequently seen in doses higher than 300 mg/m2/daily, and it is more frequently characterized with an increase in triglyceride levels (55). An algorithm has been developed to prevent the development of hyperlipidemia during treatment with bexarotene, such that antihyperlipidemic drugs should be started 1–2 weeks before the start of bexarotene treatment (56). Central hypothyroidism may develop secondary to the drug intake during bexarotene treatment (57), having been reported in 40% of cases in clinical studies. Preventive treatment methods should be started early in order to prevent the development of side effects, and patients should be closely followed up (58). A decrease in T4 level is observed in patients 2–3 weeks after the start of treatment (59). Central hypothyroidism secondary to bexarotene improves 1–2 weeks after the cessation of treatment (53). Hyperlipidemia and central hypothyroidism are the most frequently reported side effects among patients receiving bexarotene (54). In a clinical study of patients being treated with bexarotene, dyslipidemia and secondary hypothyroidism were reported in 100% and 40%–100% of patients, respectively, and the most severe side effect in the study was the development of acute pancreatitis due to elevated triglycerides (52,55). The other side effects occurring during oral bexarotene treatment are lethargy, myalgia, anemia, neutropenia, leukopenia, elevated liver enzymes, hepatitis, nausea, vomiting, diarrhea, exfoliation, itching, cataract, and extracutaneous lymphoma (54,60). Dose-dependent leukopenia has been reported to develop in 28% of patients at 4–8 weeks. Leukopenia is reversible and resolves when the dose is decreased or stopped (2). Pregnant patients or patients looking to become pregnant should refrain from all types of retinoid treatments including bexarotene due to their teratogenic effects (58). The side effects of topical bexarotene are limited to the area of application in general, and the reported side effects to date are rashes, irritation, itching, pain at the application site, and asymptomatic retinoid erythema (61). Bexarotene is the only FDA-approved systemic retinoid in MF treatment, although close follow-up is required to identify such side effects during treatment as hyperlipidemia and hypothyroidism. Starting on antihyperlipidemic drugs prior to treatment will permit long-term use of bexarotene in optimal doses, and using topical bexarotene rather than oral bexarotene in cases with localized lesions is a safer alternative. As in the case of other retinoids, any woman of childbearing potential must not become pregnant while taking alitretinoin and for at least 1 month after its discontinuation. Physicians should inform patients about teratogenicity and adopt iPLEDGE or pregnancy prevention program (PPP) program. Alitretinoin does not appear to pose a risk to female partner or to fetus in the case of pregnant partner of a male patient (62). Alitretinoin treatment is associated with an overall 23% rate of development of side effects, headache (7.5%), increased blood triglycerides (4.9%), and increased blood cholesterol (3.8%) being the most frequent. Treatment discontinuation was mostly due to headache or increased triglyceride levels (63). Alitretinoin is associated with dyslipidemia. This is especially prevalent in patients with obesity, diabetes, alcohol intake, and a family history of dyslipidemia. Therefore, fasting glucose, total cholesterol, and triglyceride levels should be checked before and after the start of treatment. If triglyceride levels rise to uncontrollable high levels or signs of pancreatitis develop, treatment should be discontinued (62). Treatment with any systemic retinoid, including alitretinoin, can be associated with transient and reversible increases in liver transaminases. Reduction of the dose or discontinuation of alitretinoin treatment should be considered in the case of persistent and clinically relevant elevation of transaminases to more than two- to threefold increase of the normal levels (62). Like all other retinoids, alitretinoin can cause xerosis, cheilitis, photosensitivity, dry eye, arthralgia, and myalgia (62). Alitretinoin can also be associated with psychiatric alterations. Prior to initiation of alitretinoin treatment and at each visit during therapy, patients should be asked about depression, mood disturbance, or any psychiatric disorder (62). Alitretinoin treatment should be regularly followed up and pregnancy test, serum transaminases, blood lipid levels, and fasting blood glucose levels should be obtained before treatment and at 1 month after start of treatment. Monthly pregnancy tests should be performed in women of childbearing potential. Other tests are required as clinically needed (62). The National Institute for Health and Clinical Excellence (NICE) recommends that alitretinoin be prescribed to patients with severe chronic hand dermatitis and a Dermatology Life Quality Index (DLQI) score of at least 15. NICE recommends that alitretinoin treatment be stopped as soon as an adequate response is obtained, if chronic hand dermatitis continues to be severe at 12 weeks of treatment, or if response is inadequate at 24 weeks of treatment (64). Topical alitretinoin gel is indicated for Kaposi sarcoma, and got FDA approval in 1999. Adverse events related to topical treatment with alitretinoin gel tend to be mild to moderate in severity and are limited to the site of application. The most frequent adverse event is skin irritation occurring at the application site (32%) followed by paresthesia, itch, pain, and peeling (65). Physicians should inform patients about these application site reactions. Alitretinoin Conclusions Alitretinoin is indicated for the treatment of chronic hand dermatitis that is refractory to potent topical corticosteroids in adults (over 18 years) (62). Isotretinoin, acitretin, bexarotene, and alitretinoin have important mucocutaneous, metabolic, and teratogenic side effects. Accordingly, patients should be questioned in detail about the Laboratory and Clinical Follow-Up various side effects at each clinical visit and appropriate tests should be run prior to the start of treatment and during treatment to identify the possible side effects that may develop. All retinoids are teratogenic; appropriate precautions and close followup should be undertaken in women of childbearing potential. Bexarotene treatment requires close follow-up to identify important side effects of hyperlipidemia and hypothyroidism. When appropriate clinical and laboratory follow-up is performed, retinoids can be safely and effectively used in the treatment of various dermatologic disorders. REFERENCES 1. Thielitz A, Krautheim A, Gollnick H. Update in retinoid therapy of acne. Dermatologic Therapy. 2006;19:272–279. 2. Patton TJ, Lara FK. Systemic retinoids. In: Wolverton SE, editor. Comprehensive Dermatologic Drug Therapy. 2nd ed. Philadelphia, PA: Saunders-Elsevier, 2007; pp. 275–300. 3. Goodfield MJ, Cox NH, Bowser A et al. Advice on the safe introduction and continued use of isotretinoin in acne in the U.K. 2010. Br J Dermatol. 2010;162:1172–1179. 4. Ellis CN, Krach KJ. Uses and complications of isotretinoin therapy. J Am Acad Dermatol. 2001;45:150–157. 5. Brelsford M, Beute TC. Preventing and managing the side effects of isotretinoin. Semin Cutan Med Surg. 2008;27:197–206. 6. Scheinfeld N, Bangalore S. Facial edema induced by isotretinoin use: A case and a review of the side effects of isotretinoin. J Drugs Dermatol. 2006;5:467–468. 7. Polat M, Oztaş P, İlhan MN et al. Clinical side-effects and results of systemic isotretinoin treatment in patients with nodulocystic acne. T Klin Dermatol. 2008;18:72–76. 8. Kaymak Y, Ilter N. The results and side effects of systemic isotretinoin treatment in 100 patients with acne vulgaris. Dermatol Nurs. 2006;18:576–580. 9. Çıkım AÇ, Seyhan M. Akne vulgaris tedavisinde izotretinoinin etkinliği ve yan etkileri. Turkderm. 2008;42:51–55. 10. Wolverton SE, Harper JC. Important controversies associated with isotretinoin therapy for acne. Am J Clin Dermatol. 2013;14:71–76. 11. Lammer EJ, Chen DT, Hoar RM et al. Retinoic acid embryopathy. N Engl J Med. 1985;313:837–841. 12. Kellett SC, Gawkrodger DJ. A prospective study of the responsiveness of depression and suicidal ideation in acne patients to different phases of isotretinoin therapy. Eur J Dermatol. 2005;15:484–488. 13. Bremner JD, Shearer KD, McCaffery PJ. Retinoic acid and affective disorders: The evidence for an association. J Clin Psychiatry. 2012; 73:37–50. 14. Schaffer LC, Schaffer CB, Hunter S et al. Psychiatric reactions to isotretinoin in patients with bipolar disorder. J Affect Disord. 2010;122:306–308. 15. Aktan Ş. Retinoidler. In: Tüzün Y, Gürer MA, Serdaroğlu S et al. editors. Dermatoloji. İstanbul: Nobel Tıp Kitabevi, 2008; pp. 2230–2237. 16. Meigel WN. How safe is oral isotretinoin? Dermatology. 1997;195:22–28. 17. Passier JL, Srivastava N, van Puijenbroek EP. Isotretinoininduced inflammatory bowel disease. Neth J Med. 2006;64:52–54. 205 18. Bernstein CN, Nugent Z, Longobardi T et al. Isotretinoin is not associated with inflammatory bowel disease: A population-based case-control study. Am J Gastroenterol. 2009;104:2774–2778. 19. Crockett SD, Porter CQ, Martin CF et al. Isotretinoin use and the risk of inflammatory bowel disease: A case-control study. Am J Gastroenterol. 2010;105:1986–1993. 20. Charakida A, Mouser PE, Chu AC. Safety and side effects of the acne drug, oral isotretinoin. Expert Opin Drug Saf. 2004;3:119–129. 21. Zane LT, Leyden WA, Marqueling AL et al. A populationbased analysis of laboratory abnormalities during isotretinoin therapy for acne vulgaris. Arch Dermatol. 2006;142: 1016–1022. 22. Altman RS, Altman LJ, Altman JS. A proposed set of new guidelines for routine blood tests during isotretinoin therapy for acne vulgaris. Dermatology. 2002;204:232–235. 23. Ertam I, Alper S, Unal I. Is it necessary to have routine blood tests in patients treated with isotretinoin? J Dermatolog Treat. 2006;17:214–216. 24. Hansen TJ, Lucking S, Miller JJ et al. Standardized laboratory monitoring with use of isotretinoin in acne. J Am Acad Dermatol. 2016;75:323–328. 25. Ormerod A, Campalani E, Goodfield M. British Association of Dermatologists guidelines on the efficacy and use of acitretin in dermatology. Br J Dermatol. 2010;162:952–963. 26. Soriatane [product monograph]. US: Allergan Inc; 2018. Available at: https://soriatane.ca/Physician_Information/ Product_Monograph. 27. Geiger JM, Walker M. Is there a reproductive safety risk in male patients treated with acitretin (Neotigason/Soriatane)? Dermatology. 2002;205:105–107. 28. Bae YS, Van Voorhees AS, Hsu S et al. Review of treatment options for psoriasis in pregnant or lactating women: From the Medical Board of the National Psoriasis Foundation. J Am Acad Dermatol. 2012;67:459–477. 29. DiGiovanna JJ, Helfgott RK, Gerber LH et al. Extraspinal tendon and ligament calcification associated with long-term therapy with etretinate. N Engl J Med. 1986;315:1177–1182. 30. Okada N, Nomura M, Morimoto S et al. Bone mineral density of the lumbar spine in psoriatic patients with long term etretinate therapy. J Dermatol. 1994;21:308–311. 31. Halkier-Sørensen L, Andresen J. A retrospective study of bone changes in adults treated with etretinate. J Am Acad Dermatol. 1989;20:83–87. 32. Van Dooren-Greebe RJ, Lemmens JA, De Boo T et al. Prolonged treatment with oral retinoids in adults: No influence on the frequency and severity of spinal abnormalities. Br J Dermatol. 1996;134:71–76. 33. Menter A, Korman NJ, Elmets C et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol. 2009;61:451–485. 34. Katz HI, Waalen J, Leach EE. Acitretin in psoriasis: An overview of adverse effects. J Am Acad Dermatol. 1999;41:7–12. 35. Gollnick HPM. Oral retinoids–efficacy and toxicity in psoriasis. Br J Dermatol. 1996;135:6–17. 36. Kragballe K, Jansen CT, Geiger JM et al. A double-blind comparison of acitretin and etretinate in the treatment of severe psoriasis—Results of a Nordic multicenter study. Acta Derm Venereol (Stockh). 1989;69:35–40. 206 37. Geiger JM, Czarnetzki BM. Acitretin (Ro 10-1670, etretin): Overall evaluation of clinical studies. Dermatologica. 1988;176:182–190. 38. Starling J, Koo J. Evidence based or theoretical concern? Pseudotumor cerebri and depression as acitretin side effects. J Drugs Dermatol. 2005;4:690–696. 39. Geiger JM, Saurat JH. Acitretin and etretinate. How and when they should be used. Dermatol Clin. 1993;11:117–129. 40. Roenigk HH Jr, Callen JP, Guzzo CA et al. Effects of acitretin on the liver. J Am Acad Dermatol. 1999;41:584–588. 41. Vahlquist C, Selinus I, Vessby B. Serum-lipid changes during acitretin (etretin) treatment of psoriasis and palmoplantar pustulosis. Acta Derm Venereol (Stockh). 1988;68:300–305. 42. Davidson MH, Stein EA, Bays HE et al. Efficacy and tolerability of adding prescription omega-3 fatty acids 4 g/d to simvastatin 40 mg/d in hypertriglyceridemic patients: An 8-week, randomized, double-blind, placebo-controlled study. Clin Ther. 2007;29:1354–1367. 43. Ashley JM, Lowe NJ, Borok ME et al. Fish oil supplementation results in decreased hypertriglyceridemia in patients with psoriasis undergoing etretinate or acitretin therapy. J Am Acad Dermatol. 1988;19:76–82. 44. Vahlquist C, Olsson AG, Lindholm A et al. Effects of gemfibrozil (Lopid) on hyperlipidemia in acitretin-treated patients. Results of a double-blind cross-over study. Acta Derm Venereol (Stockh). 1995;75:377–380. 45. Sturkenboom MC, Middelbeek A, de Jong van den Berg LT et al. Vulvo-vaginal candidiasis associated with acitretin. J Clin Epidemiol. 1995;48:991–997. 46. Hartmann D, Forgo I, Dubach UC et al. Effect of acitretin on the response to an intravenous glucose-tolerance test in healthy volunteers. Eur J Clin Pharmacol. 1992;42:523–528. 47. Tan SR, Tope WD. Effect of acitretin on wound healing in organ transplant recipients. Dermatol Surg. 2004;30: 667–673. 48. Beck HI, Foged EK. Toxic hepatitis due to combination therapy with methotrexate and etretinate in psoriasis. Dermatologica. 1983;167:94–96. 49. Berbis P, Bun H, Geiger JM et al. Acitretin (RO10-1670) and oral contraceptives: Interaction study. Arch Dermatol Res. 1988;280:388–389. 50. Guenther LC. Alefacept is safe and efficacious in the treatment of palmar plantar pustulosis. J Cutan Med Surg. 2007;11:202–205. 51. Pathirana D, Omerod AD, Saiag P et al. European S3-guidelines on the systemic treatment of psoriasis vulgaris. J Eur Acad Dermatol Venereol. 2009;23:S5–S70. Retinoids in Dermatology 52. Duvic M, Martin AG, Kim Y et al. Phase 2 and 3 clinical trial of oral bexarotene (Targretin capsules) for the treatment of refractory or persistent early-stage cutaneous T-cell lymphoma. Arch Dermatol. 2001;137:581–593. 53. Duvic M, Hymes K, Heald P et al. Bexarotene is effective and safe for treatment of refractory advanced-stage cutaneous T-cell lymphoma: Multinational phase II-III trial results. J Clin Oncol. 2001;19:2456–2471. 54. Abbott RA, Whittaker SJ, Morris SL et al. Bexarotene therapy for mycosis fungoides and Sezary syndrome. Br J Dermatol. 2009;160:1299–1307. 55. Sokołowska-Wojdyło M, Lugowska-Umer H, MaciejewskaRadomska A. Oral retinoids and rexinoids in cutaneous T-cell lymphomas. Postepy Dermatol Alergol. 2013;30:19–29. 56. Talpur R, Ward S, Apisarnthanarax N et al. Optimizing bexarotene therapy for cutaneous T-cell lymphoma. J Am Acad Dermatol. 2002;47:672–684. 57. Smit JW, Stokkel MP, Pereira AM et al. Bexarotene-induced hypothyroidism: Bexarotene stimulates the peripheral metabolism of thyroid hormones. J Clin Endocrinol Metab. 2007;92:2496–2499. 58. Huen AO, Kim EJ. The role of systemic retinoids in the treatment of cutaneous T-cell lymphoma. Dermatol Clin. 2015;33:715–729. 59. Panchal MR, Scarisbrick JJ. The utility of bexarotene in mycosis fungoides and Sézary syndrome. Onco Targets Ther. 2015;8:367–373. 60. Bouwhuis SA, Davis MD, el-Azhary RA et al. Bexarotene treatment of late-stage mycosis fungoides and Sezary syndrome: Development of extracutaneous lymphoma in 6 patients. J Am Acad Dermatol. 2005;52:991–996. 61. Breneman D, Duvic M, Kuzel T. Phase1 and 2 trial of bexarotene gel for skin-directed treatment of patients with cutaneous T-cell lymphoma. Arch Dermatol. 2002;138:325–332. 62. Toctino [product monograph]. Ontario, Canada: GlaxoSmithKline Inc., 2017. Available at: http://ca.gsk.com/ media/1352344/toctino-product-monograph.pdf 63. Diepgen TL, Pfarr E, Zimmermann T. Efficacy and tolerability of alitretinoin for chronic hand eczema under daily practice conditions: Results of the TOCCATA open study comprising 680 patients. Acta Derm Venereol. 2012;92:251–255. 64. Rodgers M, Griffin S, Paulden M et al. Alitretinoin for severe chronic hand eczema: A NICE single technology appraisal. Pharmacoeconomics. 2010;28:351–362. 65. Bodsworth NJ, Bloch M, Bower M et al. Phase III vehiclecontrolled, multi-centered study of topical alitretinoin gel 0.1% in cutaneous AIDS-related Kaposi’s sarcoma. Am J Clin Dermatol. 2001;2:77–87. 33 Teratogenicity and Registry Programs Reese L. Imhof and Megha M. Tollefson Introduction and History Vitamin A and its bioactive metabolite, retinoic acid, are vital to mammalian embryogenesis. The role of vitamin A in embryonic development is made possible through enzymes that control the conversion of retinol, the alcohol form of vitamin A, to an aldehyde (retinaldehyde) and then to retinoic acid, a carboxylic acid. Through binding to retinoid receptors, retinoic acid plays a crucial role in signal transduction and gene transcription pathways that regulate the development of many organs (1). Both deficient and excess levels of vitamin A during embryogenesis can cause congenital malformations (2,3). It has been well established through studies in animals that large doses of vitamin A and its related compounds are teratogenic. In 1953, Sidney Q. Cohlan (1915–1999) reported in Science that pregnant rats given high doses of vitamin A resulted in a successful pregnancy in only 10%, and that 10% often produced offspring with various congenital anomalies. The congenital malformations that were observed in the pregnant rats exposed to excess vitamin A included exencephaly, brachygnathia, macro­ glossia, cleft lip, cleft palate, and gross defects of the eye, while the control group of pregnant rats did not experience these malformations. It was also observed that the highest number of fetal abnormalities occurred with more vitamin A intake on days two through six of gestation (4). Synthetic retinoids are very similar in chemical composition to vitamin A and have been shown to cause birth defects in humans when taken orally (5,6). The teratogenic effects of retinoids predominantly involve structures originating from the cranial neural crest (5–7). The distinguishing pattern of birth defects that are often seen with maternal retinoid use, termed fetal retinoid syndrome or retinoic acid embryopathy, often involve craniofacial, cardiac, thymic, and central nervous system malformations. Human pregnancies with fetal exposure to isotretinoin (13-cis retinoic acid) in particular have been a­ ssociated with an increased risk of miscarriage and major congenital malformations (8,9), leading to isotretinoin being classified as X and contraindicated in pregnancy. Before being prescribed retinoids, patients must be counseled about teratogenic effects. As many women of childbearing age are prescribed retinoids, concern regarding teratogenic effects has led to the implementation of registry and pregnancy prevention programs. Effects on Embryonic Development and Morphogenesis Retinoic acid appears to act primarily through paracrine signaling, but it is not made by all cells at all stages of development (10). The molecular pathways involved in retinoic acid−induced teratogenesis remain an area of active research. One theory is that excess retinoic acid actually induces a long-lasting, localized retinoic acid deficiency (3). Retinoic acid’s effects on development may also be related to its role in Hox gene expression (11–13). Hox genes are critical regulators of pattern formation in vertebrates, particularly in the development of the body plan of the embryo. It is believed that when embryos are exposed to excess retinoic acid, Hox genes malfunction, subsequently disrupting the genetic control of the body shape and patterning of the pharyngeal arches (14). Translational research has suggested that overexpression of tumor suppressor p53, a pro-apoptotic transcription factor, may also help explain retinoic acid’s teratogenic effects. Developmental studies have supported a vital role of p53 in neural crest cell homeostasis. In addition, overactivation of p53 is associated with fetal alcohol syndrome, Treacher Collins syndrome, and CHARGE syndrome, which exhibit similar craniofacial abnormalities seen in retinoic acid embryopathy. It is hypothesized that retinoic acid induces overactivation of p53 during embryogenesis and increases neural crest cell apoptosis (15–17). Isotretinoin has been shown to disrupt mesoderm formation during cardiac differentiation via abnormal expression of genes involved in signaling pathways, such as TGF-β signaling, that control early mesoderm differentiation (18). Major Components of Retinoid Teratogenicity: Review of Congenital Abnormalities As retinoids are believed to be involved in the Hox signaling pathways that are crucial in the development of the pharyngeal arches, it is the derivatives of the pharyngeal arches that are often affected by excess retinoic acid exposure during pregnancy. Although there have been over 70 different anomalies described in the literature from excessive retinoid exposure, the malformations that are most frequently seen are cardiovascular, 207 208 Retinoids in Dermatology craniofacial, central nervous system, and thymic (8,14,19–22). These retinoid embryopathy–associated malformations are outlined in Table 33.1. Table 33.2 compares teratogenicity over three generations of retinoids. TABLE 33.1 The Malformations Most Often Associated with Retinoid Embryopathy System Circulatory (22–24) Lymphatic/Immune (22–24,30,33) Nervous (22–32) Ocular/Visual (22–26) Skeletal (includes Craniofacial) (22–26,30,34,35) Retinoid Embryopathy–Associated Malformations Septal, aortic arch and conotruncal defects (transposition of the great vessels, hypoplastic aorta, interrupted aortic arch, septal defects, tetralogy of Fallot, truncus arteriosus, and retroesophageal right subclavian artery) Abnormal thymus (thymic hypoplasia, thymic aplasia, thymic ectopia) Neural tube defects, microcephaly, holoprosencephaly, hydrocephalus, cortical and cerebellar defects including cortical agenesis and myelomeningocele, DandyWalker malformation, developmental delay, intellectual disability, hearing loss, and vestibular dysfunction Microphthalmia, ocular hypertelorism/ telecanthus, optic nerve atrophy Cleft palate, cleft lip, micrognathia, depressed nasal bridge, midface hypoplasia, microtia, anotia, stenotic or absent auditory canals, growth retardation, aplasia or hypoplasia of long bones, and limb reduction While all systemic retinoids are considered teratogenic, studies regarding the comparative teratogenicity of retinoids have suggested differences in teratogenic potential (36,37). This may be due to their different interactions with the nuclear retinoic acid receptors (RARs) and retinoid X receptors (RXRs) (38). Some retinoids have been suspected to have reduced teratogenicity due to decreased placental transfer, but when investigated in animal models are found to have potent teratogenicity (39). A study comparing the teratogenicity of first-(non-aromatic) and second(monoaromatic) generation oral retinoids in rats found the incidence of abnormal fetuses was markedly increased (50%–100%) by isotretinoin (13-cis retinoic acid), tretinoin (all-trans-retinoic acid), etretinate, acitretin, and N-(4-hydroxyphenyl)-retinamide (37). Fenretinide, another first-generation retinoid, is also considered to have teratogenic potential, although evidence is limited (37,40,41). There have been no reports of teratogenicity in humans consequent to fetal exposure of alitretinoin (9-cis retinoic acid) (42); however, it is still considered teratogenic and a study of pregnant mice found that it was approximately half as potent a teratogen as tretinoin (all-trans-retinoic acid) (43). The second-generation monoaromatic retinoids etretinate and its active metabolite acitretin are known to be potent teratogens, and it is recommended that they be avoided if possible in women of childbearing potential (44–46). As a precaution with etretinate/acitretin, the United States Food and Drug Administration (FDA) developed a program called “Do Your P.A.R.T.” and recommends that women should not become pregnant for at least 3 years after treatment discontinuation. This is due to the number of reported birth defects after discontinuation of therapy and the lengthy half-life of etretinate/acitretin (approximately 100 days) (44,47–49). Given TABLE 33.2 A Comparison of the Systemic Retinoids Used Specifically for Dermatologic Purposes Systemic (Oral) Retinoid Retinoid Generation Isotretinoin (13-cis retinoic acid) First (non-aromatic) Alitretinoin (9-cis retinoic acid) First (non-aromatic) Fenretinide First (non-aromatic) Second (monoaromatic) Etretinate Acitretin Bexarotene Second (monoaromatic) Third (polyaromatic) Clinical Uses Comparative Level of Teratogenicity Nodulocystic acne—severe, recalcitrant (FDA approved) Non-FDA uses include: acanthosis nigricans, acne vulgaris, dermal angiomatosis, basal cell carcinoma, cellulitis, condyloma acuminatum, cutaneous sarcoidosis, eccrine poroma, elastosis perforans serpiginosa, epidermolysis bullosa, granuloma annulare, hypertrophic-type discoid lupus erythematosus, keratoacanthoma, keratosis, keratosis follicularis, malassezia folliculitis, melanoma, Muir-Torre syndrome, mycosis fungoides, papillomatosis, parakeratosis, perioral dermatitis, psoriasis, pyoderma faciale, rosacea, squamous cell carcinoma, steatocystoma multiplex, transient acantholytic dermatosis Cutaneous Kaposi sarcoma (FDA approved) Non-FDA uses include: chronic hand eczema, ichthyoses, Darier disease, pityriasis rubra pilaris, premalignant and malignant skin lesions, lupus erythematosus Cutaneous T-cell lymphoma (non-FDA use) ++++ Psoriasis (FDA approved) Non-FDA uses include: Bowenoid papulosis, cutaneous amyloidosis, cutaneous sarcoidosis, disorder of keratinization, hidradenitis suppurativa, keratoacanthoma, lichen planus, pemphigus, plasma cell vulvitis, psoriatic arthritis, recurrent streptococcal erysipelas Psoriasis (FDA approved), lichen planus (non-FDA use), skin cancer prophylaxis in transplant patients (non-FDA use) Cutaneous T-cell lymphoma (FDA approved), psoriasis (non-FDA use), Kaposi sarcoma (non-FDA use) +++++ ++ +++ +++++ Unknown 209 Teratogenicity and Registry Programs the lengthy post-acitretin contraception period, isotretinoin may be used for women of childbearing age with psoriasis, although isotretinoin is less effective than acitretin for psoriasis (23). Fetal malformations have been reported with the third-­ generation polyaromatic retinoids. While topical tazarotene has minimal systemic absorption and elimination is rapid, it is considered a teratogenic substance and contraindicated in pregnancy, as it is unknown what level of exposure can result in teratogenic effects in humans (50,51). Oral adapalene is known to be teratogenic in animals, and while there is a lack of data on the risk of topical adapalene, a study on transdermal absorption following daily application of 0.1% adapalene gel detected no circulating adapalene and only small amounts in the feces (52). A case of retinoid embryopathy was reported in a woman treated with topical adapalene gel from 1 month prior to conception until 13 weeks gestational age; however, the authors note that one report does not necessarily establish causality (52). Topical Retinoids Clinical indications for topical retinoids in dermatology include acne vulgaris (tretinoin, adapalene, tazarotene), photoaging (tretinoin, tazarotene), psoriasis (tazarotene), cutaneous T-cell lymphoma (bexarotene), and cutaneous Kaposi sarcoma (alitretinoin). Some additional, non-FDA approved clinical indications for topical retinoids include ichthyoses, rosacea, pigmentary disorders, pityriasis rubra pilaris, actinic keratoses, lentigines, striae, lichen planus, verrucae planae, corticosteroid-induced atrophy, wound healing, Darier disease, and skin cancer therapy and prevention (23). While topical all-trans-retinoic acid (tretinoin) has been shown to undergo minimal systemic absorption and negligibly increases endogenous levels (53,54), the question of whether topical retinoids are teratogenic has remained a subject of debate. Animal studies have suggested a low risk of embryotoxicity with the application of topical tretinoin (55). Studies on absorption of topical retinoids in laboratory animals have also shown plasma concentrations lower than those seen with nonteratogenic oral doses (56). While many clinicians believe that topical retinoids do not lead to retinoid embryopathy, there have been some cases of suspected topical retinoid−related embryotoxicity reported in the literature (57–59). Two cases were described in Lancet. In one case, the infant had multiple congenital defects including supraumbilical abdominal wall defects, diaphragmatic hernia, dextroposition of the heart, and a right-sided upper limb reduction defect previously associated with oral isotretinoin. In this case, there was maternal topical 0.05% tretinoin exposure both before conception and during the first 5 weeks of gestation (57). The other case reported in Lancet involved an infant born with hypoplastic ear and atresia of the external auditory meatus on the right side. The mother in this case had also used topical 0.05% tretinoin before conception and during the first 11 weeks of gestation (58). Although these cases have been reported, multiple prospective cohort studies have suggested that there is not an increased risk of retinoid embryopathy with topical retinoid exposure (56,60,61). In addition, a systematic review and meta-analysis was performed utilizing data from 654 pregnant women who were exposed to topical retinoids and 1375 unexposed control pregnant women and did not detect significant increases in rates of major congenital malformations, spontaneous abortions, stillbirth, elective termination of pregnancy, low birthweight, or prematurity (62). While these findings are reassuring, the authors preface that the statistical power is not adequate to justify the use of topical retinoids during pregnancy. Given the ambiguous risk–benefit ratio, it is still generally recommended to use with caution, approach every patient individually, and if possible avoid topical retinoids during pregnancy (22,61,63). Retinoid Exposure: Other Considerations There is a lack of data regarding retinoid use while breastfeeding, but it is recommended that systemic retinoids be avoided while breastfeeding. Many providers also advise patients to avoid topical retinoids while breastfeeding (22). Male Partners and Retinoid Embryopathy There remain limited data regarding the safety of systemic retinoids in reproductively active men and pregnancy outcomes where only the male partner was taking systemic retinoids at the time of conception (64). One population-based study included 80 fathers who were exposed to isotretinoin during the last 3 months prior to conception. The authors report that while overall the odds of adverse pregnancy outcomes were not increased, seven pregnancies ended in a preterm birth and there was one case of a patent ductus arteriosus and Down syndrome (65). Post-marketing surveillance for isotretinoin reported four pregnancies with defects compatible with retinoid exposure when the father was taking isotretinoin; however, it should be noted that two of these cases had other possible explanations and two were incomplete reports (64). In looking at available data from paternal treatment with acitretin, birth defects seen in pregnancies fathered by male acitretin patients were not consistent with retinoid embryopathy and did not occur at frequencies greater than what was expected in the general population (64,66). In addition, drug levels in the ejaculate of men on a retinoid for greater than or equal to 1 month have concluded that the risk of teratogenicity is negligible (64). It is advised that male patients be informed that there are limited data regarding the risk that paternal retinoid exposure may pose during conception (67). While retinoid exposures that men have are unlikely to increase risks to a pregnancy, it is still generally advised that men avoid systemic retinoids if possible when they are actively trying to father children (23). History and Overview of Registry/ Pregnancy Prevention Programs (in the United States and Internationally) Various risk management programs and registries have been developed in an attempt to prevent fetal exposure to isotretinoin and mitigate risks associated with isotretinoin. In the United States, the first approach came voluntarily from the pharmaceutical company Hoffmann-La Roche (Roche) in 1982 when they began distributing Accutane, the first approved form of isotretinoin. The teratogenic effects of isotretinoin were well known from animal research, so Roche released the drug with warnings and brochures for patients; however, there were multiple reports of pregnancies in patients on isotretinoin with resultant 210 fetal malformations (68,69). Between 1998 and 2005 the FDA developed a number of risk management programs, including the Pregnancy Prevention Program (PPP) and the SMART (System to Manage Accutane-Related Teratogenicity) program (68–71). The FDA continually evaluated these measures and concluded that they were not sufficient in reducing the number of isotretinoinexposed pregnancies (71). Therefore in 2006, the FDA mandated the most rigorous program currently in use—a single, shared, computer-based risk evaluation and mitigation strategy program called iPLEDGE. In order to receive isotretinoin, all patients are required to participate in the iPLEDGE program. In addition, all healthcare providers, pharmacies, and wholesale distributors must also register with iPLEDGE. Patients registered as women of childbearing potential are required to use two forms of birth control chosen from an approved iPLEDGE list, with abstinence included as an option. They must also complete prescriber-administered pregnancy testing before and during isotretinoin usage, with two negative pregnancy tests required prior to starting isotretinoin therapy (69,71,72). From the date of the second negative pregnancy test, patients have a 7-day window during which time they must receive their isotretinoin prescription; if it is not dispensed during this period, the patient will be “locked out” of the system and must wait to submit a new negative pregnancy test (69). Due to the time it can take to clear isotretinoin systemically, there is an additional final pregnancy test required by iPLEDGE post-treatment. This is important, as there have been cases of congenital malformations arising due to maternal isotretinoin exposure 1 month before pregnancy. It is advised that women allow at least 1 month following cessation of isotretinoin before attempting to conceive (22,69,73). Patients taking isotretinoin are also advised through iPLEDGE not to donate blood for at least 1 month after they stop taking the drug (68,74). iPLEDGE has not been without criticism. Studies have suggested that iPLEDGE has not significantly decreased the risk of fetal exposure to isotretinoin when compared to the prior SMART program (75–77). Some feel that the iPLEDGE program’s information on pregnancy prevention is not focused on what works best; rather it focuses on scaring patients about the risks of isotretinoin, which typically is not as effective (77). Other potential issues that have been discussed include that some patients may not be willing to discuss their sexual activity with their provider, some may receive inadequate counseling about contraceptive use, some may not feel motivated to follow through with using two different forms of contraception for every sexual episode over months of treatment, and some may turn to the internet to obtain isotretinoin without a prescription (71). Failure rates of abstinence have been discussed as another issue, as one study found that 19% of women who committed to abstinence while on isotretinoin therapy admitted to having intercourse. This is a particular concern with teenagers, due to teenagers’ higher risk of unintended pregnancy (77). In addition, the requirement of registering patients in only one of three mutually exclusive categories (men, women of nonchildbearing potential, or women of childbearing potential) has brought ethical concerns for patients who are transgender or intersex. This classification system conflates childbearing potential with female gender identity and impedes culturally competent care for transgender and intersex patients. This could easily be improved by using gender-neutral categorization and including guidance for this patient population (78). Retinoids in Dermatology In order to improve the iPLEDGE program, an emphasis on the effectiveness of contraceptives is recommended as well as the removal of requirements that do not effectively support the mission of the program. It has been suggested that iPLEDGE materials should be revised so that patients have access to clear information on how to avoid isotretinoin-associated birth defects with a focus on contraceptives that are most effective. For example, subdermal implants and intrauterine contraceptives are 20 times more effective than oral contraceptives. Providing information on the relative effectiveness of different contraceptive options could improve prevention of isotretinoin-exposed pregnancies (77). Other countries have developed rigorous isotretinoin pregnancy risk management programs as well. In Europe, the European Commission developed a standardized PPP for all isotretinoincontaining products, and some countries, such as Australia and Singapore, also have restricted prescribing rights for isotretinoin (79); however, studies have suggested that not all isotretinoin prescriptions are compliant with the program requirements (79,80). It has been suggested that stringent risk management programs, such as iPLEDGE and PPP in Europe, might not be effective in decreasing the risks of fetal exposure to isotretinoin when used alone. Evidence suggests that these programs increase patients’ fears of teratogenic risks and impart barriers to obtaining these medications but do not translate into a significant reduction in pregnancy exposures to isotretinoin (79). A systematic review evaluating the efficacy of the PPP for isotretinoin in Europe found deficiencies in the implementation of the PPP—compliance was often poor, with pregnancies occurring despite the PPP. The authors concluded that the PPP should be further evaluated to determine how to correct the failures in implementation and whether new measures need to be taken (80). Management during Pregnancy Evidence regarding the management of women who conceive during or after exposure to systemic retinoids is limited. Due to the lack of available data, there are no reliable guidelines for pregnant women to follow if exposed. Given the known teratogenicity of retinoids, pregnancies that have been exposed to systemic retinoids often result in termination either spontaneously or through medical intervention (81,82). It is recommended that counseling be individualized for each patient. Initial counseling includes a discussion of the individual risk of teratogenicity and what options exist for the individual patient. Some women may decide to terminate their pregnancy, while others may not. A maternal fetal medicine consultant may be an appropriate referral. In subsequent antenatal care, identification of developing malformations could lead to a late termination of pregnancy. While there are few guidelines for antenatal management, some interventions may supplement antenatal care. High-dose folic acid is thought to reduce the risk of neural tube defects; however, this benefit may be limited, as the neural tube closes around day 30 of development and women often present later than this. At 16–19 weeks, alpha-fetoprotein levels may indicate neural tube defects (22); however, ultrasound imaging at this time may be a more reliable option. Unfortunately, not all affected fetuses will show defects that are identifiable via imaging (30,83). Last, long-term developmental problems may not be possible to predict (22). Teratogenicity and Registry Programs Conclusions Retinoids are effective in treating many conditions in dermatology and are important clinically in improving distressing conditions; however, the prevention of teratogenicity must be a primary focus. Fetuses exposed to retinoids primarily develop craniofacial, central nervous system, cardiovascular, and thymic abnormalities. Counseling and education regarding teratogenic effects should be provided to patients. Such education should include information on risk of spontaneous miscarriage, fetal malformations, and developmental delay. In order to avoid retinoid embryopathy, effective pregnancy prevention programs are of utmost importance. If pregnancy occurs, care within maternal and fetal medicine can help families in their decision-making process. REFERENCES 1. Duester G. Retinoic acid synthesis and signaling during early organogenesis. Cell. 2009;134:921–931. 2. Zile MH. Vitamin A and embryonic development: An overview. J Nutr. 1998;128:455–458. 3. Lee L, Leung CY, Tang W et al. A paradoxical teratogenic mechanism for retinoic acid. Proc Natl Acad Sci USA. 2012;109:13668–13673. 4. Cohlan S. Excessive intake of Vitamin A as a cause of congenital anomalies in the rat. Science. 1953;117:535–536. 5. Rothman KJ, Moore LL, Singer MR et al. Teratogenicity of high vitamin A intake. N Engl J Med. 1995;333:1369–1373. 6. Hershel J. Retinoids and teratogenicity. J Am Acad Dermatol. 1998;39:118–122. 7. Mulder GB, Manley N, Grant J et al. Effects of excess vitamin A on development of cranial neural crest-derived structures: A neonatal and embryologic study. Teratology. 2000;62:214–226. 8. Lammer EJ, Chen DT, Hoar RM et al. Retinoic acid embryopathy. N Engl J Med. 1985;313:837–841. 9. Benke PJ. The isotretinon teratogen syndrome. JAMA. 1984;251:3267–3269. 10. Kumar S, Duester G. SnapShot: Retinoic acid signaling. Cell. 2012;147:1422. 11. Langston AW, Gudas LJ. Retinoic acid and homeobox gene regulation. Curr Opin Genet Dev. 1994;4:550–555. 12. Marshall H, Morrison A, Studer M et al. Retinoids and Hox genes. FASEB J. 1996;10:969–978. 13. Clagett-Dame M, Knutson D. Vitamin A in reproduction and development. Nutrients. 2011;3:385–428. 14. Tantibanchachai C. Retinoids as teratogens. In: Embryo Project Encyclopedia. [Internet]. Arizona: Arizona State University School of Life Sciences Center for Biology and Society; 2014. [cited 2018 Aug 30]. Available from: ISSN: 1940-5030 http://embryo.asu.edu/handle/10776/7566. 15. Melnik BC. Overexpression of p53 explains isotretinoin’s teratogenicity. Exp Dermatol. 2018;27:91–93. 16. Melnik BC. p53: Key conductor of all anti-acne therapies. J Transl Med. 2017;15:195. 17. Shin DM, Xu XC, Lippman SM et al. Accumulation of p53 protein and retinoic acid receptor beta in retinoid chemoprevention. Clin Cancer Res. 1997;3:875–880. 18. Liu Q, Van Bortle K, Zhang Y et al. Disruption of mesoderm formation during cardiac differentiation due to developmental exposure to 13-cis-retinoic acid. Sci Rep. 2018;8:12960. 211 19. Morrison DG, Elsas FJ, Descartes M. Congenital oculomotor nerve synkinesis associated with fetal retinoid syndrome. J AAPOS. 2005;9:166–168. 20. Braun JT, Franciosi RA, Mastri AR et al. Isotretinoin dysmorphic syndrome. Lancet. 1984;1:506–507. 21. Hill RM. Isotretinoin teratogenicity. Lancet. 1984;1:1465. 22. Browne H, Mason G, Tang T. Retinoids and pregnancy: An update. Obstetr Gynaecol. 2014;16:7–11. 23. Bolognia J, Schaffer J, Cerroni L, editors. Medical therapy retinoids. In: Dermatology E-Book, 4th ed. Amsterdam: Elsevier; 2018, pp. 2209–2210. 24. Erenel H, Ozel A, Oztunc F et al. Antenatal diagnosis of fetal retinoid syndrome at 20 weeks of gestation: A case report. Fetal Pediatr Pathol. 2018;29:1–5. 25. Mondal D, R Shenoy S, Mishra S. Retinoic acid embryopathy. Int J Appl Basic Med Res. 2017;7:264–265. 26. Jahn AF, Ganti K. Major auricular malformations due to Accutane (isotretinoin). Laryngoscope. 1987;97:832–835. 27. Danzer E, Schwarz U, Wehrli S et al. Retinoic acid induced myelomeningocele in fetal rats: Characterization by histopathological analysis and magnetic resonance imaging. Exp Neurol. 2005;194:467–475. 28. Aldinger K, Doherty D. The genetics of cerebellar malformations. Semin Fetal Neonatal Med. 2016;21:321–332. 29. Rosa FW. Retinoic acid embryopathy. N Engl J Med. 1986;315:262. 30. Hand, JL. Retinoic acid: A familiar teratogen. PediatrDermatol. 2012;29:774–776. 31. Chan A, Hanna M, Abbott M et al. Oral retinoids and pregnancy. Med J Austr. 1996;165:164–167. 32. Padmanabhan R. Retinoic acid-induced caudal regression syndrome in the mouse fetus. Reprod Toxicol. 1998;12:139–151. 33. Cohen M, Rubinstein A, Li JK et al. Thymic hypoplasia associated with isotretinoin embryopathy. Am J Dis Child. 1987;141:263–266. 34. Coberly S, Lammer E, Alashari M. Retinoic acid embryopathy: Case report and review of the literature. Pediatr Pathol Lab Med. 1996;16:823–836. 35. Lowenstein EB, Lowenstein EJ. Isotretinoin systemic therapy and the shadow cast upon dermatology’s downtrodden hero. Clin Dermatol. 2011;29:652–661. 36. Steele CE, Marlow R, Turton J et al. In-vitro teratogenicity of retinoids. Br J Exp Pathol. 1987;68:215–223. 37. Turton JA, Willars GB, Haselden JN et al. Comparative teratogenicity of nine retinoids in the rat. Int J Exp Pathol. 1992;73:551–563. 38. Beckenbach L, Baron JM, Merk HF et al. Retinoid treatment of skin diseases. Eur J Dermatol. 2015;25:384–391. 39. Nau H, Elmazar MM, Ruhl R et al. All-trans-retinoyl-betaglucuronide is a potent teratogen in the mouse because of extensive metabolism to all-trans-retinoic acid. Teratology. 1996;54:150–156. 40. Kenel MF, Krayer JH, Merz EA et al. Teratogenicity of N-(4hydroxyphenyl)-all-trans-retinamide in rats and rabbits. Teratog Carcinog Mutagen. 1988;8:1–11. 41. Veronesi U, Mariani L, Decensi A et al. Fifteen-year results of a randomized phase III trial of fenretinide to prevent second breast cancer. Ann Oncol. 2006;17:1065–1071. 42. Morris M, Schifano L, Fong R et al. Safety of alitretinoin for severe refractory chronic hand eczema: Clinical studies and postmarketing surveillance. J Dermatolog Treat. 2016;27:54–58. 212 43. Kochhar DM, Jiang H, Penner JD et al. Placental transfer and developmental effects of 9-cis retinoic acid in mice. Teratology. 1995;51:257–265. 44. Davis SA, Yentzer BA, Feldman SR. Acitretin prescribing patterns in women of childbearing potential. J Drugs Dermatol. 2013;12:799–802. 45. Geiger JM, Baudin M, Saurat JH. Teratogenic risk with etretinate and acitretin treatment. Dermatology. 1994;189:109–116. 46. Goldfarb MT, Ellis CN, Vorhees JJ. Retinoids in dermatology. Mayo Clinic Proceedings. 1987;62:1161–1164. 47. DiGiovanna JJ, Mauro T, Milstone LM et al. Systemic retinoids in the management of ichthyoses and related skin types. Dermatol Ther. 2013;26:26–38. 48. Maradit H, Geiger JM. Potential risk of birth defects after acitretin discontinuation. Dermatology. 1999;198:3–4. 49. Ortiz NE, Nijhawan RI, Weinberg JM. Acitretin. Dermatol Ther. 2013;26:390–399. 50. Marks R. Early clinical development of tazarotene. Br J Dermatol. 1996;135:26–31. 51. Epstein EL, Stein-Gold L. Safety and efficacy of tazarotene foam for the treatment of acne vulgaris. Clin Cosmet Investig Dermatol. 2013;6:123–125. 52. Autret E, Berjot M, Jonville-Bera AP et al. Anophthalmia and agenesis of optic chiasma associated with adapalene gel in early pregnancy. Lancet. 1997;350;339. 53. Chen C, Jensen BK, Mistry G et al. Negligible systemic absorption of topical isotretinoin cream: Implications for teratogenicity. J Clin Pharmacol. 1997;37:279–284. 54. Johnson EM. A risk assessment of topical tretinoin as a potential human developmental toxin based on animal and comparative human data. J Am Acad Dermatol. 1997;36:S86–S90. 55. Nau H. Embryotoxicity and teratogenicity of topical retinoic acid. Skin Pharmacol. 1993;6:35–44. 56. Veraldi S, Rossi LC, Barbareschi M. Are topical retinoids teratogenic? G Ital Dermatol Venereol. 2016;151:700–705. 57. Lipson AH, Collins F, Webster WS. Multiple congenital defects associated with maternal use of topical tretinoin. Lancet. 1993;341:1352–1353. 58. Camera G, Pregliasco P. Ear malformation in baby born to mother using tretinoin cream. Lancet. 1992;3 39:687. 59. Navarre-Belhassen C, Blanchet P, Hillaire-Buys D. Multiple congenital malformations associated with topical tretinoin. Ann Pharmacother. 1998;32:505. 60. Shaprio L, Pastuszak A, Curto G et al. Safety of first-trimester exposure to topical tretinoin: Prospective cohort study. Lancet. 1997;350:1143–1144. 61. Panchaud A, Csajka C, Merlob P et al. Pregnancy outcome following exposure to topical retinoids: A multicenter prospective study. J Clin Pharmacol. 2012;52:1844–1851. 62. Kaplan YC, Ozsarfati J, Etwel F et al. Pregnancy outcomes following first-trimester exposure to topical retinoids: A systematic review and meta-analysis. Br J Dermatol. 2015;173:1117–1118. 63. Akhavan A, Bershad S. Topical acne drugs: Review of clinical properties, systemic exposure, and safety. Am J Clin Dermatol. 2003;4:473–492ç. 64. Kumar P, Das A, Lal NR et al. Safety of important dermatological drugs (retinoids, immune suppressants, anti-androgens and thalidomide) in reproductively active males with respect to pregnancy outcome: A brief review of literature. Indian J Dermatol Venereol Leprol. 2018;84:539–546. Retinoids in Dermatology 65. Engeland A, Bjørge T, Kjersti Daltveit A et al. Effects of ­preconceptional paternal drug exposure on birth outcomes: Cohort study of 340 000 pregnancies using Norwegian population-based databases. Br J Clin Pharmacol. 2013;75: 1134–1141. 66. Geiger JM, Walker M. Is there a reproductive safety risk in male patients treated with acitretin (neotigason/soriatane)? Dermatology. 2002;205:105–107. 67. Albrecht J, Nast A. Paternal drug exposure: Plenty of confounders, few conclusions. Br J Dermatol. 2017;176:847–848. 68. Brinker A, Kornegay C, Nourjah P. Trends in adherence to a revised risk management program designed to decrease or eliminate isotretinoin-exposed pregnancies: Evaluation of the accutane SMART program. Arch Dermatol. 2005;141:563–569. 69. Leyden JJ, Del Rosso JQ, Baum EW. The use of isotretinoin in the treatment of acne vulgaris: Clinical considerations and future directions. J Clin Aesthet Dermatol. 2014;7:3–21. 70. Maloney ME, Stone SP. Isotretinoin and iPLEDGE: A view of results. J Am Acad Dermatol. 2011;65:418–419. 71. Abroms L, Maibah E, Lyon-Daniel K et al. What is the best approach to reducing birth defects associated with isotretinoin? PLOS Med. 2006;3:e483. 72. Werner CA, Papic MJ, Ferris LK et al. Women’s experiences with isotretinoin risk reduction counseling. JAMA Dermatol. 2014;150:366–371. 73. Shirazi M, Abbariki E, Pirjani R et al. Congenital microtia in a neonate due to maternal isotretinoin exposure 1 month before pregnancy: Case report. J Obstet Gynaecol Res. 2015;41:975–978. 74. Shin SY, Shin YH, Lee SW et al. Blood donors on teratogenic drugs and donor deferral periods in a clinical situation. Vox Sang. 2012;102:362–364. 75. Cheetham TC, Wagner RA, Chiu G et al. A risk management program aimed at preventing fetal exposure to isotretinoin: Retrospective cohort study. J Am Acad Dermatol. 2006;55:442–448. 76. Shin J, Cheetham TC, Wong L et al. The impact of the iPLEDGE program on isotretinoin fetal exposure in an integrated health care system. J Am Acad Dermatol. 2011;65:1117–1125. 77. Pierson JC, Ferris LK, Schwarz EB. We pledge to change iPLEDGE. JAMA Dermatol. 2015;151:701–702. 78. Yeung H, Chen SC, Katz KA et al. Prescribing isotretinoin in the United States for transgender individuals: Ethical considerations. J Am Acad Dermatol. 2016;75:648–651. 79. Kovitwanichkanont T, Driscoll T. A comparative review of the isotretinoin pregnancy risk management programs across four continents. Int J Dermatol. 2018;57:1035–1046. 80. Crijns HJ, Straus SM, Gispen-de Wied C et al. Compliance with pregnancy prevention programmes of isotretinoin in Europe: A systematic review. Br J Dermatol. 2011;164:238–244. 81. Henry D, Dormuth C, Winquist B et al. Occurrence of pregnancy and pregnancy outcomes during isotretinoin therapy. CMAJ. 2016;188:723–730. 82. Berard A, Azoulay L, Koren G et al. Isotretinoin, pregnancies, abortions and birth defects: A population-based perspective. Br J Clin Pharmacol. 2007;63:196–205. 83. Boyle RJ. Effects of certain prenatal drugs on the fetus and newborn. Pediatr Rev. 2002;23:1–17. 34 Management of Vitamin A and Retinoid Side Effects Asli Tatliparmak and Berna Aksoy Introduction The term “retinoids” refers to chemical compounds that are derivatives of vitamin A or all-trans retinol. There are two main types of receptors that bind to retinoids: retinoid-binding proteins and retinoid nuclear receptors (1). • First-generation (non-aromatic) retinoids are retinol, isotretinoin, tretinoin, and alitretinoin. • Second-generation (mono-aromatic) retinoids are etretinate, acitretin, and motretinate. • Third-generation retinoids are adapalene, tazarotene, and bexarotene (1). The safety profile and side effects of synthetic retinoids are now well established. Adverse effects are dose-dependent. The majority of side effects are thought to develop as a result of hypervitaminosis A syndrome, but synthetic retinoids have different biologic activities from natural vitamin A (retinol) and its active metabolite, retinoic acid. For this reason, side effects may occur due to both hypervitaminosis and hypovitaminosis of vitamin A (2). Management of Topical Retinoid Side Effects Tretinoin, adapalene, and tazarotene are the topical retinoids currently used in dermatologic practice. The major adverse effect of topical retinoids is irritant contact dermatitis, also named retinoid dermatitis, which includes erythema, dryness, scaling, burning, and itching. The irritative potential depends on the concentration and formulation of the product, with retinoids in an alcoholic gel solution or in a lotion formulation being more irritating. Retinoid dermatitis can be reduced by application of moisturizers or, in more severe cases, the use of low- to mid-potency corticosteroids for 3–7 days (3). The irritation may be prevented by applying the moisturizer before applying the topical retinoid. Percutaneous absorption of topical tretinoin 0.05% is low and ranges between 1% and 2% even after long-term application. Topical tretinoin and adapalene are labeled as pregnancy category C, indicating that a risk cannot be ruled out, because data in humans are lacking and animal studies are either positive or lacking data. Tazarotene is designated pregnancy category X, prohibiting its use during pregnancy and breastfeeding (3). Several years ago, tretinoin cream was thought to be photosensitizing (4). Recent evidence suggests that topical retinoids are neither phototoxic nor photoallergic (5). They are irritants, and if patients expose their irritated skin to sunlight or drying wind, this will exacerbate their discomfort. Evening application of these topical retinoids has been suggested to maximize patient comfort and compliance (5). Management of Systemic Retinoid Side Effects Teratogenicity The most important side effect of retinoids is teratogenicity. Oral retinoids are considered as category X. Fetal malformations caused by retinoids are induced by perturbations of the neural crest cells and central nervous system (6). Two nuclear ligandinduced receptors (retinoic acid receptors and retinoid X receptors) seem to have important roles in retinoid teratogenicity by affecting downstream genes that are important in development (7). These defects, also called retinoic acid embryopathy, may lead to abnormalities of the central nervous system, face, heart, eye, and thymus (8). There is evidence that retinoids decrease the efficacy of oral contraceptives, especially progesterone-only compounds such as the minipills having only norethindrone, by inducing CYP450; therefore, additional contraception using ­barrier methods should be employed (9). Before initiating treatment, there should be two separate pregnancy tests (urine or serum). The patient should start her systemic retinoid treatment on the second or third day of the next menstrual cycle. During treatment, monthly pregnancy tests should be performed (10) and are required by the American iPLEDGE program. When retinoid treatment is discontinued, pregnancy should be avoided for an additional 1 month after isotretinoin, alitretinoin, and bexarotene use, and for 3 years after receiving acitretin (1,11). Mucocutaneous Side Effects Mucocutaneous side effects vary with the agent. Isotretinoin causes more mucosal dryness due to decreasing sebum production, reduced stratum corneum thickness, and altered skin barrier function. Acitretin has been associated with higher incidences of alopecia and palmoplantar dermatitis, whereas bexarotene induces milder mucocutaneous and ocular side effects than other 213 214 retinoids (8,12). Xerosis and cheilitis, in general, are the most frequent side effects of retinoids (8). Twice-daily dosing regimens have been proposed to decrease most side effects such as cheilitis (13). Vitamin E (alpha-­tocopherol) at 800 IU daily was proposed to decrease ­mucocutaneous side effects of oral isotretinoin treatment but later it was shown to be controversial (13,14). Administration of oral omega-3 has also been suggested to decrease the mucocutaneous side effects of retinoids (15). Retinoids in Dermatology severe paronychia, topical antibacterials or silver nitrate cauterization have been suggested to be useful (16,21). Hair Dose-dependent diffuse telogen hair loss is commonly seen with etretinate and acitretin but less often with isotretinoin (2,22). Such hair loss occurs with higher doses, so the problem can be remedied by reducing the dosage and/or duration of the treatment (22). Cheilitis Cheilitis affects nearly all patients. Secondary Staphylococcus aureus infection may occur. A moisturizing lip balm or petrolatum may be started on the first day of retinoid treatment and applied at least 4–5 times per day (16). In more severe cases, there may be perioral inflammation, requiring the use of m ­ oderate-potency topical steroids (17). If the cheilitis persists, S. aureus infection should be considered (17). Xerophthalmia and Blepharoconjunctivitis The most frequent ocular adverse effects due to retinoids include dry eye, conjunctivitis, hordeolum, chalazion, blepharitis, and ocular pain. Artificial teardrops and/or gels are used in the treatment of dry eye illness. Other therapeutic options include topical steroids, topical cyclosporine, and topical autologous serum (18). Xerophthalmia due to decreased meibomian gland secretion can lead to blepharoconjunctivitis, more often in patients wearing contact lenses (19). Musculoskeletal Side Effects Upwards of 50% of patients receiving retinoids may have muscular pain (6), usually minor enough for patients to obtain relief with nonsteroidal anti-inflammatory drugs (23). When the pain is severe enough or not responsive to anti-inflammatory drugs, consideration should be given to discontinuing the retinoid (16). Myalgia can also be observ
 0
0
advertisement
Related documents



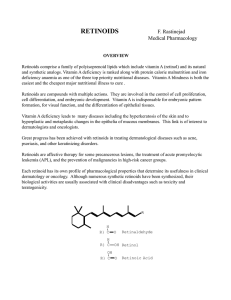
Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users